
Abstract
Hepatitis E virus (HEV) is a common cause of acute hepatitis infections. Our previous 3-year study at two large Thai hospitals established an occurrence of 4–5% of HEV infections from swine HEV genotype 3 in suspected acute hepatitis patients, with the high incidence in older adults. This study was a serosurvey to determine the prevalence of HEV infections among Thai adults. We obtained sera from 630 healthy blood donors with a median age of 38 (18–64) years who attended Thai Red Cross transfusion units throughout Thailand. The donors were domiciled in 16 provinces in the northern (n = 159), central (n = 193), northeastern (n = 158), and southern (n = 120) regions. The seroprevalence of IgG antibody to HEV (anti-HEV) was determined by the EUROIMMUN test kit, using indirect enzyme-linked immunosorbent assay (ELISA) based on recombinant antigens derived from ORF2 of HEV genotypes 1 and 3. Demographic data, including information related to HEV infection risk (the number of pigs and the proportion of Muslims in each province), were also obtained. The overall anti-HEV prevalence among Thai adults was 29.7%. The frequencies of anti-HEV found in the northern (28.9%, 95% confidence interval [CI] = 22.4–36.4), northeastern (34.8%, 95% CI = 27.8–42.5), and central (35.8%, 95% CI = 29.3–42.7) regions were similar, whereas the frequency in the southern (14.2%, 95% CI = 9.0–21.5) region, known to have a large Muslim population, was low. An increasing frequency of the specific antibody was observed among the elderly. A low HEV infection rate was associated with an Islamic population where there are low number of pigs and low swine consumption. Furthermore, the higher anti-HEV incidences in the northeastern provinces might relate to the local cultural practice of consuming undercooked pork. Besides the need for an HEV vaccination in the future, there is a requirement for rapid early diagnosis; the undertaking of prevention–management campaigns might also reduce the number of infected patients.
Introduction
Hepatitis E virus (HEV) is one of the etiological agents causing enterically transmitted hepatitis (3,11,19). HEV is a positive-sense single-stranded RNA virus that belongs to the Hepeviridae family and the Orthohepevirus genus.
There are four genotypes (G1–4) for most infections in humans; G1 and G2 are mainly found in developing countries and infect only humans, whereas G3 and G4 are mainly present in developed countries and infect both humans and animals.
An HEV infection is mainly asymptomatic, but it can cause acute viral hepatitis, whose clinical signs are similar to those of the other viral hepatitis. It can also cause chronic infection, especially in immunocompromised and immunodeficient patients, such as HIV-infected and organ-transplant patients (7,11,12,17). The mortality rate is as low as 1–2%; however, patients with fulminant hepatitis from an HEV infection during pregnancy have been reported to have high mortality rates (20–25%), especially in India (10).
HEV infections usually occur by the fecal–oral route after the consumption of contaminated food or water. Additional routes of HEV transmission that have been proposed are blood-borne, human-to-human, and vertical transmission (from mother to child) (1,16).
A high prevalence of anti-HEV, including the presence of HEV genome closely related to humans, has been found in domestic and wild pig populations, suggesting that pigs are also an HEV reservoir and transmit the virus to humans (zoonosis) (15,19). HEV is diagnosed by the detection of anti-HEV IgM and IgG antibodies in serum. The analysis of HEV RNA in sera and stools is also employed (7,16).
In Thailand, the seroprevalence of anti-HEV IgG has been reported as ranging from 7–37% in several population groups such as Thai troops, pregnant women, children, the Hmong (a hill tribe ethnic group), and healthy people who have been directly exposed or not exposed to pigs (6,14,21,22). In our previous report, hepatitis E was found to have caused ∼4–5% of acute HEV infections at two large Bangkok hospitals during 2008–2011 (24). As well, that study identified that acute hepatitis E occurred more frequently among older adults than among young individuals. Therefore, it is of interest to serosurvey the prevalence of HEV infections among adults in the Thai population.
