
Abstract
Several hepatitis B virus (HBV) factors, including viral load, genotype, genome mutations, and cytokine production, have been reported to be associated with different risks of progression of liver disease. The aim of this study was to verify if there is an association among the levels of cytokines (interleukin [IL]-35, IL-6, IL-17A, interferon [IFN]-γ) in the plasma, viral load, and the different genotypes of HBV in patients with acute or chronic hepatitis B. Methods: 49 serum samples, 20 from acute and 29 from chronic cases, were submitted to a real-time and nested-polymerase chain reaction to quantify, detect, and genotype HBV DNA. The cytokines IL-35, IL-6, IL-17A, and IFN-γ were detected by an enzyme-linked immunosorbent assay (ELISA). The median viral load was 3.15 log10 IU DNA/mL and 2.90 log10 IU DNA/mL for acute and chronic patients, respectively. Genotype A, D, E, and F were identified in chronic carriers of HBV infection, while only genotype A and F were identified in individuals with acute infection. IFN-γ (p = 0.024) and IL-17A (p = 0.046) levels were significantly increased in chronic patients and IL-6 and IL-35 were higher in patients with acute infection, however, without statistical difference. IL-17A and IFN-γ can be modulating proinflammatory effects and inducing hepatocellular damage, in chronic patients, and IL-6 and IL-35 may be involved in viral elimination and protection against chronicity during the acute phase of infection. These results can contribute to understanding of the complex regulatory mechanisms of the host antiviral response related to cytokine production during acute and chronic HBV infection.
Introduction
Hepatitis B virus (HBV) affects 2 billion people worldwide (55). Of these, ∼257 million persons, or 3.5% of the world population have a chronic infection with a risk of developing advanced liver disease, cirrhosis, and/or hepatocellular carcinoma, which cause 500 to 700 thousand deaths per year in the world (28,55).
HBV belongs to the family Hepadnaviridae genus Orthohepadnavirus (23,34,50). Currently, HBV isolates are classified into 10 genotypes (A–J) and several subtypes, with a different geographic distribution (16,31,47). The genotypes A, D, and F are predominant in Brazil (27,37). Studies have shown that different genotypes and most of the subgenotypes have particular epidemiological and virological properties. In addition to the distinct geographical distribution, evidence suggests that genotypes are the result of HBV biology (58), determining the course of the disease (41), and affecting the response to antiviral therapy (46).
The disease caused by the HBV can result in asymptomatic infection, acute self-limiting hepatitis, chronic hepatitis, or fulminant hepatitis, which can lead to cirrhosis or hepatocellular carcinoma (HCC) and in more severe cases requires liver transplantation. The degree of complication of chronic infection is closely associated with viral replication rate (28).
Serologic markers can be used to diagnose and distinguish between acute and chronic infections. Commercially available serological tests are used to detect HBV surface antigen (HBsAg), envelope antigen (HBeAg), HBV surface antibody (anti-HBs), HBV core antibody (anti-HBc), antibody of the HBV envelope (anti-HBe), and HBV DNA. The acute phase of HBV infection is characterized by the presence of surface antigen (HBsAg) in the serum, followed by the appearance of anti-HBc and total anti-HBc IgM. HBeAg is indicative of viral replication and infectivity and appears at the end of the incubation period and disappears shortly before the onset of HBsAg in the development of the symptomatic phase. It is a marker related to the presence of the viral genome (1,18,48,52).
Approximately 5–10% of cases of infected adults and a significantly higher percentage of HBV-infected infants and children develop a chronic infection characterized by continuous detectable expression of HBsAg for at least 6 months after the initial infection (26).
Chronic HBV infection comprises five different phases, they are the following: (1) chronic HBeAg-positive infection with normal alanine aminotransferase (ALT) (former immunotolerant phase), (2) chronic HBeAg-positive hepatitis with elevated ALT (former immunoreactive phase), (3) chronic HBeAg-negative infection with normal ALT (or inactive carrier), (4) HBeAg-negative chronic hepatitis with elevated ALT, and (5) HBsAg-negative phase (or hidden infection) (13).
