
Abstract
Severe fever with thrombocytopenia syndrome (SFTS) is a novel infectious disease caused by bunya virus. The purpose of this study was to investigate the clinical characteristics of SFTS patients and their virus-related immune disorders in vivo. Patients with SFTS admitted to Nanjing Drum Tower Hospital from 2017 to 2020 were retrospectively analyzed, and divided into survival group and death group according to the 28-day survival. Clinical characteristics and laboratory examination results of SFTS patients were recorded, and dynamic changes of immune function and inflammatory factors were statistically analyzed. Prolonged activated prothrombin time (APTT) (p = 0.001), high viral load (p = 0.001), and elevated human leukocyte antigen DR (HLA-DR) level (p = 0.002) were independent prognostic risk factors for SFTS patients. Compared to the survival group, the nonsurvival group was more prone to hemorrhagic and neurological symptoms (p < 0.05). Natural kill (NK) cell count, interleukin-10, interferon-α, and tumor necrosis factor-α scores in the nonsurvival group continued to increase after admission, while CD3+ T, CD4+ T, and CD8+ T cell counts continued to decrease. CD3+ T lymphocyte count was negatively correlated with viral load (R = 0.3883, p < 0.001), CD4+ T lymphocyte count was negatively correlated with viral load (R = 0.28933, p < 0.001), CD8+ T lymphocyte count was negatively correlated with viral load (R = 0.781, p < 0.001), and HLA-DR was positively correlated with viral load (R = 0.489, p < 0.001). High viral load, prolonged APTT time, and elevated HLA-DR level are independent prognostic risk factors for SFTS patients. The T lymphocyte subsets of SFTS patients continue to decrease after infection, and the number of T lymphocyte subsets can reflect the severity of the disease.
Introduction
Severe fever with thrombocytopenia syndrome (SFTS) is a novel infectious disease caused by a novel Bunyavirus infection, which was first reported in central China in 2009 (38); the incidence of the disease gradually expanded from central China to eastern China, East Asia, and Southeast Asia (11,15,21,24,30,34,36,37,40). The mode of transmission is mostly the bite of tick, and it is transmitted from person to person (10,13,35). The annual incidence rate has being increasing by nearly 6%. The annual confirmed cases has exceeded 5,000 (14,17), with a high mortality rate of about 6–30%, especially in Pakistan, which is a country with substantial severe fever with thrombocytopenia syndrome viral (SFTSV) activity, with a mortality rate of 16.2–30% (37).
The treatment is mostly symptomatic as there are no effective drugs and vaccines for the treatment of SFTS, which is listed as one of the 10 most infectious diseases requiring special attention by World Health Organization (WHO) (22).
Immune dysfunction occurs when the immune system fails to defend itself effectively, is too strong to attack, or is too weak to defend itself against certain triggers. The secondary infection that occurs after viral infection and the inability to identify the virus are usually associated with immune dysfunction. Secondary infection in SFTS patients is often associated with high mortality. Therefore, evaluating the immune status of SFTS patients may help identify high-risk patients.
To reduce the fatality rate of SFTS patients and identify high-risk patients early, patients with SFTS admitted to Nanjing Drum Tower Hospital from 2017 to 2021 were included in this study. The dynamic changes of peripheral blood immune cell count and inflammatory cytokines were analyzed. Furthermore, the correlation between immune cell count and viral load was also analyzed.
Materials and Methods
Ethical approval and consent to participate
This study was approved by the Ethics Committee of Nanjing Drum Tower Hospital, Affiliated Hospital of Nanjing University Medical School. The data used in this study were anonymized before use and were collected during routine procedures, which did not pose any additional risk to patients. Considering the retrospective nature of this study, the ethics Committee of Drum Tower Hospital of Nanjing University Medical College gave up the requirement of informed consent of individual patients.
General data
The clinicopathological data of patients diagnosed with SFTS admitted to Nanjing Drum Tower Hospital from January 2017 to October 2020 were retrospectively collected, which include age, gender, occupation, time from onset to admission, female maidworm bite history, past medical history, and laboratory immunity-related indicators.
Inclusion criteria
The inclusion criteria were as follows: (a) Bunya viral RNA positive, (b) age between 18 and 75 years, and (c) a hospital stay longer than 7 days.
Exclusion criteria
The exclusion criteria were as follows: (a) death within 24 h after admission; (b) lack of clinicopathological data related to patients; and (c) patient is diagnosed with suspicious or other immune deficiency diseases.
