
Abstract
Although cytomegalovirus (CMV) and Epstein–Barr virus (EBV) are considered latent viruses, their reactivation occurs in immunosuppressed conditions. We previously reported that CMV and EBV are reactivated in patients receiving immunosuppressive therapy and/or chemotherapy. This retrospective, single-center study aimed to determine the frequency of viral reactivation and clinical characteristics of patients with B cell lymphoma (B-ML) receiving chemotherapy. Twenty-four patients (mean age 73 years, range 40–87 years; male-to-female ratio, 15:9) with diffuse large B cell lymphoma (n = 15), follicular lymphoma (n = 8), or mantle cell lymphoma (n = 1) were enrolled. Serum CMV and EBV DNA levels were analyzed using quantitative real-time polymerase chain reaction in patients with B-ML receiving chemotherapy. We determined the cumulative reactivation of each virus and analyzed the relationship between viral reactivation and clinical characteristics. Three patients experienced relapse or refractory (R/R) disease and the others had de novo lymphomas. The frequencies of CMV and EBV reactivations were 54.2% and 37.5%, respectively. CMV reactivation occurred significantly earlier during chemotherapy courses in R/R patients than in de novo patients (p = 0.0038), while EBV reactivation was frequently found before treatment. Baseline serum levels of soluble interleukin-2 receptor were higher (4318.0 vs. 981.1 U/mL, p = 0.010) and hemoglobin levels were lower (11.1 vs. 13.0 g/dL, p = 0.0038) in patients with EBV reactivation than in those without reactivation. These findings were not observed in patients with CMV reactivation. CMV reactivation was associated with iatrogenic immunosuppression, whereas EBV reactivation was related to immunosuppression by lymphoma, indicating that the mechanisms of these viral reactivations differed.
Introduction
Cytomegalovirus (CMV) and Epstein–
Reactivation and reentry of a lytic cycle of herpesviruses can be triggered by a broad range of physiological and environmental factors, including immunosuppression, stress, chemotherapy, radiotherapy, hypoxia, infection with other pathogens, and prostaglandins (Weidner-Glunde et al., 2020). CMV and EBV are normally held in abeyance as latent viruses through cellular and immune surveillance mechanisms. Viruses frequently reactivate in immunosuppressed patients receiving steroid therapy and chemotherapy. Recently, multiple instances of viral reactivation within the Herpesviridae family have been reported. Reactivation of latent viruses is extremely common in patients with prolonged sepsis and is consistent with the development of immunosuppression (Walton et al., 2014).
These viral reactivations are also associated with poor outcomes in hematopoietic stem cell transplantation (Li et al., 2022; Zhou et al., 2020). Patients who developed coreactivation of CMV and EBV had worse outcomes in terms of lower 1-year overall survival and leukemia-free survival, and the coreactivation was associated with prolonged CMV or EBV duration and poor CD4+CD25+ T cell reconstitution on day 30 post-transplantation. It is therefore reasonable to assume that coreactivation of CMV and EBV may indicate an even more severe clinical condition than that for the reactivation of each virus alone. The incidence and clinical characteristics of patients with B cell lymphoma (B-ML) receiving treatment, for these viral reactivations, are unknown.
We previously reported that CMV and EBV are reactivated in patients receiving immunosuppressive therapy and/or chemotherapy, and our results suggested an association between their reactivation and aging and treatment intensity (Hatayama et al., 2020). The relationship between viral reactivation and chemotherapy requires further investigation. Thus, this study aimed to determine the frequency of CMV and EBV reactivation and the clinical characteristics of patients with B-ML receiving chemotherapy.
Materials and Methods
Patients and clinical samples
Archived serum samples from patients who were diagnosed with B-ML who received chemotherapy at the Tottori University Hospital, Tottori, Japan, from 2021 to 2022 were used in this study. Serum samples were collected before treatment and at the end of each treatment cycle and were stored at −20°C until they were used in this study. Clinical information including patient age, sex, disease, stage, regimen, and response, was retrospectively collected. Laboratory data were also collected retrospectively. Complete blood count was assessed using the XN3000 analyzer (Sysmex, Kobe, Japan). Biochemical tests were performed using the LABOSPECT 008α platform (Hitachi High-Tech Co., Tokyo, Japan). Moreover, interleukin-6 was measured utilizing the Cobas e801 system (Roche, Basel, Switzerland), using a sandwich electrochemiluminescence immunoassay. Measurement of soluble IL-2 receptor (sIL-2R) was conducted using the Lumipulse L2400 system (Fujirebio, Inc., Tokyo, Japan), using a chemiluminescence enzyme immunoassay.