Approximately two-thirds of the patients who seroconvert HBeAg to anti-HBe undergo a period of “flare” or reactivation defined as the abrupt increase in ALT in patients with chronic HBV. Reactivations can occur spontaneously several times in the same individual and do not necessarily result in seroconversion and can occur in 10% of HBeAg negative patients (30,49).
The participation of adaptive immunity is essential for the viral elimination and termination of HBV infection. CD4+ T lymphocytes activate CD8+ T lymphocytes (CTL) and promote differentiation of B lymphocytes (LB) into plasma cells for the production of antibodies (6,35).
Cytokines represent a large family of molecules, including cytokines associated with Type 1 (Th1) T cell responses (e.g., interleukin-2 [IL-2], interferon [IFN-γ]), which have a functional contribution to immune responses; type 2 (Th2) T cell response (e.g., IL-4, IL-6, IL-10), which play a role in humoral immune responses; regulatory T cell-associated (Treg) cytokines with, for example, tumor growth factor beta (TGF-β) and IL-10, which are associated with immunomodulation and immunosuppression; and Type 17 T cell response (Th17) (e.g., IL-17, IL-22, IL-23), which play critical roles in mediating inflammation (22). Cytokines initiate downstream signaling pathway activities by binding to specific receptors expressed on target cells and play important roles in responses against viral infections (29).
As HBV is a noncytopathic virus, both HBV-related liver damage and viral control are immune-mediated. There is growing evidence that cytokine-mediated immune responses play an important role in determining clinical outcomes during HBV infection (5,10,57).
The aim of this study was to verify if there are associations among the levels of cytokines (IL-35, IL-6, IL-17A, IFN-γ) in the plasma, viral load, and the genotypes with acute or chronic hepatitis B.
Materials and Methods
Population studied
This study was approved by the FIOCRUZ Research Ethics Committee with number CAAE 06109812.4.0000.5248. All patients in the study were aware of and according to their participation in the research, after signing the informed consent form, according to resolution number 466, of December 12, 2012 of the National Health Council—Ministry of Health of Brazil. Individuals coinfected with HIV and hepatitis, A, C, and E were excluded from the study. Socioepidemiological data, information about infection, HBV treatment, and risk behaviors were obtained from each patient record or from the questionnaire.
This study was a retrospective one, and the collection of samples was carried out between 2014 and 2017. A total of 49 individuals from National Reference Laboratory for Viral Hepatitis were included. This clinic serves as the National Reference Centre for Hepatitis Viruses in Brazil and receives persons suspected of having viral hepatitis, including acute and chronic cases and their contacts. The patients were divided in two different groups of infection: (1) 20 serum samples from acute hepatitis B patients and (2) 29 serum samples from chronic hepatitis B patients (without antiviral therapy). The inclusion criteria for the acute patients were the presence of HBsAg less than 6 months, anti-HBc IgM, HBeAg, and detection of HBV DNA and for the chronic patients, detection of HBsAg more than 6 months.
Sample collection
Peripheral blood samples were collected (5 mL) from each individual in a vacutainer tube (Becton Dickinson and Company, Franklin Lakes) containing sodium heparin (20 mL) to obtain plasma. After centrifugation, the plasma was separated and stored at −70°.
Biochemical tests
Serum samples were subjected to biochemical doses of liver enzymes, such as aspartate aminotransferase; ALT; alkaline phosphatase; total, direct, and indirect bilirubin; and gamma-glutamyl transferase through a system of quantitative determination by photometry in kinetic mode using a commercial kit (LabMax 560; LabTest, Minas Gerais, Brazil) according to the manufacturer's instructions.