Data collection and grouping
The white blood cell (WBC) count, platelet (PLT) count, neutrophil ratio, lymphocyte ratio, hemoglobin, D-dimer, prothrombin time (PT), activated prothrombin time (APTT), creatinine, urea nitrogen, lactate dehydrogenase (LDH), creatine kinase isoenzyme (CK-MB), bilirubin, C-reactive protein (CRP), and other data were recorded on days 1, 3, 5, 7, 9, 11, and 13 after the onset of symptoms; at the same time, lymphocyte subsets, natural kill (NK) cell counts, inflammatory factors, and other immune-related data of hospitalized patients were recorded on day 1, 6, and 11 after symptom onset. In addition, viral load, sepsis-related organ failure assessment (SOFA) score, and Glasgow Coma Scale (GCS) score of patients were recorded on days 1, 5, 10, and 15 after symptom onset.
Patients were divided into survival group and death group according to the 28-day survival.
Cytokines measurement
The concentrations of cytokines in the serum of different patients were measured by the LEGENDplex bead-based multiplex assay (Biolegend, CA) according to the manufacturer's protocol.
Flow cytometry
Peripheral blood mononuclear cells were isolated by Ficoll gradient centrifugation. Antibodies used include anti-CD19 (HIB19), anti-CD3 (UCHT1), anti-CD4 (OKT4), andti-CD8 (SK1), anti-CD16 (3G8), andti-CD56 (5.1H11), and anti-human leukocyte antigen DR (HLA-DR) (L243). Antibodies were purchased from eBioscience, Biolegend, or MD Bioproducts. Flow cytometric analysis was performed on a 3-laser FACSAria III (BD Biosciences, New York).
Statistical analysis SPSS 21.0 software was used for data analysis
Data conforming to the normal distribution were analyzed using mean and standard deviation (SD), and data conforming to the non-normal distribution were analyzed using median and quartile. Mean + SD was used to represent correlation analysis results. Independent sample t test or Mann–Whitney U test was selected to compare the data between the two groups. The count data were expressed as n (%), and X was used for comparison between group2 inspection. One-way analysis of variance (ANOVA) and binary logistic regression were used to analyze prognostic factors of SFTS patients, relationships among variables were assessed with Pearson or Spearman's rank correlation and repeated measurement analysis of variance (generalized estimating equations) was used for the values of repeated measurements. p < 0.05 was considered statistically significant.
Results
Clinical features
Among the 122 patients with SFTS included in the study, there were no significant differences between the survival group and the death group in the time from onset to admission, gender, and previous medical history (p > 0.05). The incidence of severe neurological symptoms and hemorrhagic symptoms in the nonsurvival group was higher than that in the survival group (p < 0.05), and the PLT count, WBC count, lymphocyte count, and albumin count at admission were lower than those in the survival group (p < 0.05). In addition, patients in the death group had higher age, D-dimer at admission, APTT time, PT time, AST, LDH, viral load, SOFA score, and CRP count than patients in the survival group (p < 0.05). The detailed clinical characteristics of SFTS patients in the survival and nonsurvival groups are shown in Table 1.
Clinical Characteristics of Severe Fever with Thrombocytopenia Syndrome Patients in the Survival Group and the Nonsurvival Group
A p-value of less than 0.05 implies significance, and displays in bold.
ALT, alanine transaminase; APTT, activated prothrombin time; AST, aspartate aminotransferase; CRP, C-reactive protein; HLA-DR, human leukocyte antigen DR; LDH, lactate dehydrogenase; NK, natural kill; NLR, neutrophil to lymphocyte ratio; PLT, platelet; PT, prothrombin time; WBC, white blood cell.
Analysis of prognostic risk factors for SFTS patients
One-way ANOVA of SFTS patients showed that age (p = 0.032), WBC count (p = 0.015), neutrophil to lymphocyte ratio (p < 0.001), APTT time (p = 0.042), LDH (p = 0.001), CRP (p = 0.008), albumin (p = 0.001), viral load (p = 0.001), and CD3+ were significantly correlated with the survival status of SFTS patients. In further binary logistic regression analysis, prolonged APTT time, high viral load, and elevated HLA-DR were independent prognostic risk factors for SFTS patients. Other detailed data are shown in Table 2.
Univariate and Multivariate Analysis of Severe Fever with Thrombocytopenia Syndrome Patients
A p-value of less than 0.05 implies significance, and displays in bold.
