
Abstract
To better understand dynamic changes of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) immune response, a prospective, single-center, cohort study was conducted on longitudinal immune response in 34 COVID-19 convalescent patients over 23 months in Chongqing. Two blood samples from convalescent patients were collected, first sample collected during 10–13 months (M10–13) after infection (pre-SARS-CoV-2 vaccination) and second sample collected during 20–23 months (M20–23) after infection (post-SARS-CoV-2 vaccination). The SARS-CoV-2-specific humoral and cellular immunity were traced by testing total antibody (Ab), anti-nucleocapsid (NP) immunoglobulin M (IgM), anti-NP immunoglobulin G (IgG), and anti-spike (S) IgG Abs, lymphocyte subset count, and Th1 cytokines. Healthy donors (30) were also included in the study as the uninspected healthy controls. Our data showed significant change in mean titer of SARS-CoV-2-specific Ab response from M10–13 to M20–23 included, namely, SARS-CoV-2-specific total Ab as 219 AU/mL increasing to 750.9 AU/mL; anti-NP IgM as 3.5 AU/mL decreasing significantly (p < 0.001) to 0.6 AU/mL; anti-NP IgG as 7.9 AU/mL increasing to 87.1 AU/mL; and anti-S IgG as 499.0 RU/mL increasing to 1,802.3 RU/mL. Our observations suggested that one vaccine dose might have been sufficient for COVID-19 convalescent patients. Larger sample sizes are needed to compare better immune effect of protein subunit vaccine. Besides, compared to healthy donors, patients had decreased CD3+ and CD8+ T lymphocyte counts during two periods. Patients had most cytokines recovered normally within 2 years, but IL-6 level was significantly elevated; however, IL-6 was negatively correlated with IgM and positively correlated with IgG. Changes in cytokines might have been caused by SARS-CoV-2 infection or vaccination. Patients with comorbidities were associated with decreased CD3+ and CD8+ T lymphocytes and lower Ab titers following SARS-CoV-2 vaccination. Vaccination enormously increased humoral immunity beneficial in COVID-19 convalescent patients. Elderly COVID-19 convalescent patients with comorbidities needed more attention.
Introduction
Protective and persistent host immune response against viral infection usually comes from the combined action of B and T lymphocytes. Duration and effectiveness of humoral and cellular immunity against primary infection of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) are key questions in understanding the COVID-19 pandemic. Antibodies (Abs) against viral nucleocapsid (NP) and spike (S) proteins are elicited in majority of patients (Zhao et al., 2020). The S-protein is a primary target for neutralizing Abs, which can block viral entry (Ju et al., 2020). Levels of immunoglobulin M (IgM) and immunoglobulin G (IgG) against NP and S proteins increase gradually after symptom onset, which is correlated with virus neutralization titer (To et al., 2020). Normally, Ab titers can reflect the progress of viral infection, and correspond to disease severity.
However, duration of humoral and cellular immunity has not been well elucidated. Rapid decline of SARS-CoV-2-specific Ab levels in some patients heighten public concerns about the long-term effectiveness of COVID-19 vaccine (Ibarrondo et al., 2020). Furthermore, whether a single dose could offer adequate protection or multiple doses are required in recovered patients is still a matter of debate (Stamatatos et al., 2021). To date, the longest observation period assessing the Ab response (anti-NP and anti-S IgM/IgG) has been 6–18 months (Dehgani-Mobaraki et al., 2021; Dehgani-Mobaraki et al., 2022; Gallais et al., 2021; Liu et al., 2021; Zeng et al., 2021). Besides, longitudinal studies with larger cohort size for longer time frames are needed to determine persistence of SARS-CoV-2-specific immune response.
In this study, we investigated the prevalence of SARS-CoV-2-specific humoral and cellular immunity in serial blood samples collected from 34 COVID-19 convalescent patients and 30 healthy donors during month 10–13 (M10–13) and month 20–23 (M20–23) post-SARS-CoV-2 infection. We assessed the dynamic changes of immunity indicators in these individuals. We further analyzed the natural immunity after infection and immune response activated by COVID-19 vaccine during the convalescence period. The findings in this study may be of help to understand the long-term duration of humoral immune response, herd immunity, and efficacy of vaccines, which are beneficial in controlling the COVID-19 pandemic.
Materials and Methods
Patients
In total, 34 COVID-19 recovered cases were enrolled in this study, including 29 mild to common patients and 5 severe to critical patients. According to the Novel Coronavirus Pneumonia Prevention and Control Program (5th edition) published by the National Health Commission of China, clinical classifications are as follows: (i) mild: patients present mild symptoms with no imaging sign of pneumonia; (ii) common: patients have fever and respiratory tract symptom with imaging sign of pneumonia; (iii) severe: patients, who present respiratory distress with respiratory rate ≥30 breath/min, or SpO2 (oxygen saturation) ≤93% on room air, or PaO2 (arterial blood oxygen partial pressure)/FiO2 (fraction of inspired oxygen) ≤300 mmHg (1 mmHg = 0.133 kPa); and (iv) critical: patients, who present respiratory failure requiring mechanical ventilation support or shock, and multiple organ dysfunction syndrome requiring ICU admission.
These patients were enrolled from Chongqing Red Cross Hospital (People's Hospital of Jiangbei District) in China, who tested positive for SARS-CoV-2 by reverse transcription quantitative polymerase chain reaction (RT-qPCR) during February to March 2020. Therefore, the patients were followed up longitudinally for 23 months. Blood samples from these individuals were collected during M10–13 and M20–23 after infection.
In addition, 30 healthy, age- and sex-matched SARS-CoV-2 RT-qPCR-negative donors were enrolled from Chongqing Red Cross Hospital (People's Hospital of Jiangbei District). All healthy subjects followed the same visit schedule. Participants completed a questionnaire at each visit, including COVID-19 exposure, symptoms, virological findings, and eventually vaccination; and 12 mL blood sample was collected from each participant. The participant or their legally authorized representative gave written informed consent for study enrollment in accordance with the Declaration of Helsinki. The study was approved by the Ethics Committee of Chongqing Red Cross Hospital (People's Hospital of Jiangbei District).