Detection of HBV serological markers in serum samples
To include the patients in the study, all samples were tested through enzyme immunoassays (EIA) for HBsAg (BioElisa HBsAg 3.0; BioKIT, Barcelona, Spain), anti-HBc IgM (BioElisa anti-HBc; BioKIT), anti-HBc IgM (ETI CORE IgMK Plus; DiaSorin, Saluggia, Italy), HBeAg, and anti-HBe (e411 Cobas; Roche Diagnostics, Mannhein, Germany) according to the instructions from each manufacturer. Anti-HAV IgM (DiaSorin), anti-HCV (Murex anti-HCV 4.0; DiaSorin), anti-HEV (BioKit), and Anti-HIV (DS-EIA-HIV-AGAB-SCREEN, RPC, Diagnostic System, Berkshire, Russia) were used to exclusion screening.
Molecular assay and phylogenetic analysis
All samples positive to HBsAg were tested to HBV-DNA by nested polymerase chain reaction (PCR) and Abbott Real-Time HBV kit (Abbott Laboratories). Extraction of HBV genetic material was performed according to the commercial kit (High Pure Viral Nucleic Acid Kit; Roche Diagnostics) for plasma samples. The pre-S/S genome region was amplified using a seminested PCR assay (51).
Nested PCR products were loaded into a 1.5% agarose gel and stained with ethidium bromide to visualize the bands of an expected length of 1,200 bp. Amplicons obtained by nested PCR with an expected HBV size were purified using the High Pure PCR Product Purification Kit (Roche Diagnostics) according to the manufacturer's instructions. The sequence of the pre-S/S genes was determined from a single PCR fragment by using a BigDye Terminator Kit v3.1 (Applied Biosystems, Foster City, CA), and sequencing reactions were analyzed on an ABI3730xl automated sequencer (Applied Biosystems).
HBV genotyping was performed by phylogenetic analyses of the pre-S/S gene with HBV sequences representing all genotypes available in GenBank. Phylogenetic analysis was performed using the maximum likelihood method with the online version of the PhyML program (19). The reliability of the phylogenies was estimated with the approximate likelihood-ratio test (3) based on a Shimodaira-Hasegawa-like procedure (SH-aLRT). The GenBank accession numbers for the HBV sequences obtained in this study are MN845892-MN845928.
Detection of the cytokines IL-6, IL-17A, IFN-γ, and IL-35
Cytokines Human IL-6 (EUA, cat. DY206; R&D Systems, Minnesota), Human IL-17-A (cat. 900-M84; Peprotech, Cranbury), Human IFN-γ (cat. 900-K27; Peprotech, Cranbury), and Human IL-35 (Cat. E-EL-H2443; Elabscience, Wuhan, Hubei, China) were analyzed in the plasma of peripheral blood by Sandwich ELISA kits as the method in compliance with manufacturer's directions. Standard curves were prepared by serial dilutions of the aliquot corresponding to cytokine pattern supplied by the manufacturer. The determination of the optical density of samples and standards was performed using Expert® Plus spectrophotometer (Biochrom, Cambridge, UK).
Data analysis
Descriptive statistics of the qualitative variables was determined by frequency distribution and quantitative variables by medians and interquartile ranges and mean and standard deviation. Afterward, to analyze the association between the infection situation and personal and clinical characteristics, the Pearson chi-square test was used for categorical variables and Mann–Whitney U test (median) or Student's t-test (mean) for continuous variables, both at 95% confidence intervals and p-value ≤0.05. Correlation between cytokines and viral load was estimated by Spearman test (the data did not present a normal distribution), and values of p < 0.05 were considered as significant.
Results
Study population
In study population, 59.2% were males and the mean age was 45.59 ± 14.07 years, men being almost 7 years older than women. There was no statistically significant difference for age and viral load between patients with acute and chronic infection (Table 1).
Demographic, Epidemiological, Clinical, and Genotypic Characteristics of the Population
SD, standard deviation.
Among the patients with chronic hepatitis B infection, most of them were classified as inactive carriers (24/29), followed by patients with flare (3/29), chronic HBeAg-positive infection with normal ALT (1/29), and HBeAg-negative chronic hepatitis with elevated ALT (1/29).