Materials and Methods
Study population
As part of a nationwide survey on anti-HEV, a total of 630 samples from blood donors in 16 provinces with ∼40 samples in each province were obtained as follows: northern provinces, n = 159 (Chiang Mai, Lampang, Nakhon Sawan, and Phitsanulok); central provinces, n = 193 (Bangkok, Chonburi, Lopburi, Prachuap Khiri Khan, and Ratchaburi); northeastern provinces, n = 158 (Khon Kaen, Nakhon Phanom, Nong Khai, and Ubon Ratchathani); and southern provinces, n = 120 (Krabi, Pattani and Songkhla). A detailed breakdown is given in Table 1. These archived sera samples were from part of a substudy of the serosurveillance of immunity to diphtheria, pertussis, and tetanus that was conducted in Thailand in 2013. The samples were obtained from 30–40 donors in each province who were aged 18–64 years and had participated in the regional Thai Red Cross blood transfusion service. All of the samples were stored at −20°C until use. This study was approved by the Ethics Committee for Research in Humans, Faculty of Medicine, Siriraj Hospital (IRB No. 762/2558).
Seroprevalence and Geometric Mean Titer of Hepatitis E Virus IgG in Thai Donors from Distinct Geographic Regions of Thailand
BK, Bangkok; CB, Chonburi; CI, confidence interval; CM, Chiang Mai; GMT, geometric mean titer; HEV, hepatitis E virus; KB, Krabi; KK, Khon Kaen; LB, Lopburi; LP, Lampang; NK, Nong Kai; NP, Nakhon Phanom; NS, Nakhon Sawan; PC, Prachuap Khiri Khan; PL, Phitsanulok; PT, Pattani; RB, Ratchaburi; SK, Songkhla; UB, Ubon Ratchathani.
Serological assay
IgG antibody against HEV (anti-HEV) in serum was performed by using the indirect HEV ELISA kit (EUROIMMUN, Lübeck, Germany) based on recombinant target antigens derived from ORF2 of HEV genotypes 1 and 3 (26). The method was performed in accordance with the manufacturer's instructions. In brief, diluted sera (100 μL, 1:101 dilution), as well as positive and negative controls and three calibrators for standard curve (100 μL), were incubated with the target antigens on a microtiter plate at room temperature for 30 min. After performing a washing step, antihuman IgG antibodies conjugated with peroxidase enzyme were added to the plates and incubated at room temperature. A second washing step was then performed, and a TMB/H2O2 substrate solution was added and incubated. Once the stop solution was added, the color intensity was measured at the wavelength of 450/630 nm. The anti-HEV result was determined qualitatively or semiquantitatively, as recommended by the test kit. The qualitative result was determined for the prevalence of HEV Ab in the seroepidemiology. A ratio value of ≥1.1 over the index (serum sample over the extinction value of calibrator) was interpreted as positive, <0.8 was considered as negative, and the ratio value between 0.8 and <1.1 was borderline. The semiquantitative result value may be regarded as the level (international unit [IU]) of immunity status of HEV Ab, which was obtained from the calibration curve of three calibrators within the linear graph. A result of ≥2.2 IU/mL was interpreted as positive, <1.6 IU/mL was considered as negative, and between 1.6 and <2.2 IU/mL was borderline. Repeated borderline results in duplicate were classified as antibody negative.
Demographic data and data analysis
Demographic data on the gender and age group of the subjects were recorded. Based on previous reports in this study area, swine should be considered as a possible source of HEV infection, and HEV infection through the consumption of contaminated pork might be one of HEV risk factors (21 –24). Therefore, information related to the risk of HEV infection (namely, nonpork consumption, such as in a Muslim population; and the number of pigs in each province) was also included. The data were obtained from the website of the National Statistical Office and the Information and the Communication Technology Center*. The anti-HEV results are presented as frequency (%), geometric mean titer (GMT), and 95% confidence intervals (95% CIs). The chi-square test was used to compare the prevalence of anti-HEV in each geographic region and age group, utilizing PASW Statistics 18 (SPSS, Inc., Chicago, IL). A p-value of <0.05 was considered a statistically significant difference.
