
Abstract
B7-H3, one of the costimulatory members participating in checkpoint pathway, has been shown to be upregulated after hepatitis B virus (HBV) infection. To further explore the clinical significance of dynamic B7-H3 expression during the progression of HBV infection, we systematically investigated the expression pattern of B7-H3 and the correlation of B7-H3 expression with the ratio of T lymphocyte subsets and clinical parameters at different stages in the course of the disease. Flow cytometry and enzyme-linked immunosorbent assay data showed that soluble form of B7-H3 (sB7-H3) was positively correlated with the frequency of Treg cells in acute hepatitis B (AHB), chronic hepatitis B (CHB), and hepatocellular carcinoma patients with HBV infection (HBV-HCC). Membrane form of B7-H3 (mB7-H3) expressed on Treg cells and monocytes was positively correlated with the frequency of Treg cells in CHB. SB7-H3 had relationship with mB7-H3 expressed on Treg cells and monocytes at different stages during HBV infection, except for HBV-HCC. MB7-H3 expressed on Treg cells was positively correlated with that on monocytes in AHB, CHB, HBV-liver cirrhosis, and HBV-HCC. The B7-H3 expression was positively correlated with aspartate aminotransferase and alanine aminotransferase levels in CHB and sB7-H3 level was higher in late tumor/node/metastasis (TNM) stage in HCC. Higher mB7-H3 expression was associated with greater tumor size, later TNM stage, and worse prognosis in HBV-HCC indicated by immunohistochemistry. Taken together, these results suggested that B7-H3 might contribute to the progression of HBV infection by triggering inhibitory signals in effector T cells and it was closely associated with the progression and poor prognosis during HBV infection. B7-H3 could be utilized as a potential clinical indicator and a potential target for therapeutic strategies against HBV infection.
Introduction
H
An abnormal immune response is one of the main factors causing chronic HBV infection. During infection, HBV-specific CD8+ T lymphocytes play an important role in viral clearance (7, 13). The negative coinhibitory ligands expressed on CD14+ monocytes and CD4+ CD25high Treg cells can inhibit the function of effector T cells (1). Since the costimulatory signaling pathways are necessary for T cell activation and different costimulatory molecules have different function in modulating T cell activation, blocking the inhibitory costimulatory molecules may provide a new method for the treatment of HBV infection-related disease (9, 14).
B7-homologue 3 (B7-H3), also known as CD276, is a costimulatory member of the B7 family (6). B7-H3 has soluble form (sB7-H3) and membrane form (mB7-H3). B7-H3 expression remains a low level in normal cells as well as in inactivated T lymphocytes. Several immune cell types express increased B7-H3 after activation, including B cells, T cells, and natural killer cells (5, 6), as well as in various cancer cells such as breast (2), ovarian (18), prostate (4), pancreatic (19), gastric (10), and non-small cell lung cancers (17). These suggested the importance of B7-H3 in infection immunity and antitumor immunity.
Based on our previous finding, B7-H3 expressed on the membrane of peripheral CD14+ monocytes and CD4+ CD25high Treg cells. Treg cells had higher level of B7-H3 than monocytes. The B7-H3 expression in peripheral monocytes, Treg cells, and sB7-H3 increased as HBV infection-related disease progresses (16). In this study, we aspire to further explore the clinical significance of dynamic B7-H3 expression during the progression of HBV infection.
Materials and Methods
Clinical samples
Blood from healthy control donors (HC) (n = 20), patients with acute hepatitis B (AHB) infection (n = 25), patients with CHB infection (n = 83), LC patients with HBV infection (HBV-LC) (n = 22), and HCC patients with HBV infection (HBV-HCC) (n = 28) was collected along with tissue from HCC patients with HBV infection (n = 61). The HBV-HCC tissue was collected from January 2017 to February 2018. Healthy donors were serum HBV antigen and antibody negative and did not have viral hepatitis and any autoimmune disease. AHB was defined by the presence of HbsAg, HbeAg, HbcIgM (≥1:1,000), HBV-DNA, and medical history. CHB was defined by persistent elevation of alanine aminotransferase (ALT) levels for 6 months. The diagnosis of HBV-LC was dependent on computed tomography (CT)-acquired images and laboratory findings. HBV-HCC was diagnosed by histology, alpha-fetoprotein (AFP) levels, and CT imaging findings. Clinical data were extracted from medical records. All patients were not coinfected with hepatitis C virus, hepatitis D virus, or HIV and did not have other liver-damaging conditions such as autoimmune disease, alcoholic liver disease, or drug-induced hepatitis. None of the patients received antiviral therapy and/or immune therapy before enrollment. HBV-HCC patients included in the survival analysis have received the same treatment. Permission for this study was obtained from the Ethics Committee of The Fifth People's Hospital of Suzhou. Informed consent was obtained from all patients involved in this study.
