
Abstract
Lymphocytes are the main orchestrators that regulate the immune response in SARS-COV-2 infection. The exhaustion of T lymphocytes is a contributing factor to lymphopenia, which is responsible for the COVID-19 adverse outcome. However, it is still not demonstrated on a large scale, including cancer patients. Peripheral blood samples were obtained from 83 SARS-CoV2 infected cancer patients, and 29 COVID-19 infected noncancer patients compared to 28 age-matched healthy controls. Lymphocyte subsets were assessed for CD3, CD4, CD8, CD56, PD-1, and CD95 using flow cytometry. The data were correlated to the patients' clinical features, COVID-19 severity and outcomes. Lymphopenia, and decreased CD4+ T cells and CD8+ T cells were significantly observed in COVID-19 cancer and noncancer patients compared to the control group (p < 0.001, for all). There was a significantly increased expression of CD95 and PD-1 on the NK cells, CD4+ T cells, and CD8+ T cells in COVID-19 cancer and noncancer patients in comparison to the control group. The increased expression of CD95 on CD8+ T cells, as well as the increased expression of PD-1 on CD8+ T cells and NK cells are significantly associated with the severity of COVID-19 infection in cancer patients. The increased expression of CD95 and PD-1 on the CD4+ T cells, CD8+ T cells, and NK cells was observed significantly in nonsurviving patients and those who were admitted to the intensive care unit in COVID-19 cancer and noncancer patients. The increased expression of PD-1 and CD95 could be possible prognostic factors for COVID-19 severity and adverse outcomes in COVID-19 cancer and noncancer patients.
Introduction
The coronavirus disease pandemic 2019 (COVID-19) originated from a novel coronavirus called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). COVID-19 infection was first described in December 2019 in Wuhan, China, and then spread worldwide, which overwhelmed health care systems (Jacob et al, 2021). The pathophysiology of COVID-19 has not been determined precisely yet. However, multiple reports suggest that the degree of immune dysfunction could be responsible for the outcome of COVID-19 (Li et al, 2020; Pezeshki and Rezaei 2021; Song et al, 2020).
Lymphocytes are the orchestrators that regulate the immune response, as they are involved in the cellular and humoral immune response. In addition, it had been proposed that COVID-19 pathogenesis could result from the exhaustion of T lymphocytes and induction of cytokine storm (Luo et al, 2021). Recently emerged reports highlighted the alterations occurred in lymphocyte subsets, including T-helper (CD4+) and T-cytotoxic (CD8+T) cells, as well as natural killers (NK), and their implication on the prognosis of COVID-19 (Razavi et al, 2021; Rezaei et al, 2021; Wang et al, 2020). This lymphocyte alteration might be the core reason for altered immune response and subsequently the decimal morbidities and mortality in COVID-19 infection.
The programmed death (PD-1) molecule is one of the CD28 receptor superfamily. The PD-1 is expressed on activated T lymphocytes to inhibit their effector functions and their proliferation through binding to its ligand PD-L1. The overexpression of PD-1 is a clue for severe antigenic stimulation and contributes to T cell exhaustion and dysfunction (Badoual et al, 2013). Thus, constructing targeted therapy against PD-1 (Nivolumab) was proposed as a treatment protocol in many diseases including lung cancer, head and neck malignancies, and hepatocellular carcinoma (Badoual et al, 2013; Cui et al, 2020; Feng et al, 2017). Lately, anti-PD-1 has been introduced as a potential therapeutic target for SARS- Co-V2 infection (Awadasseid et al, 2021).
The CD95 (FAS) is an extracellular protein death receptor that is recognized as a member of the tumor necrosis factor family. It mediates cellular apoptosis through activation of the caspases of the apoptotic program, which results in cleavage of the intracellular component and subsequently cellular execution (Sharma et al, 2000).
Immunocompromised patients with COVID-19 infection are more susceptible for profound consequences as hospitalization, intensive care admission (ICU), mechanical ventilation, and increased incidence of mortality. Cancer patients are considered an extremely vulnerable group due to the immunosuppression status provoked by either the cancer itself or the cancer therapy, as well as the presence of associated comorbidities (Jacob et al, 2021; Pathania et al, 2021; Zhang et al, 2021).
Our knowledge of evaluating the immune status in COVID-19-infected cancer patients needs more studies. Therefore, in this study, we tried to assess the role of the immunological response in the disease progression and the clinical outcome in COVID-19 cancer patients. The lymphocyte subsets in the form of CD4+, CD8+, CD3+, and NK in association with PD-1 and CD95 were assessed in the peripheral blood of COVID-19 cancer patients and COVID-19 noncancer patients in relation to the normal healthy control. The data were correlated to the COVID-19 severity, ICU admission, and survival in all participated individuals. This will allow for better follow-up of the patients and could help for finding a new therapeutic regimen for COVID-19 patients, especially those suffering from accompanying malignancy.
