
Abstract
The coronavirus infectious disease 2019 (COVID-19), which is initiated by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has imposed critical challenges to global health. Understanding the kinetic of SARS-CoV-2-specific IgM and IgG responses in different subsets of COVID-19 patients is crucial to get insight into the humoral immune response elicited against the virus. We investigated IgM and IgG responses against SARS-CoV-2 nucleocapsid (N) and receptor-binding domain (RBD) of spike protein in two groups of recovered and deceased COVID-19 patients. The levels of IgM and IgG specific to N and RBD proteins were detected by ELISA. N- and RBD-specific IgM was higher in deceased patients in comparison with recovered patients, while there was no significant difference in N- and RBD-specific IgG between the two groups. A significant correlation was observed between IgG and IgM titers against RBD and N, in both groups of patients. These results argue against impaired antibody response in deceased COVID-19 patients.
Introduction
The coronavirus infectious disease 2019 (COVID-19), which emerged in December 2019 in Wuhan, China, is caused by a novel coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which has imposed devastating global health consequences (5,6). Although a large number of patients are asymptomatic, the clinical spectrum of the disease varies from mild to severe acute respiratory distress syndrome, which is marked by neutrophil and monocyte extravasation into bronchi, cytokine storm, and tissue damage from widespread inflammation (44). As of January 5, 2021, over 83 million COVID-19 cases have been reported worldwide to WHO, of whom 1.8 million succumbed to the infection since the start of the pandemic (1).
Coronaviruses are enveloped, nonsegmented, single positive-stranded RNA viruses with a diameter of 50–200 nm. Based on serotype and genomic characteristics, the coronavirus subfamily is divided into four genera: α, β, γ, and δ. SARS-CoV-2 belongs to the genus β, similar to SARS-CoV and Middle East respiratory syndrome coronavirus (MERS-CoV) (41,42). The virus has four structural proteins, including spike (S), envelope (E), membrane (M), and nucleocapsid (N) (42,43). Among them, S protein has a key role in viral attachment, fusion, and cell entry and is regarded as a target for vaccine development (15,35). To mediate its function, virus spike binds to its cognate receptor, the human angiotensin-converting enzyme 2 through its receptor-binding domain (RBD) and is activated after proteolysis by human proteases. This region of S protein is the main target for the host neutralizing antibodies (nAbs) (31,37). These antibodies could be used as potential prophylactic and therapeutic tool and have central importance in vaccine design and development (14,31). The N protein of the virus is involved in the transcription, replication, packaging of the genome into virions, and interference with cell cycle and is highly immunogenic for the host immune system (8,16). Although the N and S proteins of SARS-CoV-2 are considered as the main immunogenic proteins (26), information on the antibody responses against them in COVID-19 patients who recover from disease compared to those who succumbed to infection is limited.
Several risk factors are reported for COVID-19 severity, of which the most significant risk factor for death is age ≥65 years
N- and S-specific IgM and IgG increase gradually after clinical symptoms onset. Some studies have reported association between disease severity and the kinetic of the antibody response and also correlations between anti-RBD IgG nAbs and serum levels of proinflammatory biomarkers in severe patients (13). Thus, assessment of the kinetic of antibody response and antibody class-switching in the recovered and deceased COVID-19 patients may help to delineate the association between the kinetic of antibody response and disease severity in these patients.
The present study was conducted to compare the IgM and IgG antibody responses against SARS-CoV-2 RBD and N proteins in serum samples collected from recovered and deceased Iranian COVID-19 patients.
Materials and Methods
Ethics approval
This study was approved by the Ethical Committee of the National Institute for Medical Research Development (NIMAD) of Iran (IR.NIMAD.REC.1399.194). Written consent was obtained from all patients included in this study or their legal representatives.
Patients and sample collection
The total number of 120 cases, including 97 COVID-19 patients (39 deceased patients and 58 recovered patients) and 23 healthy controls, were recruited in this study. Healthy control samples were collected from the Blood Transfusion Organization of Iran 5 months before the COVID19 epidemic in Iran and stored at −20°C. All patients were laboratory-confirmed positive for SARS-CoV-2 by real-time PCR using throat or nasopharyngeal swab specimens. Patients' sera were collected during routine clinical testing and incubated in 56°C for 30 min to inactivate viruses and then stored at −20°C until use. The mean age and standard deviation of recovered and deceased patients and controls were 55.12 ± 14.48, 62.73 ± 14.24, and 50.52 ± 5.06, respectively. The recovered group included 37 male and 21 female patients, the deceased group included 26 male and 13 female patients, and the healthy control group included 18 male and 5 female individuals.
