
Abstract
Middle East respiratory syndrome coronavirus (MERS-CoV) causes viral pneumonia disease in humans. The close contact with camels and drinking milk may cause MERS-CoV transfer to humans. This study was designed to detect the existence of MERS-CoV in camel milk samples collected from healthy animals of various barns located around Saudi Arabia. Camel milk samples were examined for MERS-CoV RNA by real time-quantitative polymerase chain reaction, also enzyme-linked immunosorbent assay was performed to detect IgG antibodies directed against Middle East respiratory syndrome receptor-binding domain. Among 83 camel milk samples tested, the result showed that seven samples (8.4%) were positive for MERS-CoV RNA, whereas 40.9% of camel milk samples had antibodies directed against MERS-CoV. The findings indicate that some regions (East and South part) are characterized by a high incidence of viral antibodies. The Southwestern region displayed the lowest infection rates. Among the camel breeds, the lowest positivity for detection of MERS-CoV RNA and IgG antibodies was found in Sahilia. This could be related to a higher resistance to viral infection of the breed Sahilia and/or to the geographical origin of the camels sampled in the study. This needs to be more explored to reduce spread of infection and also to understand the underlying reasons. The presence of viral RNA in camel milk samples warrants for measures to prevent possible foodborne transmission of MERS-CoV through milk consumption.
Introduction
The Middle East respiratory syndrome coronavirus (MERS-CoV) was first detected in 2012 in Saudi Arabia (Zaki et al, 2012). It is characterized by severe viral pneumonia leading to death. By the end of May 2021, a total of 2,574 laboratory-confirmed cases of MERS, including 886 associated deaths (case fatality ratio 34.4%) were reported globally (World Health Organization Regional Office for the Eastern Mediterranean, 2021). Domestic animals and wildlife may be an important cause of viral infection. Dromedary camels were the only species from which antibodies specific to MERS-CoV have been detected after many seroepidemiological studies on camels, cattle, sheep, goats, horses, and poultry in the Arabian Peninsula and the Middle East (Hemida et al, 2013; Meyer et al, 2014; Perera et al, 2013; Reusken et al, 2013a; Reusken et al, 2013b).
Serological evidence of infection of dromedaries from the Arabian Peninsula (Saudi Arabia, United Arab Emirates [UAE], Oman, Qatar, and Jordan) by MERS-CoV has been reported with a seroprevalence in adult animals generally being >90%. Moreover, serological evidence of dromedary infections in Africa (Egypt, Ethiopia, Nigeria, Tunisia, Sudan, and the Canary Islands) were also reported with a similarly high seroprevalence, except Tunisia and Canary Islands, where adult seroprevalence was only 54% and 14%, respectively (Corman et al, 2014; Perera et al, 2013; Reusken et al, 2014a).
Infection by MERS-CoV in the Kingdom of Saudi Arabia and UAE occurs often during winter and spring (Majumder et al, 2014; Oboho et al, 2015). Approximately, from 20 to 200 cases reported every year in the Saudi Arabia (Ministry of Health Report Status, 2020). The camel movement in the Arabian Peninsula may play an important role in MERS-CoV spreading during this period.
The consumption of raw milk is mainly due to the widespread belief that camel milk has preventive and curative properties against many diseases and that boiling milk destroys its nutritional and medicinal value (Shamsia, 2009). Camels were proposed as a source of infection in one human MERS case (Memish et al, 2015; Memish et al, 2014). In a study that reported the discovery of MERS-CoV RNA in camel milk (Hemida et al, 2015), it was not known whether the milk was contaminated or the udder was infected by the regular spread of the virus through the bloodstream. The possibility of a local infection of the udder by infected offspring is also not excluded. Regardless of the ways the virus can enter to milk, these facts support the possibility that raw camel milk can be a source of infection with the MERS-CoV. Very little is known about the potency of camel milk to bear the virus, hence to increase the awareness about raw camel milk as a possible virus vector, the present study was undertaken to screen the presence of MERS-CoV RNA and anti-MERS-receptor-binding domain (RBD) antibodies in camel milk samples.
