
Abstract
The majority of children with coronavirus diseases 2019 (COVID-19) are asymptomatic or develop mild symptoms, and a small number of patients require hospitalization. Multisystem inflammatory syndrome in children (MIS-C) is one of the most severe clinical courses of COVID-19 and is suggested to be a hyperinflammatory condition. This study aimed to compare quantitative antibody levels against SARS-CoV-2 spike protein in children with COVID-19 and MIS-C. Blood samples from 75 patients [n = 36 (48%) with mild/asymptomatic (group 1), n = 22 (29.3%) with moderate-to-severe SARS-CoV-2 infection (group 2) and n = 17 (22.6%) patients with MIS-C (group 3)] were analyzed 3 months after COVID-19. The majority of the children with asymptomatic/mild COVID-19 symptoms (80.6%), moderate/severe disease (90.9%), and MIS-C (82.4%) had detectable IgG antibodies to SARS-CoV-2 spike protein (p = 0.567). The mean antibody value against SARS-CoV-2 spike protein was 321.9 ± 411.6 in group 1, 274 ± 261 in group 2, and 220 ± 299 in group 3, respectively (p > 0.05). Patients diagnosed with COVID-19 (asymptomatic/mild+moderate/severe) and those with MIS-C were also compared; the antibody positivity rates [COVID-19 group: 85.5%, MIS-C group: 82.4%, (p = 0.833)] and mean antibody values [COVID-19 group: 303.9 ± 360.3, MIS-C group: 220 ± 299, (p > 0.05)] were similar in both groups. In conclusion, the majority of children with COVID-19 and MIS-C developed a detectable antibody level against SARS-CoV-2 spike protein 3 months after COVID-19. Quantitative antibody levels were similar in both asymptomatic/mild disease, moderate/severe disease, and MIS-C group. Long-term studies evaluating antibody responses in children with COVID-19 and MIS-C are needed for more accurate vaccine schedules.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has different clinical courses in children and adults. Several studies reported that the majority of children (15–42%) with COVID-19 present with the asymptomatic or mild disease and do not require hospitalization (Viner et al, 2020; Wu and Mcgoogan, 2020; Wurzel et al, 2021; Zhou et al, 2020). The underlying causes of the mild course of COVID-19 in children remain uncertain. Differences in the immune response to SARS-CoV-2 can explain the different clinical outcomes in children and adults. Expression of the viral entry receptor angiotensin-converting enzyme-2 (ACE2) and the Transmembrane Serine Protease 2 (TMPRS2) is required in the airway epithelium for the spread of infection in children, which is decreased compared with adults (Weisberg et al, 2021; Zimmermann and Curtis, 2020). It may explain the less severe disease in childhood. Antibodies against previous seasonal human coronavirus infections may be protective against SARS-CoV-2 in children (Weisberg et al, 2021).
Pulmonary disease and severe clinical course occur in a small proportion of SARS-CoV-2-positive children (6). Risk factors for severe disease in children include younger age and preexisting medical conditions such as obesity, asthma, diabetes mellitus, and malignancy (Götzinger et al, 2020).
As the pandemic continues, pediatric patients with severe-to-critical illnesses have been more frequently reported. Extrapulmonary findings, including neurological manifestations and cardiac dysfunction, have been reported in <5% of hospitalized children (Irfan et al, 2021). It is also known that the pediatric patients (0–27%) may also develop long COVID-19 symptoms (fatigue, breathlessness, “brain fog” and depression, decreased ability of the patient to re-engage in normal activities), particularly children above 12 years (Molteni et al, 2021).
Multisystem inflammatory syndrome in children (MIS-C) is a syndrome that is one of the most severe clinical presentations of COVID-19 and mostly affects previously healthy children (Verdoni et al, 2020). MIS-C occurs ∼4–6 weeks following a clinically insignificant acute infection with SARS-CoV-2. It is more common in Black, Hispanic, and South Asian populations and the peak age for MIS-C is 9–10 years. Clinical features of MIS-C are similar to Kawasaki disease (KD); however, it differs in its epidemiological features and clinical and laboratory characteristics. MIS-C is most commonly characterized by fever, rash, conjunctival injection, gastrointestinal symptoms (particularly pain), lymphopenia, marked inflammation, and myocardial dysfunction (Feldstein et al, 2020).
