
Abstract
Hepatitis A virus (HAV) and hepatitis E virus (HEV) cause most of the global burden of viral hepatitis. Geographical and seasonal patterns contribute to the epidemiological status of infectious diseases. The extent of these features in the setting of HAV and HEV infections has not been analyzed in detail. This point is important in highly endemic countries of both viruses, where the pediatric population is at high risk of contracting these infections. A comparison between the frequency of antibodies to HAV and HEV and viral RNA detection in serum samples from pediatric patients with acute hepatitis from South and West Mexico was performed. All samples were positive for HAV mono-infection, which was most frequently detected in the metropolitan areas during the rainy season in the South (90%) and all year round in the West (42%). No HEV mono-infection was detected in the studied regions. A 58% frequency for HAV/HEV co-infection was found in the West, predominantly in the metropolitan areas during the rainy months. A 10% frequency for co-infection broadly distributed in the South throughout the year was also found. Our findings underscore that the distribution of HAV and HEV infections varies through the year and differs among Mexico's distinct geographical regions.
Introduction
Although hepatitis A virus (HAV) and hepatitis E virus (HEV) infections are the leading causes of acute viral hepatitis worldwide, studies on both viruses have been neglected. Despite a highly effective vaccine against HAV that has been broadly distributed for the past 30 years and a vaccine licensed in China against HEV in 2012, both viruses still represent a global health concern (6). Currently, the World Health Organization estimates 10 million new cases of HAV each year (16), whereas HEV causes 20 million new infections annually (17).
HAV, first identified in 1973, is a small, positive-strand RNA virus and is the causative agent of acute and self-limiting hepatitis in humans. Contaminated food and water are the main sources of infection in resource-poor countries. HAV is also considered a foodborne pathogen based on documented outbreaks of infection caused by the consumption of frozen fruits worldwide (13). Overall, HAV prevalence is classified as high (>50% of the population), intermediate (15–50%), and low levels of endemicity (<15%) based on the detection of immunoglobulin G (IgG) antibodies to HAV (IgG anti-HAV). High endemicity of HAV is found in low-income countries, where infection typically occurs during early childhood (13).
HEV is a quasi-enveloped, positive-strand RNA virus. Although major viral hepatitis E outbreaks have been described since the 1950s, the infection remains underestimated; it is endemic in many low-income countries, where it is mainly transmitted through the fecal/oral route by contaminated food and water (4). In addition, HEV is also recognized as an emerging infection in developed regions, where it has been associated with zoonotic transmission by the consumption of raw pig meat (11).
HEV causes self-limiting viral hepatitis in immunocompetent individuals. Moreover, in immunocompromised patients, the infection may progress to chronic disease with the potential development of liver cirrhosis (4,11). Estimating the prevalence of HEV hepatitis by examining the frequencies of antibodies is still challenging due to variations in the sensitivity of diagnostic assays worldwide. In general, it is accepted that HEV infection has its peak incidence in early adulthood. However, pediatric societies recommend testing for HEV infection in children with extrahepatic manifestations or who have increased transaminases (5,14).
Suboptimal sanitation conditions and low income are associated with the diseases caused by HAV and HEV. These conditions are highly prevalent in developing regions, including Latin American countries (6). In this scenario, in the early 1980s, Mexico was considered a region of high endemicity for HAV infection. At that time, 90% of children between 1 and 5 years in Mexico were positive for IgG anti-HAV antibodies. Currently, data from the Mexican Ministry of Health reveal that of the total number of viral hepatitis cases from 1994 to 2017, 78.4% corresponded to HAV, and the pediatric population in Mexico is still the most prone to be infected with this virus (3,13).
Regarding HEV, Mexico is considered endemic for infection based on an outbreak reported in the 1990s (4). At present, information relative to the epidemiological status of this virus is not reported by the Ministry of Health in Mexico. However, data from scientific reports indicate that HEV circulates in swine (10) and humans; the virus has also been detected in pediatric patients (9), while IgG anti-HEV antibodies have been detected in adult patients with chronic liver disease (15). Moreover, we recently found a high frequency of anti-HAV and anti-HEV antibodies in pediatric patients with acute hepatitis (12). In conjunction, these findings support the requirement of scrutiny of these typically neglected infections in the country, particularly considering that differences in the geographical and seasonal distribution of HAV and HEV have not been analyzed in Mexico.