Blood assays
Analysis of SARS-CoV-2-specific total Abs
SARS-CoV-2-specific total Abs assay (Xiamen InnoDx Biotech Co., Xiamen, China) is a paramagnetic particle chemiluminescent immunoassay (CLIA) for qualitative detection of SARS-CoV-2-specific total Ab in human serum and plasma using the automated iFlash immunoassay system. The iFlash-2019-nCoV total Ab assay is a dual-Ab sandwich immune assay method. It is mainly used for the evaluation of Abs in patients recovering from COVID-19 or auxiliary evaluation of the effect of SARS-CoV-2 vaccine. Levels of anti-SARS-CoV-2-specific total Ab in the sample were detected by iFlash optical system.
Analysis of SARS-CoV-2-specific anti-NP IgM and IgG Abs
SARS-CoV-2-specific anti-NP IgM and IgG Abs were detected by CLIA using an Auto LumoA2000 automated chemiluminescent immunoanalyzer (Zhengzhou Antu Bioengineering Co., LTD). Detection method was developed based on magnetic particle chemiluminescence immunoassay. Matched regent was developed based on magnetic particle and recombinant protein containing SARS-CoV-2-NP. The tests were conducted on an automated magnetic chemiluminescence analyzer and Ab levels were expressed by chemiluminescence signal, according to the manufacturer's instructions. Results were expressed as AU/mL. Values less than 1.00 AU/mL (<1.00 AU/mL) were considered nonreactive, and greater than or equal to 1.00 AU/mL (≥1.00 AU/mL) as reactive.
Analysis of SARS-CoV-2-specific anti-S IgG Abs
SARS-CoV-2-specific anti-S IgG Abs were assayed according to testing procedures (Bao et al., 2021). In brief, 5 μL plasma and 95 μL sample dilutent were added to 96-well ELISA plates, coated with SARS-CoV-2 recombinant S proteins (Sino Biological, Inc., Beijing, China), incubated at 37°C for 1 h. After washing thrice with wash buffer (1 × ), the wells were incubated with 100 μL enzyme conjugate for 30 min at 37°C.
After washing thrice with wash buffer (1 × ), 100 μL of tetramethylbenzidine was added to each well and incubated at 37°C for 15 min, followed by the addition of 100 μL of stopping solution to all the wells. Optical density at 450/630 nm was measured using a microplate reader (PHOmo; Autobio Diagnostics Co., Zhengzhou, China). The cutoff value for positivity was set at >20 RU/mL for SARS-CoV-2-specific anti-S IgG. Cutoff values for Ab positivity were determined based on receiver operating characteristic curves with data from convalescent COVID-19 patients and negative healthy donor samples following the procedure of Marcotte et al. (2022).
Lymphocyte subset determination
Percentage and absolute count of total T cells (CD3+), CD4+ and CD8+ T cells, B cells (CD19+), and NK cells (CD16+ CD56+) were determined by using Trucount tubes and BD Multitest six-color TBNK reagent kit (BD Biosciences), according to the manufacturer's instructions. Briefly, 50 μL of whole blood was labeled with a six-color TBNK Ab cocktail for 15 min at room temperature. After adding 450 μL of FACS Lysing Solution, samples were analyzed with the FACSCanto flow cytometer using FACSCanto clinical software (BD Biosciences) (Zhang et al., 2021). CD45 cells from BD Multitest six-color TBNK reagent was used for flow cytometry gating. We adopted a Chinese national multicenter study to define a reference range of normal values for peripheral blood lymphocyte subsets in healthy adults (Liu et al., 2022).
Cytokine analysis
IL-2, IL-4, IL-6, IL-10, IFN-γ, and TNF-α were quantified using BD Cytometric Bead Array Human Th1/Th2 Cytokine Kit (Weimi Bio-Tech, Guangzhou, China) following the manufacturer's instructions. Briefly, 25 μL of cytokine standard or plasma sample was mixed with 10 μL of fluorescent Ab at room temperature for 2.5–3 h. Tubes were washed with 1 mL PBS and resuspended in 150 μL PBS before acquisition on a BD FACSLyric flow cytometer (Becton Dickinson, San Jose, CA, USA). Data were analyzed for individual cytokine concentration using the FCAP Array Software Version 3.0 (BD Biosciences) (Belaid et al., 2022). According to the reagent instructions (Weimi Bio-Tech), detection limits within normal value range were, respectively, 5.71 pg/mL for IL-2; 2.8 pg/mL for IL-4; 5.3 pg/mL for IL-6; 4.91 pg/mL for IL-10; 7.42 pg/mL for IFN-γ; and 4.6 pg/mL for TNF-α.
Statistical analysis
Statistical analysis was performed using SPSS (Version 25.0). Graphs were plotted using GraphPad Prism 9.0. Student's t-test was performed to compare two groups and one-way analysis of variance to compare more than two groups. Pearson's correlation coefficients were calculated. Positive rates were analyzed by χ 2 test or Fisher's exact tests. Descriptive statistics for the main characteristics of the study group were expressed as Median (interquartile range [IQR]) for continuous variables, and as absolute frequency (percentage) for the categorical variables. Results were analyzed and nonparametric test (Mann-Whitney U test) was used for the data not distributed within normal range. p-Values <0.05 were considered significant.
Results
Demographic and clinical characteristics of subjects
In total, 34 COVID-19 convalescent patients were enrolled in this study (Table 1). Median age was 59.0 (IQR = 39.0–67.2) years, and 16 (47.1%) patients were male. Among all patients, 5 (14.7%) were severe and critical cases, 8 (23.5%) lost their sense of smell, 6 (17.6%) lost their sense of taste, and 17 (50.0%) had one or more comorbidities such as chronic bronchitis, tumor, diabetes, or cardiovascular diseases. Median time of serum sample collection from 34 patients during M10–13 was 326 days (IQR = 306–340), and 28 patients during M20–23, it was 645 days (IQR = 637–685).
Demographics and Clinical Characteristics of Patients and Healthy Donors
p-Values were calculated with Student's t-test, χ 2 test, or Fisher's exact tests using SPSS (Version 25.0).
IQR, interquartile range; NA, not applicable.