SARS-CoV-2 has different antigenic structures such as nucleoprotein, N; envelope protein, E; matrix, M; and spike protein, S. Spike protein plays the most important role in the pathogenesis. It binds to the ACE2 receptor on host cells and induces membrane fusion. Antibodies binding to the receptor-binding domain of the SARS-CoV-2 spike protein can prevent attachment to the host cell and neutralize the virus. Several studies showed that MIS-C patients possess higher SARS-CoV-2 spike immunoglobulin G (IgG) than COVID-19 patients (Anderson et al, 2021; Rostad et al, 2020). In contrast, a previous study showed an insignificant difference (Weisberg et al, 2021). Data on post-COVID antibody levels in childhood are limited. Therefore, we aimed to determine quantitative antibody levels against SARS-CoV-2 spike protein in children with COVID-19 and MIS-C 3 months after COVID-19.
Methods
A single-center retrospective study was conducted at a tertiary-level university hospital. Seventy-five pediatric patients with COVID-19 and MIS-C were included between September 2021 and February 2022. The demographics (age, gender, dates of disease onset, diagnosis), clinical (duration and severity of symptoms associated with COVID-19), and laboratory (biochemical tests and complete blood count, chest X-ray, and computerized chest tomography (CT) information) were recorded; data of cases were extracted from patients' medical records. The duration of hospitalization, pediatric intensive care-PICU admission, management, and outcomes were recorded. Quantitative antibody levels against SARS-CoV-2 spike protein in the 3rd month after the infection were measured. None of the patients was vaccinated against COVID-19.
Patients were also evaluated for post-COVID-19 syndrome symptoms, such as anorexia, weakness, fatigue, anxiety disorder, anosmia, ageusia, arthralgia, influenza-like symptoms, sleep problems, decreased physical activity, headache, concentration and memory disorder, changes in gastrointestinal functions, and weight loss.
Inclusion and exclusion criteria were as follows:
Pediatric patients between 0 and 18 years of age, without underlying chronic conditions (malignancy, immunodeficiency, steroid use, renal failure etc.), not vaccinated against COVID-19, and with a positive SARS-CoV-2 PCR were included. The antibody measurements were performed 3 months after infection.
Patients older than 18 years of age, those with chronic diseases, under steroid and any immunosuppressive agents, and had already been vaccinated against COVID-19 were excluded.
Definitions
According to the Turkish Ministry of Health (COVID-19: Novel Corona Virus Disease Guideline, 2020) and WHO interim guidelines (Clinical Management of COVID-19 Interim Guidance 2020), disease severity was categorized as asymptomatic, mild, moderate, or severe among the children diagnosed with COVID-19 who had evidence of SARS-CoV-2 infection (by positive PCR test in the blood).
Asymptomatic illness was defined in children with a positive SARS-CoV-2 PCR test but did not have symptoms associated with COVID-19.
Mild illness was defined in children with upper respiratory tract infection symptoms who had no signs of pneumonia (no auscultatory abnormalities) or hypoxia. Fever, cough, muscle pain, stomach discomfort, myalgia, nausea, headache, and diarrhea were nonspecific symptoms.
Moderate illness was defined in children with nonsevere pneumonia symptoms/signs such as rapid breathing, cough, and chest indrawing during clinical assessment or on imaging.
The severe illness was defined as severe pneumonia, cough, trouble breathing, respiratory distress, lethargy, and convulsions in children.
Patients with asymptomatic/mild illness were classified as group 1, those with moderate/severe illness were classified as group 2, and patients with MIS-C were classified as group 3.
MIS-C was defined according to the Centers for Disease Control and Prevention (CDC) diagnostic criteria of MIS-C as including fever lasting more than 1 day; two of the following symptoms, such as rash or bilateral nonpurulent conjunctivitis, mucocutaneous inflammation signs, hypotension, shock, myocardial dysfunction, pericarditis, valvulitis, coronary abnormalities, coagulopathy, or acute gastrointestinal symptoms; evidence of inflammation; no other microbial cause; and with evidence of previous SARS-CoV-2 infection (PCR or serology positivity) (CDC Health Alert Network, 2020).
