
Abstract
Infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) stimulates the plasma B cells to secrete specific antibodies against the viral antigen. However, not all antibodies can prevent the virus from entering the cells. The subpopulation of antibodies which blocks the entry of the virus into host cells is termed neutralizing antibodies (NAbs). The gold standard test for the detection of NAbs is the viral plaque reduction and neutralization test; however, various other methods can also be utilized to detect NAbs. In this study, we have developed an Enzyme Linked Immunosobent Assay (ELISA)-based protocol for rapid detection of SARS CoV-2 NAb by inhibiting the binding of the spike protein receptor-binding domain to angiotensin converting enzyme 2 and compared it with cPASS neutralizing antibody kit, which was approved by the Food and Drug Administration (FDA). The results obtained suggest that the in-house ELISA developed for the detection of NAbs against SARS-CoV-2 is rapid and reliable. Compared to FDA-approved GenScript's cPass assay, the specificity and the sensitivity of the in-house-developed ELISA kit were 100% (95% confidence intervals of 69.15–100.00) and 96% (95% confidence intervals of 86.29–99.51), respectively. Thus, the ELISA protocol developed to test the neutralizing activities of antibodies is rapid, which requires a BSL-2 infrastructure facility and can be easily performed. It has very high potential applications in the rapid screening of NAb against SARS-CoV-2.
Introduction
The causative agent of coronavirus disease 2019 (COVID-19) is severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is known to be infectious in humans. The SARS-CoV-2 virus has a positive sense, single-stranded RNA genome, which has about 29,903 nucleotide sequence that makes about 14 genes that are transcribed into ∼27 proteins (Andersen et al., 2020; Zhou et al., 2020). It includes nonstructural proteins (nsp1–14), structural proteins, and accessory proteins. Structural proteins include spike (S), envelope (E), membrane protein (M), and nucleocapsid (N) proteins (Mishra et al., 2021; Satarker and Nampoothiri, 2020; Shereen et al., 2020).
The spike (S) protein is involved in the recognition of host cell receptors and the cell membrane fusion process. The spike protein consists of two subunits known as the S1 and S2. Out of the two subunits, S1 subunit of the spike protein contains the receptor-binding domain (RBD), which recognizes the host cell surface receptor, that is, angiotensin converting enzyme-2 (ACE2). Several studies have reported that the RBD of the virus spike protein displays a strong binding affinity to the human ACE2 receptor, which leads to endocytosis in the host cells (Lempp et al., 2021), on the contrary, the S2 subunit mediates the fusion of the viral and the host cell membranes by forming a six-helical bundle via the two heptad repeat domains (Jackson et al., 2022).
Human ACE2 is known to convert a peptide hormone known as angiotensin I to angiotensin 1–9 (Donoghue et al., 2000). The receptor protein ACE2 is reported to be expressed ubiquitously in the majority of tissues, including the heart, kidney, intestine, lungs, and the alveolar epithelial type II cells (Scialo et al., 2020; Zhang et al., 2020). It is also a known receptor for SARS-CoV. The SARS-CoV S protein binds with the ACE2 receptor (Hoffmann et al., 2020; Shang et al., 2020).
Infection with SARS-CoV-2 initiates an immune response, which includes the production of binding antibodies in the blood. Not all binding antibodies can block the entry of the virus into the cell. The subpopulation of the antibodies that can block virus entry into the cells is termed neutralizing antibodies (NAbs).
NAbs testing is limited to laboratories equipped with BSL-3 or 4 facilities with standard detection techniques, that is, Conventional Virus Neutralization Test (VNT) or Pseudovirus based VNT. All other assays such as ELISA and the Lateral Flow Assay detect quantitatively the level of total antibodies in the sample, but fail to differentiate between the levels of binding as well as the NAbs (Tan et al., 2020).
In the present study, we have established ELISA-based test method that detects NAbs without the need for any live virus and can be performed in a Biosafety level 2 facility. By using a commercially available RBD from the spike protein of the SARS-CoV-2 virus and the ACE2 receptor present on the host cell, our test method mimics the biological interaction between the virus-host in an ELISA plate. The interaction between the RBD–ACE2 is known to be inhibited by a type of antibodies known as NAbs, which are present in the sera of previously infected or vaccinated individuals. The ELISA test method was compared with Food and Drug Administration (FDA)-approved commercially available GenScript cPass™ SARS-CoV-2 Neutralization Antibody Detection kit for the detection of Neutralization antibodies (Genscript Biotech, Leiden, The Netherlands).