Among vaccinated patients, four vaccine categories were divided according to type and dose of vaccine administered, including 6 vaccinated patients with single-dose protein subunit vaccine (ZF2001), 6 vaccinated patients with single-dose inactivated vaccine (CoronaVac or BBIBP-CorV), 1 vaccinated patient with multidose protein subunit vaccine (ZF2001), and 15 vaccinated patients with multidose inactivated vaccine (CoronaVac or BBIBP-CorV). At the same time, 30 healthy donors were recruited and sampled with the same schedule, and they were also vaccinated with SARS-CoV-2 vaccine before M20–23 sampling. Types of vaccination and time from last dose of vaccine to serum collection in patients and healthy donors are shown in Table 1.
SARS-CoV-2-specific Abs in COVID-19 convalescent patients
Using serum samples from the patients and healthy donors, SARS-CoV-2-specific total Ab, anti-NP IgM, anti-NP IgG, and anti-S IgG were detected. Changes in mean titer and patients' positive rate of SARS-CoV-2-specific Ab response from M10–13 to M20–23 (Fig. 1) included, namely, SARS-CoV-2-specific total Ab as 219 [95% confidence interval (Cl) = 138.0–300.0] AU/mL and 100% (34/34) increasing to 750.9 (95% Cl = 640.8–861.0) AU/mL and 100% (28/28) (Fig. 1a); anti-NP IgM as 3.5 (95% Cl = 0.1–7.1) AU/mL and 44.1% (15/34) decreasing significantly (p < 0.001) to 0.6 (95% Cl = 0.1–1.0) AU/mL and 14.3% (4/28) (Fig. 1d); anti-NP IgG as 7.9 (95% Cl = 5.4–10.4) AU/mL and 97.1% (33/34) increasing to 87.1 (95% Cl = 40.9–133.3) AU/mL and 100% (28/28) (Fig. 1c); and anti-S IgG as 499.0 (95% Cl = 348.7–649.2) RU/mL and 100% (34/34) increasing to 1,802.3 (95% Cl = 838.5–2,766.0) RU/mL and 100% (28/28) (Fig. 1b).
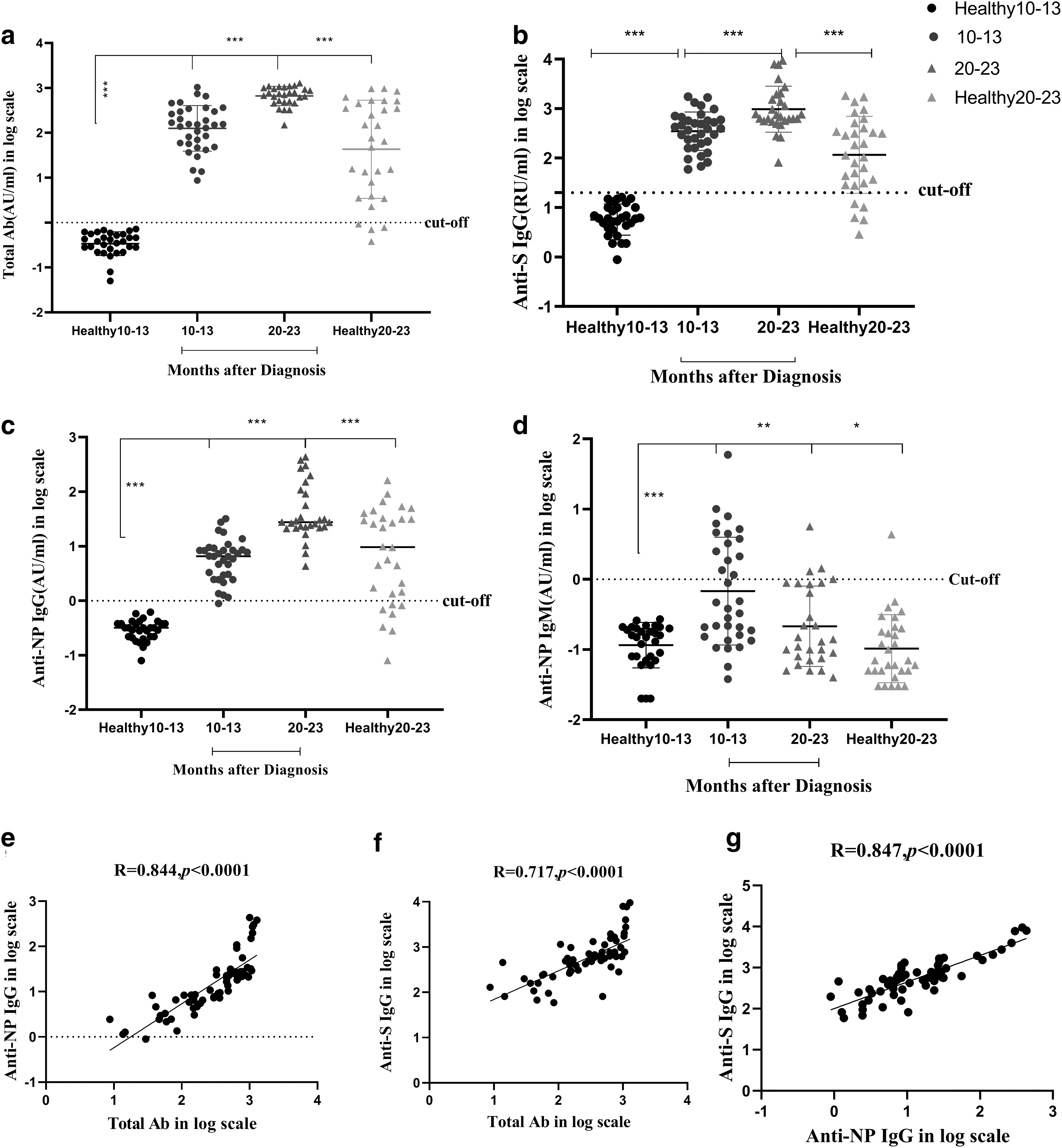
SARS-CoV-2-specific antibodies were analyzed in COVID-19 convalescent patients and healthy donors, including total Ab
Mean titers of SARS-CoV-2-specific total Abs, anti-NP IgG, and anti-S IgG Abs increased threefold (p < 0.001) during M20–23 in postvaccinated convalescent patients, compared during M10–13 in prevaccinated convalescent patients. In healthy donors, mean titer and positive rate of these Abs during M20–23, included, namely, SARS-CoV-2-specific total Ab as 241.1 (95% Cl = 127.4–354.8) AU/mL and 86.7% (26/30) (Fig. 1a); anti-NP IgG as 25.0 (95% Cl = 12.1–38.0) AU/mL and 83.3% (25/30) (Fig. 1b); and anti-S IgG as 362.8 (95% Cl = 174.4–551.2) RU/mL and 76.7% (23/30) (Fig. 1c); thus, mean titers of all these Abs in healthy donors during M20–23 were almost equal to those of COVID-19 convalescent patients during M10–13, but decreased threefold than in COVID-19 convalescent patients during M20–23.