All patients were admitted to Imam Khomeini hospital affiliated to Tehran University of Medical Sciences. Physical examination and pulse oximetry were performed for all patients and chest computerized tomography (CT) scanning was performed for suspicious cases. Patients with the following criteria were admitted; (1) saturation of oxygen (SpO2) level <93% without supplementary oxygen and (2) characteristics of COVID-19 disease on the patient's CT scan, that is, involvement of more than half of the lungs. Also, patients with comorbidities and severe symptoms or signs of COVID-19 on their CT scan with normal SpO2 levels were admitted.
Major clinical manifestations observed in patients include fever, cough, dyspnea, and low blood oxygen saturation levels. The interval between the onset of symptoms and admission was 8.6 ± 7.2 days for the deceased group and 9.6 ± 7.3 days for the recovered group. Deceased patients were initially transferred to intensive care unit (ICU) and underwent oxygen ventilation, but a few days later passed away due to disease complications. Serum samples were collected from all patients 3–7 days after hospital admission.
Patients were classified into severe and nonsevere groups. Severe illness includes patients who had SpO2 <60% or required ICU or received invasive (mechanical) ventilation. Among the 39 deceased patients, 32 (82.05%) were classified as severe, and 7 (17.95%) were nonsevere. Among the 58 recovered patients, 17 (29.31%) were classified as severe and 41 (70.69%) were nonsevere.
Determination of serum IgM and IgG levels against RBD and N proteins
Recombinant nucleocapsid protein of SARS-CoV-2 expressed in Baculovirus insect cells (Cat# 40588-V08B; Sino Biological, Inc., China) and a recombinant RBD of SARS-CoV-2 spike protein expressed in HEK293 cells (Cat# 40592-V08H; Sino Biological, Inc.) were used at 2 μg/mL and 1.5 μg/mL, respectively, to coat 96-well microtiter plates (Maxisorp, Nunc, Denmark) in phosphate buffered saline (PBS) (pH 7.4) overnight at 4°C. After blocking with 3% skim milk in PBS containing 0.05% Tween 20 (Sigma Aldrich, Germany) and washing with PBS-0.05% Tween 20, the plates were incubated with 1:50 diluted sera at 37°C for 1 h, followed by washing. Subsequently, washed plates were incubated with appropriate dilution of HRP-conjugated sheep antihuman IgM or IgG (produced in our laboratory) at 37°C for 1 h. The optical density of the reactions was measured at 450 nm after addition of tetramethylbenzidine substrate solution followed by a stop solution of 1M H2SO4.
Statistical analysis
GraphPad Prism software, version 8 (GraphPad Software, Inc., La Jolla, CA) was used for plotting graphs and statistical analysis. Statistical analysis was performed using the Spearman correlation test for intragroup analysis and Mann–Whitney test for extragroup analysis in both groups of recovered and deceased patients. p Values ≤0.05 were considered significant.
Results
Determination of nucleocapsid-specific serum IgM and IgG levels
The antibody response to N protein of SARS-CoV-2, both IgG and IgM, was measured in serum samples from the two groups of patients and healthy controls. As illustrated in Figure 1, the level of both isotypes is significantly higher in both groups of patients compared to healthy subjects (p < 0.0001). Serum level of IgG was not significantly different between recovered and deceased groups. However, N-specific IgM was higher in deceased patients compared to recovered patients (p = 0.012).
