
Abstract
Hepatitis B surface antigen (HBsAg) loss and/or seroconversion is the ideal endpoint for the treatment of patients with chronic hepatitis B (CHB), whereas the “functional cure” of hepatitis B virus (HBV) infection is hard to obtain with routine therapeutics. Thus, potential new strategies are explored to cure HBV infection. A combination immunomodulatory therapeutic regime was used in a 43-year-old female patient with hepatitis B e antigen (HBeAg)-negative CHB; the regimen included consecutive combination therapy with recombinant human granulocyte–macrophage colony-stimulating factor (rhGM-CSF) plus HBV vaccine, in addition to ongoing normal interferon (IFN)-α2b treatment. The serum levels of alanine aminotransferase (ALT), HBV DNA, HBsAg, and hepatitis B surface antibody (HBsAb) were monitored every 6 months. The ALT level normalized and HBV DNA decreased to a level below the limit of detection within 3 months after the initiation of IFN-α2b therapy. After an entire year of IFN treatment, serum HBsAg decreased to a very low level (3.16 IU/mL), and HBsAb was still negative (0.78 mIU/mL). Then, rhGM-CSF and the HBV vaccine were applied, in addition to continuous IFN therapy. A steady decline in HBsAg was observed, and HBsAg loss with HBsAb seroconversion was achieved 12 months after initiation of the combination treatment with rhGM-CSF and HBV vaccine; the IFN-α2b was discontinued for the later 6 months. A therapeutic regimen with GM-CSF plus HBV vaccine could keep the immune system actively stimulated and trigger an HBV-specific immune response to control, or even clear the virus; this regimen may be helpful in the “cure” of HBV infection when combined with IFN-α.
Introduction
Chronic hepatitis B virus (HBV) infection accounts for the major causes of liver failure, liver cirrhosis, and hepatocellular carcinoma. Over 257 million people worldwide are chronically infected with HBV, of which >887,000 die of HBV-related liver failure, liver cirrhosis, and hepatocellular carcinoma every year (2,7). The prevalence of HBV infection in China has been well controlled through the national prophylaxis plan; however, 93 million people still have chronic HBV infection, 20 million of whom are patients with chronic hepatitis B (CHB) (3).
Interferon (IFN)-α or pegylated IFN-α (PEG-IFN-α) and nucleos(t)ide analogues (NUCs) are currently available therapeutics for CHB (7). With both antiviral and immune modulation activities, IFN-α treatment can lead to hepatitis B surface antigen (HBsAg) loss and/or seroconversion, that is, “functional cure” of HBV infection, in a small number of patients (∼10%) (7). The effects of IFN-α may be confined to the HBV genotype and limited by the levels of HBsAg and hepatitis B e antigen (HBeAg), and the age of infection; therefore, only a minority of CHB patients are sensitive to and suitable for IFN-α treatment (5). NUCs are widely used for CHB treatment; they have a high performance in replication inhibition and a convenient oral dosage (7). Although it is hard to clear HBsAg by NUC monotherapy, and although long-term treatment with NUCs may decrease serum HBsAg and even lead to HBsAg loss and/or seroconversion, most patients receiving NUC treatment have to take NUCs for a very long duration, potentially even for life. After the discontinuation of NUC treatment, even in those who have satisfied all the standard criteria for treatment stop, virological rebound will occur in more than half of patients, which may lead to liver injury and even liver failure in some patients (8). Thus, an ideal endpoint for CHB treatment is characterized by seroclearance of HBV DNA and HBsAg, with/without HBsAb seroconversion (6).
Methods
Subject
A 43-year-old female farmer was diagnosed with CHB in 2006 after a routine physical examination. The patient was positive for HBsAg, HBeAg, and hepatitis B core antibodies; she had an elevated alanine aminotransferase (ALT) (84 U/L) and HBV DNA of 4.53 × 107 IU/mL; her serum total bilirubin (TBiL) and liver ultrasonic examination were normal. A mother-to-child transmission of HBV was excluded since the parents are both negative for HBV. The exact route of HBV infection was unclear because her husband and children were also negative on HBV testing. Her ALT normalized a month after oral liver protectants without antiviral treatment. No abnormal findings were observed on yearly liver function tests and ultrasonic examinations from 2007 to 2014, and interestingly, spontaneous HBeAg seroconversion occurred in 2013, although the HBV DNA level was still 4.53 × 104 IU/mL at that time. On August 8, 2015, an elevated ALT of 128 U/L was found, with an HBV DNA level of 4.53 × 105 IU/mL, and the patient had a normal serum TBiL and liver ultrasonic examination.
Therapeutic regime
IFN-α2b (Harbin Pharmaceutical Group Holding Co., China) was the primary treatment, with a dose of 5 MU injected intramuscularly every other day after daily use for half a month. One year after the initiation of IFN-α treatment, consecutive combinations with recombinant human granulocyte–macrophage colony-stimulating factor (rhGM-CSF) plus HBV vaccine were added to the ongoing IFN-α treatment; the monthly procedure was three successive daily applications of 150 μg of rhGM-CSF (Harbin Pharmaceutical Group Holding Co.) by subcutaneous injection followed by a 20 μg of HBV vaccine (Shenzhen Kangtai Biological products Co., China) intramuscular injection in the deltoideus triangularis on the 4th day. The combination treatment lasted for 2 years with discontinuation of IFN-α during the last 6 months. The study protocol was approved by the ethics committee of Taihe Hospital. Written informed consent was given by the patient.