The findings showed that anti-NP IgM titers declined significantly over time being mostly negative 2 years after infection. In the meantime, majority of COVID-19 convalescent patients, in their natural immune state, could maintain their SARS-CoV-2-specific IgG level until at least 13 months after infection. After first follow-up, 28 patients and healthy controls were vaccinated with COVID-19 vaccine. Immunization induced specific Abs (SARS-CoV-2-specific total Ab, anti-NP IgG, and anti-S IgG) in the vaccinees, and levels of induced three Ab titers were significantly higher in convalescent patients than in healthy donors by at least threefold (all p < 0.001).
It can be seen that vaccination has a beneficial promotion effect on Ab production. Meanwhile, the IgM of COVID-19 convalescent patients was mostly negative 2 years after infection, and anti-NP IgM was positive in four convalescent patients during M20–23, including three severe to critical convalescent patients and one mild patient. SARS-CoV-2-specific total Abs were significantly and positively correlated with anti-NP IgG (Fig. 1e) and anti-S IgG (Fig. 1f); and higher anti-NP IgG was significantly correlated with anti-S IgG (Fig. 1g).
Effect of SARS-CoV-2 vaccination types on humoral immunity in COVID-19 convalescent patients
Analysis of SARS-CoV-2-specific anti-NP IgG and anti-S IgG for COVID-19 convalescent patient and healthy donor groups was done to explore if SARS-CoV-2 vaccination types affected humoral immunity in COVID-19 convalescent patients. Type of vaccines administered to COVID-19 convalescent patients and healthy donors are shown in Table 1. M10–13 indicated patients before vaccination, M20–23 indicated patients after vaccination.
Elevated levels of serum-specific Abs after vaccination with inactivated and protein subunit vaccines were found. For the inactivated vaccine group, mean absorbance value (MAV) of anti-S IgG increased 2.08-fold during M20–23 compared to M10–13 in COVID-19 convalescent patients, and 3.84-fold in healthy donors (Fig. 2a); MAV of anti-NP IgG increased 5.12-fold during M20–23 compared to M10–13 in COVID-19 convalescent patients, and 2.71-fold in healthy donors (Fig. 2b).
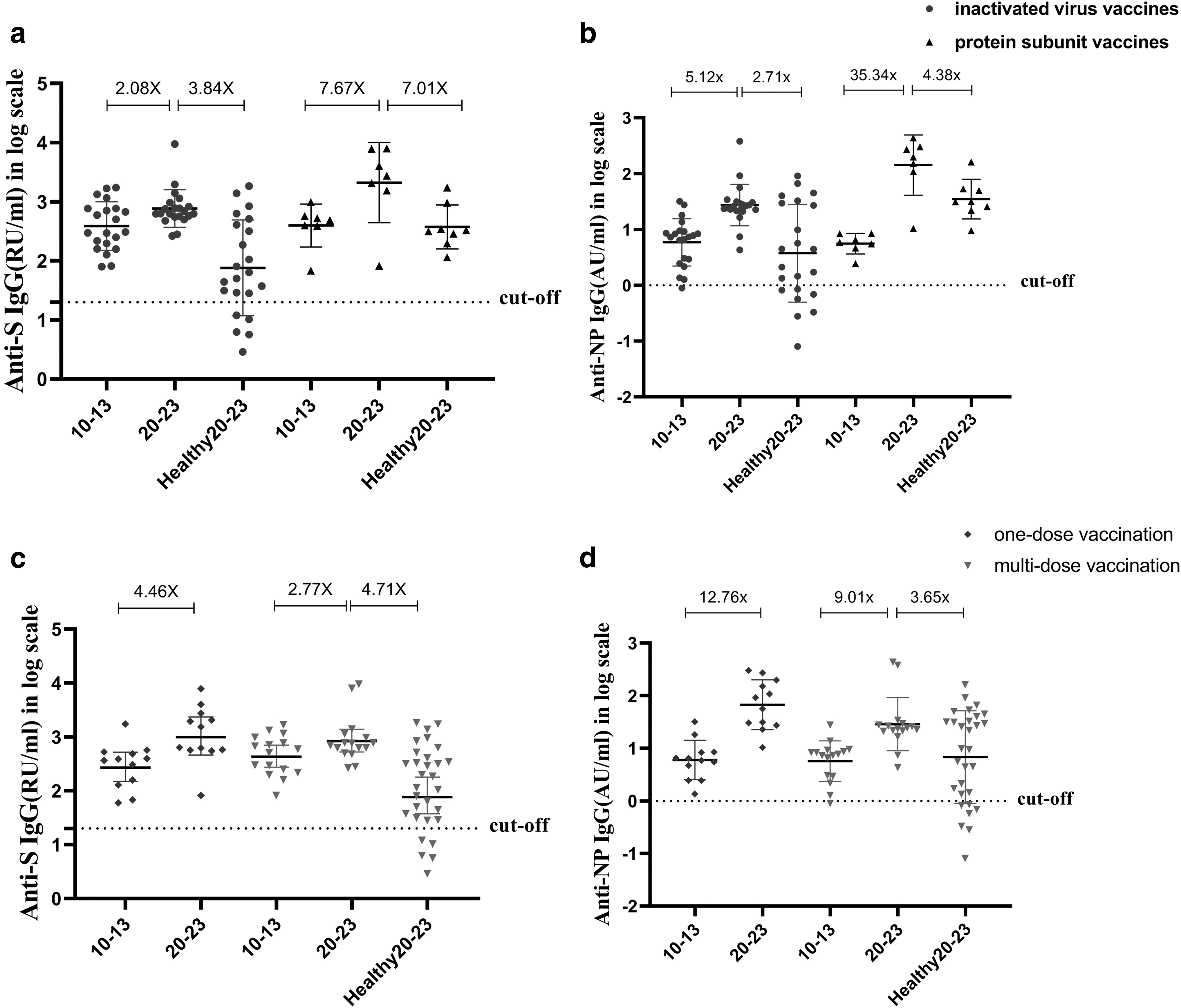
SARS-CoV-2-specific IgG levels in COVID-19 convalescent patients and healthy donors, who had received inactivated virus vaccines or protein subunit vaccines, anti-S IgG
For protein subunit vaccine group, MAV of anti-S IgG increased 7.67-fold during M20–23 compared M10–13 in COVID-19 convalescent patients, and 7.01-fold in healthy donors (Fig. 2a); MAV of anti-NP IgG increased 35.34-fold during M20–23 compared to M10–13 in COVID-19 convalescent patients, and 4.38-fold in healthy donors (Fig. 2b). Thus, protein subunit vaccine produced higher Ab titers than inactivated vaccine; however, only 7 patients (25%) received the protein subunit vaccine, compared to 21 patients who received the inactivated vaccine.