Methods
This is a retrospective cohort study that included 83 COVID-19 cancer patients, and 29 COVID-19-infected noncancer patients, compared to 28 normal healthy controls. The cancer patients were diagnosed and treated at the National cancer institute (NCI), Cairo University, during the period from January 2021 till May 2021. The COVID-19 noncancer patients were included from the health care providers or their family members, who proved to be positive for COVID-19 infection, while the normal healthy volunteers were presented to the hospital for blood donation and proved to be negative for COVID-19 by RT-PCR.
All patients were confirmed for COVID-19 infection through viral detection by real-time PCR, in addition to the clinical and radiological assessment.
All the included patients were newly diagnosed with cancer at the time of the study. Patients with hematological malignancies in the form of acute lymphoblastic B, T cell lymphoma, or non-Hodgkin lymphoma were in the induction phase of chemotherapy (before disease evaluation), while those with solid tumors, including soft tissue sarcomas, Ewing's sarcoma, and gastrointestinal tumors, administrated neoadjuvant chemotherapy in their induction phase (intensive chemotherapy).
The study protocol was approved by the ethics committee of the NCI, Cairo University. All samples were obtained after informed consent according to the 2011 Helsinki guidelines.
Flow cytometry analysis
Peripheral blood samples (5 mL) were obtained from all participants on EDTA tubes. Samples were stained and acquired within 2 h of drawing, where bulk lysis was performed to detect the lymphocyte subsets. The isolated lymphocytes were assessed for immunophenotyping using anti-human monoclonal antibodies for CD4 (FITC) clone (13B8.2), CD8 phycoerythrin clone: B9.11 (PE), CD3 (PE-cy5,5) clone: UCHT1, all were purchased from Beckman Coulter, while CD56 (FITC) clone: NCAM16.2, FAS (CD95, APC) clone: DX2, and PD-1 (CD279, PC7) clone: EH12.1 were purchased from Becton Dickson. Matched isotype control was used to set the cutoff. Each sample was divided into two tubes, the first tube stained with CD4-FITC, CD8-PE, CD3-PE-cy.5.5, PD1- PC7, and CD95-APC. The second tube was stained with CD56-FITC, CD3-cy5.5, PD1- PC7, and CD95 (Fas, APC) according to the manufacturers' instructions.
All tubes were incubated in dark for 20 min, and then lysis was done by adding ammonium chloride for 5 min. After that, the tubes were centrifuged for 500 g, washed with phosphate buffer saline, and recentrifuged. Samples were acquired for at least 20,000 events and daily QC was performed before running the tested tubes. The immunophenotyping was performed using the cytometer (Becton Dickinson, BD, FACS Canto II) for acquisition and analyzed by BD FACSDiva 8.0.2.
Gating strategy
The Boolean Sequential gating strategy was used; first, gating on low forward side scatter region was selected and applied on the CD3+ CD4+ population. Then gating on CD4+ PD-1 and CD4+ CD95+ was applied. Second, CD8+ CD3+ cells were chosen for gating on CD8+ PD-1+ and CD8+CD95+. For the NK selection, a low forward side scatter region was obtained and CD56+ CD3− was selected for gating on CD56+ PD-1+ and CD56+ CD95+ (Fig. 1).