Materials and Methods
Collection of milk samples
Camel milk samples were collected during the period from May to July from 83 Arabian camels in small rural barns from different cities located around the Kingdom of Saudi Arabia, except the northern region where camel farming is less (Fig. 1). Collection area was geographically divided to four main regions in Saudi Arabia: 22 samples from Central region (Riyadh, Qassim, and Hail), 24 from Western region (Madina, Jeddah, Al Taif, and Makkah), 20 from Southwestern region (AlBaha, ‘Asir, and Jazan) and 17 from the East and South region (Eastern province and Najran) (Fig. 2). The barns were selected based on the abundance of camels and milk, as well as the breeds of camels available in the different areas. Samples were collected from camels belonging to the four main breeds: Majhim (28), Hamra (17), Maghatir (22), and Sahilia (16) (Fig. 1) (Abdallah and Faye, 2012) at different ages. Majhim is black coated with a pointed hump long hair covering the body and long legs. They are originated from north-eastern part of the country and are the best dairy producers of the Kingdom.
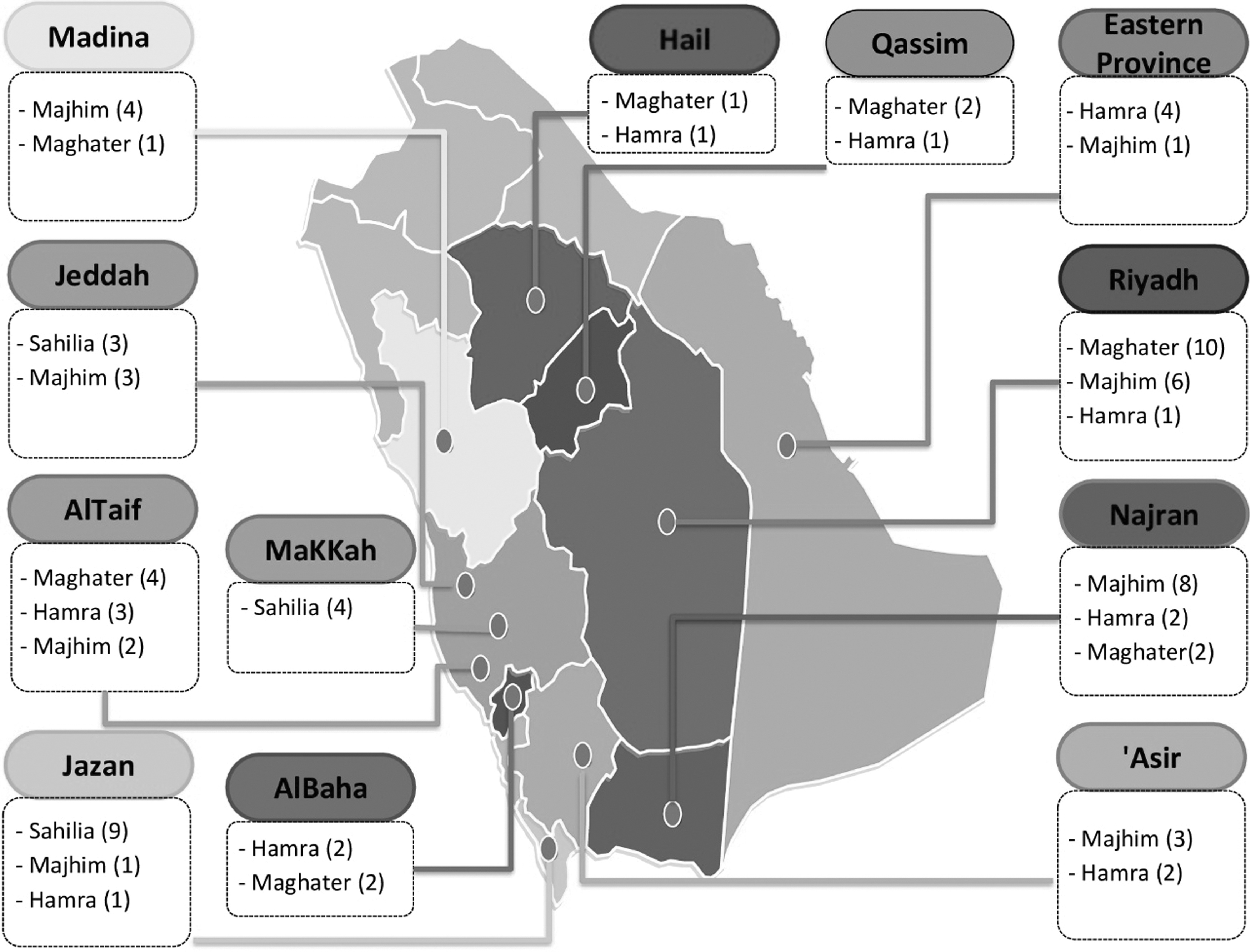
Sample collection sites in Saudi Arabia highlighting different cities and breeds of camels.