CI, confidence interval; CK-MB, creatine kinase isoenzyme; OR, odds ratio.
Dynamic analysis of immune function in survival and non-survival group
The CD3+ T, CD4+ T, and CD8+ T, B lymphocyte count, NK cell count, and HLA-DR of SFTS patients were recorded and statistically analyzed. Results showed CD4+ T and CD8+ T lymphocyte count decreased gradually in the nonsurvival group, while B lymphocyte count and NK cell count increased gradually. CD3+ T lymphocytes and HLA-DR tended to be stable. In the survival group, CD4+ T and CD8+ T lymphocyte count and HLA-DR decreased gradually, while B lymphocyte count and NK cell count increased gradually; CD3+ T cells tended to stabilize. Detailed results are shown in Figure 1.
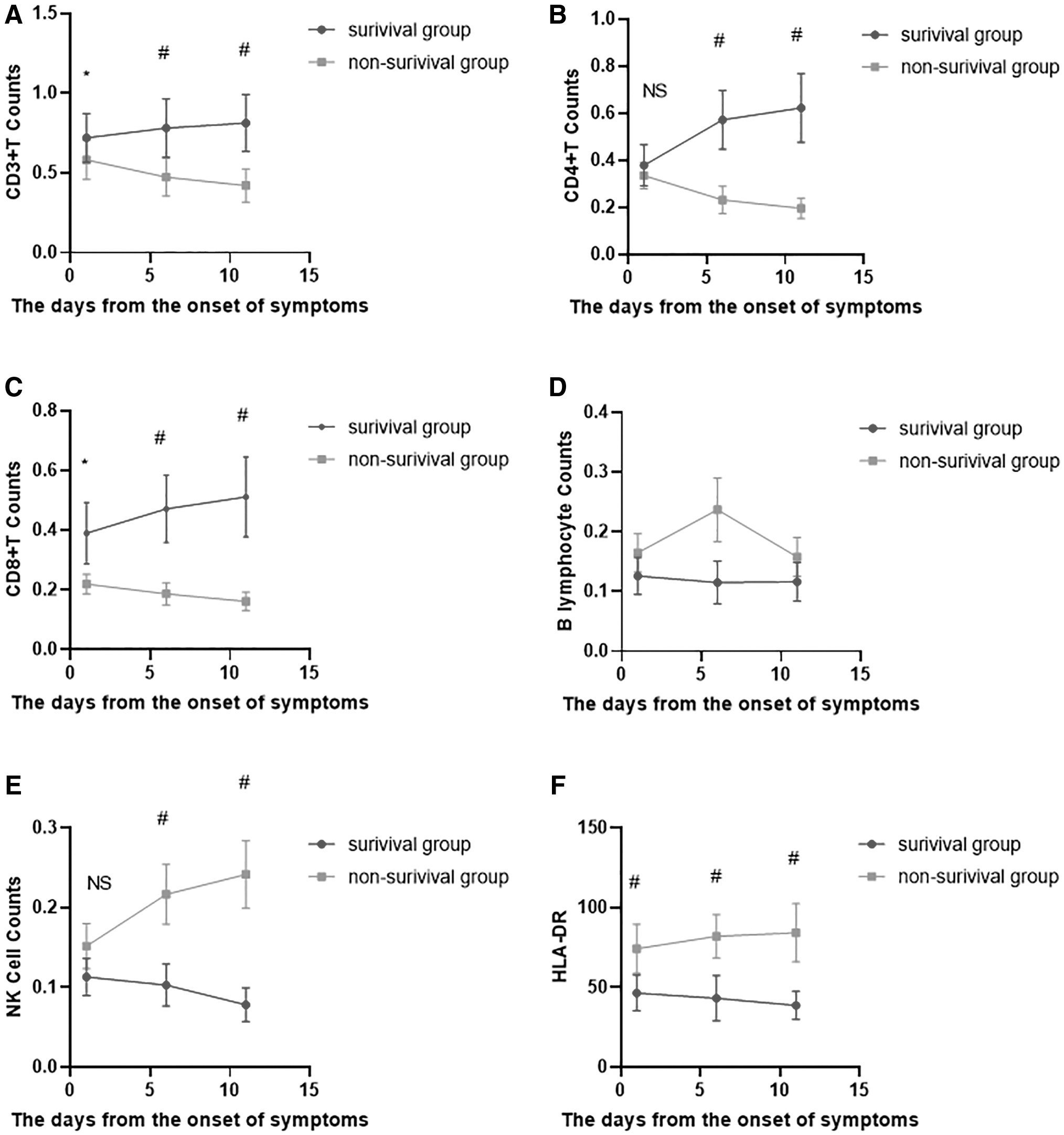
Dynamic analysis of immune function in SFTS patients.