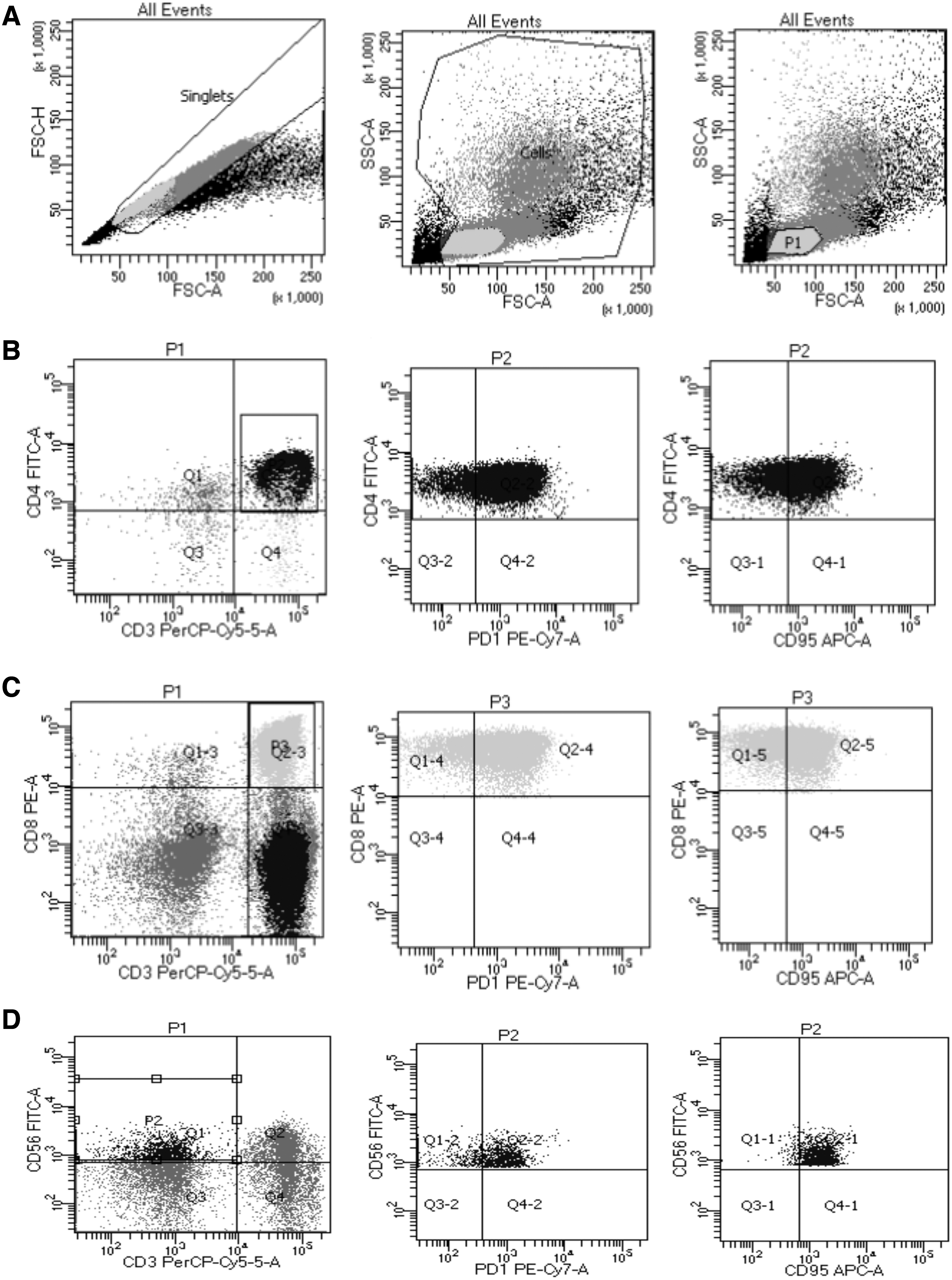
Detection of CD95 and PD-1 expression on peripheral blood of COVID-19-infected patient.
Assessment of interleukin-6
Interleukin 6 (IL-6) was assessed in the serum of patients and healthy controls using the enzyme-linked immunosorbent assay technique, according to the manufacturer's instructions (BT LAB, Cat. no. E0090Hu, China). The data were assessed using Bio Tek ELx808 microplate reader.
Statistical analysis
The statistical analysis was performed using a statistical software package (SPSS, Inc., version 22.0; Chicago, IL). The qualitative data were presented as frequencies and percentages, while the quantitative data were presented as mean and standard deviation (SD), or median and interquartile range (IQR) according to the used normality tests. Comparisons between patients' groups were done using ANOVA or Kruskal–Wallis test with the appropriate post hoc tests. The Mann–Whitney test or the T-independent test was used to assess the association of T cell subsets, PD1, CD95, and the patients' outcomes. All p values were two tailed, and it was considered statistically significant if p < 0.05.
Results
The first group represented the COVID-19-infected cancer patients (83 patients), which formed of 48 (57.8%) males and 35(42.2%) females. Their age ranged from 5 to 71 years with a median of 38 years. Thirty-seven (44.6%) patients were diagnosed with hematological malignancies versus 46 (55.4%) patients diagnosed with solid tumors. There were 25 (30.1%) patients who showed disease remission, while 58 (69.9%) showed progressive disease. The severity of COVID-19 varied as follows: mild in 33 (39.8%) patients, moderate in 24 (28.9%) patients, and severe in 26 (31.3%) patients. There were 25 (30.1%) patients admitted at the ICU, where 16 (19.3%) of them required mechanical ventilation, and death occurred in 15 (18.1%) patients (Table 1). In addition, patients with solid tumors had a significantly progressive disease course and relative lymphopenia compared to those with hematological malignancies (p = 0.03 and 0.006, respectively, Table 2).
Clinical Features of the Assessed COVID-19 Cancer and COVID-19 Noncancer Patients
NA, not applicable.
Illustration of the Clinical Features and the Expression of the Assessed T Cell Subsets Within the COVID-19 Cancer Patients
Bold value indicates statistically significant at p < 0.05.
The second group represented the COVID-19-infected noncancer patients (29 patients). It consisted of 16 (55.2%) males and 13 (44.8%) females. Their age ranged from 9 to 72 years, with a median age of 32 years. The COVID-19 presentation varied as follows: mild in 14 (48.3%) cases, moderate in 6 (20.7%) patients, and severe in 9 (31%) patients. There were 10 (34.5%) patients admitted to the ICU, where 8 (27.6%) of them needed mechanical ventilation and died. There was no significant difference between the two groups of COVID-19 patients regarding the previously described clinical data (Table 1).
The third group formed of 28 healthy control subjects: 10 pediatrics (6 males and 4 females) with a median age of 10 years (range: 5.5–16 years) and18 adults (10 males and 8 females) with a median age of 35.5 years (range: 19–51 years).