For each patient, whole blood count [white blood cell, absolute neutrophil count, absolute lymphocyte count, hemoglobin (Hb), platelet count], as well as biochemical parameters, such as urea, creatinine, aspartate aminotransaminase, alanine amino transaminase, sodium, C-reactive protein (CRP), procalcitonin, D-dimer, fibrinogen, ferritin, troponin T, erythrocyte sedimentation rate, and N-terminal pro-brain natriuretic peptide (NT-proBNP) values at first admission, were recorded.
Molecular analysis
A viral transport medium containing VNat, combined nasopharyngeal and oropharyngeal swab specimens were obtained (Bioeksen). Our Molecular Virology Laboratory evaluated all samples using the Bio-speedy® SARS CoV-2 Double Gene RT-qPCR (Bioeksen). The Rotor-Gene was used for reverse transcription–polymerase chain reaction (RT-PCR) (Qiagen). This assay amplifies and detects two viral targets (ORF1ab and N), with a detection limit of 200 genomes per mL. The human gene target RNAse P (RP) was evaluated in each sample to employ an internal control. Results were considered positive if the signal was detected (Ct <35) for RP, ORF1ab, and N genes.
Quantification of SARS-CoV-2 serum antibody values
Blood samples were obtained in gel-coated tubes and centrifuged at 1,780 g for 10 min in this study. Following the centrifugation step, serum samples were aliquoted and frozen at a temperature of −80°C. Serum samples were thawed and analyzed by using Anti-SARS-CoV-2 QuantiVac ELISA IgG (Euroimmun, Lubeck, Germany), a quantitative enzyme-linked immunosorbent assay (ELISA) test that uses recombinant S1 antigen subunit. Clinical specimens were tested using an automated ELISA system, the Euroimmun Analyzer I (Euroimmun), in line with the manufacturer's instructions. Antibody levels above 11 R.U./mL are considered positive, 8–11 R.U./mL are regarded borderline, and fewer than 8 R.U./mL are considered negative. By multiplying the results in R.U./mL by 3,2, the results were converted to a standardized binding antibody unit/mL (BAU/mL). Thus, <25.6 BAU/mL results were considered negative, ≥25.6 to <35.2 BAU/mL borderline, and ≥35.2 BAU/mL positive. All samples were tested using the same method at a 1:16 dilution, and the results were noted (Beavis et al, 2020; WHO, 2021).
Ethics approval
The Research Ethics Committee of Ege University Faculty of Medicine and the Ministry of Health approved the study (Ethical decision No:22–3T/30). This study was carried out in accordance with the Helsinki Declaration. The written consent of the children's parents was obtained.
Statistical analysis
The SPSS statistics software was used to perform the statistical analysis (version 25 for Windows). Mean SD or medians (interquartile range) were used for continuous data, and categorical variables and percentages were used. The Student's t-test was used for normally distributed, categorical data, and the 2 tests. The Mann–Whitney U test was performed to examine differences in nonparametric data. A p-value of 0.05 was used to determine the statistical significance of differences and correlations.
Results
This study included 75 patients categorized into three disease phenotypes; 36 (48%) patients with mild/asymptomatic infection (group 1), 22 (29.3%) patients with moderate-to-severe infection (group 2) and 17 (22.6%) patients with MIS-C (group 3). Demographic and laboratory data are shown in Table 1. The pediatric intensive care unit (PICU) admission rate (p < 0.001) and length of stay in PICU (p = 0.007) were found to be significantly higher in group 2.
Demographic and Laboratory Data of Patients
The bold values indicate statistical analysis differences and correlations were considered significant at p < 0.05.
CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; PICU, pediatric intensive care unit; ALC, absolute lymphocyte count; ANC, absolute neutrophil count; Hb, hemoglobin; WBC, white blood cell.
Fever was significantly more frequent in group 2 (p = 0.001). Chest pain, cough, and dyspnea were significantly more common in group 2 than in other groups (p < 0.001). Post-COVID symptoms did not show a significant difference among the three groups.