Analysis of dynamic changes of inflammatory factor expression in SFTS patients
The expression levels of interleukin (IL)-6, IL-8, IL-10, tumor necrosis factor (TNF)-α, interferon (IFN)-α, and IFN-γ in SFTS patients were recorded. The results showed that the expression levels of IL-10, IFN-α, TNF-α, and IFN-γ increased gradually in the nonsurvival group, and there were statistical differences in the expression levels of IL-10, TNF-α, and IFN-α at all three time nodes. The expression level of IL-6 decreased gradually, and the IL-8 level decreased first and then increased. The expression levels of IL-10, IFN-α, TNF-α, and IFN-γ in the survival group decreased gradually, while IL-6 increased slowly, and IL-8 level increased initially and then decreased. Detailed results are shown in Figure 2.
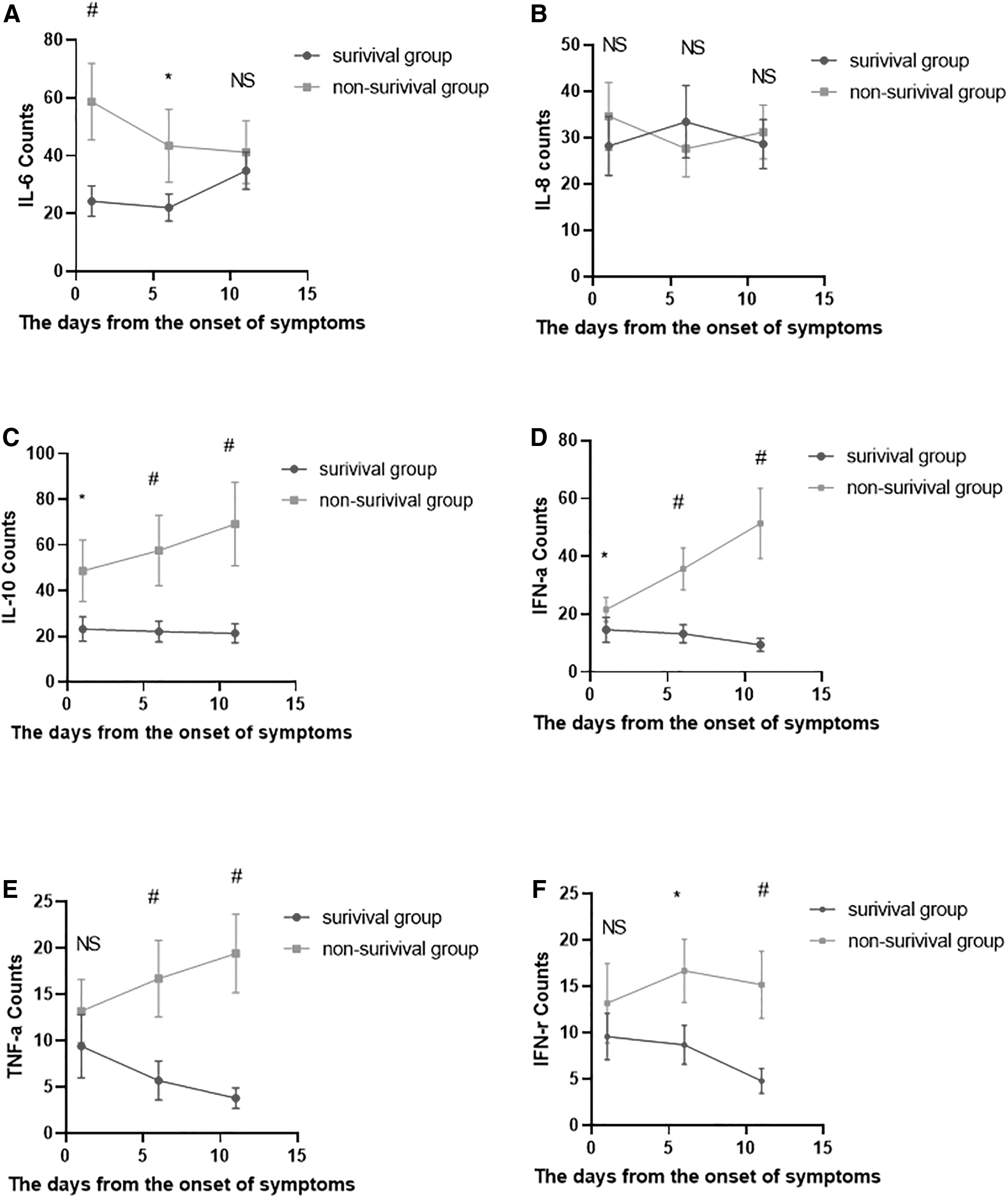
Analysis of dynamic changes of inflammatory cytokine expression in SFTS patients.