Differential expression of T cell subsets among the patients' groups
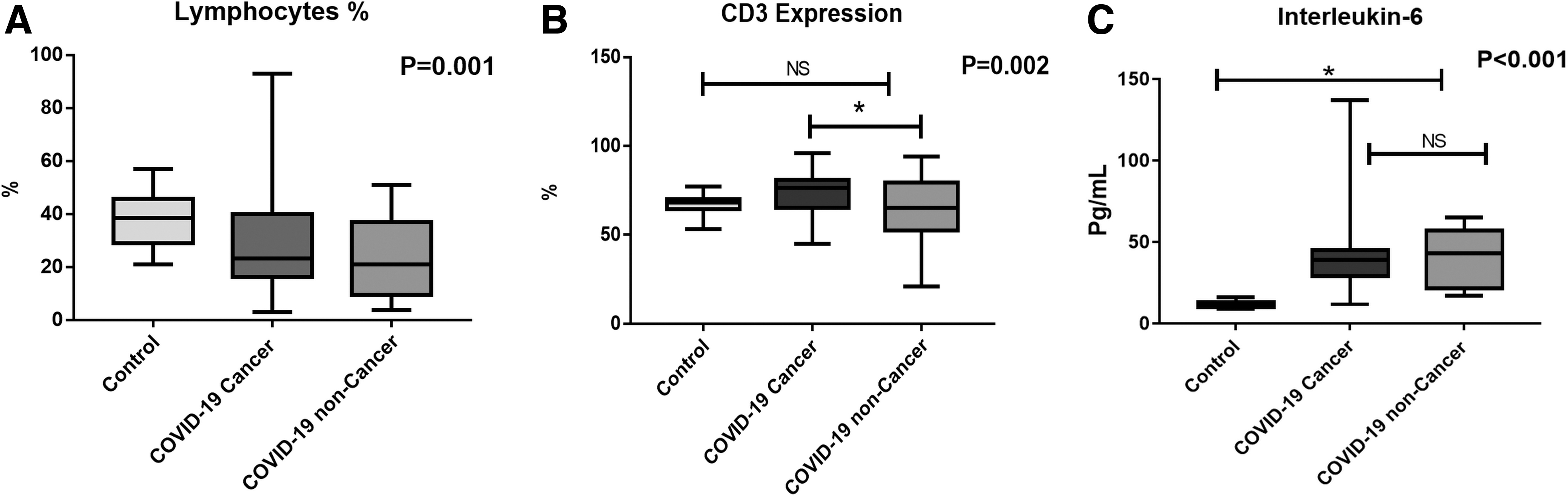
There was a significant decrease in the absolute and relative lymphocyte count in COVID-19 patients (cancer and noncancer) compared to the control healthy group (p < 0.001 and p = 0.001, respectively, Fig. 2A). The CD3+ cells were significantly decreased in COVID-19 noncancer patients compared to the COVID-19 cancer group [(64 ± 18.7) vs. (73.8 ± 12.4), p = 0.003], while there was no significant difference between the normal control group and COVID-19 cancer patients or COVID-19 noncancer patients (p = 0.057 and p = 0.698, respectively, Fig. 2B).
Comparison between the healthy controls, COVID-19 cancer patients, and the COVID-19 noncancer patients regarding
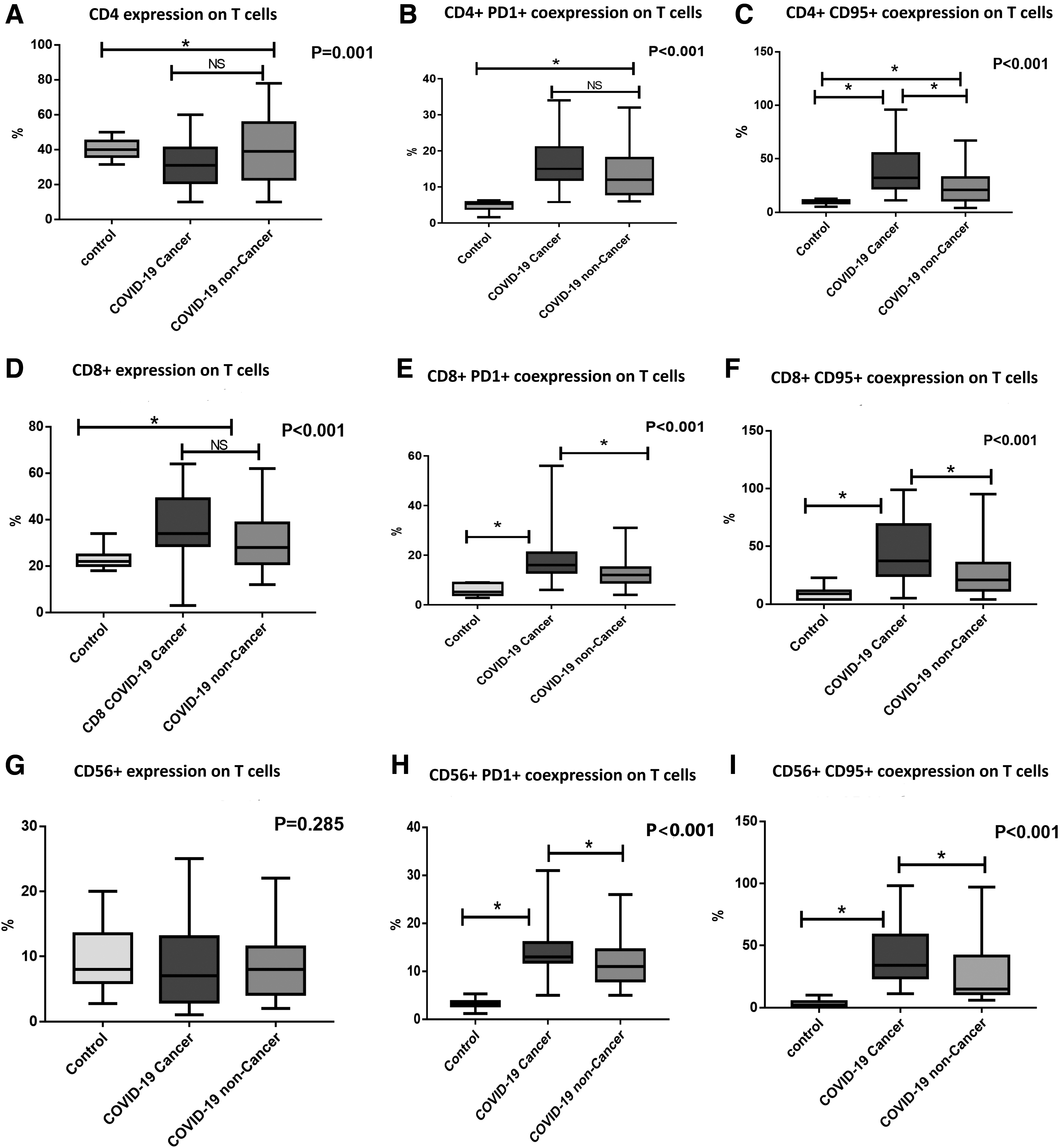
The CD4+ T cells were significantly decreased in COVID-19 cancer patients (30.2 ± 11) compared to the COVID-19 noncancer group (39.9 ± 18.8, p = 0.007) and the control group (40.4 ± 5.3, p = 0.005), while there was no significant difference between the COVID-19 noncancer patients and the control group regarding the CD4 expression on T cells (p = 0.989, Fig. 3A). While concerning the absolute CD4+ T cell count, there was a significant decrease in COVID-19 cancer patients [0.39 (range: 0.01–3.5)], compared to COVID-19 noncancer patients [58 (range: 5–172)] and the control group [1129 (range: 501–1606), p < 0.001].
The expression of T cell subsets;
T lymphocytes co-expressing CD4+PD1+ were significantly decreased in the control group (4.6 ± 1.4) compared to the COVID-19 cancer (16.5 ± 4.9) and noncancer patients (13.7 ± 6.9), p < 0.001, (Fig. 3B), while cells co-expressing CD4+ CD95+ were significantly increased in COVID-19 cancer patients and COVID-19 noncancer patients compared to the control group [34 (range: 11.2–96), 21 (range: 3.9–67), and 10.1 (range: 5–12.5), respectively; p < 0.001, Fig. 3C].