Flow cytometry analysis
To determine CD4+, CD8+, CD14+, and CD25+ populations and B7-H3 expression in the peripheral blood, CD3-ACP, CD4-PerCP, CD25-FITC, and CD14-FITC were purchased from BD Pharmingen (San Jose, CA); B7-H3-PE was purchased from Biolegend (San Diego, CA). Briefly, for each test, 50 μL of fresh heparinized whole blood from the patients or healthy donors was incubated with antibodies (10 μL) for 15 min, lysed with red blood cell lysis buffer, then subsequently dealt with phosphate-buffered saline, mixed, and eventually detected by BD FACS Aria with BD FACS Diva software support (San Jose, CA). Data were analyzed by FlowJo (San Carlos, CA).
Enzyme-linked immunosorbent assay
The peripheral blood samples were collected with a plasma preparation tube and allowed to clot for 2 h at room temperature. The tube was then centrifuged at 3,000 rpm for 15 min and the resulting serum was stored at −80°C for the enzyme-linked immunosorbent assay (ELISA). The level of sB7-H3 in the serum was analyzed with ELISA Kits (BlueGene, Co., Ltd., Shanghai, China) according to the manufacturer's instructions.
Detection for HBV-DNA load and liver function tests
HBV-DNA was quantified with the Roche Light Cycler 480 Real-Time PCR System (Roche, Germany) and reagents (Sansure Biotech, Ltd., Hunan, China). Standard automatic biochemistry analyzer (Hitachi7600) and reagents (Wako Pure Chemical Industries, Ltd., Japan) were employed to detect the liver function, including ALT, aspartate aminotransferase (AST), and so on.
Immunohistochemical staining of B7-H3
For immunohistochemistry analysis, goat anti-human B7-H3 polyclonal antibody (1:150) was purchased from R&D (Minneapolis, MN). The sections were deparaffinized in xylene, dehydrated in descending dilutions of ethanol, and then treated with 3% hydrogen peroxide, which blocked the endogenous peroxidase activity. The sections were then autoclaved in 0.01 M citrate buffer (pH 6.0) for 2 min for antigen retrieval, incubated with 3% bovine serum albumin, which blocked nonspecific staining, and incubated with primary antibody followed by testing with a ChemMate Envision Detection Kit (Gene Tech Company Limited, Shanghai, China). Finally, the sections were counterstained by hematoxylin. All tissue staining was performed in a single experiment.
Evaluation of immunohistochemical staining
B7-H3 expression was evaluated by two independent pathologists who were unaware of the patients' clinical profiles. B7-H3 expression was scored based on both the staining intensity and the percentage of stained cells. B7-H3 staining intensities were scored as 0, 1, 2, and 3, and the categories were defined as follows: 0 = negative, 1 = weak, 2 = moderate, and 3 = strong. The percentage of cells that stained was manually evaluated (0–100%). The final B7-H3 staining score was derived from the percentage of stained cells and the intensity scores. HBV-HCC patients were divided into two groups—B7-H3Negative/Weak and B7-H3Moderate/Strong—according to median of the scores.
Statistical analysis
Statistical analysis was performed using SPSS 22.0 software (SPSS Inc., Chicago, IL). The Spearman correlation test, Pearson's chi-squared test, and Fisher's exact test were applied to compare statistical evaluations among groups and for correlation analysis. Univariate analysis of progress-free survival was estimated using the Kaplan–Meier method, and multivariable analysis was performed using the Cox proportional hazards regression model. A two-tailed p < 0.05 was considered statistically significant.