Materials and Methods
This study was conducted at the Servicio de Biologia Molecular, Hospital Civil de Guadalajara Fray Antonio Alcalde. In this comparative and retrospective study, immunoglobulin M (IgM) and IgG anti-HAV antibodies, IgM and IgG anti-HEV antibodies, and HAV and HEV-RNA were analyzed in serum samples from 222 pediatric patients (<16 years of age) with acute hepatitis from South and West Mexico. The samples collected in 2015 were obtained from the Laboratorio Estatal de Salud Publica del Estado de Oaxaca (n = 93) located in South Mexico and the Servicio de Biologia Molecular, HCFAA, Guadalajara (n = 129), located in West Mexico.
Acute hepatitis was defined as hepatomegaly, fever (>38°C), jaundice with elevated values of serum aspartate aminotransferase (AST) (>38 IU/L), and alanine aminotransferase (ALT) (>35 IU/L), as previously reported (12,15). Clinical and demographic features of the patients were previously recorded. Serum samples from patients with acute or chronic hepatitis C virus and hepatitis B virus (HBV) infections, patients with human immunodeficiency virus infection, patients undergoing treatment with hepatotoxic drugs, and patients diagnosed with autoimmune hepatitis were excluded. None of the included patients had been vaccinated against HAV or HBV. After the children's parents signed informed consent, blood samples from the children were obtained by venipuncture. This study was conducted under the statutes of the Helsinki Code, version 2013, and approved by the Ethics Committee of the HCFAA (IRB: HCG/CI-883).
A third-generation microparticle immunoenzymatic assay (Ax-SYM HAVAB-M 2-0; Abbott Laboratories, Chicago, IL) with an Ax-SYM analyzer (Abbott Laboratories) was used to screen for the presence of anti-HAV IgM and IgG antibodies in the serum samples. The presence of anti-HEV IgM and IgG antibodies in the collected samples was tested using a commercial ELISA kit following the manufacturer's instructions (MIKROGEN, Neuried, Germany). The presence of antibodies was screened in triplicate for each sample. The final reading was obtained with a WHYM201 microplate reader (Poweam Medical Co., Ltd., Nanjing, China).
Serum samples were tested for HAV and HEV viremia. For both viruses, RNA extraction was performed from 300 μL of patient serum with a QIAmp Viral RNA mini kit according to the manufacturer's specifications (Qiagen, Germany). HAV-RNA detection was carried out using unified protocols published for HAV typing protocol with two-step real-time polymerase chain reaction (PCR) (7). In this protocol, a fragment of 71 bp at the 5′ end of the nontranslated region (nt504–nt574) of HAV was amplified (7). Briefly, cDNA was generated in two steps. First, 12 μL of purified RNA was used to carry out a total reaction in 20.8 μL in two steps for each reaction. Random primers (2.5 ng/μL), 0.5 mM dNTP MIX (Promega, USA), and 5.8 μL H2O (RNase and DNase free) were used. The mix reaction was heated to 95°C for 2 min and placed on ice for 2 min. For the second step, 9.2 μL of a second mix of 2 U RNaseOUT™ (Invitrogen, USA), 6 μL of 5 × First-Strand Buffer (Invitrogen) [20 mM Tris-HCl (pH 7.5), 100 mM NaCl, 0.1 mM EDTA, 1 mM DTT, and 0.01% (v/v) NP-40, 50% (v/v) glycerol], 5 mM DTT (Invitrogen), and 1.33 U of SuperScript™ III (Invitrogen) was used. The reaction conditions were 22°C for 10 min, 50°C for 60 min, and 95°C for 2 min. For real time (RT)-quantitative PCR (qPCR) from 5 μL of cDNA, 15 μL of the following mix was added: 1 × TaqMan Master Mix (Invitrogen), 1 mM Q solution (Invitrogen), 0.5 μM HAV-5-F 5′-CAGTGGATGCATTGAGTG-3′ primer, 0.5 μM HAV-5-R 5′-CTAAGCACAGACAGGTC-3′ primer, 0.25 μM HAV-5′-Probe 5′-CCTARAGACAGCCCTGAC-3′, 0.5 μM EAV-2049-F 5′-CTTGCTAATTTACTGG-3′, 0.5 μM EAV-2147-R 5′-CTATTCTGCC 3CTCTTCTGTAC 3′, 0.25 μM EAV-2102-Probe 5′-CTATTCTGTACCTGCCGCAAT-3′, and 4 μL of cDNA (RNase and 3CTCTTCTGTAC 3′, 0.25 μM EAV-2102-Probe 5′-CTATTCTGTACCTCTGCCGCAAT-3′). The amplification conditions for the HAV-Net protocol were followed (7).