HBV DNA detection in plasma and phylogenetic analysis
All HBV DNA was quantified by real time PCR, the median of the viral load for acute patients was 3.15 ± 2.46 log10 IU of HBV DNA/mL, and for chronic patients, it was 2.90 ± 2.47 log10 IU of HBV DNA/mL.
In 69.39% (34/49) of samples, it was possible to amplify by conventional PCR the complete gene from the Pre-SS region (1,200 bp). The isolates obtained were mostly of genotype A (28/34), 19 samples of subgenotype A1, and 09 samples of subgenotype A2. One sample was classified as genotype D (1/34) and one as genotype E (1/34). Four were classified as genotype F (4/34), subgenotype F1 (Table 1).
Regarding the distribution of genotypes, it was observed that 70.0% of the individuals with acute HBV infection belonged to genotype A and 10.0% to genotype F. The chronic profile was the one with the highest genotype diversity, 48.3% of the samples belong to genotype A, 3.4% to genotype D, 3.4% to genotype E, and 6.9% to genotype F. No correlation was found between virus genotypes and cytokine production.
Detection of the cytokines IL-6, IL-17A, INF-γ, and IL-35
The median levels of IFN-γ (p = 0.024) and IL-17A (p = 0.046) were statistically higher in chronic patients compared to acute patients (Table 2). The Figure 1 shows the median levels of IL-6 and IL-35 that were higher in acute patients when compared to the chronic group. The IL-17A and INF-γ showed p-value <0.005 when acute and chronic groups were compared.
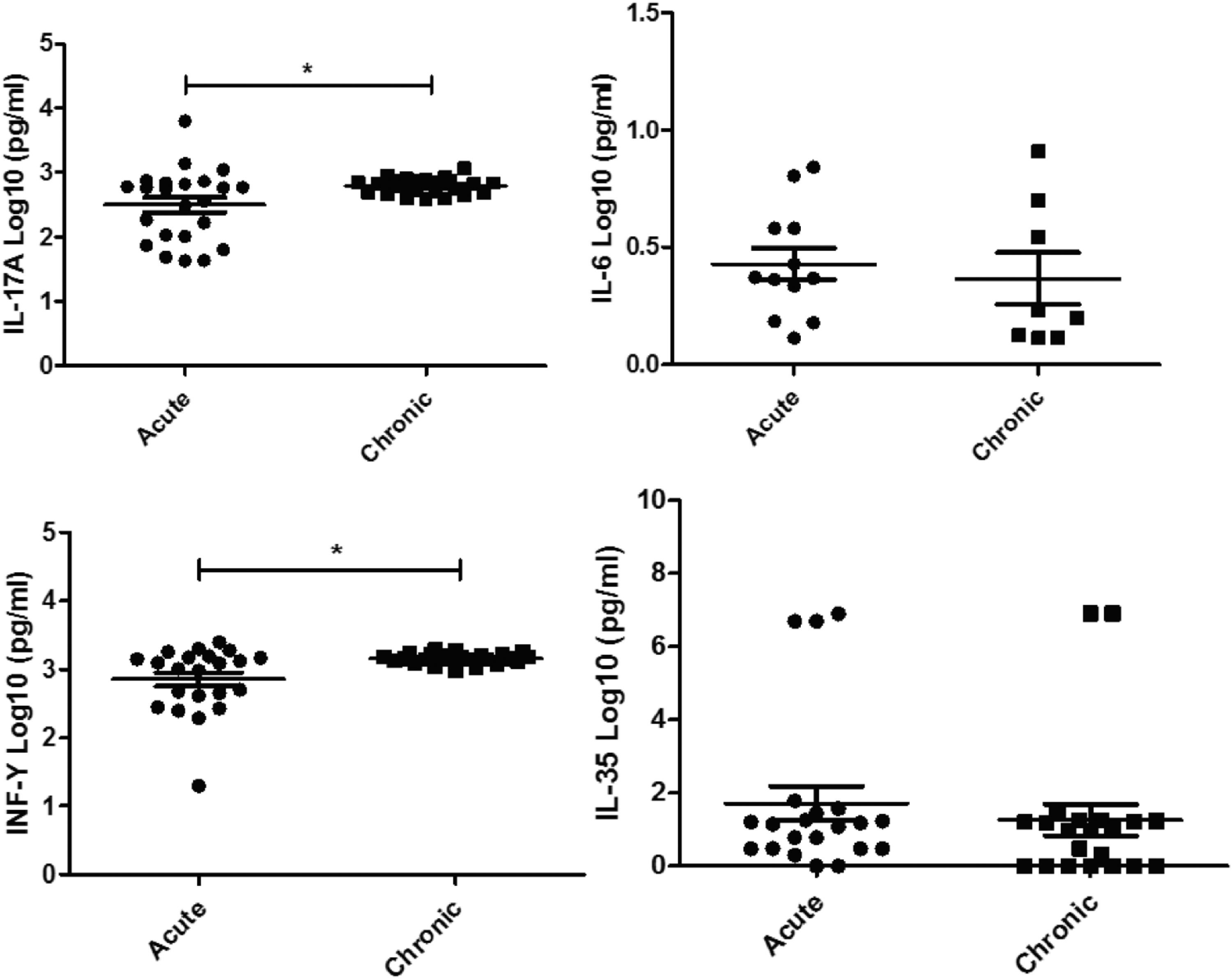
Comparison of cytokines found in acute and chronic patients by ELISA using the nonparametric Mann–Whitney test. *p < 0.05. ELISA, enzyme-linked immunosorbent assay; IL, interleukin.
Median Levels of Cytokines in Acute and Chronic Hepatitis B
IL, interleukin.
A negative correlation between viral load and IL-17A (p = 0.031) was observed through the Spearman correlation coefficient (Table 3 and Fig. 2).

Negative correlation between viral load and IL-17A through the Spearman correlation coefficient.
Correlation Between Viral Load and Cytokines by Rô de Spearman
Discussion