CRP and procalcitonin values were significantly higher in group 3 than in group 2 (p < 0.001 and p = 0.045), and Hb values were significantly lower (p = 0.050) whereas D-dimer, fibrinogen, and NT-proBNP were higher in group 3 (Table 1).
Quantitative values and positive rate of antibody levels to SARS-CoV-2 in children
Quantitative antibody levels were measured 3 months after COVID-19 in all patients. The majority of the children with asymptomatic/mild COVID-19 symptoms (80.6%), moderate/severe disease (90.9%), and MIS-C (82.4%) had detectable IgG antibodies to SARS-CoV-2 spike protein. The mean antibody values against SARS-CoV-2 spike protein was 321.9 ± 411.6 in group 1, 274 ± 261 in group 2, and 220 ± 299 in group 3. There were no significant differences between the groups for antibody positivity (p = 0.567) and negativity (p = 0.922). Although antibody values were lower in group 3, it was not statistically significant (p > 0.05).
Patients with antibody positivity were compared in terms of their quantitative values. Although there was no statistical difference, it was found that the rate of high values of antibody (>200 BAU/mL) was higher in asymptomatic (44.4%) and moderate/severe disease (50%) groups than in the MIS-C (29.4%) group (Tables 2 and 3).
Comparison of Antibody Positivity Against SARS-CoV-2 Spike Protein in Children with Asymptomatic/Mild, Moderate/Severe COVID-19 and Multisystem Inflammatory Syndrome in Children
BAU, binding antibody unit.
Comparison of Quantitative Antibody Values Against SARS-CoV-2 Spike Protein in Children with Asymptomatic/Mild, Moderate/Severe COVID-19, and Multisystem Inflammatory Syndrome in Children
Comparison of patients with COVID-19 and MIS-C
All patients with COVID-19 (asymptomatic/mild+moderate/severe) and those with MIS-C were also compared. The antibody positivity rate was similar in patients with COVID-19 (85.5%) and MIS-C (82.4%) (p = 0.833) (Table 4). The mean antibody value against SARS-CoV-2 spike protein was 303.9 ± 360.3 in the COVID-19 group and 220 ± 299 in the MIS-C group. Although antibody levels were higher in the COVID-19 group, they were insignificant (p > 0.05). The proportion of the patients with high antibody titers (200 BAU/mL) was higher in COVID-19 patients (46.6%) than in MIS-C (29.4%) (Table 5), but it did not show a significant difference (p = 0.27) (Tables 4 and 5)
Comparison of Antibody Positivity Against SARS-CoV-2 Spike Protein in Children with COVID-19 and Multisystem Inflammatory Syndrome in Children
Comparison of Quantitative Antibody Values Against SARS-CoV-2 Spike Protein in Children with COVID-19 and Multisystem Inflammatory Syndrome in Children
Comparison of antibody values according to age groups
Children included in the study were divided into three age groups (0–4 years, 5–11 years, and 12–18 years). Among the study group, children 0–4 years of age (100% n = 7), 78.2% (n = 18/23) of children in the 5–11 age group, and 84% (n = 38/45) of children in the 12–18 age group developed detectable IgG antibodies to SARS-CoV-2 spike protein. There was no significant difference between age groups in terms of quantitative antibody values (Tables 6, 7 and Figs. 1, 2).