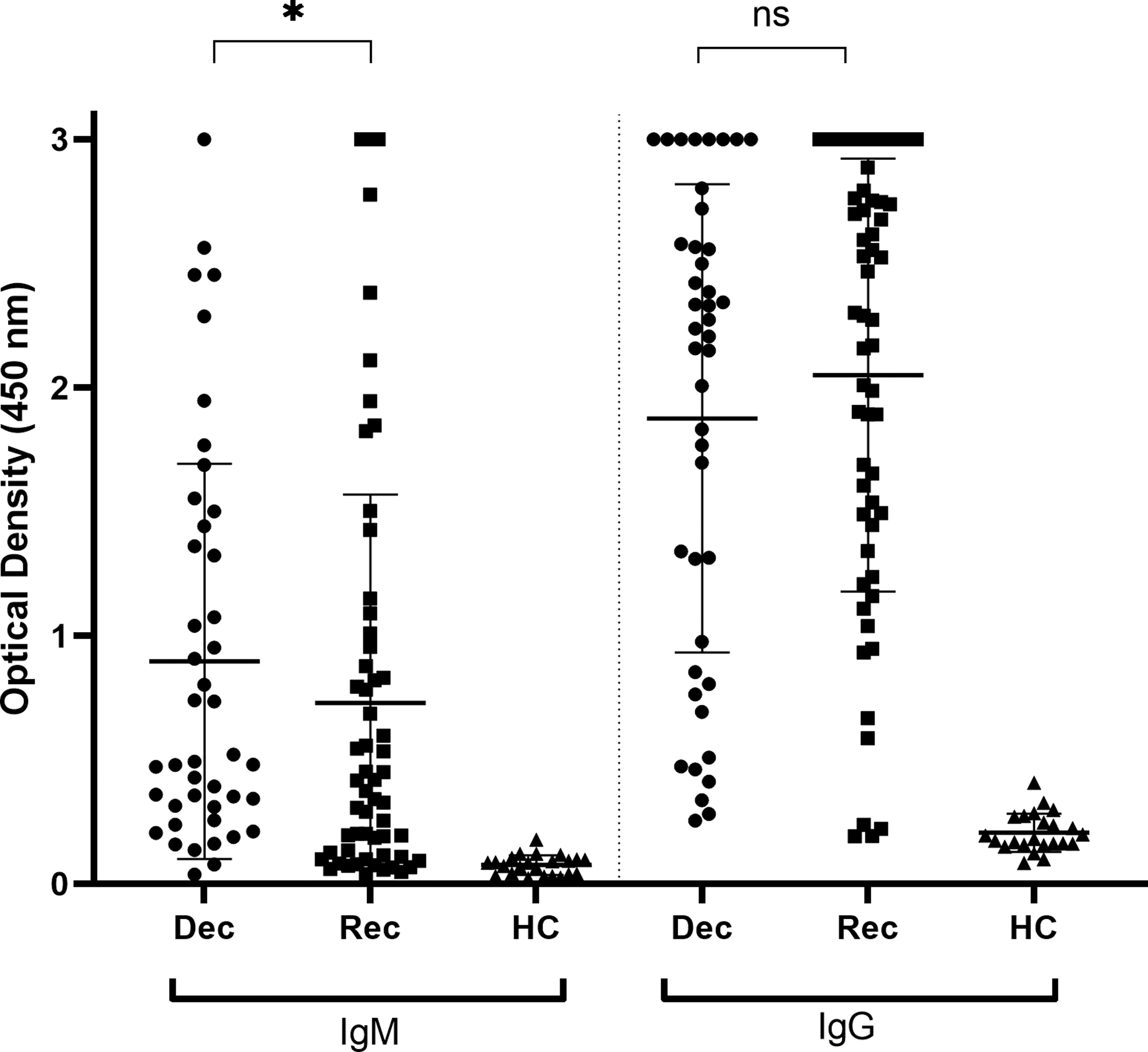
IgM and IgG responses against N in SARS-CoV-2 patients and healthy subjects. *p-Values <0.05. Dec, Deceased patients; Rec, Recovered patients; HC, healthy controls; ns, nonsignificant; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; N, nucleocapsid.
Serum levels of RBD-specific IgG and IgM
Similar to the antibody responses against N protein, the levels of RBD-specific IgG and IgM were significantly higher in both groups of patients compared to healthy subjects (p < 0.0001) (Fig. 2). While IgM titer was significantly higher in deceased compared to recovered patients (p = 0.011), the IgG level was similar in both groups. A significant correlation was observed between IgG and IgM titers against RBD and N in both groups of patients (Fig. 3).
