
Abstract
We determined anti-rubella and anti-measles immunoglobulin G (IgG) in 7- to 19-year-old children and adolescents with vaccine only-induced immunity of Córdoba, Argentina, during a 6-month period over 2021–2022. Of the 180 individuals studied, 92.2% and 88.3% were positive for anti-measles and anti-rubella IgG, respectively. No significant differences were found comparing anti-rubella IgG concentrations (p = 0.144) and anti-measles IgG concentrations (p = 0.105) of individuals classified by age, but anti-measles IgG and anti-rubella IgG levels were significantly higher among female individuals compared with males (p = 0.031 and p = 0.036, respectively). Female subjects in the younger age group had higher concentrations of anti-rubella IgG as well (p = 0.020), even when anti-measles IgG concentrations did not differ among female age-subgroups (p = 0.187). In contrast, age subgroups of male individuals did not have significantly different IgG concentrations for rubella (p = 0.745) or measles (p = 0.124). Among samples with discordant results (22/180, 12.6%), 9.1% were negative for rubella but positive for measles; 13.6% were equivocal for rubella and positive for measles; 22.7% were equivocal for rubella and negative for measles, while 54.5% were positive for rubella but negative for measles. The findings indicate a seroprevalence below recommended for preventing measles in the population studied, while they evidence the need for standardization of serological tests for rubella IgG.
Introduction
Measles vaccine was included in the national immunization schedule of Argentina in 1978 (Biscayart et al., 2018; Luthy and Kantor, 2020). Following Pan American Health Organization/World Health Organization (PAHO/WHO) recommendations, a measles control and elimination program was implemented in 1993. Periodic, massive immunization campaigns and the Measles National Surveillance Network conducted a marked reduction in cases, reaching maximum at the end of the 20th century.
The last large autochthonous outbreak of measles occurred in 1998 (Isa et al., 1999), coinciding with the incorporation of measles, mumps and rubella (MMR) vaccine into the national immunization calendar. With a 2-dose scheme (at 12 months and at 4–6 years old) (Ministerio de Salud de la Nación, 1997), this strategy led to only six measles cases confirmed in the year 2000 (Isa et al., 2009) and sporadic imported cases detected after that (28 cases confirmed nation-wide between 2009 and 2017) (Biscayart et al., 2018).
Regarding rubella, epidemics in Argentina occurred every 5–8 years before vaccination, accompanied by an increase in cases of congenital rubella syndrome (CRS). The largest outbreak, with more than 85,000 postnatal cases, was registered in 1992 and the last rubella outbreak took place in 2007–2008, when 2,218 postnatal cases and 3 CRS cases were notified. No autochthonous cases have been detected since 2009 and a few imported rubella cases have been reported in 2011, 2012, 2014, and 2019 (Ministerio de Salud de la Nación, 2022a; Ministerio de Salud de la Nación, 2014).
The Sanitary Region of the Americas certified the elimination of endemic transmission of rubella in 2015 and measles elimination goal was achieved in 2016 (PAHO/WHO 2016; PAHO/WHO, 2015). However, an extended measles outbreak occurred during 2019–2020, with 23,961 cases reported, including 21 deaths, in 15 countries of the region (PAHO/WHO 2020a; PAHO/WHO, 2020b). During this outbreak, 183 cases (1 death) were confirmed in Argentina (Ministerio de Salud de la Nación, 2020; WHO, 2022).
The current global scenario sustains the chances for re-introduction from regions where outbreaks are still occurring, such as Africa, Asia, and Europe (WHO, 2022). This year, two imported measles cases were detected in Argentina after exposure in Africa and Europe (Ministerio de Salud de la Nación, 2022b). In addition, the immunological window probably increased in children due to the difficulties in vaccinating during COVID-19 pandemic and the growing vaccine hesitancy.
Therefore, monitoring the level of protection against measles and rubella is suggested, especially among individuals who have not had the infection naturally. In this study, we aimed at determining the immune status against measles and rubella in individuals from Córdoba, Argentina, who should have received two doses of MMR and no natural contact with these viruses, according to the national immunization schedule and data of the integrated epidemiological surveillance program for measles, rubella, and CRS.
