
Abstract
The kinetics of postvaccination serum anti-Spike IgG concentration were determined in 1,541 health care workers (Sant'Andrea Hospital of Rome, Italy) with no prior infection by SARS-COV-2. Anti-Spike IgG were measured at 3, 12, and 24 weeks after the completion of the primary vaccine cycle (two doses of the BNT162b2 vaccine by Biontech/Pfizer) and 3 weeks apart a third BNT162b2 dose. Stratification of the study population by age (decades from 21–30 to 61–70) highlighted that 24 weeks after cycle completion all age groups had an order of magnitude reduction in serum IgG titers. Considering older adults (age 61–70), they had significantly lower serum IgG titers at each time point compared with younger people, except after the booster dose, which induced similar and elevated IgG titers despite the age.
Introduction
The observed decline over time in the serum anti-Spike IgG titers after anti-COVID-19 vaccination (6,8,12) and the rapid diffusion of novel SARS-COV-2 variants led many governments and health care stakeholders to recommend a booster dose. In Italy, the vaccination campaign started at the end of 2021 with immunization of health care workers (HCW), whereas the third dose campaign started around October 2021 and was available for people since the fourth month by second dose. Thus, the HCW population received the booster dose around 9 months after completion of the primary vaccination.
Presently, with the rapid and massive diffusion of the Omicron variant, the third dose of vaccine has demonstrated its efficacy in preventing severe COVID-19 disease (1,11), but people and stakeholders are concerned about the timing and the appropriateness of further vaccination series. Thus, it is hoped that the booster dose can induce a more durable immune response. Preliminary data showed that booster induces a neutralizing antibody response against highly divergent SARS-CoV-2 variants (2) and increases protection (10).
In this report, we describe the kinetics of serum anti-Spike IgG antibodies after second and third doses of BNT162b2 vaccine in a large cohort of naive Italian HCW (N = 1541). The serum anti-Spike IgG were measured at 3, 12, and 24 weeks after second dose and at 3 weeks after booster dose. The data show that the booster dose raises the anti-Spike IgG concentration above the maximum value observed after second dose, which was 3 weeks apart it. Interestingly, the increase is consistent also for people in the age range 61–70 years, who conversely had a decreased humoral response, compared with younger people, after the second dose.
Materials and Methods
Study design and population
The study included 1,541 HCW (976 females and 565 males) recruited at the Sant'Andrea Hospital of Rome, Italy, from January 2021 to November 2021, who underwent BNT162b2 (Biontech/Pfizer) vaccination and who did not have COVID-19 infection before or during the study period. A postvaccination volunteer serological screening was performed at 3, 12, and 24 weeks after second dose (T1, T2, and T3) and at 3 weeks after booster dose (T4). All participants completed the primary vaccination cycle between January 2021 and February 2021 and received the booster dose between October 2021 and November 2021. COVID-19 infection prior or during the study period was excluded by determination of serum anti-Nucleocapsid IgG. The study was conducted in accordance with the Declaration of Helsinki, and was approved by the Ethical committee of Sapienza University of Rome (reference number 5773_2020).
Serological assays
Serum concentration of anti-Spike and anti-Nucleocapsid IgG were determined by the chemiluminescent microparticle immunoassay Architect IgG SARS-CoV-2 (Abbott Laboratories, Abbott Park, IL), according to the manufacturer's instructions. IgG's concentration is expressed as binding antibody units (BAU)/mL. The upper threshold of quantification was 11,360 BAU/mL.
Statistics
Statistical analysis was performed using the SPSS software, version 25 (IBM Statistics). Normality of data was assessed by the Kolmogorov–Smirnov test. Non-normal data were expressed as median and interquartile range (IQR) and analyzed using test for median difference, nonparametric pairwise Mann–Whitney U test, Kruskal–Wallis test, or Friedman test of difference among repeated measures, as appropriate.
Results
Serum anti-Spike IgG were determined at 3, 12, and 24 weeks after second dose (T1, T2, and T3) and at 3 weeks after booster dose (T4). We obtained data from 1,378 subjects at T1, 1,332 subjects at T2, 1,203 subjects at T3, and 314 subjects at T4. All subjects had at least two measures, 245 subjects had all time-points measures. The median age of the study group was 48 (IQR 36–55, range 21–71) and no statistically significant difference in median age was detected between males and females (48 [IQR 36–56] vs. 47 [IQR 36–54], respectively).