Results
Investigating the correlation between B7-H3 expression and the frequency of T lymphocyte subsets during the progression of HBV infection
This study detected the frequency of T lymphocyte subsets in peripheral blood and B7-H3 expression pattern to explore the influence of B7-H3 on immune system. B7-H3 expression on CD4+ CD25high Treg cells and CD14+ monocytes at different disease stages is shown in Supplementary Figure S1 (Supplementary Data are available online at
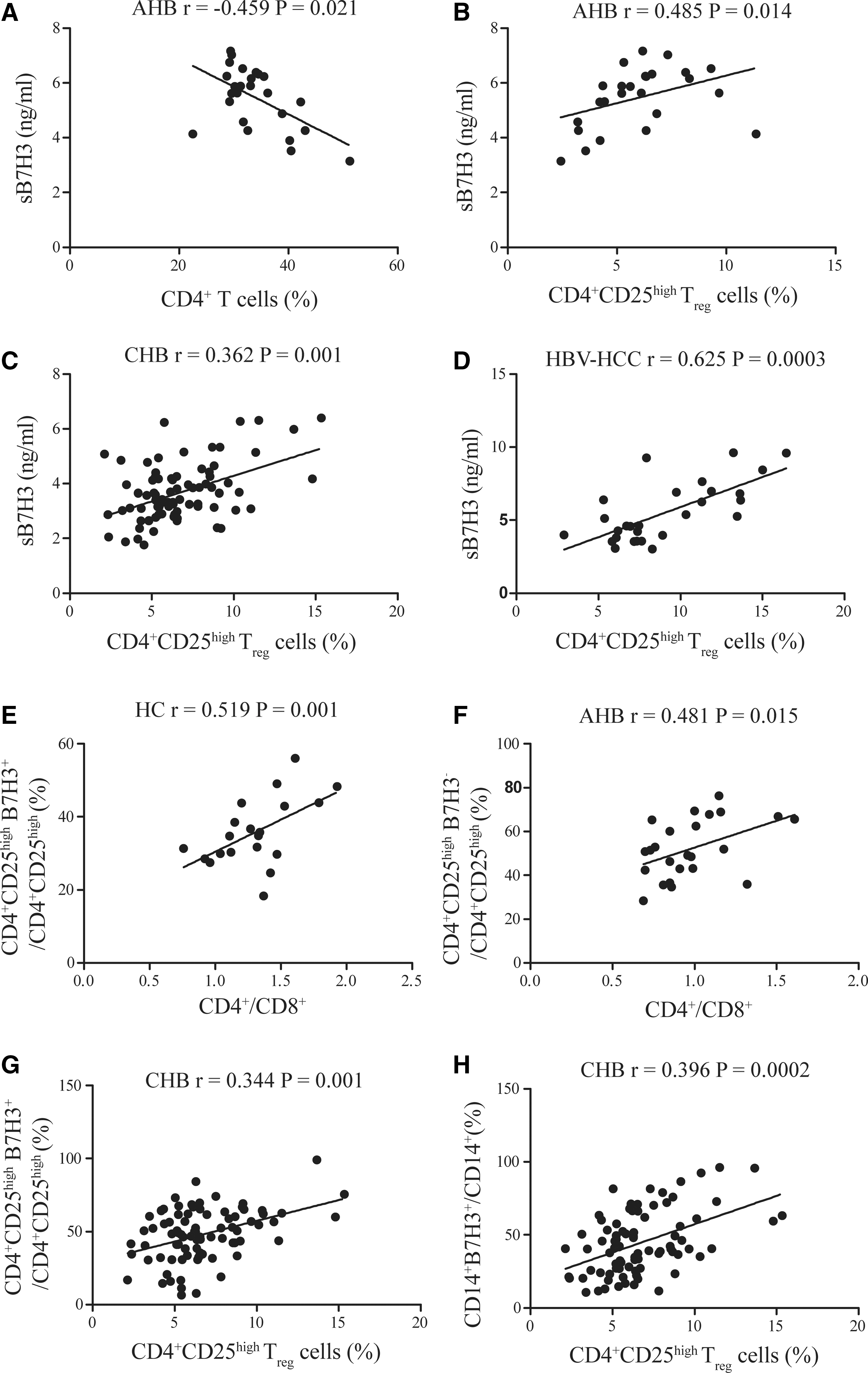
The correlation between B7-H3 expression and T lymphocyte subset frequency during the progression of HBV infection.