Materials and Methods
Study design, samples, and inclusion/exclusion criteria
A retrospective, descriptive, cross-sectional study was carried out. The population studied included male and female individuals born between September 1, 2002, and August 31, 2014. They were 7–19 years old, should have received the two doses of MMR according to the national immunization schedule, and, considering surveillance data, were not exposed to natural measles of rubella infection.
Individuals included in the study population were selected among patients who attended for routine biochemical analysis during September 2021 through February 2022 at Fundación para el Progreso de la Medicina (FPM), a main diagnosis center of Córdoba, Argentina. The minimum sample size was calculated using the mean number of 7- to 19-year-old-individuals attending FPM during a 6-month period (N = 250), with 95% confidence level, 3% precision and expected proportion of loss, and 85% assumed seroprevalence.
To maximize the sample, we took into account the primary failure of anti-measles vaccine component (since 5–10% do not develop antibodies) and also considered data of a local survey of vaccine hesitancy (Sepich et al., 2021), which revealed that 5% of parents do not vaccinate their children with all the recommended vaccines.
With these parameters, the minimum sample size was 177. Cryopreserved serum samples from individuals within the target population were randomly selected from the FPM biobank. One serum sample per individual was included. Hemolyzed, lipemic, or insufficient volume samples (<500 μL) were excluded, as well as those samples from individuals with diagnoses that could influence the response generated by vaccine, due to either the pathology itself or treatment.
Antibody assays
Determination of anti-rubella virus immunoglobulin G (IgG) was performed using ARCHITECT Rubella IgG chemiluminescent microparticle immunoassay (CMIA) system from ABBOTT Diagnostics G.m.b.H. (ABBOTT) strictly following the manufacturer's instructions, including the three-concentration controls. Sample results ≥10 IU/mL were considered positive and ≤4.9 IU/mL negative, whereas 5.0–9.9 IU/mL was “greyzone” (equivocal), as expressed by the ABBOTT reagent insert.
Anti-measles virus IgG was determined using Measles G Antibody Test System from MBL Bion, intended as an indirect fluorescent assay for qualitative or semi-quantitative detection. The procedure was performed as stated by the manufacturer. As indicated, a laboratory-standardized protocol was used to establish the positive control titer. According to this, a sample was considered positive if it exhibited the characteristic staining pattern at a dilution ≥1/16. Samples were considered negative when exhibiting less than 1+ fluorescence at a dilution <1/16.
Data analysis
Prism-GraphPad software was used for statistical analysis of data, applying Chi-squared, analysis of variance and Kruskal–Wallis tests as required, with a significance level α = 0.05.
Results