Materials and Methods
The recombinant human ACE2 was obtained from SignalChem (Cat. No. A51C2-G341F-100), Coronavirus 2019 Spike Glycoprotein-S1 RBD (319–541 a.a), Biotinylated was obtained from ProSpec (Cat. No. SARS-030), Streptavidin conjugated to horseradish peroxidase was obtained from Rockland (S000-03), Anti-2019-novel coronavirus spike NAb was obtained from Elabscience (Cat. No. E-AB-V1024), and 3,3′,5,5′-tetramethylbenzidine (TMB) substrate was obtained from Surmodics (Cat. No. TMBX-1000-01) to develop the neutralizing antibody ELISA kit. The assay diluent contains phosphate buffer saline with pH 6.6–7.2 (Cat. No. SM01-1000). The blocking buffer was obtained from Surmodics (Cat. No. ST01-0050). The wash buffer used for the kit was obtained from Surmodics, which contains Tris-buffered saline solution with 0.5% Tween 20 (Cat. No. WSHW-1000-01).
Ethics approval
The purpose and goal of the study were informed to the study participants, and they consented to participate by signing the consent form before taking part in the study.
Blood collection and serum separation
A total of 100 serum samples were analyzed from 50 vaccinated and/or naturally infected subjects and 50 true negative samples which were taken before December 2019 (sera samples stored at −80°C). In brief, 10 mL of blood was collected from the antecubital vein in unheparinized vacutainer blood collection tubes and stored at 4°C for an hour. The blood in the absence of an anticlotting agent resulted in the formation of a clot at the bottom with a clear layer of serum formed above the clotted blood. The serum was then gently collected using a micropipette in a sterile microcentrifuge tube and centrifuged for 10 min at 1,200 rpm. The serum was then again centrifuged to remove any residual amount of red blood cells if present. The clear serum was aliquoted in tubes and stored at −40°C for further experimentation.
Details of the procedures and methods developed for NAb ELISA of SARS-CoV-2
A 96-well ELISA plate was coated with recombinant hACE2 receptor protein (200 ng/well) and overnight incubated at 4°C. Plate was washed five times with wash buffer and then blocked for 2 h using blocking buffer at room temperature. S1-RBD-Biotin (300 ng/mL) was mixed with the positive control (Anti-2019-novel coronavirus spike NAb), negative control, and serum samples (serum samples were diluted in 1:1 ratio in assay diluent buffer) for 1.5 h at room temperature. After 1.5 h, the plate was washed five times with wash buffer and the mix was added to the wells and incubated for an hour.
After completion of incubation, the plate was again washed five times, and streptavidin-horseradish peroxidase (HRP) conjugate (500 ng/well) was added to the wells and further incubated for 1 h at room temperature. After washing, substrate TMB/H2O2 was added and color was developed, the reaction was stopped by the addition of 50 μL of the stop solution. After which the optical density (OD) was measured spectrophotometrically at 450 nm.
To check the quality of the test results, negative and positive controls were used. The average OD spectrophotometrically observed at 450 nm of the positive controls must be below 0.35 and negative control must be above 1.0.
The results were reported as Signal Inhibition (%) and were calculated using the following formula: Signal Inhibition (%) = (1−[OD of sample]/Mean OD of Negative control) × 100. If the percentage inhibition was >30%, it was considered positive, indicating the presence of S1-RBD NAb. If percentage inhibition was <30%, sample was considered negative, indicating S1-RBD NAb is absent or below the detection limit.
The assay was validated with FDA-approved cPass neutralizing antibody assay kit for sensitivity and specificity.
GenScript surrogate VNT
According to the manufacturer's instruction, the GenScript cPass SARS-CoV-2 Neutralization Antibody Detection Kit (Genscript Biotech, Leiden, The Netherlands) assay was performed. In brief, the positive and negative controls and the serum samples of the tests were diluted to a ratio of 1:9 in the sample dilution buffer. After this, the diluted sample and the control were mixed with HRP-RBD working solution in a 1:1 ratio and incubated for 30 min at 37°C. In a 96-well plate precoated with the ACE2 receptor, 100 μL of the diluted control and the samples were added. The plate was then incubated for 15 min at 37°C and subsequently washed four times with 300 μL of wash buffer. After washing each well, 100 μL of substrate solution was added, after which the plate was incubated for 15 min in the dark at room temperature.
Finally, to stop the reaction after the color is developed, 50 μL of stop solution was added to each well and the OD was measured at 450 nm using ELISA-Reader. Signal inhibition was calculated using the following formula Inhibition (%) = (1–[Sample OD450/Average Negative Control OD450]) × 100.
Statistical analysis
The data obtained for percent inhibition by in-house neutralizing antibody ELISA kit and cPass kit were correlated with Pearson correlation coefficient (R). The data are considered significant at p < 0.05.