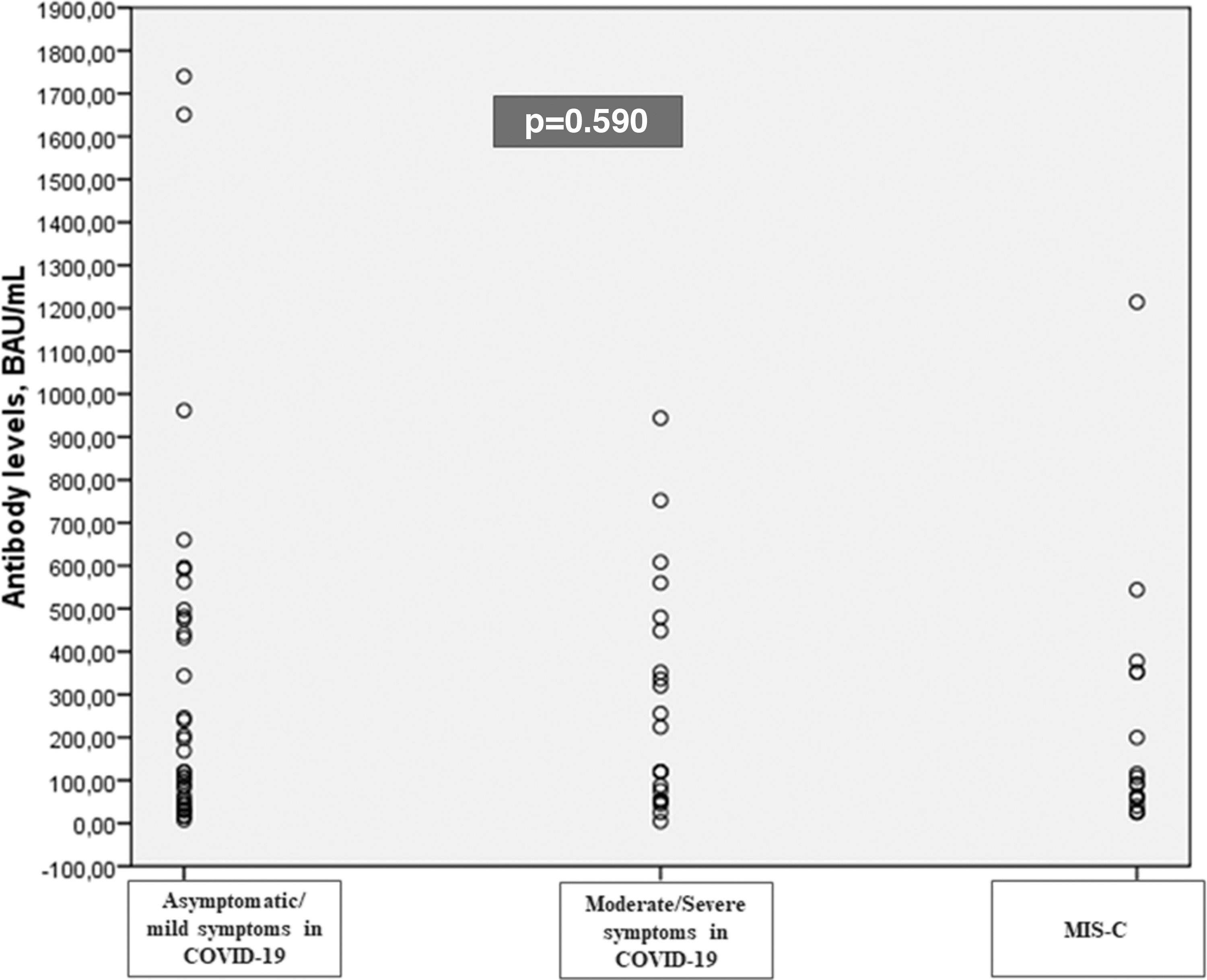
Quantitative antibody values against SARS-CoV-2 spike protein [BAU/mL (mean ± SD)] in children with asymptomatic/mild, moderate/severe COVID-19 and MIS-C. BAU, binding antibody unit; MIS-C, multisystem inflammatory syndrome in children.