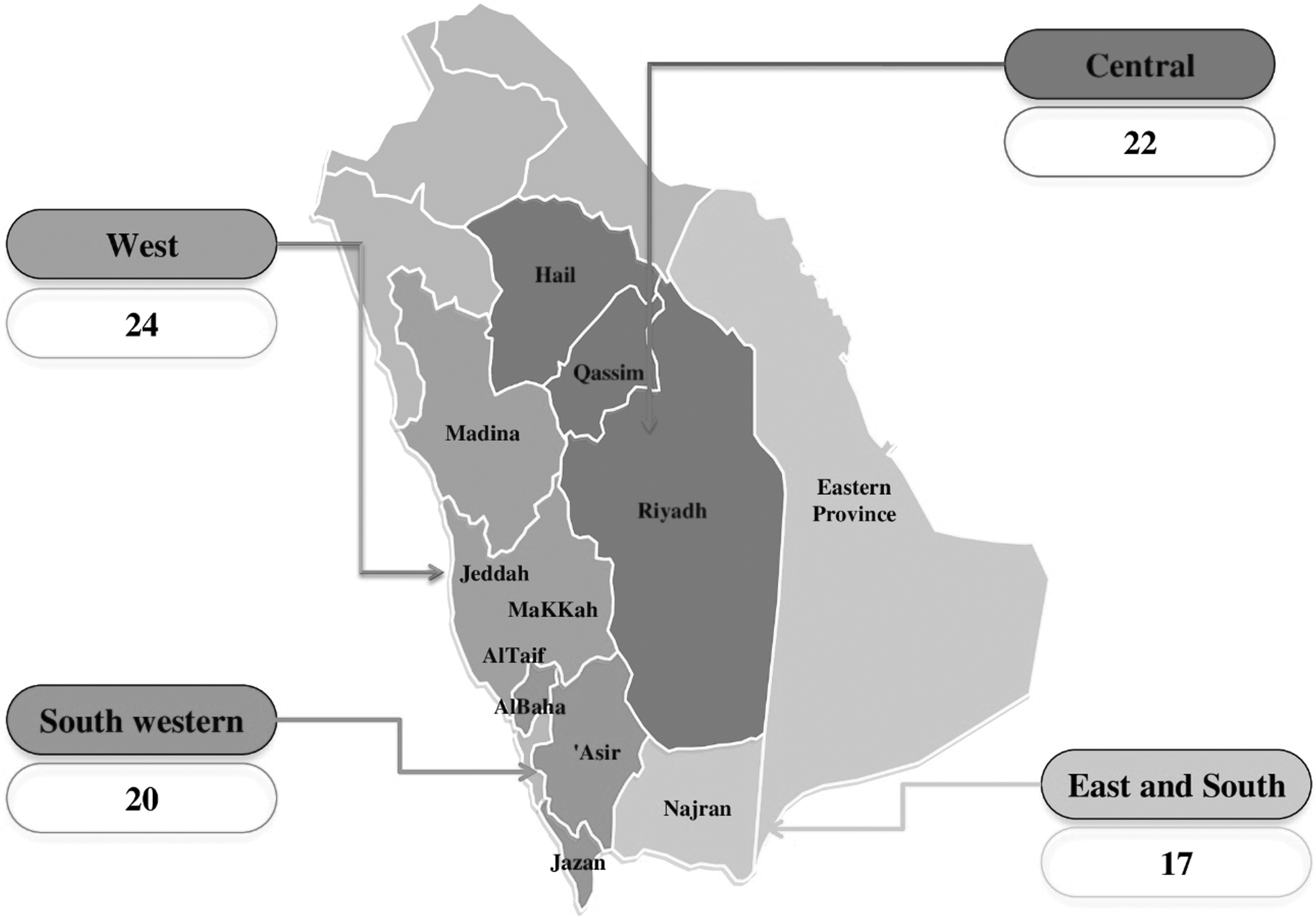
Locations of camel milk samples examined for MERS-CoV from different regions of Saudi Arabia. Total number of camel milk samples collected from each region is indicated. MERS-CoV, Middle East respiratory syndrome coronavirus.