The effect of vaccination dose was also analyzed on humoral immunity. MAV of anti-S IgG increased 4.46-fold during M20–23 compared to M10–13 in patients receiving one-dose vaccination; 2.77-fold during M20–23 compared to M10–13 in patients receiving multidose vaccination; and 4.71-fold in healthy donors (Fig. 2c). MAV of anti-NP IgG increased 12.76-fold during M20–23 compared to M10–13 in patients receiving one-dose vaccination; 9.01-fold during M20–23 compared to M10–13 in patients receiving multidose vaccination; and 3.65-fold in healthy donors (Fig. 2d). The results showed that the receipt of more than one vaccine dose did not elicit greater Ab response.
Dynamic changes in lymphocyte subsets and cytokines in COVID-19 convalescent patients
Dynamic changes in white blood cells (WBC), total lymphocyte count, lymphocyte subset count, and Th1-cytokines were also determined in COVID-19 convalescent patients. Results showed that WBC (Fig. 3a) and total lymphocyte count (Fig. 3b) were not significantly different in COVID-19 convalescent patients among groups during the follow-up, whereas in healthy controls, CD3+ (Fig. 3c) and CD8+ (Fig. 3d) T cell counts were significantly decreased during M10–13 and M20–23 (all p < 0.05), while CD45+ WBC counts (Fig. 3e) were significantly decreased during M10–13 (p < 0.05) and then returned to normal during M20–23. NK cell counts (Fig. 3f) were significantly increased during M20–23 (p < 0.05). Flow cytometry gating strategy is shown in Supplementary Figure S1. Supplementary Table S1 shows proportion of patients with normal and abnormal lymphocyte subsets at two periods, proportion of CD3+ and CD8+ decreased significantly during M10–13 and M20–23.
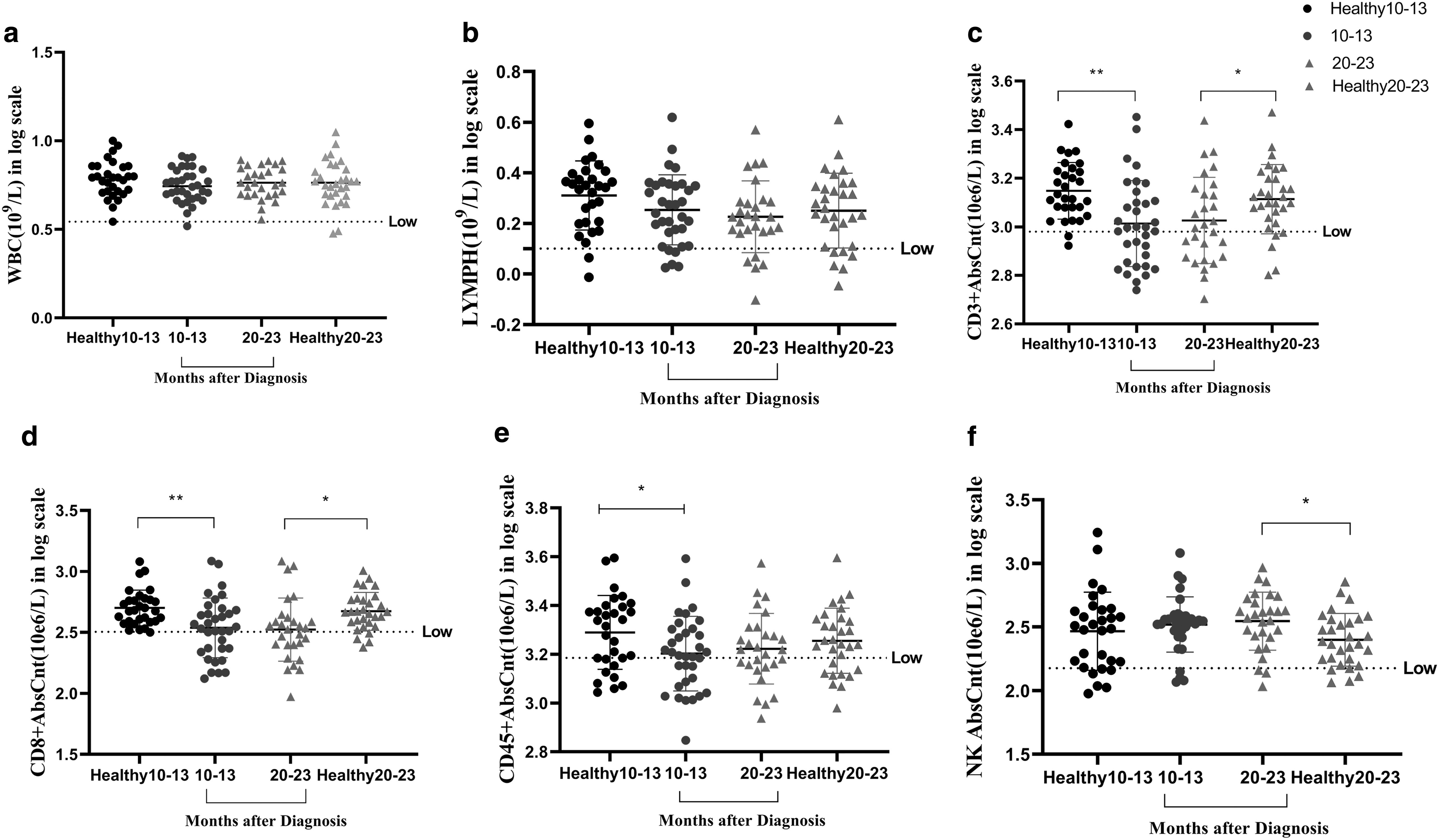
Dynamic changes in lymphocyte subsets in COVID-19 convalescent patients and healthy donors using standard hematological examination methods, including WBC
Levels of six cytokines were also analyzed in convalescent patients. Results showed that the response of these cytokines to infection was variable. Compared with healthy controls, IL-6 (Fig. 4d) and IFN-γ (Fig. 4e) levels were significantly reduced during M10–13 (all p < 0.01), while IL-2 (Fig. 4a) and TNF-α (Fig. 4f) levels were significantly increased during M10–13 (all p < 0.05). For the patients, IL-4 (Fig. 4b), IL-6, and IFN-γ levels were significantly higher during M20–23 compared to M10–13 (all p < 0.01). There was no significant difference in IL-10 (Fig. 4c) levels among all groups. The results suggested that increase of IL-2 and TNF-α levels might be associated with infection. Proportion of patients with normal and abnormal cytokines in both periods is shown in Supplementary Table S1. Proportion of IL-6 increased significantly during M20–23.