Regarding the frequency of T cells expressing CD8, it was significantly increased in COVID-19 cancer patients and COVID-19 noncancer patients compared to the control group [36 (3–64), 28 (12–62), and 22 (18–34), respectively, p < 0.001, Fig. 3D], while there was a significant decrease in the absolute CD8+ T cell count in COVID-19 cancer patients [0.49 (range: 0.02–1.9)], compared to COVID-19 noncancer patients [40 (range: 7.6–285)] and the control group [590 (range: 328–1100), p < 0.001].
The T cells co-expressing CD8+PD1+ were significantly increased in COVID-19 cancer patients compared to the COVID-19 noncancer patients and the control group [17 (9–56), 12 (4–31), and 5.15 (2.8–9.1), respectively, p < 0.001, Fig. 3E]. Similarly, CD8+ CD95+ co-expression was significantly increased in COVID-19 cancer patients and COVID-19 noncancer patients compared to the control group [43 (6–99), 21 (4.2–95), and 9.1 (4–22.8), respectively, p < 0.001, Fig. 3F].
There was no significant difference between the assessed patients' groups regarding CD56 expression on NK cells (p = 0.285, Fig. 3G). However, CD56+PD1+ was significantly expressed in COVID-19 cancer patients in comparison to COVID-19 noncancer patients and the control group [13 (range: 9–31), 11 (range: 5–26), and 3.35 (range: 1.2–5.3), respectively, p < 0.001, Fig. 3H]. Similarly, co-expression of CD56+CD95+ was significantly increased in COVID-19 cancer patients compared to COVID-19 noncancer patients and the control group [37 (range: 12–98), 15 (range: 6–97), and 2.15 (range: 1–10), respectively, p < 0.001, Fig. 3I].