We tested 180 serum samples, 100 (55.6%) of female and 80 (44.4%) of male individuals. Rubella and measles seroprevalence was 92.2% and 88.3% (p = 0.213), respectively (Fig. 1). No significant differences were observed regarding concentration of anti-rubella IgG (p = 0.144) and anti-measles IgG (p = 0.105) when comparing individuals classified by age groups.
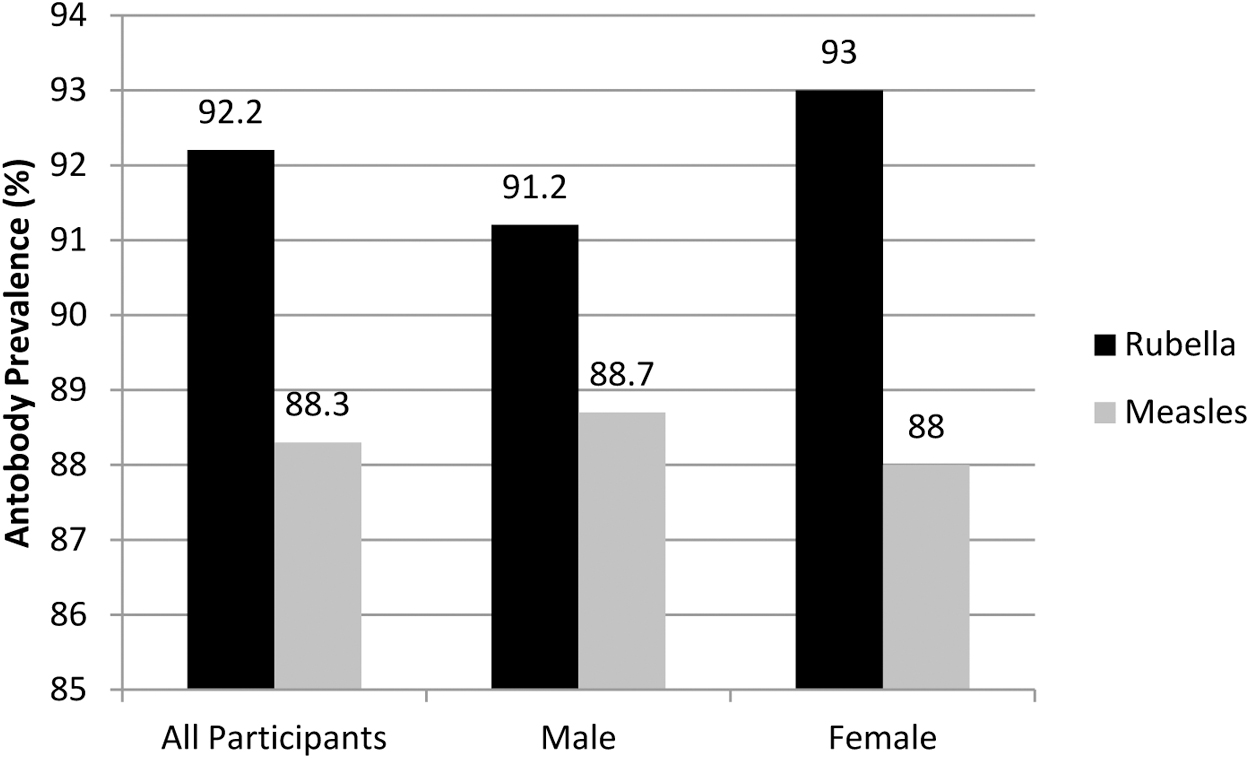
Prevalence of anti-rubella and anti-measles virus IgG among 7 to 19 year-old healthy chiildren and adolescents from Córdoba, Argentina, 2021–2022. No statistically significant differences were identified between men and women in the prevalence of antibodies against rubella (p = 0.7815) and measles (p = 0.5336). ABBOTT, ABBOTT Diagnostics G.m.b.H.; CMIA, chemiluminescent microparticle immunoassay; IgG, immunoglobulin G.
However, when individuals were classified by sex and age subgroups analyzed, anti-rubella IgG concentration among female individuals was significantly higher in the youngest group (p = 0.020), whereas no significant differences were identified among measles titers (p = 0.187). By contrast, no significant differences were identified comparing rubella (p = 0.745) or measles (p = 0.124) antibody titers among male individuals of different age groups (Table 1). Female individuals in the whole study sample had a significantly higher rubella IgG concentration (p = 0.0036) and measles IgG titer (p = 0.0310).
Frequency of Anti-Rubella IgG and Anti-Measles IgG Among 7–19-Year-Old Healthy Children and Adolescents, Classified by Sex and Age Range. Córdoba, Argentina, 2021–2022
The values highlighted in bold are those that are statistically significant.
The differences observed when comparing anti-rubella or anti-measles antibodies among all participants or among female and male participants grouped by age were not statistically significant except for anti-rubella IgG among female age subgroups (*). In addition, statistically higher concentrations of anti-rubella IgG (p=0.036) and anti-measles IgG (p=0.031) were observed among all female individuals compared to male (**).
IgG, immunoglobulin G; IQR, interquartile range; Max, maximum; Min, minimum; POS, positive; RUBELLA, Rubella virus.
In 158 out of 180 (87.8%) samples, anti-rubella IgG and anti-measles IgG results were concordant: 154 (85.6%) positive and 4 (2.2%) negative. Twenty-two samples (12.6%) had discordant results: 2 (9.1%) were negative for rubella IgG but positive for measles IgG; 3 (13.6%) were equivocal for rubella and positive for measles; 5 (22.7%) were equivocal for rubella and negative for measles; and 12 (54.5%) were positive for rubella but negative for measles.
Discussion
Rubella has a considerably lower basic reproductive rate (R0) than measles: 5–7 versus 12–18 (Lambert et al., 2015). This explains why, given that rubella vaccine coverage is practically the same as for measles, no extended rubella outbreaks have been reported. In addition, primary vaccine failure does not appear to participate in sustained rubella transmission.