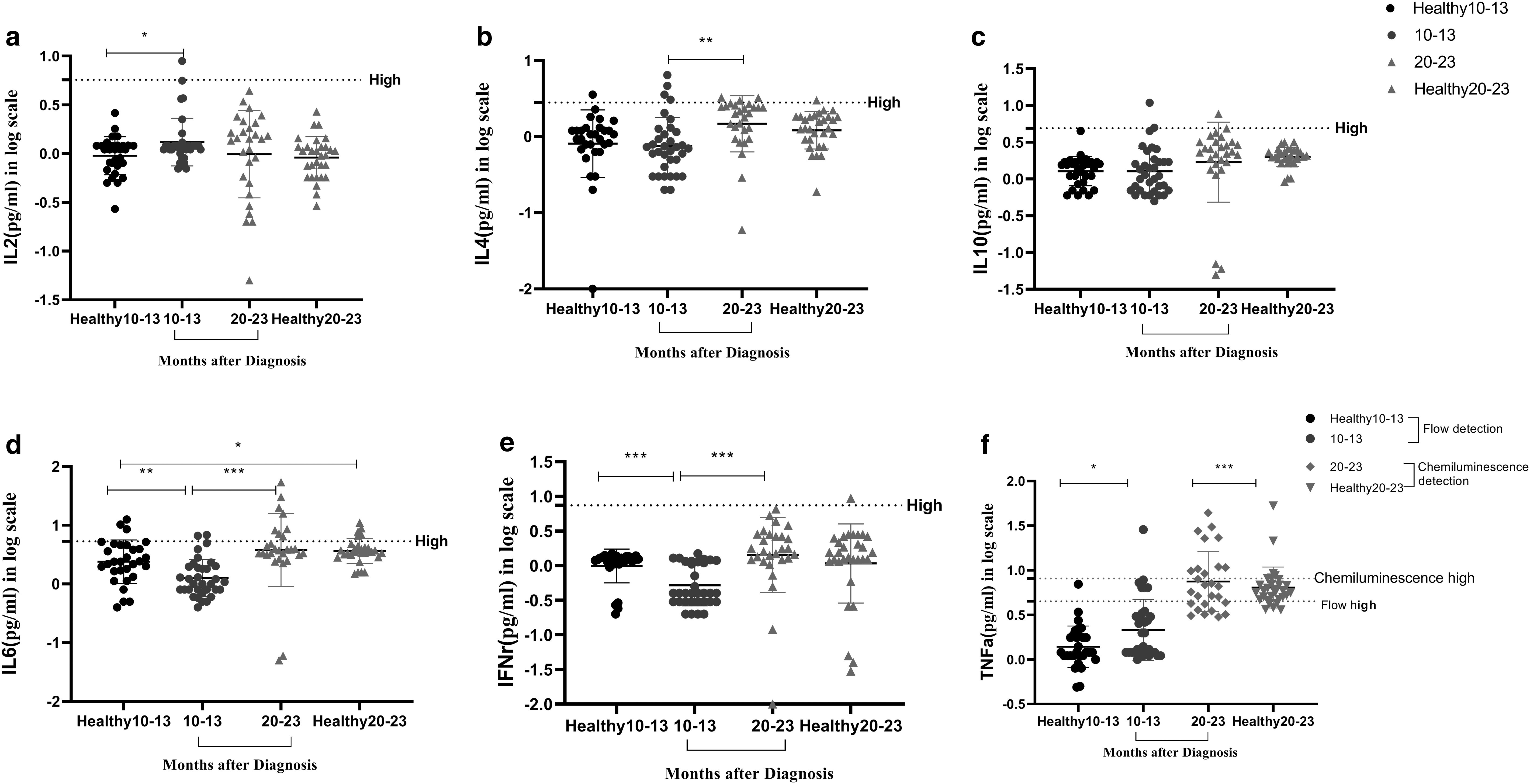
In total, six cytokines were analyzed in COVID-19 convalescent patients and healthy donors by flow cytometry, including IL-2
Pearson correlation was employed between lymphocyte subsets, Th1-cytokines, and Abs. Results showed that IFN-γ was positively correlated with SARS-CoV-2-specific total Abs (Supplementary Fig. S2a) and anti-NP IgG (Supplementary Fig. S2g). IL-6 was positively correlated with SARS-CoV-2-specific total Abs (Supplementary Fig. S2b) and anti-NP IgG (Supplementary Fig. S2f), and IL-6 was negatively correlated with anti-NP IgM (Supplementary Fig. S2c). NK was positively correlated with anti-NP IgM (Supplementary Fig. S2d). IL-4 was positively correlated with anti-NP IgG (Supplementary Fig. S2e).