Hamra is medium-size dairy breed with a clear brown coat color. Maghater have a white-yellow coat color. They have pointed ears and low pilosity. Sahilia live along the Red Sea coast and have a red coat color, a small head with a pronounced forehead (Fig. 3). The age of camels was chosen randomly. Young camels between 3 and 5 years of age were 41 and animals older than 6 were 42.

Four selected camel breeds for sample collection.
Milk samples were collected according to the procedure of Suárez-Vega et al (2015) as described below:
The following protocol was used during the sampling process to ensure RNA purification of high yield and quality. Before sampling, milk collection tubes were cleaned with RNaseZap (Sigma-Aldrich) and autoclaved. The udder was cleaned with soap and water and then disinfected with 70% alcohol. Finally, the nipples were cleaned using RNAseZap (Ambion, Austin, TX). Milk from the udder was passed directly into 50-mL RNAse-free tubes. Samples were maintained at 4°C during transport from the farm to the laboratory.
RNA extraction and real time-quantitative polymerase chain reaction for detection of MERS-CoV RNA
RNA was extracted from camel milk samples, according to the manufacturer's instructions using the Fast RNATM ProBlue Kit (MP Biomedicals, China). Prevalence of MERS-CoV in camel milk samples was assessed by real time-quantitative polymerase chain reaction (RT-qPCR) using specific probes for the RNA virus. MERS-CoV primers used for the specific and exclusive in vitro quantification of the coronavirus isolates were designed based on sequences for the Eramus Medical Center strain by targeting envelope protein gene upstream (UpE), which was used for screening and Open Reading Frame 1a was used for confirmation of the MERS-CoV diagnosis (Corman et al, 2012a; Corman et al, 2012b). In short, 5 μL of extracted RNA was transferred to PCR tubes and UpE primers were used for RT-qPCR, which was performed with the Human Coronavirus 2012 (MERS) Kit (GENESIG, Primer design Ltd, UK) according to the manufacturer's protocol.
All samples were run in 48-well reaction plates by PROPLATE48 and analyzed using Prime Pro 48 RT-qPCR system (TECHNE version 5.2.15.0) (Stone, Staffordshire, UK). The reaction conditions were as follows: 55°C for 10 min (reverse transcription), 95°C for 2 min (enzyme activation), 95°C for 10 sec (denaturation), and 60°C for 1 min for 50 cycles (amplification).
Anti-MERS-RBD enzyme-linked immunosorbent assay
The presence of antibodies against the MERS RBD in camel milk samples was detected using an anti-MERS-RBD IgG Enzyme-Linked Immunosorbent Assay (ELISA) Kit (Alpha Diagnostic International, TX). The kit is an indirect ELISA used for the detection and quantification of IgG antibodies directed against MERS-CoV RBD. The ELISA assay was carried out following the manufacturer's instructions. Assay steps were performed at room temperature (Mohd et al, 2016; Müller et al, 2014). In brief, the milk samples were diluted 1:100 in sample diluent to reduce nonspecific binding; the diluted samples were incubated in wells coated with the purified RBD antigen of MERS coronavirus (MERS-RBD). In the case of positive samples, the specific antibodies will bind MERS antigens. A second incubation is carried out by an enzyme-labeled anti-camel IgG horseradish peroxidase conjugate (peroxidase conjugate) stimulating the reaction to detect the bound antibodies. The substrate is then added and its product is detected by fluorescence. The results were read on microplate reader (Randox ELx800, UK)
Data management and statistical analysis
Data were collected from RT-qPCR machine as Quantity of viral RNA, and from ELISA reader as optical density (OD) values. Data were analyzed by the Statistical Package for Social Sciences (SPSS) for Windows version 22.0 (SPSS, Inc., Chicago, IL).
Results
Detection and quantification of MERS-CoV RNA in camel milk samples by RT-qPCR
Among 83 milk samples tested, only 7 camel milk samples (8.4%) contained MERS-CoV RNA as detected by real-time qPCR assays. These positive samples were as follows: 2/22 in Central region (Riyadh, Qassim, and Hail), 4/17 in East and South region (Najran and Eastern province), and 1/24 in West region (AlTaif, Jeddah, Makkah, and Madina). Meanwhile, MERS-CoV RNA was not detected in 20 camel milk samples collected in the Southwestern region (Jazan, Asir, and AlBaha) (Table 1).