Data collection
All parameters, including TBiL, ALT, HBV DNA, HBsAg, and HBsAb, were measured by the Department of Laboratory Tests at Taihe Hospital, Hubei University of Medicine. All data were retrieved from the electronic medical records system of Taihe Hospital.
Results
From September 9, 2015, on, the patient received IFN-α2b therapy. The ALT level normalized and the HBV DNA decreased to a level below the limit of detection within 3 months. The white blood cells were decreased by IFN-α2b and fluctuated ∼2.4–3.1 × 109/L, even with the use of granulocyte colony-stimulating factor. The indexes of renal and thyroid function remained normal throughout the duration of IFN treatment. Except for neutropenia and an initial influenza-like illness, the IFN-associated side effects, including fatigue, anorexia, weight loss, and a mild increase in hair loss, persisted throughout the duration of the IFN treatment; additionally, anxiety that would have been insufferable without psychological care occurred 12 months after the initiation of IFN treatment.
After 12 months of IFN treatment, quantitation of HBsAg and HBsAb showed that HBsAg decreased to a very low level (3.16 IU/mL) and HBsAb was still negative (0.78 mIU/mL). Then, combination therapy with rhGM-CSF and HBV vaccine was applied. As a result, a steady decline in HBsAg was observed, and HBsAg decreased to 0.79 IU/mL 6 months after the combination treatment. At that time, IFN-α had been used for 1.5 years, and rhGM-CSF plus HBV vaccine therapy has been used for 6 months. The treatment with rhGM-CSF plus HBV vaccine was continued, while IFN-α was discontinued. Interestingly, the HBsAg continued to decline and decreased to a level <0.05 IU/mL (0.03 IU/mL); simultaneously, the level of HBsAb started to rise and increased to a level >10 mIU/mL (38.25 mIU/mL) 23 months after the initiation of IFN treatment, thus the goal of HBsAg seroconversion was attained (Fig. 1). All treatments were stopped thereafter, and the levels of HBsAg and HBsAb were monitored.
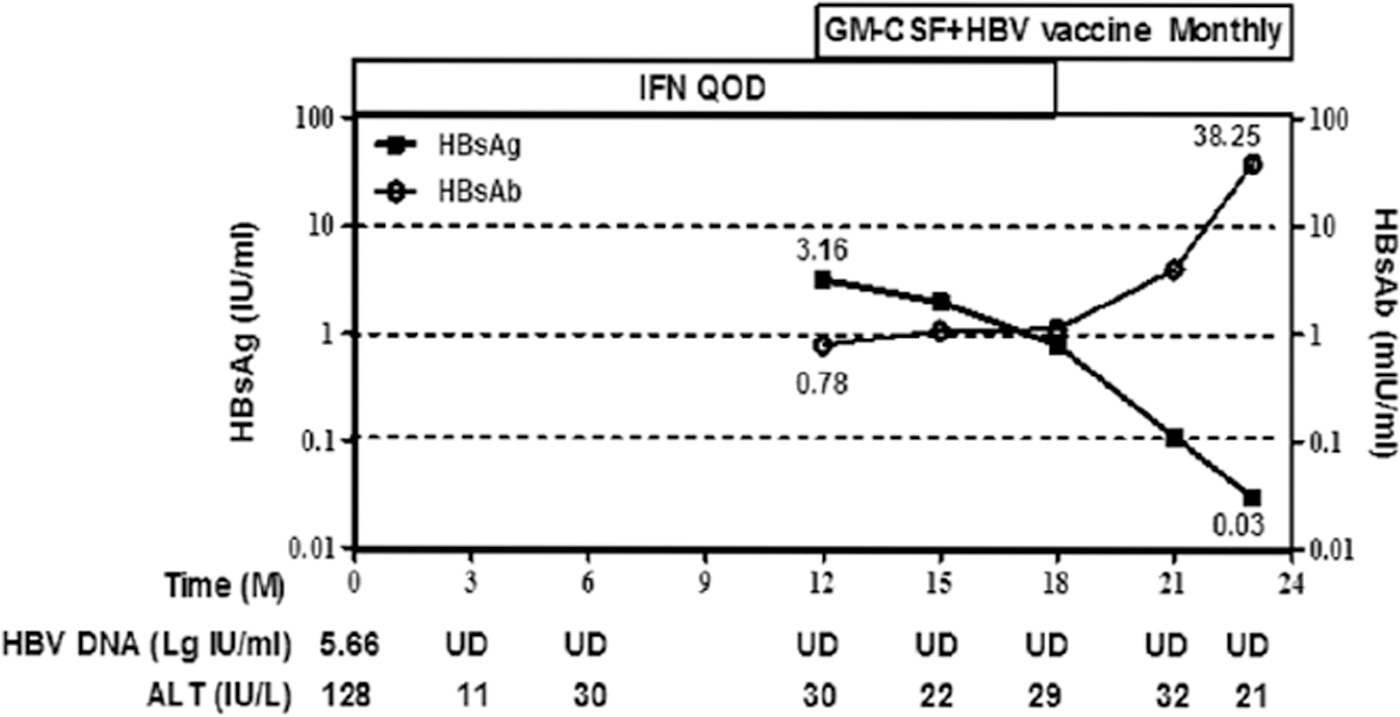
The kinetics of HBsAg, HBsAb, HBV DNA, and ALT during the treatment period. HBV DNA levels are indicated as Lg IU/mL. ALT, alanine aminotransferase; HBsAb, hepatitis B surface antibody; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; UD, under the detection limit.