Correlation analysis of viral load
In this study, viral load was an independent risk factor for death in SFTS patients. CD3+ T lymphocyte count was negatively correlated with viral load (R = 0.3883, p < 0.001), CD4+ T lymphocyte count was negatively correlated with viral load (R = 0.28933, p < 0.001), CD8+ T lymphocyte count was negatively correlated with viral load (R = 0.781, p < 0.001), and HLA-DR was positively correlated with viral load (R = 0.489, p < 0.001), as shown in Figure 3.

Correlation analysis of CD3+ T, CD8+ T, HLA-DR, and viral load.
Discussion
Since 2011, the incidence of SFTS has expanded from central China to East Asia, the Eastern Pacific, Australia, and other places, and has become one of the top 10 infectious diseases that WHO focuses on (11,21,22,24,34,37). Through retrospective analysis of the past medical history, clinical characteristics, and laboratory examination indicators of SFTS patients, our study found that patients in the death group had more severe clinical symptoms, higher viral load, higher incidence of double infection, and more disorganized immune function. In binary logistic regression analysis, we found that high viral load, prolonged APTT time, and elevated HLA-DR level were independent risk factors for death of SFTS patients.
Till date, there have been few studies on immune dysfunction in SFTS patients, and the consequences after immune dysfunction are still unclear. Therefore, this study focuses on the dynamic changes of T lymphocyte, B lymphocyte, and inflammatory factors, as well as the correlation between lymphocyte and viral load.
T lymphocyte subsets play an important role in immune clearance in diseases caused by viral infection (3,25). CD8+ T lymphocytes secrete killing cytokines such as TNF-α and IFN-γ after interaction with major histocompatibility complex (MHC) class I molecules expressed on antigen-presenting cells, which play an important role in the immune clearance process of respiratory virus and hepatitis B virus infection in vivo (7,19,31). CD4+ T lymphocytes mainly play an auxiliary killing role and can be induced to differentiate into helper T (T helper) cells to participate in immune regulation under the action of a variety of precursors. CD4+ T lymphocyte is the target of HIV, and a number of studies have reported that it is also observed in the infection of SARS-COV-2 virus and Ebola virus+ T cell decrease (2,26). When the body has immune dysfunction, the probability of double infection is higher.
In this study, CD8+ T lymphocyte count of SFTS survival group patients was significantly higher than that in the death group on days 1, 6, and 11 after symptom onset (p < 0.05), while CD8+ T lymphocyte count in the survival group showed a gradual increase, that in the death group decreased gradually.
In addition, on days 1, 6, and 11 of symptom onset, CD4+ T lymphocyte count of SFTS survival group was significantly higher than that in the death group (p < 0.05), CD4+ T lymphocyte count in the survival group increased gradually, while CD4+ T lymphocyte count in the death group decreased gradually (p < 0.05); CD3+ T lymphocyte count was significantly higher compared with death group (p < 0.05), and CD3+ T lymphocyte count in survival group showed a gradual increase, while CD8+ T lymphocyte counts in the death group decreased gradually, which was consistent with previous studies (16,29). In correlation analysis, T lymphocyte count was inversely correlated with viral load.
The results suggest that T lymphocyte count can respond. A previous study on patients with SFTS reported sustained high expression of PD-L1 on the surface of T lymphocytes in patients with fatal SFTS, but low expression in survival patients (28), suggesting that apoptosis may be the cause of T lymphocyte decrease in SFTS patients. PD-1 inhibitors have achieved good efficacy in inhibiting and eliminating persistent HBV replication and HIV (8,32). Therefore, T lymphocyte count can reflect the severity of the disease and PD-1 target blocking may be a potential immunotherapy strategy for SFTS patients.