Results
The total of 630 healthy adult subjects comprised 359 males and 271 females. The subjects were classified into five groups based on age range: 18–19 (n = 37), 20–30 (n = 192), 31–40 (n = 100), 41–50 (n = 221), and 51–64 (n = 80) years. The median age was 38 years (range: 18–64 years). Overall, the anti-HEV incidence among Thais based on the EUROIMMUN test kit was 29.7% (95% CI = 26.2–33.4). The level of anti-HEV (GMT) among the positive result was 4.67, whereas the negative result was 0.72 (data not shown). The prevalence of anti-HEV from the northern (28.9%, GMT = 1.3), central (35.8%, GMT 1.4), and northeastern (34.8%, GMT = 1.5) regions was similar (Fig. 1 and Table 1). The lowest anti-HEV prevalence was found in southern Thailand (14.2%, GMT = 0.75), where there is a large Muslim population, as illustrated in Figure 2. In addition, the frequency of anti-HEV was not correlated with a high number of pigs, as demonstrated by Chonburi and Ratchaburi provinces. The nadir of HEV IgG was observed in the southern part of Thailand in Songkhla province (7.5%), and the prevalence of anti-HEV in both Songkhla and Pattnani provinces were statistically significant to 6–10 provinces in this study (p < 0.01 or <0.05, chi-square) as given in Table 2. As detailed in Table 3, the incidence of the anti-HEV was slightly higher in older adults than in younger adults. The prevalence of anti-HEV increased, with a significant difference (p = 0.042, chi-square), from adults aged ≤40 years (prevalence = 26.1%, GMT = 1.05) to those aged >40 years (prevalence = 33.6%, GMT = 1.51).