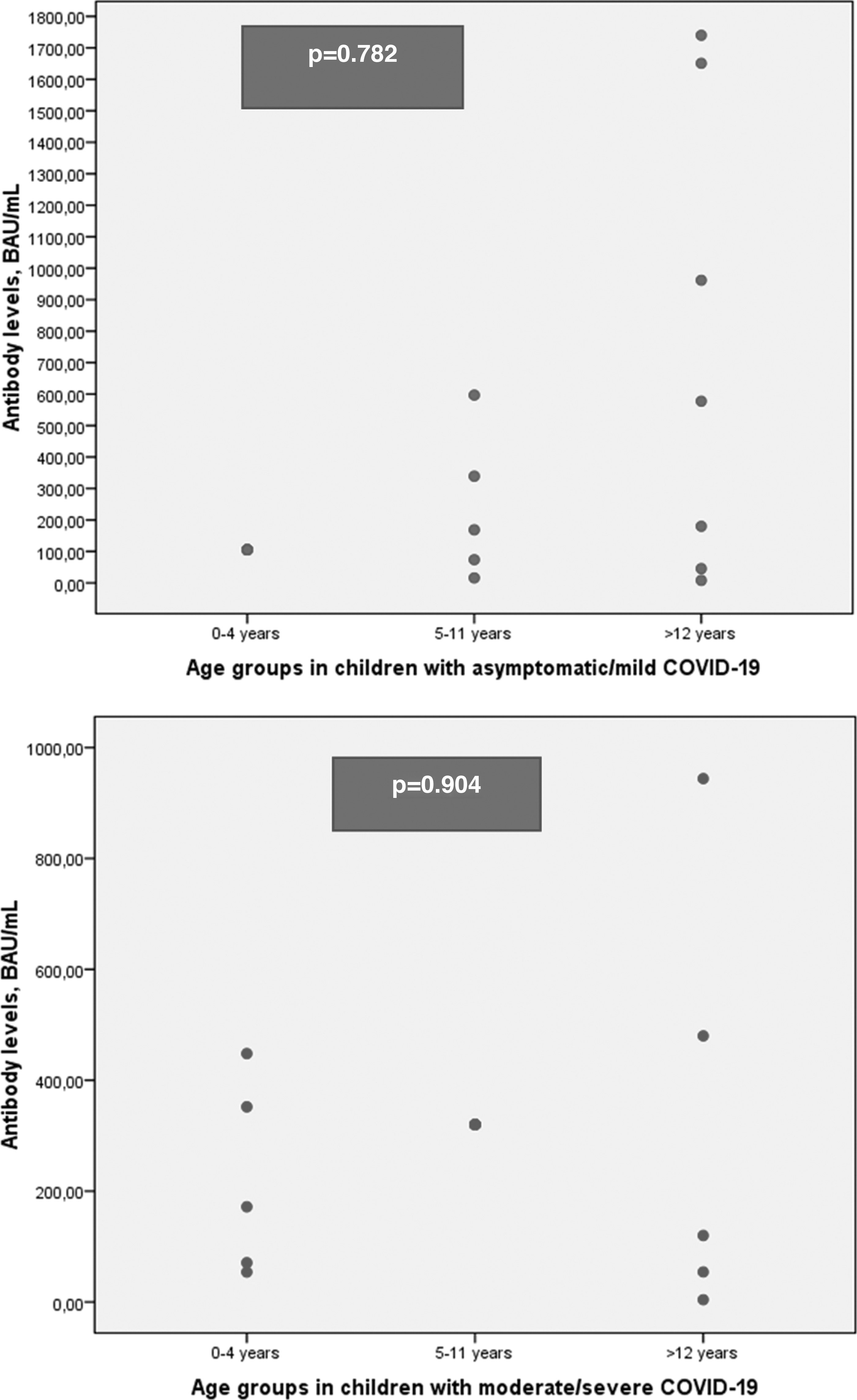
Quantitative antibody levels values against SARS-CoV-2 spike protein [BAU/mL (mean ± SD)] in children with COVID-19 and MIS-C by age groups.

Antibody Positivity Against SARS-CoV-2 Spike Protein in Children with COVID-19 and Multisystem Inflammatory Syndrome in Children by Age
Comparison of Quantitative Antibody Values Against SARS-CoV-2 Spike Protein in Children with COVID-19 and Multisystem Inflammatory Syndrome in Children According to Age Groups
Discussion
In this single-center study, children with COVID-19 (including asymptomatic/mild and moderate/severe disease) and MIS-C were evaluated for antibody response 3 months after infection, and most children developed a detectable IgG antibody response to SARS-CoV-2 spike protein. There was no difference between asymptomatic/mild disease, moderate/severe disease, and MIS-C groups in mean antibody levels.
In the pandemic's early stages, a U.S. study investigated the humoral responses to SARS-CoV-2 in children with COVID-19 and MIS-C and found that children with COVID-19 had various levels of serum IgG against all SARS-CoV-2 antigens (Anderson et al, 2021). The majority of the patients with severe COVID-19 had undetectable levels of spike antibodies, the receptor-binding domain (S-RBD), and the nucleocapsid IgG antibodies. MIS-C patients had higher antibody titers against S-RBD and full-length spike protein (Anderson et al, 2021). This may be explained by the sampling time for their study because data on the window period are unclear, and a longer time passes since the onset of infection in children with MIS-C relative to children with severe COVID-19 (a median of 5 days since symptom onset).