This study was approved by the Ethics Committee of the Tottori University Faculty of Medicine (registration no: 21A061). Informed consent was obtained using an opt-out approach.
Viral DNA quantification
DNA was extracted from 200 μL of serum or plasma using commercial DNA isolation reagents (QIAGEN, Tokyo, Japan). Primers for the CMV glycoprotein B region and EBV BamHI-W region sequences were designed as shown in Table 1 (Takara Bio, Kusatsu, Japan). Real-time detection polymerase chain reaction (PCR) was conducted using a 20 μL reaction mixture containing 900 nM of forward and reverse primers, 250 nM TaqMan Probe, TaqMan Universal PCR Master Mix (Applied Biosystems, Waltham, MA, USA), and a 5 μL template (equivalent to 20 μL of plasma or serum). The mixture was incubated at 50°C for 2 min for the initial activation of uracil-N-glycosylase, followed by the inactivation of uracil-N-glycosylase at 95°C for 5 min. Subsequent PCR amplification consisted of 50 cycles of denaturation at 95°C for 15 sec and annealing and extension at 60°C for 1 min in an ABI7500 FastDX Real-time PCR System (Applied Biosystems).
Primer and Probe Design
CMV, cytomegalovirus; EBV, Epstein–Barr virus; WHO, the World Health Organization.
The CMV DNA reference panel derived from the AD169 strain, which is the World Health Organization International HCMV standard, was purchased from the National Institute for Biological Standards and Control (NIBSC, Ridge, Hertfordshire, UK). This material was assigned a concentration of 5 × 106 International Units when reconstituted in 1 mL of nuclease-free water. For the EBV DNA reference, DNA extracted from the Namalwa cell line was used. Namalwa is a diploid cell line that contains two integrated copies of the EBV genome, and the copy number was calculated from the DNA concentration as a conversion factor of 6.6 picograms (pg) of DNA per diploid cell, where 3.3 pg of Namalwa DNA corresponds to one copy number of the EBV genome.
The Namalwa cell line was kindly provided by the University of Tokyo (Uchimaru et al., 1997). Serial dilutions were performed to create standard curves with reference DNA, and the DNA levels were calculated. Low detection limits of CMV and EBV DNA measurements have been reported previously (Hatayama et al., 2020; Hatayama et al., 2016).
Statistical analyses
All statistical analyses were performed using EZR software (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a Japanese user interface for R (The R Foundation for Statistical Computing, Vienna, Austria) (Kanda, 2013). Cumulative incidence methods were used to estimate the rates of therapeutic responses and viral coreactivation in patients with relapsed or refractory (R/R) and de novo lymphomas by applying a competing risk analysis and were compared using the log-rank test. Gray's test comparing treatment arms was also performed. Comparisons among groups were performed using the Mann–Whitney U test, and p-values <0.05 were considered statistically significant.
Results
Patient characteristics
The characteristics of the study population with B-ML are presented in Table 2. We enrolled 24 patients with diffuse large B-ML (n = 15), follicular lymphoma (n = 8), or mantle cell lymphoma (n = 1). The median patient age was 73 years (range, 40–87 years), and 136 serum samples were analyzed. The male-to-female ratio was 15:9. Three cases were R/R diseases, whereas the remaining cases were de novo. Nine patients showed bone marrow infiltration. All patients received anti-CD20 antibody therapy for B-ML. Four patients were treated with a reduced treatment intensity. Thirteen patients achieved complete remission (CR).
Clinical Characteristics of Patients with B Cell Lymphoma
BR, bendamustine and rituximab; CR, complete remission; nt, not tested; R-CEOP, rituximab, cyclophosphamide, etoposide, vincristin, prednisolone; R/R, relapsed or refractory.
Frequency of viral reactivation
CMV and EBV reactivation occurred in 54.2% and 37.5% of patients, respectively. The median number of days preceding viral reactivation was 64.5 days (range, 0–143 days) for CMV and 0 day (range, 0–123 days) for EBV (Fig. 1a, b). CMV reactivation was found during chemotherapy for B-ML, while EBV was often positive before treatment, and reactivation during treatment was rare. There was no significant difference in the cumulative positive rate between the CR and non-CR groups (CMV p = 0.26, EBV p = 0.29, Gray's test) (Fig. 1c, d). The cumulative positive rate showed that reactivation occurred significantly earlier in the R/R group than in the de novo group (CMV p = 0.0022, EBV p = 0.86, Gray's test) (Fig. 1e, f). CMV DNA positivity tended to be transient in patients who finished the treatment successfully.