Effect of comorbidities on Ab titer and lymphocyte subsets
We analyzed the effect of age, sex, loss of smell and taste, comorbidities, and disease severity on SARS-CoV-2-specific total Ab, anti-NP IgG, anti-S IgG, lymphocyte subsets, and Th1-cytokines. No significant association was found between age, sex, loss of smell and taste, or disease severity and SARS-CoV-2-specific total Ab, anti-NP IgG, anti-S IgG, lymphocyte subsets, or Th1-cytokines following infection. However, comorbidities (diabetes, cardiovascular disease, tumors, and so on) were strongly associated with SARS-CoV-2-specific total Ab, anti-NP IgG, anti-S IgG, and lymphocyte subsets. As shown in Table 2, in patients with one or more comorbidities (n = 17), CD3+, CD8+ T lymphocytes, and CD45+ WBC counts decreased significantly at two periods compared to the group (n = 17) without any comorbidity (p < 0.05), and CD4+ T lymphocytes were significantly decreased during M10–13 (p = 0.022).
Effects of Comorbidities on Antibody Titers and Lymphocyte Subsets in COVID-19 Convalescent Patients
Ab, antibody; IgG, immunoglobulin G; NP, nucleocapsid; S, spike.
More interestingly, titers of SARS-CoV-2-specific total Ab, anti-NP IgG, and anti-S IgG in patients with comorbidities were lower than those in patients without comorbidities after vaccination during M20–23 (p < 0.05), while there was no difference during M10–13. The result suggested that comorbidities (diabetes, cardiovascular disease, tumors, and so on) are associated with lower Ab titers following COVID-19 vaccination.
Discussion
In this study, we analyzed longitudinally the SARS-CoV-2-specific Ab, lymphocyte subsets, and cytokine responses in COVID-19 convalescent patients, 23 months after infection with SARS-CoV-2 (wild type), and divided them into two groups based on two time points before and after vaccination, compared to the healthy donors. To our knowledge, this is the longest observational study that reports dynamics of SARS-CoV-2-specific Abs, lymphocyte subsets, and cytokines over 23 months and the effect of vaccine on convalescent patients. The data revealed that anti-NP IgM was positive 2 years after infection in four convalescent patients, including three severe to critical convalescent patients and one mild patient.
As previously reported (Su et al., 2021), conclusions can be drawn now that the late disappearance of SARS-CoV-2-specific IgM may indicate a more serious condition; thus, prevention and surveillance of SARS-CoV-2 re-infection in the population should be strengthened. Approximately 97% of COVID-19 patients maintained SARS-CoV-2-specific total Ab, anti-NP, and anti-S IgG at least 10–13 months after infection. Although Abs represent only part immune response, the results suggested that COVID-19-positive patients develop a strong humoral immune response, and presence of SARS-CoV-2-specific anti-NP IgG and anti-S IgG Abs was associated with reduced risk of SARS-CoV-2 reinfection for at least one year, which is consistent with other recent studies (Capetti et al., 2021; Gallais et al., 2021; Li et al., 2021; Masiá et al., 2021).
The data also showed that the levels of SARS-CoV-2-specific total Ab, anti-NP IgG, and anti-S IgG were equivalent in prevaccinated convalescent patients compared to vaccinated healthy donors, but significantly higher by at least threefold in vaccinated patients. For most patients, the titer of these Abs increased at least threefold after vaccination. Our results in line with other research suggested that natural immunity may offer equal or greater protection against SARS-CoV-2 infections compared to individuals receiving SARS-CoV-2 vaccine; the combination of a previous SARS-CoV-2 infection and a respective vaccination, termed hybrid immunity, seems to confer the greatest protection against SARS-CoV-2 infections (Pilz et al., 2022).
Further, studies concerning changes in Ab levels in convalescent patients before and after vaccination provide insights into assessing the long-term efficacy of COVID-19 vaccines. Interestingly, anti-S IgG levels increased as early as 9 days after vaccination, which suggested that a robust memory B cell response is established in COVID-19 convalescents, including those with low Ab titers. Recent reports indicated that memory B cell clones expressing broad and potent anti-S Abs were retained selectively for at least one year after infection, and expanded after vaccination (Wang et al., 2021). Thus, durability of humoral responses after COVID-19 is obvious, and it may provide protection against SARS-CoV-2 infection for years (Huang et al., 2020; Wang et al., 2021).
In this study, correlation analysis of several Abs showed that SARS-CoV-2-specific total Ab correlated significantly positively with anti-NP IgG and anti-S IgG; and anti-NP IgG correlated significantly positively with anti-S IgG. Our results are inconsistent with other researchers (Ni et al., 2020; Pan et al., 2021), possibly because SARS-CoV-2-specific total Abs were detected in this study rather than neutralizing Abs. However, anti-NP IgG correlated with anti-S IgG; thus, this coordinated humoral immune response may be effective in blocking viral receptors to invade host cells. This collaborative response is important because these Abs are necessary for patients' recovery and prevention of reinfection of SARS-CoV-2. However, as SARS-CoV-2 is a new virus, the SARS-CoV-2-specific Ab changes still need further monitoring and investigation.
The effect of different vaccine types was also analyzed on the Ab levels of COVID-19 convalescent patients. As both anti-NP IgG and anti-S IgG immunoassays were performed, even the vaccinated patients could be analyzed for persistence of infection-induced immunity not generated by S-based vaccination. The results showed that in COVID-19 convalescent patients, protein subunit vaccine produced higher Ab titers than inactivated vaccine. However, it should be noted that only 7 (25%) vaccinated patients received protein subunit vaccines in this study. Larger samples are needed to study relationship between different vaccine types and specific immune response.
Because correlation between Ab levels and protection against a virus or disease may be nonmechanistic and not absolute correlates (Krammer, 2021), our observations in line with previously published studies also suggested that more than one vaccine dose was not associated with greater effectiveness (Hammerman et al., 2022; Stamatatos et al., 2021). Since maximal Ab response was elicited after only one vaccine dose in COVID-19 convalescent patients, multidose vaccination is not required for any population. Although longer longitudinal studies are needed, persistent Ab and avidity in this population may support a single-dose vaccination strategy. This would be a resource-conscious solution to help address global vaccine shortage.