Another study emphasizing the changes in antibody levels in childhood analyzed blood samples from 114 children with COVID-19 (43.9% asymptomatic and 56.1% mildly symptomatic). It showed that in both asymptomatic and mildly symptomatic children, the positive rates of anti-S IgG, anti-SARS-CoV-2 IgG, and NAb were low within 7 days after onset, but they soon reached 100% 14 to <28 days after onset.
In symptomatic children, antibodies' geometric mean titers (GMTs) were below the positive cutoff during the first 2 weeks of onset and peaked at 28 to <56 days. Antibody levels remained detectable up to 3 months after infection. Children 0–4 years of age had the highest antibody GMTs from 14 to <56 days after symptom onset (Han et al, 2022).
Several studies from European countries demonstrated that children with asymptomatic or mildly symptomatic COVID-19 developed SARS-CoV-2 IgG that persisted for more than 6 months (Bonfante et al, 2021; Méndez-Echevarría et al, 2021). In our study, we collected serum samples from the patients 3 months after COVID-19 diagnosis. Quantitative antibody levels were measured collectively at the same time and we determined that the majority of the children with asymptomatic/mild COVID-19 had detectable IgG antibodies to SARS-CoV-2 spike protein.
Previous adult studies indicated that patients with severe COVID-19 had higher titers of SARS-CoV-2 S-RBD antibodies than those with milder disease (Kuri-Cervantes et al, 2020; Mathew et al, 2020). A correlation between antibody levels and disease severity was demonstrated in several adult studies (Long et al, 2020; Qu et al, 2020). In contrast, we found higher titers in the asymptomatic/mild disease group. Recently, higher nasopharyngeal SARS-CoV-2 viral loads and low RT-PCR cycle threshold values have been reported in children with mild-to-moderate COVID-19 symptoms than in adults with similar symptoms (Heald-Sargent et al, 2020). It has been suggested that this high viral load can explain a robust immune response in asymptomatic or mildly symptomatic children.
A prospectively designed study aimed to measure serological responses in hospitalized children with COVID-19, MIS-C, and Kawasaki disease, and they found that all children with MIS-C had high titers of SARS-CoV-2 RBD IgG antibodies, which correlated with full-length spike IgG antibodies, nucleocapsid protein antibodies, and neutralizing antibodies (Rostad et al, 2020). In our study, we compared all children diagnosed with COVID-19 with those with MIS-C, and the antibody positivity rate was similar. In quantitative measurement, we found higher titers in patients with COVID-19. This difference may be due to intravenous immunoglobulin treatment in MIS-C patients, which can alter antibody responses.
Our study has some limitations; it reflects the data of a minor patient group. The number of patients in the 0–4 age group is insufficient for statistical analysis. But standardizing the sampling time in all patient groups (obtained 3 months after the diagnosis) provided an advantage. It contributes to the literature by showing that antibody levels in COVID-19 patients can also reach as high as MIS-C patients over time.
In conclusion, we found that the antibody positivity rate and quantitative antibody levels against SARS-CoV-2 spike protein in children with asymptomatic/mild COVID-19 were as high as those with severe COVID-19 disease and MIS-C. When all COVID-19 patients were compared with the MIS-C group, regardless of disease severity, it was observed that children with COVID-19 had higher antibody titers. Long-term studies are needed to examine antibody responses over time in children with COVID-19 and MIS-C for different vaccination schedules.
Footnotes
Authors' Contributions
G.A.: Conceptualization (lead); writing––original draft (lead); formal analysis (lead); writing––review and editing (equal).
S.Y.A., M.A., and N.M.B.: Conceptualization (supporting); writing––original draft (supporting); and writing––review and editing (equal).
Z.S.B. and C.C.: Methodology (lead); and writing––review and editing (equal).
Z.K. and F.O.: review and editing (equal).
F.O.: Software (lead); and writing––review and editing (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.