Analyzing the correlation between sB7-H3 expression and mB7-H3 expression on immune cell subgroups during the progression of HBV infection
SB7-H3 was negatively correlated with mB7-H3 expression on Treg cells (r = −0.644, p = 0.001) and monocytes (r = −0.661, p = 0.0003) in AHB, and positively correlated with mB7-H3 expression on monocytes in HC (r = 0.531, p = 0.016), mB7-H3 expression on Treg (r = 0.356, p = 0.001) and monocytes (r = 0.511, p = 0.0000008) in CHB, and mB7-H3 expression on monocytes (r = 0.583, p = 0.004) in HBV-LC. MB7-H3 expression on Treg cells was positively correlated with mB7-H3 expression on monocytes in AHB (r = 0.705, p = 0.00008), CHB (r = 0.785, p < 0.00001), HBV-LC (r = 0.650, p = 0.001), and HBV-HCC (r = 0.529, p = 0.0004) (Supplementary Table S3).
Analyzing the correlation between B7-H3 expression and clinical parameters during the progression of HBV infection
The results suggested that sB7-H3 was positively correlated with AST levels in CHB (r = 0.333, p = 0.002) and AFP in HBV-HCC (r = 0.581, p = 0.001). MB7-H3 expression on Treg cells and monocytes was positively correlated with ALT (r = 0.234, p = 0.033, and r = 0.352, p = 0.001, respectively) and AST levels in CHB (r = 0.288, p = 0.008, and r = 0.409, p = 0.0001, respectively). The frequency of CD14+ B7-H3+ population in CHB was positively correlated with HBV DNA load (r = 0.218, p = 0.048). However, no significant correlation between B7-H3 expression and above clinical parameters was observed in AHB, HBV-LC, and HBV-HCC groups (Table 1). Besides, the sB7-H3 level was higher in late tumor/node/metastasis (TNM) stage of HCC than early TNM stage (p = 0.03), but mB7-H3 expression on Treg cells and monocytes had no difference between different TNM stage of HCC (p = 0.96 and p = 0.42, respectively) (Fig. 2).
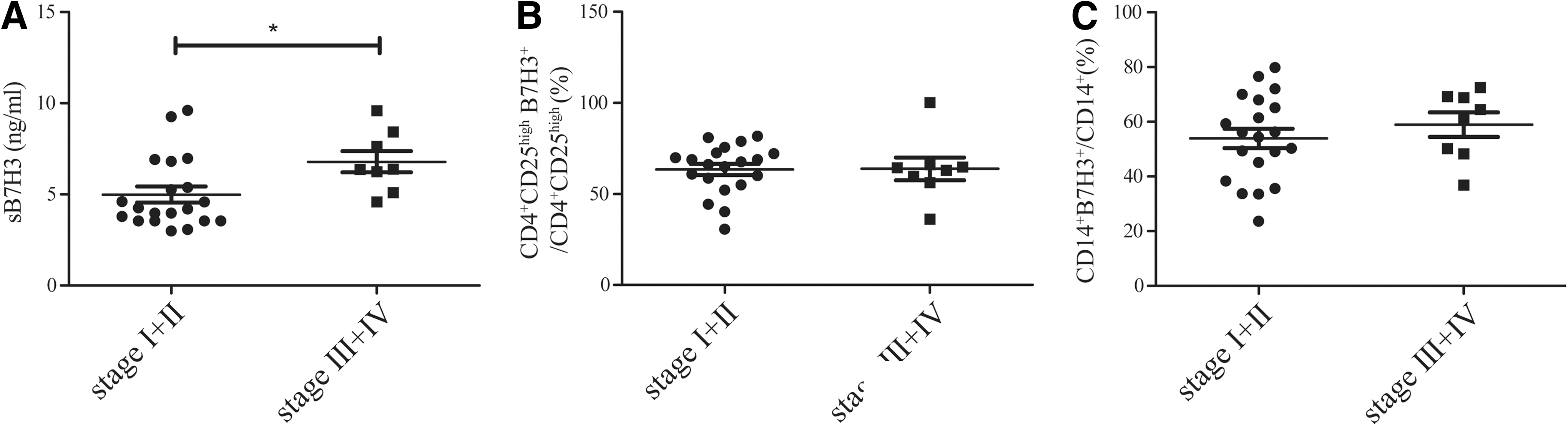
B7-H3 expression in different stages of HBV-HCC.
Correlation Between B7-H3 Expression and the Clinical Parameters During the Progression of Hepatitis B Virus Infection
AFP, alpha-fetoprotein; AHB, acute hepatitis B; ALT, alanine aminotransferase; AST, aspartate aminotransferase; B7-H3, B7-homologue; CHB, chronic hepatitis B; HBV, hepatitis B virus; HBV-HCC, hepatocellular carcinoma patients with HBV infection; HBV-LC, liver cirrhosis patients with HBV infection; HC, healthy control donors; LC, liver cirrhosis; N/A, not applicable; sB7-H3, soluble form of B7-H3.