HEV-RNA detection was carried out with a two-step RT-nested PCR (nPCR) targeting the open reading frame (ORF)-2/3 region to amplify a 164 bp in the first round and 137 bp in the second round (15). For RT-nPCR, 5 μL of purified RNA was used to carry out a two-step 12 μL reaction by using 1.75 μM primer for each reaction, 870 μM dNTP MIX, 3 μL of moloney murine leukemia virus enzyme (M-MLV) 5 × Reaction Buffer (Promega, WI) (Tris–HCl pH 8.3 250 mM, KCl 375 mM, MgCl2 15 mM, and DTT 50 mM), and 8.5 U of M-MLV RT (Promega, WI) as indicated by the manufacturer. The first nPCR step using forward-HE361 and reverse-HE364 5′-CTGGGMYTGGTCDCDCGCCAAG-3′ primers was additionally performed in a 20 μL volume containing 4 μL of complementary DNA, 1 × PCR buffer (10 mM Tris-HCl pH 8.8, 50 mM KCl), 0.625 mM MgCl2, 0.25 mM dNTP mixture, and 2.5 U of Taq polymerase.
In the second round, 2 μL of the first-round PCR was used for amplification. Primers forward-HE366 5′-GYTGATCTCTCAGCCCTTCGC-3′ and reverse-HE363 5′-GMYTGGTCDCGCCAAGHGGA-3′ were used under the same conditions as in the first step. ALT and AST levels were measured in the serum samples following routine clinical laboratory procedures (15).
Co-infection was defined as patients positive for anti-HAV and anti-HEV IgM antibodies as well as HAV-RNA and HEV-RNA. Mono-infection was defined as the presence of only anti-HAV IgM antibodies and HAV-RNA or only anti-IgM HEV antibodies and HEV-RNA.
Qualitative variables were represented using percentages. The differences between the groups were evaluated using the chi-square test. Quantitative variables are expressed as the mean ± standard deviation. The differences between the groups were assessed with Student's t-test and analysis of variance for variables with normal distribution and with nonparametric tests, Mann–Whitney U and Kruskal–Wallis, for variables not normally distributed. A p-value <0.05 was considered to be significant. All analyses were performed using GraphPad Prism version 5.01 software (GraphPad Software, Inc., San Diego, CA).
Results
The total 222 serum samples obtained from both South and West Mexico showed positive serology for anti-HAV IgM antibodies, and HAV-RNA was detected. Likewise, all samples were negative for anti-HAV IgG antibodies. These findings indicate an acute state of infection due to HAV mono-infection that was more frequent in the South (90%) (Fig. 1A, B), where it was broadly distributed, particularly during the rainy months (August–October) (Fig. 1B, C). HAV mono-infection was found throughout the year in the West (42%) (Fig. 1B, C), most commonly found in the metropolitan areas (Fig. 1B). No HEV mono-infection was found in either region. Of the 129 samples obtained from West Mexico, 58% showed HAV/HEV co-infection.