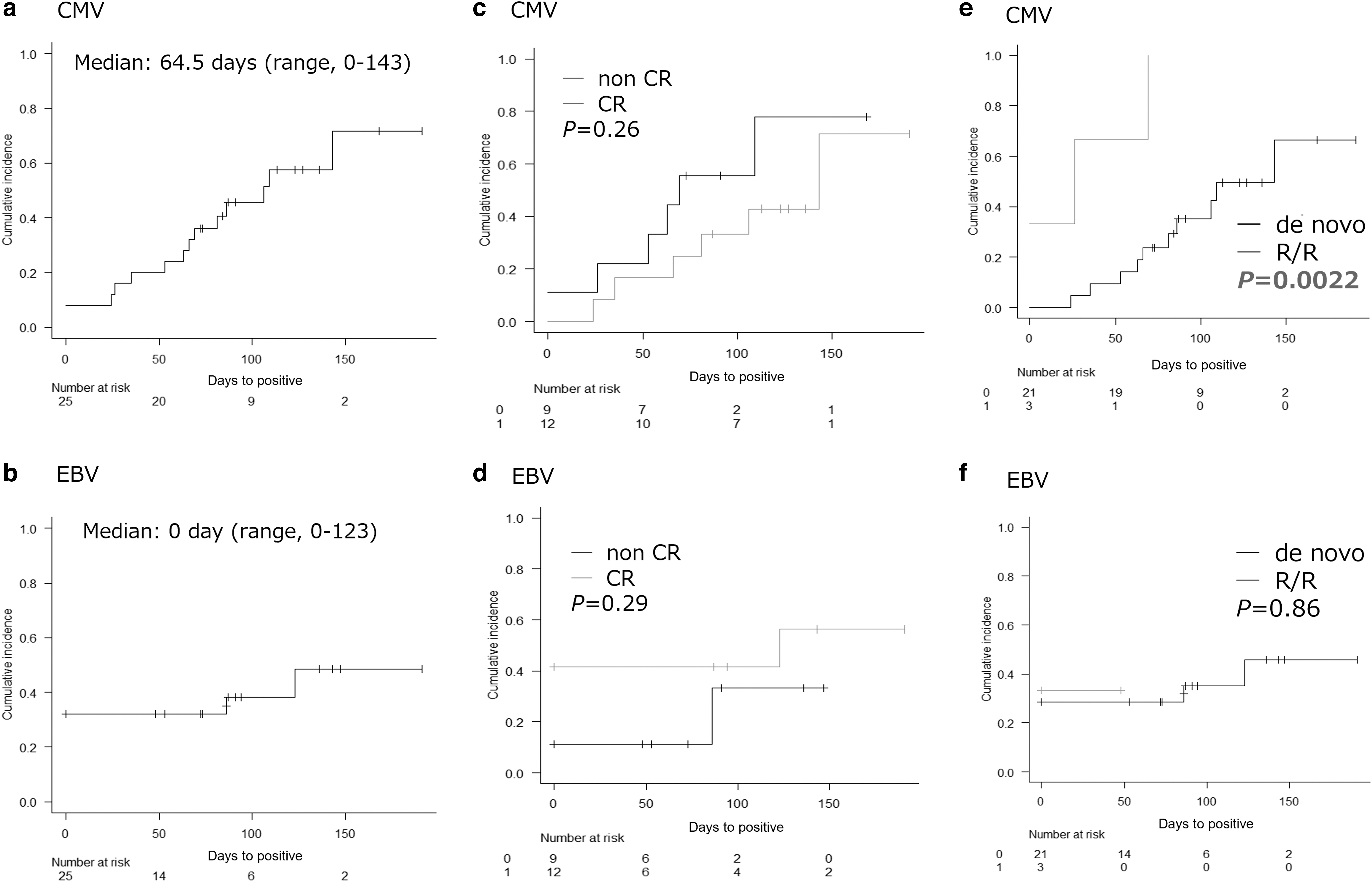
Cumulative positivity rate of CMV
In contrast, EBV DNA became negative immediately after starting treatment (data not shown). No patient developed complications due to viral reactivation.
Viral reactivation and laboratory data
Table 3 shows the viral reactivation and laboratory data at diagnosis. Patients with EBV reactivation had significantly lower hemoglobin levels (11.1 vs. 13.0 g/dL, p = 0.0038) and higher sIL-2R levels (4318 vs. 981.1 U/mL, p = 0.01) than those without reactivation. However, no significant differences were found between patients with CMV reactivation and those without reactivation (Table 3). After initiating treatment, sIL-2R levels showed a decrease regardless of the occurrence of viral reactivations. In addition, the significant difference in sIL-2R levels between the EBV-positive and EBV-negative groups became indistinguishable (data not shown).