Expression pattern of B7-H3 in HBV-HCC
To further study the expression pattern of B7-H3 in HBV-HCC and their clinical implications, we performed an immunohistochemical examination in HBV-HCC tissue (n = 61) and adjacent normal tissue (n = 61). The results showed that 35 (57.4%) tumor samples and 7 (11.5%) peritumor samples had moderate to strong B7-H3 expression (Fig. 3). Higher B7-H3 expression level was associated with greater tumor size (p = 0.014) and a later TNM stage (p = 0.033). There was no significant association between B7-H3 expression and age, gender, drinking habits, tumor differentiation, nodal status, and carcinoembryonic antigen, AFP, ALT, or AST (Table 2).
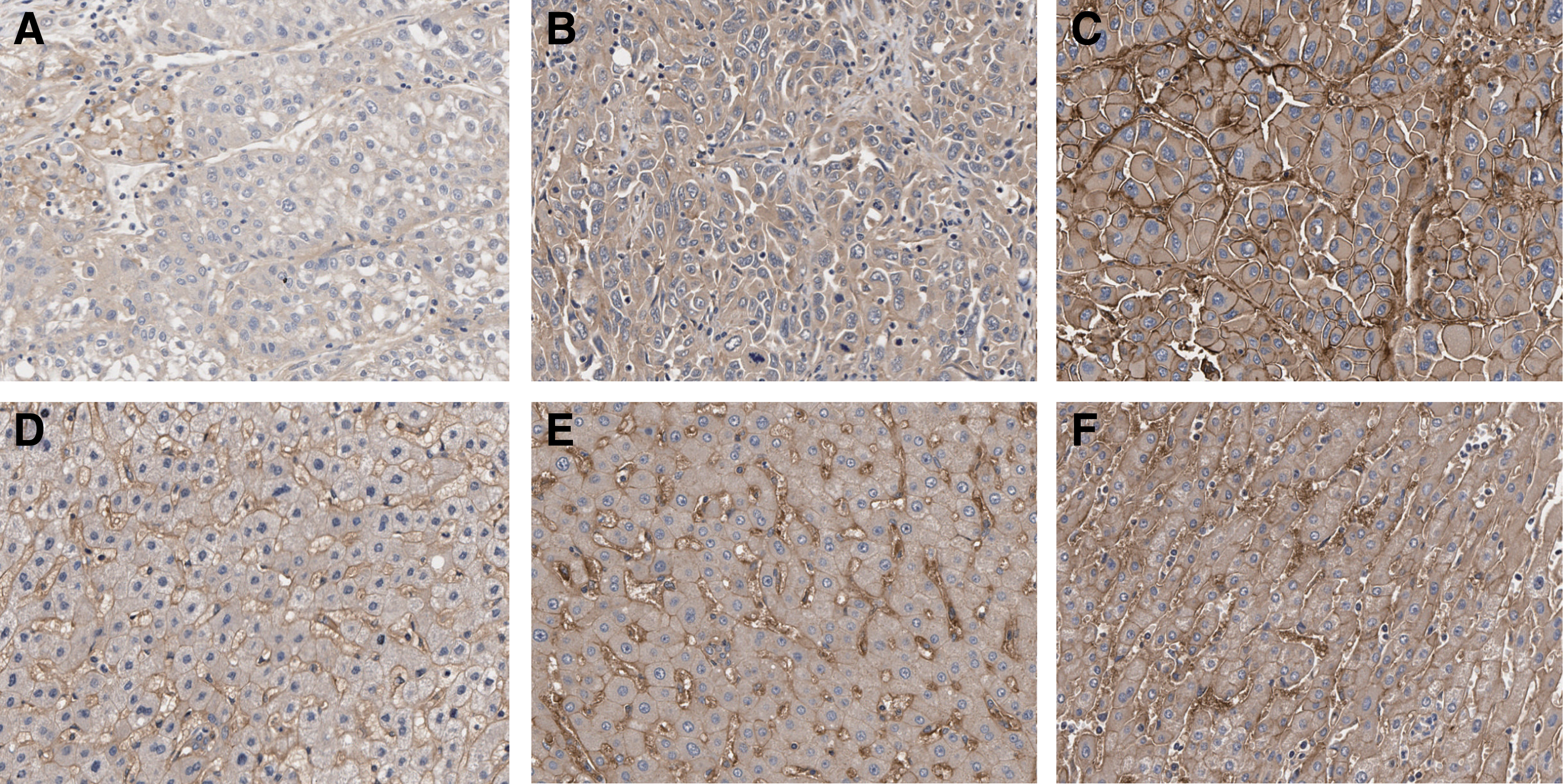
Representative B7-H3 immunohistochemical staining in HBV-HCC and adjacent normal tissues in high-magnification (200 × ) images.