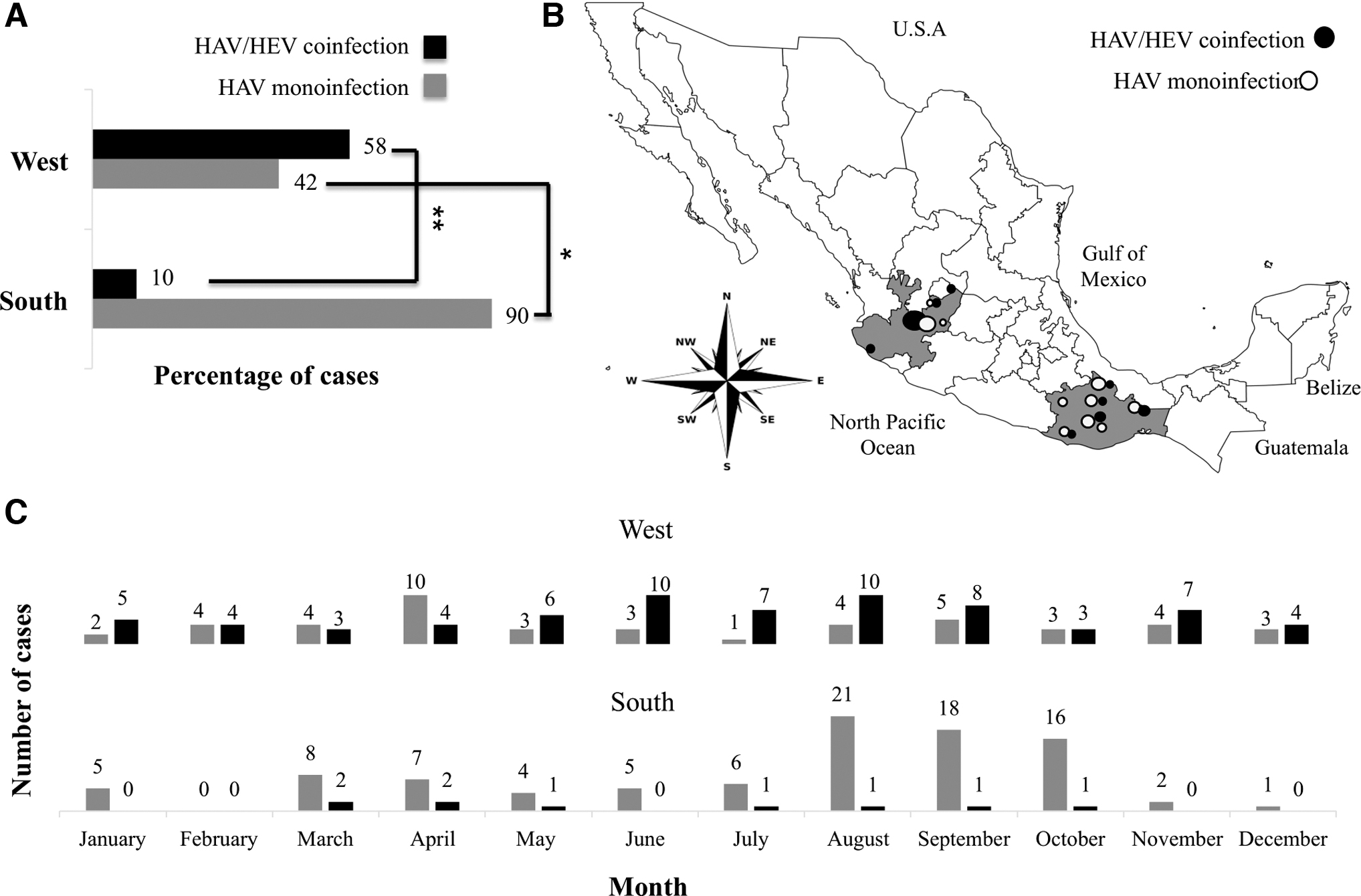
Seasonal and spatial differences in HAV and HEV infections in South and West Mexico.