Moreover, there was no significant difference between patients with solid tumors and those with hematological malignancies regarding the expression levels of T cell subsets and IL-6 (Table 2).
Association of T cell subsets with the severity of COVID-19 infection in COVID-19 cancer and COVID-19 noncancer patients
COVID-19-infected cancer patients with severe presentation showed increased PD-1 co-expression with CD8+ cells compared to mild or moderate cases [20 (11–56) vs. 15.5 (6–31), respectively, p = 0.042]. Similarly, severe COVID-19 cancer cases showed increased CD95 co-expression with CD8+ cells in comparison to mild or moderate cases [57 (6–98), respectively, p = 0.048]. In addition, the expression of PD1 on NK cells was increased in severe COVID-19 cancer patients compared to mild and/or moderate cases [14 (9–31) and 12 (5–26), respectively, 0.045, Table 3].
Association of T Cell Subsets with the COVID-19 Severity in COVID-19 Cancer and COVID-19 Noncancer Patients
Bold value indicates statistically significant at p < 0.05.
Regarding the COVID-19 noncancer patients, they showed a significant decrease in the absolute lymphocytes, relative lymphocytes, and absolute CD4+ and absolute CD8+ T cell counts in severe cases compared to moderate or mild cases [p < 0.001 for all]. Patients with severe COVID-19 infection showed increased expression of PD-1 [19 (range: 11–32)] and CD95 [39 (range: 20–67)] on the CD4+ lymphocytes compared to those with mild or moderate COVID-19 infection [PD1: 10 (6–17) and CD95: 12.5 (3.9–56), p < 0.001 for all].
Similarly, the expression of PD1 and CD95 was significantly increased on CD8+ lymphocytes in COVID-19 severe cases [18 (9–31) and 54 (23–95), respectively], compared to those with mild or moderate COVID-19 presentation [9.8 (4–15) and 13.5 (4.2–43), respectively, p < 0.001 for both]. Also, NK cells showed a significant increase in the expression levels of PD1 and CD95 in COVID-19 severe cases [17 (9.7–26) and 54 (8–97), respectively], compared to COVID-19 mild or moderate cases [9.3 (5–21) and 13 (6–43), respectively], with a significant level of p = 0.001 and 0.007, respectively (Table 3).
Association of T cell subsets with the survival in COVID-19 cancer and COVID-19 noncancer patients
There was a significant association between the expression of PD1 and CD95 on CD4 lymphocytes and the increased incidence of death in COVID-19 cancer patients (p = 0.010 and p < 0.001, respectively). Also, the expression of PD1 and CD95 on CD8+ lymphocytes increased significantly in nonsurvivors compared to the survivor COVID-19 cancer patients (p = 0.001 and p = 0.003, respectively). Similarly, the nonsurvivor COVID-19 cancer patients showed increased expression of PD1 and CD95 on the NK cells in comparison to the survivor COVID-19 cancer group (p = 0.001 for both, Table 4).
Association of T Cell Subsets with the Survival in COVID-19 Cancer and COVID-19 Noncancer Patients
Bold value indicates statistically significant at p < 0.05.
Regarding the COVID-19 noncancer group of patients, inferior survival outcomes of patients associated significantly with the increased levels of absolute lymphocyte count (p < 0.001), relative lymphocyte (p < 0.001), CD3+ cells (p = 0.003), absolute CD4+ lymphocyte count (p < 0.001), and absolute CD8+ lymphocyte count (p < 0.001), in addition to the increased expression of PD1 and CD95 on CD4+ lymphocytes (p < 0.001, for both), CD8+ lymphocytes (p < 0.001, for both), and NK cells (p < 0.001 and p = 0.001, respectively), which increased significantly in the nonsurvivors compared to the survivor COVID-19 noncancer patients (Table 4).
Association of T cell subsets with ICU admission in COVID-19 cancer and COVID-19 noncancer patients
There was a significant association between the expression of PD1 and CD95 on CD4 lymphocytes and the increased incidence of ICU admission in COVID-19 cancer patients (p < 0.001, for both). Also, the expression of PD1 and CD95 on CD8+ lymphocytes increased significantly in patients who were admitted to the ICU compared to the COVID-19 cancer patients who were not admitted to the ICU (p < 0.001, for both). Similarly, the expression of PD1 and CD95 on the NK cells increased significantly in COVID-19 cancer patients who needed ICU admission compared to those who were not admitted to the ICU (p = 0.001 for both, Table 5).
Association of T Cell Subsets with ICU Admission in COVID-19 Cancer and COVID-19 Noncancer Patients
Bold value indicates statistically significant at p < 0.05.