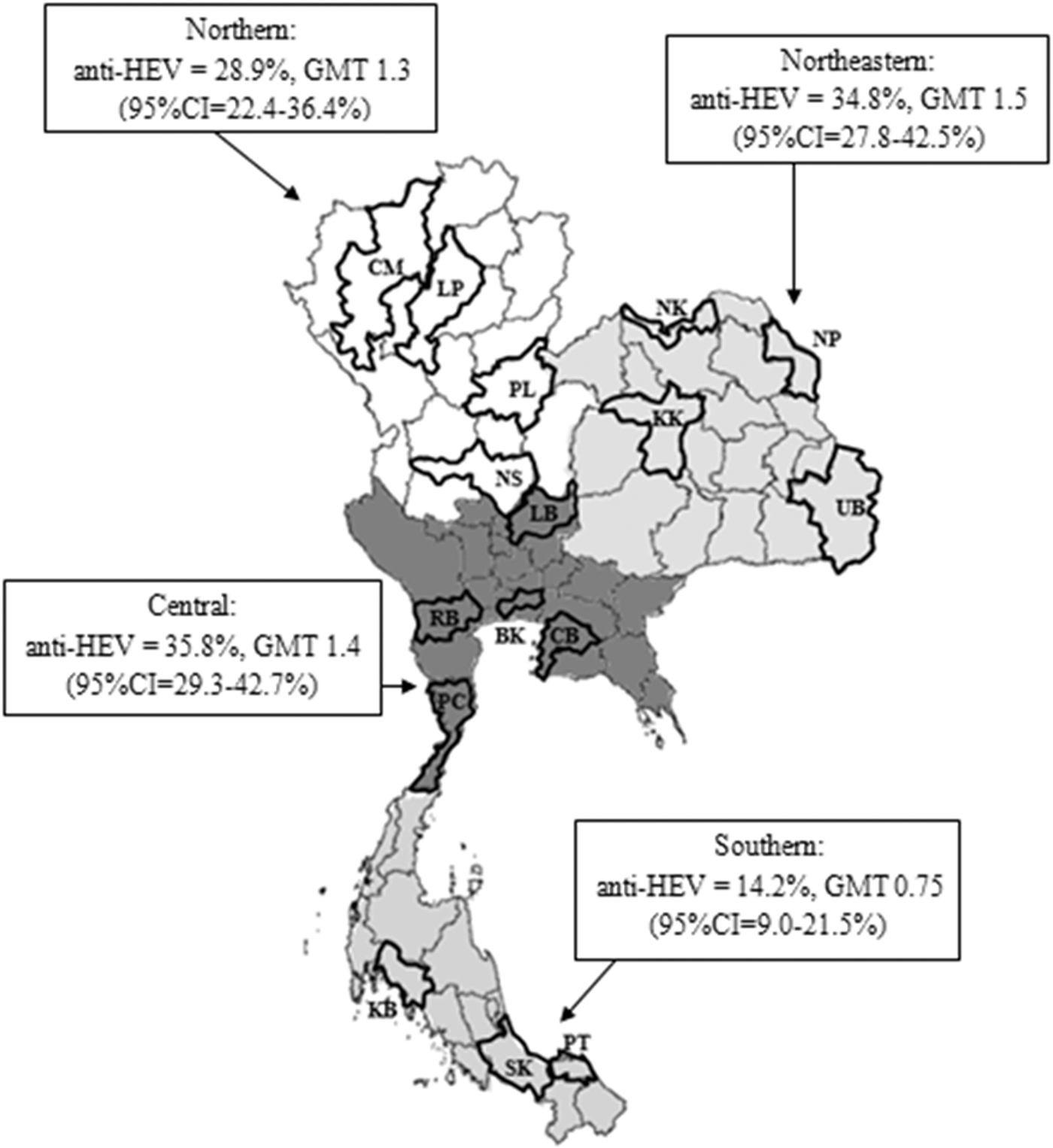
Prevalence of anti-HEV among Thai donors from distinct geographic regions of Thailand. BK, Bangkok; CB, Chonburi; CI, confidence interval; CM, Chiang Mai; GMT, geometric mean titer; HEV, hepatitis E virus; KB, Krabi; KK, Khon Kaen; LB, Lopburi; LP, Lampang; NK, Nong Kai; NP, Nakhon Phanom; NS, Nakhon Sawan; PC, Prachuap Khiri Khan; PL, Phitsanulok; PT, Pattani; RB, Ratchaburi; SK, Songkhla; UB, Ubon Ratchathani.

Prevalence of anti-HEV among Thai adults including the Muslim population and the number of pigs in each province as shown by percentage. Ab, antibody.
p-Value of the Significant Differences in the Prevalence of Anti-Hepatitis E Virus Between the Different Provinces
Significant difference (* p < 0.01 or ** p < 0.05, chi-square test).
NS, nonsignificant difference.
Immunity to Hepatitis E Virus (Anti-Hepatitis E Virus), by Age Group
Discussion
Results of anti-HEV seroprevalences have been known to vary, depending on the sensitivity and specificity of the assays (2,4,18). No method is available to confirm the actual result of anti-HEV IgG. Only the history of exposure to HEV or the presence of HEV genome/anti-HEV IgM markers in blood would be extra evidence of HEV infection. The prevalence of anti-HEV IgG determined by the EUROIMMUN test kit, based on recombinant Ag derived from HEV genotypes 1 and 3, with a limit of detection of 0.1 IU/mL in this study was 29.7%, which was similar to what was previously reported by earlier studies conducted between 2007 and 2014 in Thailand (5,23).