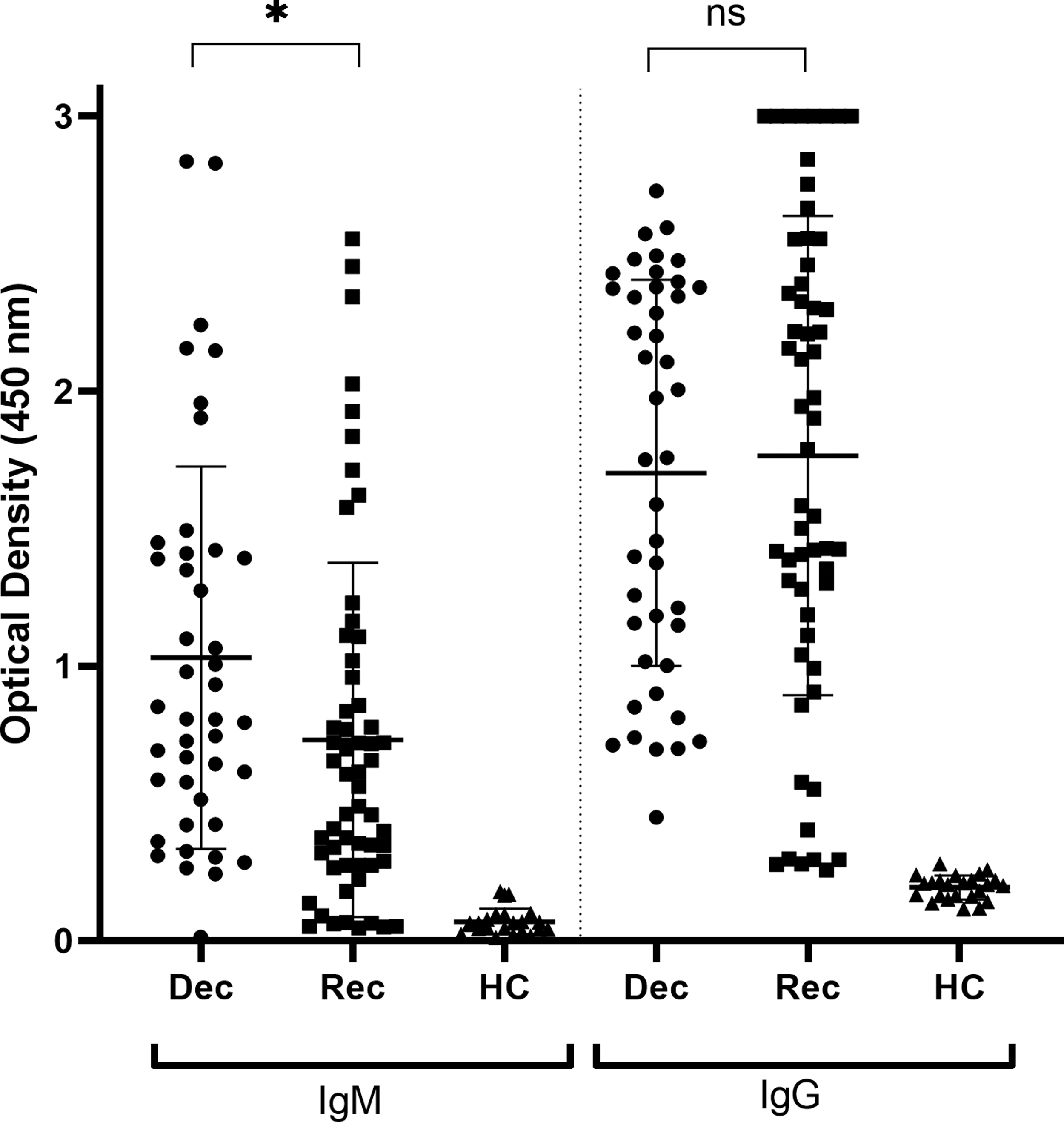
IgM and IgG responses against RBD in SARS-CoV-2 patients and healthy subjects. *p-Values < 0.05. Dec, Deceased patients; Rec, Recovered patients; HC, healthy controls; ns, nonsignificant; RBD, receptor-binding domain.