For the COVID-19 noncancer patients, the admission to the ICU associated significantly with the increased levels of absolute lymphocyte count, relative lymphocyte, absolute CD4+ lymphocyte count, and absolute CD8+ lymphocyte count (p < 0.001, for all), in addition to the increased expression of PD1 and CD95 on CD4+ lymphocytes (p < 0.001 and p = 0.001, respectively), CD8+ lymphocytes (p < 0.001, for both), and NK cells (p = 0.003 and p = 0.014, respectively), which increased significantly in patients admitted to the ICU compared to the COVID-19 noncancer patients who were not admitted to the ICU (Table 5).
The interleukin-6 level in COVID-19 cancer and noncancer patients
The serum level of IL-6 was significantly increased in COVID-19 cancer patients and COVID-19 noncancer patients in comparison to the control group [38.3(11.7–137), 43 (9–16) pg/mL, respectively, p < 0.001, Fig. 2C]. The IL6 level increased significantly in the noncancer patients with severe COVID-19 disease compared to those noncancer patients with mild or moderate COVID-19 infection [57 (17–45) pg/mL, respectively, p = 0.001, Fig. 4A].

Association of interleukin-6 expression and;
However, there was no significant difference in the serum level of IL6 according to the severity of COVID-19 infection in the COVID-19 cancer patients [43.2 (11.7–137) pg/Ml in severe cases vs. 36.6 (20–74) pg/mL in mild or moderate cases, p = 0.777, Fig. 4B]. The serum level of Il-6 increased significantly in the nonsurvivor COVID-19 noncancer patients [57 (32–65) pg/mL], in comparison to the survivor group [21 (17–45) pg/mL, p = 0.001, Fig. 4C]. However, there was no significant difference between the survivor and nonsurvivor COVID-19 cancer patients regarding the IL-6 serum level [36.6 (20–137) pg/mL compared to 38 (11.7–134) pg/mL, respectively, p = 0.820, Fig. 4D].
Similarly, the COVID-19 noncancer patients who were admitted to the ICU showed a significantly increased IL-6 level in comparison to those who did not need ICU admission [57 (32–65) pg/mL and 21 (17–45) pg/mL, respectively, p = 0.001, Fig. 4E]. However, there was no significant association between the IL-6 serum level and ICU admission in COVID-19 cancer patients [39 (11.7–134) pg/mL in the ICU admitted patients, compared to 35 (20–137) pg/mL in the patients who were not admitted to the ICU, p = 0.949, Fig. 4F].
Correlation among T cell subsets and IL-6 expression in the assessed patients' groups
There was a significant correlation between IL-6 level and increased expression of PD1 and CD95 on the surface of CD4+ lymphocytes (r = 0.740, p < 0.001 and r = 0.596, p < 0.001, respectively), CD8+ lymphocytes (r = 0.684, p < 0.001 and r = 0.656, p < 0.001, respectively), and NK cells (r = 0.737, p < 0.001 and r = 0.737, p < 0.001, respectively, Table 6).
Correlation Among T Cell Subsets and IL-6 Expression in the Assessed Patients' Groups
P, significance level <0.05; r, Spearman correlation coefficient.
Discussion
Lymphopenia is a key feature of COVID-19 infection, which might influence the outcome of patients. Although the immune dysfunction and the etiology of lymphopenia have not been understood yet, the degree of lymphopenia has been categorized as a fundamental predictor of the severity of COVID-19 cases (Hanna et al, 2020). Upregulation of lymphocyte exhaustion molecules such as PD-1, as well as the apoptosis molecules CD95, might be claimed as a contributing factor to lymphopenia (Bellesi et al, 2020). However, it is still not demonstrated on a large scale, including cancer patients.
In line with that reported in the literature, this study demonstrated a significant decrease in the absolute and relative lymphocyte counts in both cancer and noncancer COVID-19 patients' groups compared to the control healthy group. That is an indicative sign of a disturbed immune function in COVID-19 infection (Diao et al, 2020; Eissa et al, 2021; Nile et al, 2020; Nooh et al, 2021; Tan et al, 2020; Vardhana and Wolchok 2020). The data of the assessed COVID-19 noncancer patients showed that lymphopenia associated significantly with the severity of COVID-19 infection, ICU admission, and incidence of death. These data are consistent with many published studies reporting that lymphopenia is significantly observed in severe COVID-19 infection (Diao et al, 2020; Zhao et al, 2020), [23, 24], and in nonsurviving patients (Nile et al, 2020).
Therefore, lymphopenia could be considered a sensitive biomarker for COVID-19 severity in noncancer patients (Tan et al, 2020; Toor et al, 2021; Zhao et al, 2020). However, our data revealed that the reported lymphopenia had no significant impact on the patients' outcomes in COVID-19 cancer patients. This might be explained by the disturbed immune function in cancer patients owing to the effects of the cancer itself, or the anticancer treatment, which affect the immune competence of those patients.
These data showed that there was a significant decrease in the absolute value of CD4+ T cell and CD8+ T cell counts with increased IL6 levels in COVID-19 cancer patients and COVID-19 noncancer patients compared to the control group. In addition, these disturbed levels of CD4+ T cell subsets, CD8+ T cell subsets, and IL6 levels associated significantly with the severity of COVID-19 infection, ICU admission, and increased incidence of death in the group of COVID-19 noncancer patients.