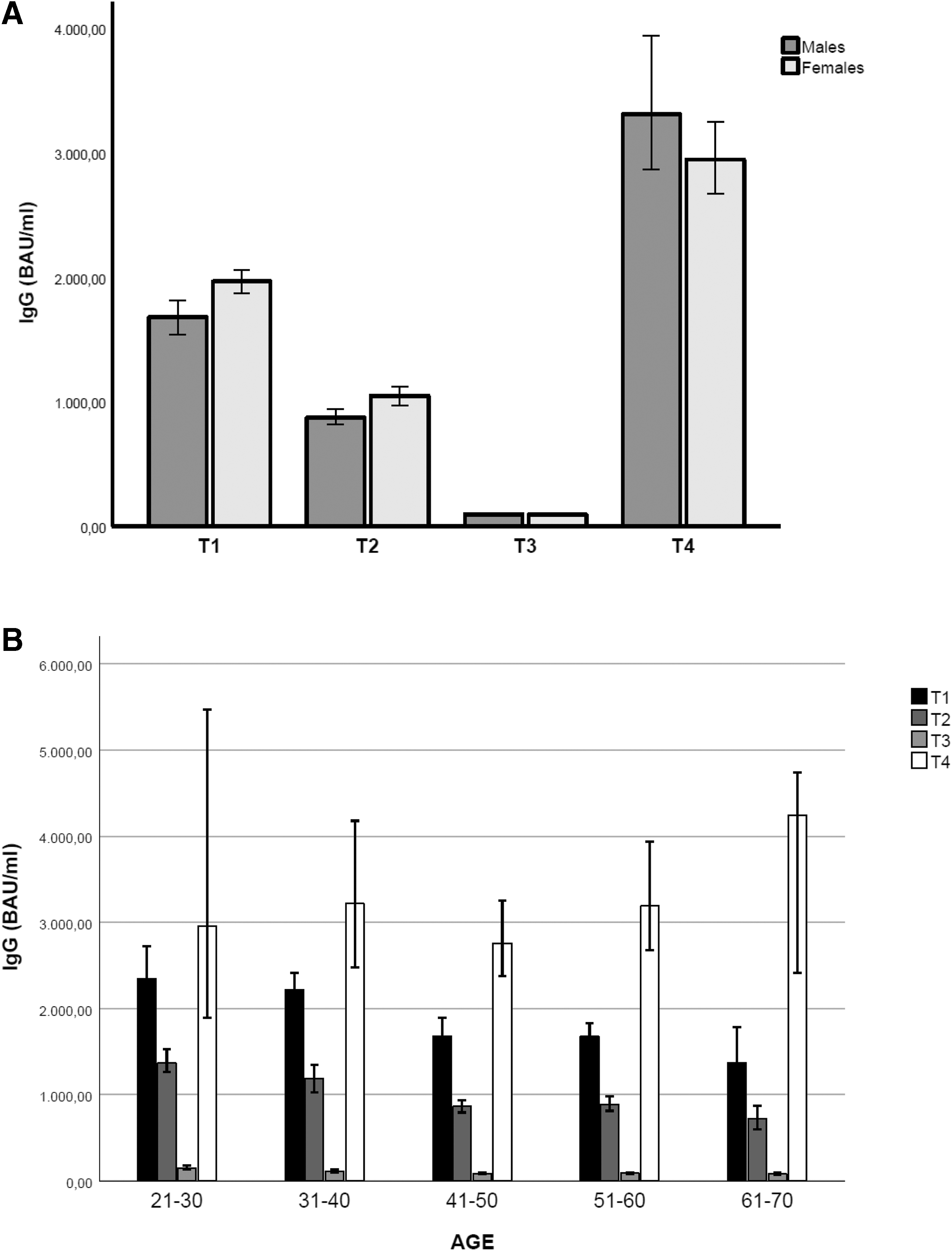
The concentration of serum anti-Spike IgG antibodies declined progressively from 3 to 24 weeks, whereas the booster dose induced about a 60% rise in serum IgG compared with the T1 concentration (Table 1 and Fig. 1). The difference was statistically significant according to the Friedman test of difference among repeated measures (N = 245, mean ranks: T1 = 3.19, T2 = 2.05, T3 = 1.00, T4 = 3.76) χ 2 = 662.04, p < 0.0001).
Serum Anti-Spike IgG Concentrations Expressed as BAU/ml, at T1, T2, T3, and T4
Bold indicates statistical significance.
Data are reported as median (interquartile range).
Mann–Whitney U test.
Kruskal–Wallis test.
BAU, binding antibody units.
A slight but statistically significant sex-related difference in antibodies serum concentration at T1 and T2, but not at T3 and T4, was detected by Mann–Whitney U testing (mean ranks T1: 713.64 vs. 649.553; T2: 691.46 vs. 623.23; T3: 607.29 vs. 591.14; T4: 157.55 vs. 157.4), with a greater IgG titer in females compared with males (Table 1 and Fig. 1A).
Stratification of the study group in 5 age classes by decades (21–30 to 61–70) allowed to detect age-related differences in the dynamics of IgG production. As shown in Table 1 and Figure 1B, in all groups the serum IgG titers decreased over time and was almost completely erased at T3. Kruskal–Wallis test (Table 1) showed that the age was related with the absolute IgG level at T1, T2, and T3 (increased age and lower IgG titer). However, after the booster dose (T4), all groups had a pronounced increase in serum IgG level, leading to similar antibodies titers among all age groups (Table 1 and Fig. 1B).
Discussion
Time-course decrease in humoral response elicited by anti-COVID-19 vaccination (5) has been a disappointing fact, since the duration of the SARS-COV-2 pandemic is extending beyond the expected, with a diffusion rate greatly enhanced by the more infectious Omicron variant of concern (VOC) and the actual possibility of novel VOCs. COVID-19 is more severe in the elderly (4,9) and, moreover, older people have shown an impaired immunological response to the primary vaccination series (7), as also confirmed by our data. The third vaccine dose has proven to be effective in preventing severe disease (3,11), but the duration of such efficacy will be established over time.
In this study, we report that although after two vaccine doses the serum IgG level shows age dependence over time (Table 1), 3 weeks after administration of the booster dose, the BNT162b2 mRNA vaccine induces a similar amplification of serum anti-Spike IgG for all age classes including subjects aged 61–70 (Table 1 and Fig. 1). Results are consistent with other studies, suggesting that the extent of the benefits from the third vaccine dose is larger in the elderly, who generally present increased risk of severe COVID-19.
Conclusions
Booster vaccination has proven to be effective to maintain protection from severe COVID-19. Stratified evaluation of its benefits could deeply contribute to plan right allocation of vaccine resources, especially considering that low-income countries have limited access to vaccine compared with high-income countries.
Footnotes
Authors' Contributions
Conceptualization by G.S., M.S., P.A., A.M., L.M., and M.B.; data curation by G.S., G.G., O.D.L.,
Authorship Confirmation Statement
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the study to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.