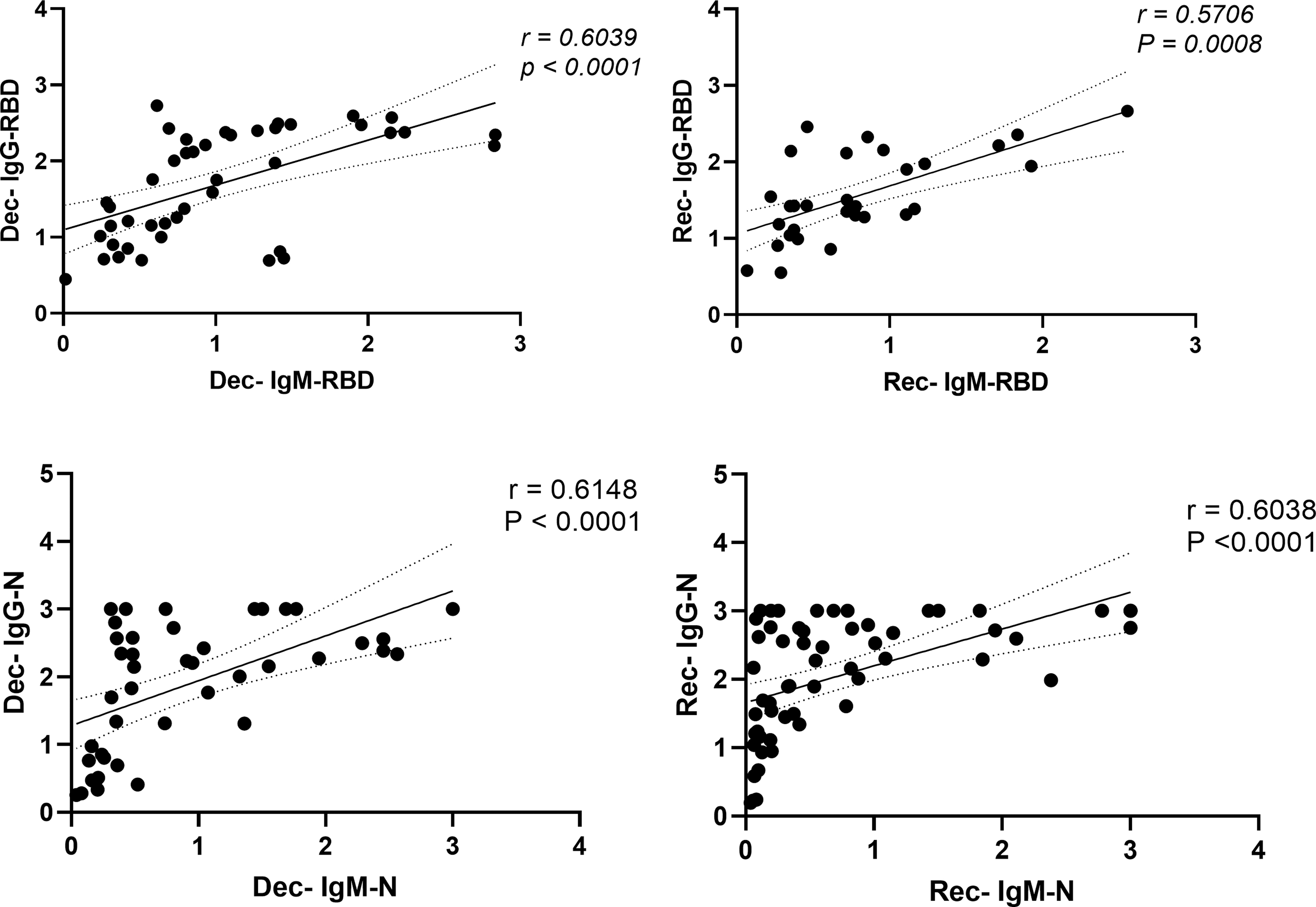
Correlation between IgM and IgG responses against N and RBD in deceased and recovered patients. Dec, Deceased patients; Rec, Recovered patients.
Discussion
The novel SARS-CoV-2 is a recently emerging virus causing a human pandemic (18). Since the humoral immune response and development of nAbs is critical for containment of viruses, assessment of the profile of antibody response in COVID-19 patients might reveal important aspects of COVID-19 pathogenesis.
The dynamics of the antibody response against SARS-CoV-2 are currently under investigation. Generally, for IgM, the mean time to seroconversion ranges from 4 to 14 days postsymptoms onset, with a peak within 2–5 weeks, followed by a decline over time to below the detection limit. Mean time to seroconversion for IgG ranges from 12 to 15 days postsymptoms onset, showing a peak between 3 and 7 weeks (28). Antibodies against SARS-CoV-2 N and RBD proteins are readily detected in COVID-19 patients (3,17). However, little information is available about the serum levels of N- and RBD-specific IgM and IgG in hospitalized patients who eventually recover or later die due to the SARS-CoV-2 infection.
At the beginning of the outbreak of the disease, it was thought that the antibody response against viral antigens, particularly nAbs induced against RBD, is poor in COVID-19 patients who later die due to the infection, suggesting that higher levels of RBD antibodies are associated with patients recovery (23). However, our findings with regard to both RBD- and N-specific antibodies do not support this proposition. There has been no significant difference between the two groups of patients concerning the serum titer of anti-RBD and anti-N IgG.