The Existence of Middle East Respiratory Syndrome Coronavirus RNA in Camel Milk Samples from Different Regions, Type, and Ages in Saudi Arabia
Between the standard dilutions.
Less than standard dilutions.
Higher than standard dilutions.
MERS-CoV, Middle East respiratory syndrome coronavirus.
The percentage of positivity for detection of MERS-CoV RNA was 10.71% in Majhim, 11.76% in Hamra, and 9.09% in Maghatir breeds of camels. However, there was no viral detection among Sahilia breed samples. This breed is mainly located in Southeastern region. With respect to age of the camels, the percentage of positivity was 9.5 and 7.3% for camels from 3–5 years of age to ≥6 years, respectively (Table 1).
The data for quantitative RT-qPCR revealed the following findings: 4 out of 7 positive samples (Samples19, 20, 22, and 56) displayed RNA quantity in the range of standard dilutions. Higher concentration of RNA was detected in sample 32, which was more than standard dilutions, whereas two samples 53 and 61 has shown lower RNA concentration than the standard dilutions (Table 1). The remaining samples were negative for MERS-CoV RNA.
Detection and quantification of MERS-CoV IgG antibodies through anti-MERS RBD ELISA
The ELISA assay was used to check the presence of anti-MERS-RBD IgG in milk samples. Anti-MERS-RBD IgG was detected in 34 camel milk samples (40.9%) out of 83 samples. Prevalence of antibodies was high in the East and South regions (Najran and Eastern province) (76.47%) followed by West region (AlTaif, Jeddah, Makkah, and Madina) (50%). However, these percentages were lower in Central region (Riyadh, Qassim, and Hail) (27.27%) and Western south region (Jazan, Asir, and AlBaha) (15%) (Table 2). Detection pattern of anti-MERS-CoV antibodies displayed similar tendency to the presence of viral RNA.
Detection of Middle East Respiratory Syndrome Coronavirus IgG Anti-Middle East Respiratory Syndrome-Receptor-Binding Domain in Camel Milk Samples from Different Regions, Type, and Ages in Saudi Arabia
RBD, Receptor-Binding Domain.
Prevalence depending on the camel breed showed that Hamra (64.7%) and Majhim (46.42%) types displayed the highest positivity rates for anti-MERS-RBD IgG followed by Maghatir (36.36%), then Sahilia (12.5%) types (Table 2). With respect to age of the camels, the percentage of positivity was 46.34 and 35.7% for camels from ≥6 years of age to 3–5 years, respectively (Table 2).
Upon comparison of results of RT-qPCR with ELISA assay it was observed that among the 34 camel milk samples, which were positive for anti-MERS-RBD IgG antibodies, only 4 contained MERS-CoV RNA (Table 3). It was also noticed that 3 milk samples that were positive for MERS-CoV RNA did not show anti-MERS-RBD IgG antibodies (Table 3).
Comparison of Detected Positive Samples RNA for Middle East Respiratory Syndrome Coronavirus by Real Time-Quantitative Polymerase Chain Reaction with Anti-Middle East Respiratory Syndrome-Receptor-Binding Domain by Enzyme-Linked Immunosorbent Assay
ELISA, enzyme-linked immunosorbent assay; RT-qPCR, Real time-quantitative polymerase chain reaction.
Discussion
In earlier studies, detection of MERS-CoV in archived serum samples showed a high serum prevalence of MERS-CoV in the tested specimens, which appeared in the 1990s (Hemida et al, 2014b; Reusken et al, 2013b). Consequently, it may indicate the possibility of the circulation of MERS-CoV in dromedary camels before its actual appearance in human as it was first announced in 2012 (Zaki et al, 2012).
The camel milk samples which were broadly collected from various regions of Saudi Arabia included East and South, West, Southwestern, and Central regions. In this study, RNA of MERS-CoV was detected in 7 samples out of 83 (8.4%) through RT-qPCR assays. Among the seven infected samples, four only contained anti-MERS-RBD antibodies. The corresponding camels are infected with the virus without displaying any symptoms. The remaining three samples did not contain anti-MERS-RBD antibodies. This might be explained by the fact that the animals are in the first infection stages. The simultaneous detection of viral RNA and antibodies to MERS-CoV in camel milk samples observed in the present study is in agreement with reports (Aljasim et al, 2020) on the prevalence of MERS-CoV RNA (38.6%) and high seropositivity (70.8%) in slaughtered camels of Riyadh, Saudi Arabia. Camel milk samples containing anti-MERS-RBD IgG without the presence of RNA are indicative of previous exposure to the virus.