Furthermore, lymphocyte subsets and cytokine responses to SARS-CoV-2 antigens were also studied in COVID-19 convalescent patients and healthy donors. Results showed that CD3+ and CD8+ T lymphocyte counts were significantly decreased during two periods in patients compared to healthy donors, while CD45+ WBC counts were significantly decreased during M10–13, returning to normal during M20–23. At the same time, proportion of CD3+ and CD8+ decreased significantly during two periods in patients compared to healthy donors.
Our results are inconsistent with the findings of other researchers (Hengeveld et al., 2020; Rank et al., 2021), where reports showed impaired cytotoxic CD8+ T cell response in elderly COVID-19 patients (Westmeier et al., 2020). The reason for significantly decreased cells in convalescent patients for up to 2 years after infection is possibly due to our investigation, which centered on elderly COVID-19 patients with comorbidities; however, it implied that they need more attention. Meanwhile, positive correlation of NK cell with IgM, in this study, is consistent with the findings of other researchers (Pan et al., 2021), indicating the development of IgM may be associated with the activation of antiviral NK cells.
Significantly higher proportion of COVID-19 convalescent patients during M20–23 presented with increased IL-6 levels. Several studies reported that IL-6 is one of the markers of severe COVID-19, being at higher levels in patients (Qin et al., 2020; Wan et al., 2020); however, in this study, patients had lower levels of IL-6 and IFN-γ during M10–13 than the healthy donors, but had increased levels of TNF-α during M10–13 and M20–23 than in healthy donors.
According to our results, there still were some COVID-19 patients who had elevated cytokines nearly 2 years after discharge. More studies are warranted to investigate the mechanism of abnormal cytokine levels in COVID-19 convalescent patients in the future. Interestingly, IL-6 levels increased significantly during M20–23. Recent reports indicated that mRNA derived from COVID-19 vaccine is a potent inducer for proinflammatory cytokine responses, which might also mediate autoimmune responses (rheumatoid arthritis or myocarditis) after COVID-19 vaccination (Nassar et al., 2021; Watanabe et al., 2022b). IFN-γ and IL-2 secretion specifically induced by the receptor-binding domain (RBD) following CoronaVac Vaccination persisted at high levels until 6 months and could be observed at 12 months (Zhao et al., 2022).
These results suggested that the significant increase in IL-6 levels during M20–23 may be caused by vaccination. Meanwhile, these findings that IL-6 was negatively correlated with IgM, but positively correlated with IgG might have been caused by vaccination. Thus, these results suggested that helper cells and cytokines such as IL-6, IFN-γ, and IL-4 play an important role in generating adequate Ab response to SARS-CoV-2 infection, and interactions between immune cells may help to speed up or delay the recovery of COVID-19 infection. Changes in these cytokines may be caused by infection or vaccination. In conclusion, although normal lymphocyte subsets and cytokines were found in most convalescent individuals, they may be the predictors of serum neutralization capacity in COVID-19 patients; however, the mechanisms need further research.
The effect of age, sex, loss of smell and taste, comorbidities, and disease severity was analyzed on Ab titers, lymphocyte subsets, and cytokines. Results suggested that CD3+, CD8+ T lymphocytes, and CD45+ WBC counts were significantly decreased in patients with one or more comorbidities at two periods, compared to the group without any comorbidity. It indicated that patients with comorbidities (diabetes, cardiovascular disease, tumors, and so on) are associated with decreased CD3+ and CD8+ T lymphocytes following COVID-19 infection.
Another interesting result showed that patients with comorbidities (diabetes, cardiovascular disease, tumors, and so on) are associated with lower Ab titers following COVID-19 vaccination; this is consistent with a study by Watanabe et al. (2022a). It has recently been reported that elderly patients and cancer patients also have lower Ab titers after receiving COVID-19 vaccine (Collier et al., 2021; Monin et al., 2021). These findings suggest that some of the more vulnerable subpopulations may respond to this vaccine in different ways. Whether this is linked to its nucleic acid nature or to the virus itself remains to be clarified and comparative studies of different types of vaccines are needed.
However, this study has several limitations. First, a relatively small sample size of study population, underrepresented patients with different types of vaccine, multiple or single doses, and multiple comorbidities, time of postvaccination sample collection (M20–23), which was 9–102 days after the last dose of vaccine, varying greatly between patients, and paucity of severe patients as only five (14.7%) were severe and critical cases in this study. Previous studies have shown that severe COVID-19 patients had higher Ab titers than other disease conditions (Lau et al., 2021; Wang et al., 2020).
Second, this single-center cohort study sampled patients only two times during research period, which limited a more dynamic observation of the immune response over time and limited the generalization of our research results. Third, due to lack of reagents, anti-RBD IgG and specific T and B lymphocytes (memory cells) could not be analyzed. Last, a neutralization test was not done to detect neutralizing antibody, which we can focus on in the next study.
In conclusion, this study provides 23 months of follow-up, the longest as per the reports in literature, to observe the dynamic changes of SARS-CoV-2-specific Ab, lymphocyte subsets, and cytokines in recovered patients. This suggests that COVID-19-positive patients develop a strong humoral immune response that reduces the risk of SARS-CoV-2 reinfection for at least 13 months, and vaccination has a beneficial promotion effect on Ab production. Receipt of more than one vaccine dose did not elicit greater Ab response; however, larger samples are needed to compare Ab titers by protein subunit vaccine compared to inactivated vaccine. Significantly decreased levels of CD3+ and CD8+ T lymphocyte counts in elderly COVID-19 convalescent patients with comorbidities for up to 2 years after infection suggest that they need more attention.
Changes in these cytokines may be caused by infection or vaccination. Comorbidities are associated with a decrease in CD3+ and CD8+ T lymphocytes, and lower Ab titers following COVID-19 infection. SARS-CoV-2-specific total Ab, anti-NP IgG, and anti-S IgG immunoassays were performed even in vaccinated patients, revealing persistence of infection-induced immunity not generated by S-based vaccination. Thus, this study focused on both cross-sectional (multiple patients) and time-series hard data.
Footnotes
Acknowledgments
The authors would like to thank all the doctors and nurses who contributed to blood sample collection and transportation, as well as all the convalescent patients involved in this study.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This work was funded by grants from Chongqing medical scientific research project (Joint project of Chongqing Health Commission and Science and Technology Bureau) (2021MSXM253), and Chongqing medical scientific research project (Joint project of Chongqing Health Commission and Science and Technology Bureau) (2020FYYX232).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.