Discussion
HBsAg loss and/or seroconversion is the ideal endpoint for CHB treatment. The effects of IFN-α have been validated for decades. The treatment usually lasts for 6 to 12 months, and a longer period may lead to a higher ratio of virological response (3,5). For this patient, serum HBsAg decreased to a level <10 IU/mL after normal IFN-α treatment for 12 months, which predicted a high probability of attaining the goal of HBsAg loss and/or seroconversion (5); thus, the period of IFN treatment was expanded.
GM-CSF, which can induce dendritic cell maturation and activation, is usually used as an adjuvant for therapeutic vaccine (4,9). In an HBV-transgenic mouse model, the 3 × GM-CSF plus HBV vaccine regimen triggered a potent HBV-specific T cell response and led to seroclearance of HBV DNA and HBsAg and the appearance of HBsAb (10).
In the current patient, when serum HBsAg decreased to a rather low level of 3.16 IU/mL after normal IFN-α treatment for 12 months, we applied 3 × GM-CSF plus HBV vaccine therapy combined with ongoing IFN-α treatment and tried to induce an HBV-specific T cell response for better immune control of HBV and even seroclearance of HBsAg and the appearance of HBsAb. As a result, the combination therapy did induce a steady decline of HBsAg, and finally serum HBsAg clearance was observed and accompanied by the appearance of protective HBsAg; with the later period of treatment with 3 × GM-CSF plus HBV vaccine after discontinuation of IFN-α, the goal of functional cure was achieved. This patient is still at risk for HBV reactivation, especially when immunosuppressive therapy is applied (1). Therefore, the patient was advised to receive further immunization with the HBV vaccine, continue monitoring of the HBsAb levels, and maintain awareness of antiviral treatment in case of immunosuppressive therapy.
The side effects of IFN-α hamper its application, usually leading to an incomplete period of treatment. Almost all the common side effects of IFN-α occurred in the current patient, and some persisted during the whole period of treatment, especially the onset of severe anxiety, which nearly forced the discontinuation of IFN-α therapy. With psychological counseling and humanistic care, the patient adhered to an 18-month period of IFN-α treatment. Even at that time, serum HBsAg remained positive (0.79 IU/mL), and may remain positive for a long time after treatment discontinuation; thus, reactivation of HBV may be induced when the immune system is impaired. An ideal end point was achieved with serum HBsAg clearance with consecutive treatment with 3 × GM-CSF plus HBV vaccine within 6 months after IFN-α discontinuation. Therefore, as it was without obvious side effects, 3 × GM-CSF plus HBV vaccine therapy may be a good choice in combination with IFN-α treatment for CHB patients, and the use of GM-CSF could antagonize the neutropenia induced by IFN-α. When IFN-α has been applied for 12–18 months and patients can no longer tolerate the side effects of IFN, consecutive treatment with 3 × GM-CSF plus HBV vaccine may be an alternative therapeutic regime to keep the immune system actively stimulated and trigger an HBV-specific immune response to control or even clear the virus.
High levels of ALT, lower levels of HBsAg and HBV DNA, genotype A or B, histological evidence of grade G2 or higher disease, and a significant decrease of HBsAg at weeks 12 and/or 24 after the start of IFN treatment may predict a good response to IFN-α treatment (2). Unfortunately, this patient lacked HBV genotyping and quantification of HBsAg before treatment initiation and before 12 months of IFN-α treatment. Although we had some clues, such as the fluctuation of ALT and the spontaneous HBeAg seroconversion 2 years before IFN treatment, indicating a certain level of immune response to HBV, this may be favorable for the combination treatment with IFN-α and 3 × GM-CSF plus HBV vaccine. In conclusion, immune modulatory therapy is effective in the case of ALT fluctuation and spontaneous HBeAg seroconversion. The monitoring of HBsAg levels and HBsAg responses will facilitate the outcome of patients with CHB, and combination therapy with 3 × GM-CSF plus HBV vaccine may be helpful in the way to a “cure” of HBV infection.
Footnotes
Acknowledgment
The authors thank Linli Chen for her excellent work conducting the liver ultrasonic examination.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was partly supported by the National Key Program for Infectious Disease of China (Grant No. 2013ZX10002-001) and Key Program for Precision Medicine of Taihe Hospital (Grant No. 2016JZ05).