The presence of HEV in pigs was first detected in the United States in 1997 (15). Domestic pigs have since been recognized as a major reservoir for HEV transmission to humans in many countries, including Thailand (8,13,19,25,26). Pigs infected with HEV have no symptoms and can release vast quantities of the virus in their stools. In the case of Thailand, it was previously reported that the prevalence of anti-HEV in swine from pig farms in the Nakhon Pathom and Ratchaburi provinces was 64.7%, with the presence of HEV RNA found at 7.7% (25). Subsequently, HEV infections were identified in Thai patients with acute viral hepatitis, and the HEV sequence was closely related to swine HEV (13,24,26). All Thai-swine HEV strains belonged to HEV genotype 3. Interestingly, the high-risk group for acute HEV infection identified in our previous study was elderly patients (24). In addition, several reports in Thailand have suggested that zoonotic HEV might be associated with pork contact and consumption (13,23,25,26).
In this study, the lowest regional prevalence (14.2%) as well as the lowest anti-HEV level among Thai adults (GMT 0.75 IU/mL) was observed in southern Thailand, which is known to have a small swine population as well as a high population of Muslims, who do not consume pork. This pattern of seroprevalence result was similar to that previously reported in Thailand (5,23). Given that the human HEV infection has been determined to be closely related to the swine HEV genotype 3 in Thailand, the findings of this study support the association of HEV transmission with pork consumption in this country (13,24,25,26). Interestingly, the low anti-HEV level (GMT = 0.75) in the southern region might support the low risk of exposure to HEV infection. An earlier study, based on an HEV seroprevalence survey, found that the burden of HEV infection varies among occupational groups that were at high risk of being exposed to pigs (24.5–27.9%) compared with government officers (16.7%) (22). However, this study demonstrated that the anti-HEV prevalence in those central Thailand provinces with large swine populations (Ratchaburi, anti-HEV 29.4%; and Chonburi, anti-HEV 32.5%) was lower than anti-HEV prevalence in the northeastern Thailand provinces with small swine populations (Nakhon Phanom, anti-HEV 47.5%; and Ubon Ratchathani, anti-HEV 47.5%). The reason why there are large number of pigs in central Thailand yet lower anti-HEV adult prevalence might be excellent swine management at the majority of the region's commercial piggeries. Furthermore, the higher anti-HEV incidences in the northeastern provinces might relate to the local cultural practice of consuming undercooked pork. From one previous study, a large outbreak of HEV infection, which was associated with poor hygiene through exposure to contaminated drinking water or food, occurred in the northeastern part of Thailand (20). Therefore, poor hygiene might be an HEV risk factor in that geographic area.
Based on the overall frequency of HEV IgG (29.7%) among Thai donors in this study, HEV infections are more common in Thailand than previously recognized. The finding suggests that people will increase the risk of exposure to HEV infections through their lifetime. The existence of high anti-HEV in the elderly population might reflect previous exposure to HEV with either a clinical or subclinical infection. Sporadic cases of HEV infection have been reported, occurring in at least 5% of suspected acute viral hepatitis patients (24). Both acute HEV infections and persistent chronic infections have been reported in immunocompromised patients, mostly in those with solid organ transplantations (12). Moreover, in our preliminary study, we also found the phenomenon of chronic HEV in renal transplant patients (personal communication).
In summary, HEV infection could be recognized in Thailand. To date, all HEV isolates have been closely related to the swine strain. The zoonotic transmission occurs through the consumption of undercooked HEV-contaminated meat, direct contact with infected animals, and exposure to a contaminated environment. Besides the need for an HEV vaccination in the future, there is a requirement for rapid early diagnosis; the undertaking of prevention–management campaigns might also reduce the number of infected patients. Recently, the presence of HEV RNA could be determined in Thai blood supply (9). Thus,
Footnotes
Acknowledgments
We express our sincere thanks to all of the donors in this study. Special thanks go to Ms. Benjawan Klaythong from Internal Medicine, Faculty of Medicine, Siriraj Hospital, for administration management. We greatly thank Dr. Kobporn Boonnak from the Faculty of Tropical Medicine, Mahidol University, for reviewing the article. This study was supported by the Thai Association for the Study of the Liver Research Development Fund.
Author Disclosure Statement
No competing financial interests exist.