These data are in agreement with Wang et al (2020), who reported the presence of lymphopenia, decreased CD4+CD3+ cells, CD8+CD3+ cells, and CD56+CD16+ NK in COVID-19 cases compared to the healthy controls. Also, they reported that severe cases with COVID-19 pneumonia had lower levels of CD4+CD3+ cells and CD8+CD3+ cells, together with a higher level of IL-6 compared to the mild cases. Therefore, the decrease in the absolute value of CD4+ T cell subsets, CD8+ T cell subsets, and increased IL-6 level could be considered adverse prognostic factors for COVID-19 noncancer patients.
Moreover, our results revealed increased expression of the apoptotic molecule CD95 and the PD-1 (a potential exhaustion molecule) on CD4+ T cells, CD8+ T cells, and NK cells in COVID-19 cancer and noncancer patients compared to normal controls. These data are in concordance with Bellesi et al (2020), who detected a significantly increased expression of CD95 (Fas) and PD-1 on both CD4+ T cells and CD8+ T cells in 42 COVID-19 patients in comparison to the control group.
Similarly, Sabbatino et al (2021) and his teamwork highlighted the role of PD-1/PD-L1 dysregulation on the immune malfunction status, as the overstimulation of PD-1/PD-L1 induced depletion and exhaustion of T lymphocytes, and subsequently might develop a state of anergy or skewed immune condition. This state of anergy produced from increased PD-1 activation on the epithelial cells and monocytes leads to the production of high levels of inflammatory cytokines such as IL-6 and TNF (Sabbatino et al, 2021).
In addition, the upregulation of PD-1 and CD95 associated significantly with the severity of COVID-19 infection, ICU admission, and decimal survival outcome in both COVID-19-infected cancer and noncancer patients. In concordance with these data, Zheng et al (2020) reported a significant increase of PD-1expression on CD4+ and CD8+ T cells in severe cases of SARS-COV-2 infection when compared to the mild case.
On the other hand, cancer patients are considered a high-risk group for the COVID-19 adverse events. This is due to the myelosuppressive and/or the immunosuppressive effect of the type of the co-existing malignancy, as well as the administrated treatment in the form of chemotherapy, radiotherapy, or cytotoxic treatment. In this context, this study showed that the cancer patients infected with COVID-19 were similar to the noncancer COVID-19 patients regarding the presence of lymphopenia, decreased CD4+ T cells and CD8+ T cells, with a significantly increased expression of CD95 and PD-1 on the CD4+ T cells, CD8+ T cells, and NK cells.
However, in the COVID-19 cancer patients, the increased expression of CD95 on CD8+ T cells, as well as the increased expression of PD-1 on CD8+ T cells and NK cells are the only markers associated with the severity of COVID-19 infection. Moreover, those patients showed that increased expression of CD95 and PD-1 on the CD4+ T cells, CD8+ T cells, and NK cells was observed significantly in nonsurviving patients and those who were admitted to the ICU. Therefore, T cell profile activation or exhaustion could be a useful prognostic marker for COVID-19 patients, especially in those who had other life-threatening conditions as in cancer patients, since the co-existence of SARS-COV-2 infection together with the malignancy makes the decision of using intensive anticancer treatment very difficult.
Although IL-6 was significantly increased in cancer patients infected with COVID-19, however, unlike noncancer patients, IL-6 had no significant association with the severity of COVID-19 infection, survival of the patients, or ICU admission. These data are contradictory to that reported by Izcovich et al (2020), that IL-6 is an important prognostic marker for COVID-19 severity. In addition, Kampan et al (2018) reported that IL-6 could be used as a targeted therapy for many cancers, including prostate, colon, renal, lung, ovarian, and multiple myeloma. This discrepancy could be explained by that the cancer patients had a disturbed immune function due to the nature of the malignant disease and the administrated anticancer therapy, together with the associated COVID-19 infection. All these factors could possibly make the cancer patients differ from the other patients regarding the course and the outcome of the SARS-COV-2 viral infection.
In conclusion, this study mounted the implication of increased expression of PD-1 and CD95 in COVID-19-infected cancer and noncancer patients, which are aggravated by the severity of the COVID-19 infection. These markers could have contributed to the exhaustion of T cells. Thus, this raises the rationale for the potential use of ant PD-1 and anti CD95 in COVID-19-infected patients. However, further studies are required to assess extensively other markers contributing to T cell exhaustion.
Footnotes
Authors' Contribution
E.Z.K. put the idea and performed the flow cytometric analysis; L.R. oversighted and took the leadership responsibility for the research activity planning and execution; A.K.B. collected the data, and performed the medical care and the follow-up of patients; H.A.N. performed the hematological and the laboratory work of the patients; H.R. performed the flow cytometric analysis of data; M.S.A. shared in the laboratory work, analyzing the data, and writing and revising the article; M.K. supervised and revised the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by Cairo University, fund No. 10/2020.