Relationships Between B7-H3 Expression and Clinicopathological Parameters
CEA, carcinoembryonic antigen; TNM, tumor/node/metastasis.
The relationship between B7-H3 expression and prognosis in HBV-HCC
Sixty-one patients with HBV-HCC were included in the prognostic analysis. The overall follow-up periods ranged from 2 to 82 weeks (median 48 weeks). Kaplan–Meier survival analysis showed that the B7-H3Moderate/Strong group had a worse survival rate than the B7-H3Negative/Weak group (p = 0.012) (Fig. 4). Multivariable analysis was performed using the Cox proportional hazards regression model to examine the association between tumor B7-H3 intensity and patient overall survival after adjusting for clinicopathologic features. High expression of B7-H3 in HBV-HCC was significantly associated with poor prognosis even after adjusting for confounding factors (p = 0.042). The adjusted hazard ratio of the B7-H3Moderate/Strong group was 2.760 (95% confidence interval, 1.040–7.324) compared to the B7-H3Negative/Weak group (Table 3), suggesting that B7-H3 is an independent risk factor for a worse survival.
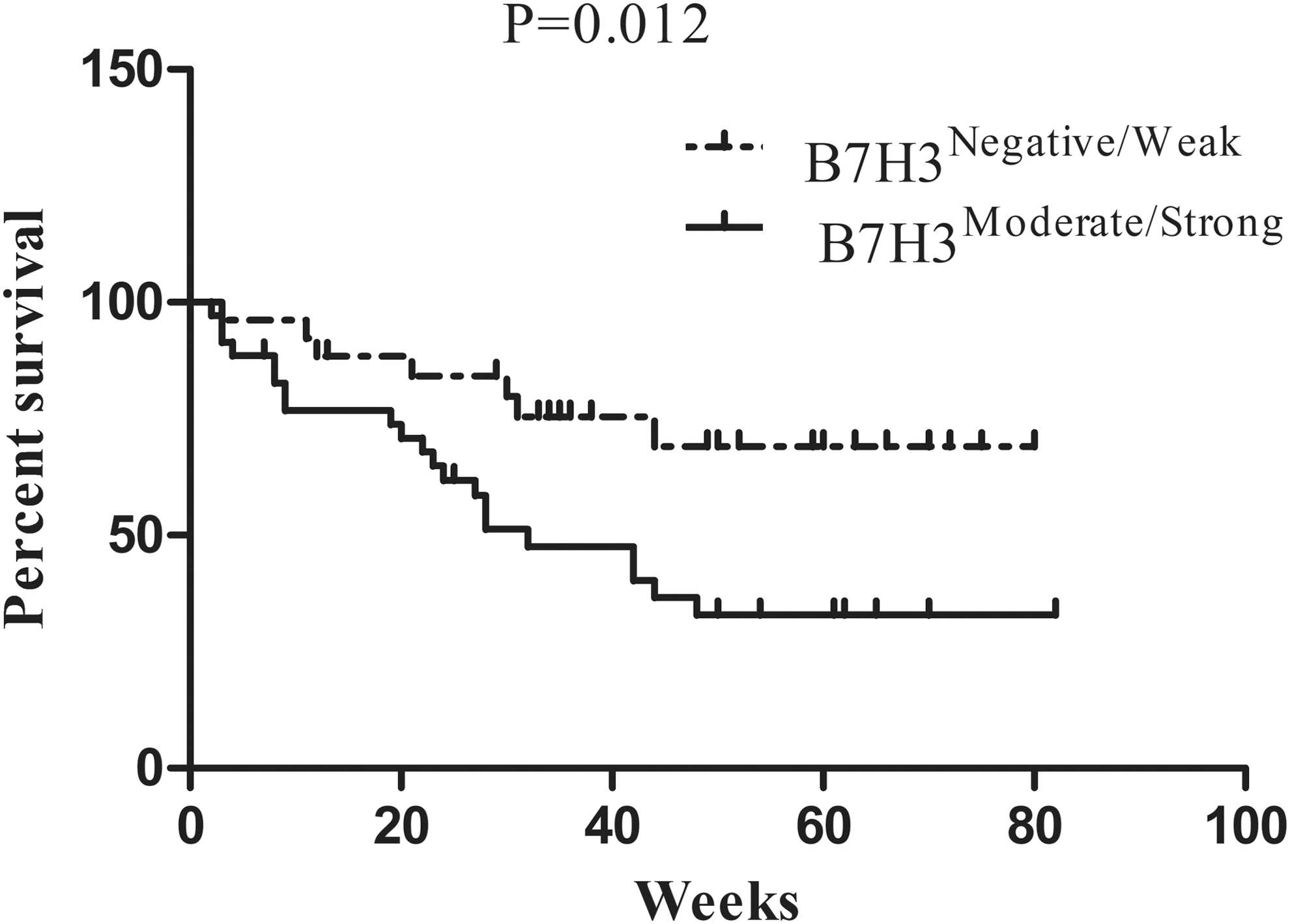
Kaplan–Meier curves of survival differences among HBV-HCC patients. High expression of B7-H3 was significantly associated with poorer survival in patients with HBV-HCC.