Hepatitis B has a wide spectrum of manifestations, ranging from an acute self-limiting disease with resolution for cure, until hepatitis chronic with progress to cirrhosis and HCC (36,39). Although a number of studies have demonstrated data about cytokines, viral load, or genotypes in patients with hepatitis B, few studies compared these data between acute and chronic hepatitis B infections. In this study, a comparison of the production of IL-35, IL-6, IL-17A, and IFN-γ between acute and chronic infection was performed, since it is already well documented in the literature that these cytokines are increased in individuals infected with HBV in relationship to healthy controls.
HBV DNA is an important marker, and all major international guidelines base their treatment decisions on the HBV DNA cutoff points, these treatment decisions based on HBV DNA have been shown to decrease the risk of liver decompensation, development of HCC, and death (17). However, the value of HBV DNA is limited, a study by Wang et al., (53) demonstrated intrahepatic replication despite the suppression of HBV DNA, and the negativity of HBV DNA does not mean a cure for HBV infection. A study published by Gao et al., (17) demonstrated that HBV DNA in patients with chronic hepatitis B is related to the level of intrahepatic cccDNA before treatment in HBeAg-positive patients. HBeAg reactive subjects generally have elevated HBV DNA viral load compared to HBeAg nonreactive subjects (20).
In our study, the median of the viral load for acute patients was 3.15 ± 2.46 log IU/mL, and for chronic patients, it was 2.90 ± 2.47 log IU/mL. These results are in agreement with the current literature that found HBV DNA viral loads within hepatitis B patients ranged from 1.13 to 8.42 log IU/mL and DNA viral load lower relative to the chronic samples; in acute HBV infection, the peak DNA levels were 5.53 and 9.23 log IU/mL (8). Nita et al., (38), analyzing a cohort of 564 chronic patients in Brazil, found a median of 2.35 log copies/mL of HBV DNA, and Sarkar et al. (40) demonstrated a median of viral load of 2.13 log copies/mL in acute patients and no significant variation of viral load among different HBV genotypes and subgenotypes. We also found no correlation between viral load and genotypes.