In contrast, samples obtained from South Mexico only showed 10% HAV/HEV co-infection (Fig. 1A). Like in HAV-positive patients, all HAV/HEV-coinfected patients were positive for anti-HEV IgM antibodies and HEV-RNA and negative for anti-HEV IgG antibodies, denoting acute infections. That was consistent with an abnormal liver profile observed in all tested samples (Table 1). However, no significant differences were found in clinical features (hepatomegaly and jaundice) or demographics (age and sex) when the patients were categorized as HAV mono-infected or HAV/HEV co-infected (data not shown).
Clinical and Demographic Characteristics of Patients
p ≤ 0.05 was considered statistically significant. * p < 0.05, ** p < 0.001.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; HAV, hepatitis A virus; HEV, hepatitis E virus; IgG, immunoglobulin G; IgM, immunoglobulin M; NS, not significant; SD, standard deviation.
In patients from South Mexico, where co-infections were less frequent, a significant increase in AST levels was found compared to patients from West Mexico (Table 1). HAV/HEV co-infections were broadly distributed in South Mexico, while HAV/HEV co-infections in West Mexico were predominantly common in the metropolitan area (Fig. 1B). Most HAV/HEV co-infections were found in the rainy months (June–August) in the West, while HAV/HEV co-infections were found throughout the year in the South (Fig. 1C).
Discussion
Herein, we found that HAV/HEV co-infection caused acute liver disease in South and West Mexico children. However, seasonal differences were found when the frequencies of HAV mono-infection in both regions were compared, suggesting that in addition to water, other transmission routes, including frozen food consumption, should be considered when analyzing HAV distribution. As expected, considering that children are the population with a higher risk of exposure to HAV in the country (13), all samples were positive for this infection in our study.
Interestingly, HAV mono-infection was found predominantly in the metropolitan areas of South and West Mexico. This finding may be related to deficient health services in the most marginalized regions of the country (13). Thus, more effective detection and notification of HAV cases, particularly in the regions with the highest poverty levels, are recommended to obtain an updated report of the epidemiological status of the disease. In the setting of HEV infection, no mono-infections were found, and a varying prevalence in the scenario of HAV/HEV co-infection depending on the geographic region was confirmed, with HEV being more frequently found in the West.
The differences in the frequencies of HEV infections by geographical distribution suggest distinct transmission routes. Moreover, finding that the West region showed a higher incidence of HEV cases relative to the South is particularly relevant when considering that the higher frequencies of pigs with IgG anti-HEV antibodies have been found in West Mexico (10). Thus, future studies should explore the possibility of zoonosis in this specific region. The high percentage of HEV-positive cases (58%) in the West contradicts the HEV seroprevalence (<10%) reported in children worldwide. However, it is in alignment with a high incidence of HEV in children from India (17.75%) and Egypt (64.7%) (11). It supports that HEV may represent a risk for the pediatric population under similar economic and sanitary conditions.
Evidence reinforces that features including geographic and seasonal patterns of infectious disease distribution are essential for the proper interpretation of disease data (2). However, only a few reports have analyzed the prevalence of HAV and HEV according to the year's seasons. In India, the analysis of 23 outbreaks caused by these viruses underscored that most of the infections occurred in the wettest seasons of the year (8). Studying the distribution of HAV and HEV in specific regions in Latin America and the seasonal patterns related to these infections in this area has not been determined (1). Furthermore, information regarding these features related to children in this geographical region is still unknown.
Our findings underscore regional and seasonal differences in HAV and HEV distribution among pediatric patients in Mexico. The data obtained in this study will help elucidate HAV and HEV burden and raise interest in these neglected diseases.
Footnotes
Acknowledgment
The authors thank Gisela DuPont for her technical assistance.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was partially funded by Grant IA201220 from the Programa de Apoyo a Proyectos de Investigación e Innovación Tecnológica (PAPIIT), Universidad Nacional Autónoma de México to N.A.F. E.D.C.-V. was supported by a scholarship from the Secretaría de Salud, México. J.Y.A.-C. and O.V.-S. were supported by PhD scholarships from the CONACYT.