Univariable and Multivariable Analyses of the Effect of B7-H3 Expression on Survival
Univariate analysis was performed using the Kaplan–Meier method (log-rank test). Multivariate analysis was performed using the Cox multivariate proportional hazards regression model in a stepwise manner (Forward: LR).
CI, confidence interval; HR, hazard ratio; Pathological N factor, describe the status of lymph node metastasis; Pathological T factor, describe the size of a primary tumor.
Discussion
The inefficient eradication of HBV results in the recruitment of nonspecifically activated T cells, which is the main cause of liver damage after HBV infection (3, 8). B7-H3 plays an essential role in infection immunity and antitumor immunity. Our previous study showed that B7-H3 expression on CD14+ monocytes, CD4+ CD25high Treg cells, and sB7-H3 in peripheral blood was significantly increased in AHB, CHB, HBV-LC, and HBV-HCC patients, suggesting that dynamic B7-H3 expression has an important role in HBV infection.
To further explore the clinical significance of B7-H3's dynamic expression over the course of HBV infection, we systematically investigated the expression pattern of B7-H3 and its correlation between the frequency of T lymphocyte subsets and clinical parameters at different stages of HBV infection.
Our results showed that the presence of sB7-H3 in peripheral blood was positively correlated with the frequency of CD4+ CD25high Treg cells in almost all stages after HBV infection, and CD8+ T cell level decreased and CD4+ CD25high Treg cell level increased as the HBV infection-related disease progressed. Combined with our previous findings that sB7-H3 also increased as HBV infection-related disease progresses, we got the conclusion that sB7-H3 was related with the downregulated immune response during HBV infection. Upon analyzing the expression pattern of B7-H3 in peripheral blood, the results showed that sB7-H3 was negatively correlated with mB7-H3 expression in CD14+ monocytes and CD4+ CD25high T cells in AHB, but positively correlated with CHB. SB7-H3 had no correlation with mB7-H3 expressed on CD14+ monocytes and CD4+ CD25high Treg cells, but has positive correlation with AFP and later TNM stage in HBV-HCC. These suggested that the main sources of sB7-H3 may be different due to different liver damage degree at different disease stages and the feedback regulation between sB7-H3 and mB7-H3. This speculation still needs further study. B7-H3 was correlated with liver damage in CHB, since sB7-H3 and mB7-H3 expression on monocytes and Treg cells were positively correlated with the ALT and AST. Furthermore, higher mB7-H3 expressed on hepatocytes was associated with greater tumor size, later TNM stage, and worse prognosis in HBV-HCC.
Conclusions
Taken the above results together, B7-H3 triggers inhibitory signals in effector T cells and is closely associated with the progression of HBV infection as well as poor overall outcomes. Hence, B7-H3 could be considered a potent clinical indicator of the progression of HBV infection and a potential target for therapeutic strategies against HBV infection.
Footnotes
Acknowledgments
This work was supported by the Science and Technology Development Foundation of Nanjing Medical University (Grant No. 2016NJMU145); the Science and Technology Plan of Suzhou, China (Grant Nos. SYS201369 and SS201657); and the Health Plan of Jiangsu, China (Grant Nos. H201652 and H2017068).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.