The criteria for assessing correlations in this study were the viral load of all patients in relationship to cytokine production, we found a significant negative correlation between viral load and IL-17A (p = 0.031) through Spearman's correlation coefficient.
As we know, HBV is a noncytopathic virus, both HBV-related liver damage and viral control are immunomediated (5) and IL-17 can directly mediate the inflammatory response in liver cells (56). Therefore, IL-17 could be mediating proinflammatory effects even with a decrease in viral load in individuals infected with HBV.
In this study, the isolates obtained were mostly of genotype A (30/37), 19 samples of subgenotype A1 (19/37), and 11 (11/37) samples of subgenotype A2. The genotype A1 has geographical distribution in Africa, Asia, and Brazil, the genotype A2 is most commonly found in Northern Europe and United States. One sample was identified as genotype D, the most prevalent genotype in Africa, Mediterranean region, and India; one sample was identified as genotype E, and this genotype is restricted to West Africa. Curiously, this sample was from an immigrant from Angola. Five samples were classified in the genotype F, subgenotype F1, and this genotype is found in Central and South America (25,47,50). Although, a high diversity of genotypes was found, no correlation was found between genotypes and cytokines.
There are clear differences in adaptive immunity in patients with chronic or resolved HBV infection. HBV-specific CD4+ and CD8+ T cell responses with a Th1 cytokine production profile are detectable in high blood titers of subjects with a favorable outcome. These Th1 cell responses along with cytotoxic responses are quantitatively stronger than those found in patients with chronic infections, which are, in contrast, characterized by weaker or undetectable virus-specific T cell responses (9,15,24,45).
Some factors inherent to the host can contribute to natural course of the infection. In this study, we found a higher prevalence of males and a higher average age among those who chronified than those with spontaneous resolution. Data from the literature confirm a three to sixfold increase in men's propensity for chronicity, hypothetically explained by the protective effect of estradiol, which induces the production of INF-γ, aiding in seroconversion to anti-HBs and anti-HBe in acute cases, in addition to its antioxidant effect, in the chronic phase, promoting a more benign course in premenopausal women (44).
Here, IL-35, IL-6, IL-17A, and IFN-γ were investigated, and these cytokines are well documented and have a great impact on the clinical outcomes associated with hepatitis B. However, this impact is still not well understood and some cytokines such as IL-6 and IL-35 have a controversial role in HBV infection, which may induce cirrhosis and HCC or eliminate HBV via inducing humoral and cellular immune response. Cytokines IFN-Y and IL-17A are well described in association with chronic hepatitis, cirrhosis, and HCC via combination with other proinflammatory cytokines.
In our study, the IL-17A was higher in chronic patients compared to the acute cases and showed a negative correlation between viral load and IL-17A. T helper 17 (Th17) cells are significantly raised in chronic HBV-infected patients. Th17 cells initiate immune-mediated pathogenesis and have an important role in the process of HBV-related liver cirrhosis (HBV-LC). The mechanisms underlying this process are associated to Th17-secreted cytokines, which include IL-17 (4). IL-17A is upregulated in HBV-mediated chronic inflammation and may be relevant for the development of liver cirrhosis and HCC (11,14,56). IL-17 can also significantly stimulate monocytes and DCs to express IL-17R and produce proinflammatory cytokines such as IL-1β, TNF-α, IL-6, and so on, which are important for liver damage during hepatitis B progression (59). In addition, IL-17 can directly mediate the inflammatory response in liver cells, and activation of the inflammatory response in liver tissue between hepatic stromal cells promoted abundant TGF-β1 expression, resulting in progression to hepatic fibrosis in hepatitis B chronic (56).