Considering their R0s, the population immunity necessary to prevent viral transmission can be estimated at 83–85% for rubella and 92–94% for measles (Moss et al., 2021). Therefore, we can conclude that the current prevalence of anti-rubella antibodies found in our study population is sufficient to prevent local circulation of the virus, whereas the situation is different for measles. These results are in agreement with a study of fertile-aged women in Córdoba during 2020 showing that 20% were susceptible to measles (Tenaglia et al., 2021). Due to the age-range studied (as older participants that might have had natural infection were included), in this work vaccine-induced as well as naturally acquired immunity are possible, in contrast to our study. In spite of that, a more generalized decrease regarding measles protection is revealed.
The difference that we observed between rubella and measles seroprevalence in this paper (92.2% vs. 88.3%, respectively), although not statistically significant, could respond to biological causes and be multi-factorial. For instance, the primary failure is higher for the measles component of MMR (Lambert et al., 2015). In addition, it has been reported that anti-measles antibodies decline over time in a greater proportion than anti-rubella antibodies (Seagle et al., 2018).
On the other hand, the higher IgG concentration in females compared with males after vaccination for both rubella and measles (p = 0.036 and p = 0.031, respectively; Table 1) from our study group is consistent with previous findings that account for stronger immune responses in women. They can produce not only higher levels but also more functional antibodies, accompanied by a higher frequency of adverse reactions and a greater probability of developing autoimmune diseases (Fischinger et al., 2019).
With all of the above, samples with discordant results are expected (mainly rubella-positive/measles-negative). Also, samples with results rubella-equivocal/measles-negative could be expected. Two individuals were negative for rubella but positive for measles, implying more complex interpretations. With respect to this, anti-rubella antibodies may not be directly comparable when using different methodologies, due to the characteristics of the international standards that have been distributed since the 1980s; thus, equivocal results by CMIA probably contain low levels of antibodies (Dimech et al., 2016). It is possible, then, that the seroprevalence found here is underestimated.
To overcome this problem, currently it is suggested that manufacturers develop qualitative tests with high sensitivity and specificity, rather than quantitative tests that measure antibodies in IU. In addition, rubella virus reinfection has been described in people who had specific IgG levels >15 IU/mL when assayed by different techniques such as enzyme-linked immunosorbent assay (91 UI/mL) and radial hemolysis (>15 IU/mL) (Aboudy et al., 2000; Dimech et al., 2016; Sawlani et al., 2013; Thayyil et al., 2016).
Therefore, the assumption that an anti-rubella IgG result >10 IU/mL indicates protection against infection or reinfection (while <10 IU/mL indicate susceptibility) may occasionally be incorrect (Cusi et al., 1993; O'Shea et al., 1994; Skendzel, 1996). The lack of standardization may affect not only seroprevalence studies but also individual results when analyzing diagnostic situations, as the findings depend on the tests used (Dimech et al., 2013), so these studies contribute to rubella elimination.
The results of this study are interpreted according to the WHO's immunization coverage goals; however, specific cellular immunity and non-specific immunity add to the immune state against an infection (Griffin, 2018). A dilution as high as 1/120 positive for measles IgG by neutralization assay is known to be protective for measles (Hatchette et al., 2017), whereas this value is unknown for rubella (Seagle et al., 2018).
Thus, having antibody concentrations below the positive cut-off value by a certain method does not necessarily imply that the individual is susceptible to infection. Beyond limitations raised, our data support the need to sustain efforts to maintain a sufficiently high prevalence of measles and rubella antibodies induced by vaccination, particularly when there is a lack of stimuli that reinforce immunity, such as wild viruses that do not circulate naturally in our region, especially regarding measles, for which a seroprevalence slightly below the target could allow reintroduction.
Footnotes
Acknowledgments
Agustín Dalmazzo and Magalí Ridano for assistance with statistical analysis and presentation.
Authors' Contributions
M.P., M.B.I., S.N., and M.P.A. contributed to the study conception and design. Material preparation and data collection were performed by M.P., M.I.R., G.H., J.A., M.T., M.B.C.S., and J.J.M. Analysis was performed by M.P., M.B.I., S.N., and M.P.A. The first draft of the manuscript was written by M.P. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Training, Teaching and Research Committee of FPM, Córdoba, Argentina.
Author Disclosure Statement
The authors have no relevant financial or non-financial interests to disclose.
Funding Information
No specific funding was received for this study.