Taking into consideration the fact that RBD, but not N, antibodies are potentially neutralizing and have been reported to closely correlate with viral neutralization (22,32,34,36), this would raise questions about the functional significance of these antibodies in deceased patients. It seems that other destructive immunopathogenic parameters are implicated, which quickly worsen and complicate the course of disease and recruit other highly pathogenic inflammatory cells and mediators to the site of infection, causing massive inflammation and obstruction (4,12). In this deteriorating condition, nAbs cannot overcome the problem and the patients may eventually die from the consequences of such overwhelming inflammatory reactions. Moreover, nAbs are mainly effective for neutralizing circulating virus particles, and once the infection is established with a high viral load, antibody molecules will not be able to effectively maintain the infection and cell-mediated players, particularly cytotoxic T cells need to be recruited to fight against infected cells (21,27,33). This scenario is in agreement with recent findings regarding the outcome of convalescent plasma therapy in COVID-19 patients, showing low or no therapeutic effects in patients with severe disease compared to those with mild or moderate disease (2,25). It has recently been shown that in recovered patients with different disease severity (severe, moderate, mild, and asymptomatic), a positive correlation is found between serum neutralizing capacity and disease severity, in particular, the highest nAb capacity was reported in severe patients sera, with a lack of ability of asymptomatic patients to mount competent nAbs (7,19,20,24).
We have also observed significantly higher serum IgM levels against both RBD and N antigens in deceased patients in comparison to the recovered group. Similar results have recently been reported in a retrospective case-control study showing significantly higher serum IgM levels, but not IgG, in deceased patients compared to mild-moderate patients. A negative correlation was found between serum IgM levels and clinical outcome, eosinophil count, and albumin levels (39).
It is possible that the recovered patients (who were mostly nonsevere) waited longer to go to the hospital and therefore have lower IgM. This, however, has not been the case, since the interval between the onset of symptoms and hospitalization was 8.6 ± 7.2 days in the deceased group and 9.6 ± 7.3 days in the recovered group, which is not significantly different. Therefore, it can be concluded that the difference in IgM level between the two groups is most likely due to the difference in the severity and outcome of the disease.
Recently, dominant presence of macrophages and a general deficiency of T cells and B cells in the lung tissues from deceased COVID-19 patients have been reported. Furthermore, T follicular helper cells and germinal centers were largely absent in the draining lymph nodes in deceased patients compared with the convalescent patients (10). As such, it can be speculated that defect in germinal center formation may lead to impaired antibody class-switching from IgM to IgG in deceased patients. The source of SARS-CoV-2 RBD and N antigens-specific IgG in these patients may be originated from short-lived extra follicular plasmablasts producing IgG during primary B cell response with no extensive affinity maturation. Indeed, such weakly reactive IgG and IgM antibodies may be responsible for the so-called antibody enhancement effect, which has already been reported in SARS-CoV2 and other coronaviruses as well as HIV and Dengue virus infections (38). Although the cause(s) of these incomplete neutralization phenomena is unclear, the antibody responses likely play an important role in determining the ultimate disease outcome of SARS-CoV-2-infected patients and therefore needs further investigation.
Footnotes
Authors' Confirmation Statement
Dr. F.M., Dr. D.H., Dr. V.S., Dr. G.A.K., Dr. J.K., Dr. A.G., Dr. S.R.R., Dr. A.R., Dr. M.S.S., Dr. R.A.F., Dr. A.-H.Z., Dr. M.M.A., and Dr. F.S. are from the Tehran University of Medical Sciences (Tehran, Iran), and Dr. M.J.-T. is from Avicenna Research Institute (Tehran, Iran), where education and research are the primary functions.
Authors' Contributions
F.M. and D.H., performing the assays and writing original draft; V.S., A.Gh., and G.A.K., reviewing and editing the article, conceptualization, and data analysis; R.A.F. and J.K., performing the assays; S.R.R and A.R., clinical samples and data collection and analysis; M.S.S., data collection and analysis; M.J.-T. and A.-H.Z., reviewing and editing the article, project conceptualization, and data analysis; M.M.A. and F.S., writing original draft, review and editing, project conceptualization, data validation, project administration, and supervision. All authors have read and agreed to the published version of the article.
Acknowledgments
The authors thank Mohammad Ali Judaki and Tannaz Bahadori for their technical assistance.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a grant from the NIMAD of Iran (Grant No. 993421).