A previous study showed that IL-17A expression in the liver tissues of the patients was positively correlated with inflammation grade and fibrosis stage, and positively stained LB suggested that IL-17A drives part in chronic HBV infection (11). The highest IL-17A levels in the serum and liver were observed in LC patients, implying that IL-17A might participate in the pathogenesis and/or progression of liver fibrosis. A study by Elkhawaga et al., (12) showed that serum IL-17A levels were also significantly elevated in chronic patients with hepatitis C with advanced stages of fibrosis.
In our study, IFN-γ was higher in chronic patients compared to the acute ones. INF-γ is the only representative of the cytokine class of the INF type II and is produced by a big variety of cells, including NK cells, CD4+ LTh1, and CD8+ LT (2). This cytokine plays a crucial role in innate and adaptive immunity. For example, IFN-γ increases Type I IFN, inflammatory cytokines, and chemokines production, which leads to leukocyte recruitment to the sites of infection, and upregulates FasL expression in CTL (cytotoxic T lymphocytes) and MHC class II and costimulatory molecules on Antigen Presenting Cells (APC), which influences CD4+ T cell responses against pathogens. Also, IFN-γ induces IL-12 secretion, which, in turn, increases the cytotoxic activity of NK cells and drives CD4+ naive T cells differentiation to the Th1 profile. In this way, IFN-γ plays a pivotal role during viral infections (32).
IL-6 and IL-35 levels were higher in acute patients when compared to the chronic group, but without statistical difference. IL-6 is a pleiotropic cytokine with well-known beneficial impacts on the liver. It increases the liver regeneration and protects against an amount of liver-damaging influences such as alcohol and carbon tetrachloride intoxication. Some studies reported that HBV entry was inhibited by up to 90% when cells were pretreated with IL-6, resulting in a substantial reduction of cccDNA and HBsAg secretion; besides it, IL-6 inhibits HBV entry through the downregulation of the viral entry receptor NTCP (7) and has been demonstrated that IL-6 protects hepatocytes from T cell-mediated damage (21).
Curiously, our findings for IL-35 differ from a study, in which serum levels of IL-35 were significantly increased in the cirrhotic process (43) and regulated the functions of viral-specific Tregs and CD8+ T cells during chronic HBV infection, which might contribute to immunotolerance and viral persistence (33,42). However, a recent study showed that IL-35 play contradictory roles in controlling viral persistence and inhibiting inflammatory responses and have an immunosuppressive function in chronic hepatitis C virus (HCV) infection (33) and another study suggests that influenza A virus infection can induce IL-35 expression and IL-35 can activate the IFN pathway and may have a potential antiviral activity (54). These findings suggest that further studies are necessary for a better understanding of the complex regulatory mechanisms of the host antiviral response related to IL-35 during HBV infection.
Conclusions
IL-17A and IFN-γ, higher in chronic patients, can be modulating proinflammatory effects and inducing hepatocellular damage. Therefore, these cytokines could be considered therapeutic targets for the adjuvant treatment of chronic hepatitis and for the prevention of liver tissue injury in HBV-infected subjects. IL-6 and IL-35, higher in acute patients, can be involved in viral elimination and protection against chronicity. In acute cases, only genotypes A and F were found, and the viral load was higher than chronic cases. These results can contribute to the understanding of the complex regulatory mechanisms of the host's antiviral response related to cytokine production and spontaneous clearance or persistence of HBV infection.
Ethical Approval
FIOCRUZ Ethics Committee (number: CAE 06109812.4.0000.5248).
Footnotes
Acknowledgments
We thank the Clinic of Viral Hepatitis of Oswaldo Cruz Foundation and Paulo Sergio Fonseca Souza, Biologist project manager of the Clinic of Viral Hepatitis of Oswaldo Cruz.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was financed by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001, Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) and Oswaldo Cruz Institute who approved the project and funded the research with scholarship and grants.