Viral Reactivation and Laboratory Data
abs, absolute; Alb, albumin; Hgb, hemoglobin; Ig, immunoglobulin; IL-6, interleukin-6; LD, lactate dehydrogenase; Ly, lymphocyte; Neu, neutrophil; NLR, neutrophil lymphocyte ratio; PLT, platelet; sIL-2R, soluble interleukin-2 receptor; WBC, white blood cell.
Discussion
Herpesviruses can reactivate from latent to lytic infection. Reactivation and reentry of the lytic cycle of CMV and EBV can be triggered by a broad range of physiological and environmental factors. Immunosuppression owing to exposure to UV radiation, stress, or chemotherapy is a common inducer of the lytic cycle of all herpesviruses (Weidner-Glunde et al., 2020). We found a high frequency of CMV reactivation during chemotherapy, particularly in R/R cases. In the case of CMV, reactivation is observed during myeloid differentiation, which is associated with cytokine secretion. CD34-positive hematopoietic stem cells and CD33-positive myeloid progenitors serve as the main reservoirs for latent CMV, which develop into latently infected CD14-positive monocytes. Latent CMV can be reactivated in these cells as a consequence of differentiation toward macrophages and myeloid dendritic cells driven by proinflammatory cytokines (interferon-γ, tumor necrosis factor-α, interleukin-4, and granulocyte macrophage colony-stimulating factor) (Hahn et al., 1998; Reddehase and Lemmermann, 2019).
The current findings suggest that CMV reactivation is triggered by repeated chemotherapy-induced bone marrow suppression, recovery of hematopoietic stem cells, and cell differentiation, and is accumulated during the treatment course. EBV is mainly dormant in B cells, which are therapeutic targets for B-ML, and this may explain why EBV reactivation during chemotherapy was rare in this study.
Comparing these viral reactivations with laboratory data, patients with EBV reactivation had significantly lower levels of hemoglobin and higher levels of sIL-2R than those without reactivation, relating to the profoundly immunosuppressive environment in lymphoma; however, there was no such relationship found in patients with CMV reactivation. Tumor progression has been suggested to promote EBV reactivation. Several in vitro studies have reported the potential role of sIL-2R in the immune system (Damoiseaux, 2020). It has also been reported that recombinant sIL-2R suppresses T cell proliferation in vitro (Chopra et al., 1989; Lindqvist et al., 2010). In particular, the shedding of sIL-2R by Tregs is thought to produce a decoy receptor for IL-2, resulting in the inhibition of T cell responses.
Furthermore, the addition of sIL-2R to Tregs increases their activation and proliferation. The resulting increase in Treg activity was reported to suppress antitumor immunity by inhibiting the proliferation of CD8-positive T cells in tumor tissues (Yang et al., 2011). IL-2 plays a crucial role in the activation and survival of effector T cells, specifically CD8-positive T cells (Boyman and Sprent, 2012). On the contrary, Treg cells predominantly consume IL-2 through high-affinity IL-2 receptors and have limited production of IL-2, thereby limiting the amount of IL-2 in the microenvironment. Thus, the lack of IL-2 essential for their activation causes effector T cells to become dysfunctional. Furthermore, IL-10 and IL-35 act by suppressing the function and proliferation of effector T cells through downregulating the expression of major histocompatibility complex and costimulatory molecules on antigen processing cells (Akdis and Akdis, 2014; Sawant et al., 2015).
Although this study clearly showed the differential reactivation patterns of CMV and EBV in patients with B-ML receiving chemotherapy, there are several limitations to our study. The small sample size derived from the single center contributes to less generalizability. Thus, this prospective study should be performed with a larger sample size in the future to validate our results.
Conclusions
CMV and EBV reactivation was frequently observed in patients with B-ML receiving chemotherapy. CMV is strongly affected by chemotherapy-induced myelosuppression, and EBV is likely associated with the immunosuppressive state induced by lymphoma before treatment. These findings may indicate variations in the host responses to these viruses and imply that the mechanisms underlying these viral reactivations are distinct.
Footnotes
Acknowledgment
We would like to thank Editage for English language editing.
Authors' Contributions
Y.H. designed and performed the study and wrote the first draft of the article; K.W. and H.I. acquired and analyzed the data; T.M., T.F., and K.K. supervised the study and reviewed and edited the article.
Ethical Approval
This study was approved by the Ethics Committee of the Tottori University Faculty of Medicine (approval no.: 21A061). Informed consent was obtained using an opt-out approach. All methods were carried out in accordance with relevant guidelines and regulations.
Availability of Data and Materials
The data sets generated and analyzed during the current study were maintained by our institution under a secure server and are not publicly available because they contain protected health information. The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by JSPS KAKENHI (grant no.: 21H04276).