B lymphocytes participate in immune surveillance and clearance mainly through humoral immunity. Previous studies have shown that B lymphocytes are the main target cells of SFTS virus (33). B lymphocyte count declines in most viral diseases, with an increase reported only in Ebola virus (27). In this study, according to the onset of symptoms, it was found that the B lymphocyte count of SFTS patients in the survival group was in dynamic balance, while the B lymphocyte count of SFTS patients in the death group showed an increasing trend initially and then a decreasing trend. There was no statistical significance at the three time nodes, which was not consistent with the results of previous studies (16,29).
HLA-DR is a class MHC-II molecule containing two Subunits (36 kDa and 27 kDa, respectively). It is expressed on a variety of immune cells (6), and can reflect the body's immune function. In this study, elevated HLA-DR was found to be an independent risk factor for death in SFTS patients. In the dynamic analysis, the survival group was in dynamic balance, while the death group continued to increase. Similar reports have been reported in HBV and HIV (1,12,20). In correlation analysis, HLA-DR was positively correlated with viral load. Therefore, HLA-DR values can reflect the severity of the disease.
NK cells are an important part of the innate immune system and are involved in antiviral immune killing and elimination. NK cells play an important role in early viral infection in humans and mice, and can effectively kill infected or transformed cells (18). In addition, NK cells can secrete a series of inflammatory factors such as IL-10, TNF-α, and IFN-γ, and these inflammatory factor storms are usually associated with the severity of viral infectious diseases (39). In this study, The NK cell count in the survival group was in a decreasing trend, while the NK cell count in the death group was in a gradually increasing trend. There were statistical differences at all three time points, but there was no correlation with viral load.
In this study, we observed significantly increased IFN-γ and IL-10 expression levels in patients in the death group. IFN-γ is a key cytokine in cellular immunity, which mainly acts on MHC class II antigen presentation and cytotoxic T cell activation (9). In this study, IFN-γ expression in the survival group was low, while that in the death group temporarily increased and then decreased, and there was a difference between the two groups at the intermediate site (p < 0.05).
Therefore, we hypothesized that IFN-γ signaling could be switched to disturbance in the death group, leading to immune evasion. IL-10 is a classic immunosuppressive factor that has been shown to inhibit secondary lymph node formation by affecting the function of follicular helper T cells and by affecting the expression of transcription factors Bcl-6 and BLAMP-16 (5,23). In addition, previous studies have shown that IL-10 can downregulate the expression level of MHC-II costimulatory factors in B7 family to produce immune escape (4). In this study, we found that IL-10 levels in the SFTS survival group showed a trend of dynamic decline after symptom onset, while the IL-10 levels in the death group showed a trend of continuous increase. Therefore, we speculated that IL-10 could be used as an indicator of disease progression in patients with SFTS.
This study also has some limitations. First of all, only 122 SFTS patients from a single center were included in the study, so the small number of samples as a retrospective study, especially the small number of patients in the death group, may lead to research bias. Second, the clinical indicators and immunological characteristics of SFTS patients after symptom onset were analyzed in this study, and some values were missing due to the difference in the time from onset to admission.
Conclusion
In conclusion, SFTSV infection will lead to a series of changes in the immune system and inflammatory factor levels of the body. Prolonged APTT time, high viral load, and HLA-DR level are independent prognostic risk factors for SFTS patients. In the death group, T lymphocyte count and HLA level continued to decrease, and T lymphocyte count and HLA-DR level were positively correlated with viral load. The decrease of T lymphocyte count may be related to increased apoptosis. So T lymphocyte count and HLA level can reflect the severity of the disease. The majority of SFTS patients are treated in local hospitals. When the immune function of SFTS patients cannot be examined by flow cytometry, the viral load can reflect the immune function of SFTS patients.
Footnotes
Authors' Contributions
All work was approved by the co-authors. W.Y. and C.M. made significant contributions to conception and study design. Data acquisition was completed by D.W., K.C., and X.S. Data analysis and interpretation were performed by B.Z. and X.C.; D.W., K.C., and X.S. have written the draft of the article and critically revised it.
Author Disclosure Statement
The authors declare that they have no conflict of interests. I would like to state on behalf of my co-authors that the work described is original research that has not been previously published and is not considered for publication elsewhere, in whole or in part. All authors read and approved the final article.
Funding Information
This work was supported by The National Natural Science Foundation of China (no. 82002082 to K.C., 81970500 to X.S.).