The prevalence of MERS-CoV RNA in different regions of Saudi Arabia varied from 23.5% in East and South to 0% in Southwestern. The East and South region seems to display a high positivity rate. This might be explained by the high frequency of camel transport in the region (Hemida et al, 2017). This is in line with reports of camel swab contaminations in UAE being the highest at the Saudi border (Yusof et al, 2015). This study revealed that the prevalence of MERS-CoV RNA in 3–5-year-old camels (9.5%) was similar to that of animals older than 6 years (7.3%). However, camels of ≥6 years showed high positivity to anti-MERS-RBD antibody (46.34%) when compared with camels of 3–5 years (35.7%) (p < 0.01). Several previous studies have reported high seropositivity and high infection rate in adult camels compared with juvenile (Hemida et al, 2017; Reusken et al, 2014b). Additionally, Hamra camel breed showed highest positivity of 11.76% to MERS-CoV RNA than Majhim (10.71%), Maghatir (9.09%), and Sahilia breeds (0%) (p < 0.01).
Hence, the highest positivity to both RNA and antibodies to MERS-CoV was recorded in Hamra breed and lowest positivity was recorded in Sahilia breed. This variation is more likely due to the difference in distribution of these breeds. Indeed, Sahilia camels were sampled only in the West and Southwestern regions, where both had the lowest prevalence of MERS-CoV RNA, whereas Hamra camels were sampled in all regions. However, a higher resistance toward MERS-CoV of the breed Sahilia is also possible and should be further investigated.
The present study showed high prevalence rates of anti-MERS-RBD-specific IgG antibodies (40.9%) in dromedary camel milk samples. Most of the earlier reports have shown high seroprevalence rates of MERS-CoV antibodies. A MERS-CoV antibodies seroprevalence of 90% was reported for camels from the North of Mali (Falzarano et al, 2017). Similarly, high seroprevalences of 75.62% and 46.9% were reported for camels from Pakistan and Kenya, respectively (Deem et al, 2017; Zohaib et al, 2018). This work is, to the best of our knowledge, the first to report the prevalence of RNA and antibodies to MERS-CoV in camel milk samples from Saudi Arabia. Detection of MERS-CoV RNA in camel milk samples is in agreement with previous studies on the persistence of RNA positivity for extended period of time in milk and stool in addition to respiratory secretions (Al Hammadi et al, 2015; Hemida et al, 2014a; Muhairi et al, 2016; Reusken et al, 2014a; Wernery et al, 2015; Yusof et al, 2017).
In camel milk samples from a region in Qatar, viral RNA was detected in five among seven samples (Reusken et al, 2014a). The detection of MERS-CoV RNA in camel milk samples suggests that the milk might be infectious. This may support the proof of transmission of MERS-CoV to the human by drinking raw milk directly without sterilization, however, further in-depth investigations are needed.
These results indicate the need to focus on the mechanism of MERS-CoV transmission from camel milk to human, as it may be one of the most important mechanisms.
Conclusion
Human infection might be acquired by direct contact with infected camels or by drinking raw camel milk. Camel milk samples collected from randomly chosen farms from various regions in Saudi Arabia showed the presence of anti-MERS-RBD antibodies (40%) and MERS-CoV RNA (about 8%). Consequently, the presence of MERS-CoV RNA in camel milk warrants measures to prevent putative foodborne transmission of MERS-CoV. To understand the epidemiology and transmission routes of MERS-CoV in Saudi Arabia, further studies are required.
Footnotes
Acknowledgments
The authors would like to thank Jeddah University for approval of this work. The authors thank the people who helped in collection of samples and also thank Riyadh Municipality Central Area Laboratories, Riyadh, for providing necessary facilities to carry out the work.
Authors' Contributions
Conceptualization, M.N.A. and N.M.; methodology, A.A.; investigation, A.A.; data curation, M.N.A.; writing—original draft preparation, A.A.; writing—review and editing, M.N.A. and N.M.; supervision, N.M. and N.M.A.; all authors have read and agreed to the published version of the article.
Ethical Approval
University of Jeddah ethical committees approved this research.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.