Results
Development of the ELISA test method for the rapid detection of neutralizing activity
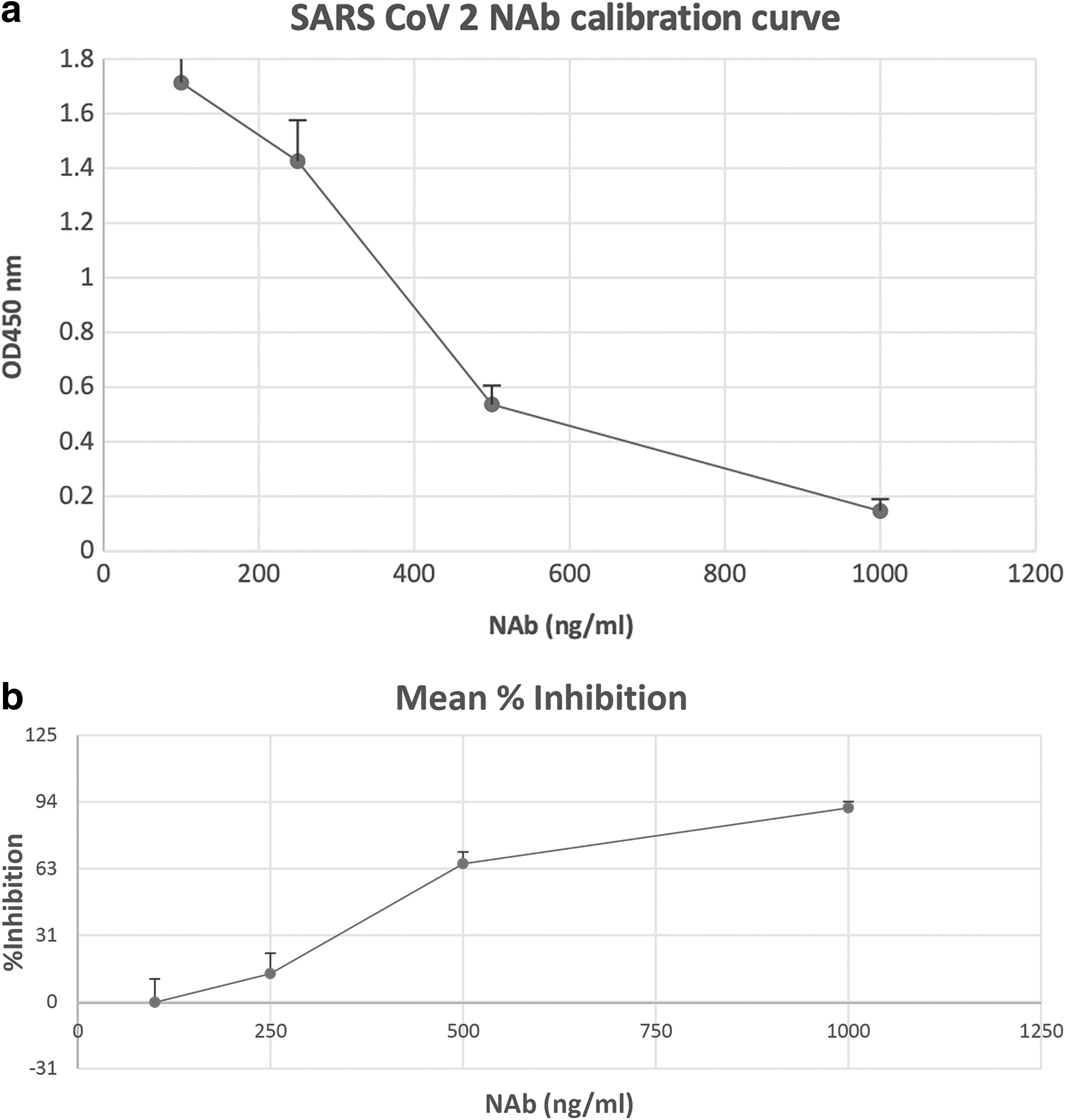
The NAb known to be specific for the S1-RBD was used as a positive control and assay diluent was used as negative control and 100 serum samples were analyzed for validating and optimizing the ELISA kit for detection of NAb against SARS-CoV-2. We have optimized the ELISA for NAb against SARS-CoV-2 and standard plots were made (Fig. 1a, b). The percent inhibition of NAbs in vaccinated and/or naturally infected individuals and true negative serum samples were analyzed and are shown in Tables 1 and 2, respectively. The test results indicate that the optimal S1-RBD protein concentration was 300 ng/mL and that of ACE2 was 0.2 μg/mL.
Test Results of Serum Samples (n = 50) of Vaccinated and/or Naturally Infected Recovered Subjects Based on % Inhibition of In-House-Developed Neutralizing Antibody ELISA Kit
ELISA, Enzyme Linked Immunosorbent Assay; NAbs, neutralizing antibodies.
Test Results of Serum Samples (n = 50) of True Negative Sera Samples Based on % Inhibition of In-House-Developed Neutralizing Antibody ELISA Kit
The results observed with these doses were comparable to those obtained in the cPass kit. The cutoff value kept for negative samples was set at ≤30%. The true negative serum samples analyzed were all below 30%. Further, we analyzed the concentration of NAb using a standard plot, and cutoff 350 ng/mL was considered negative (Fig. 2).
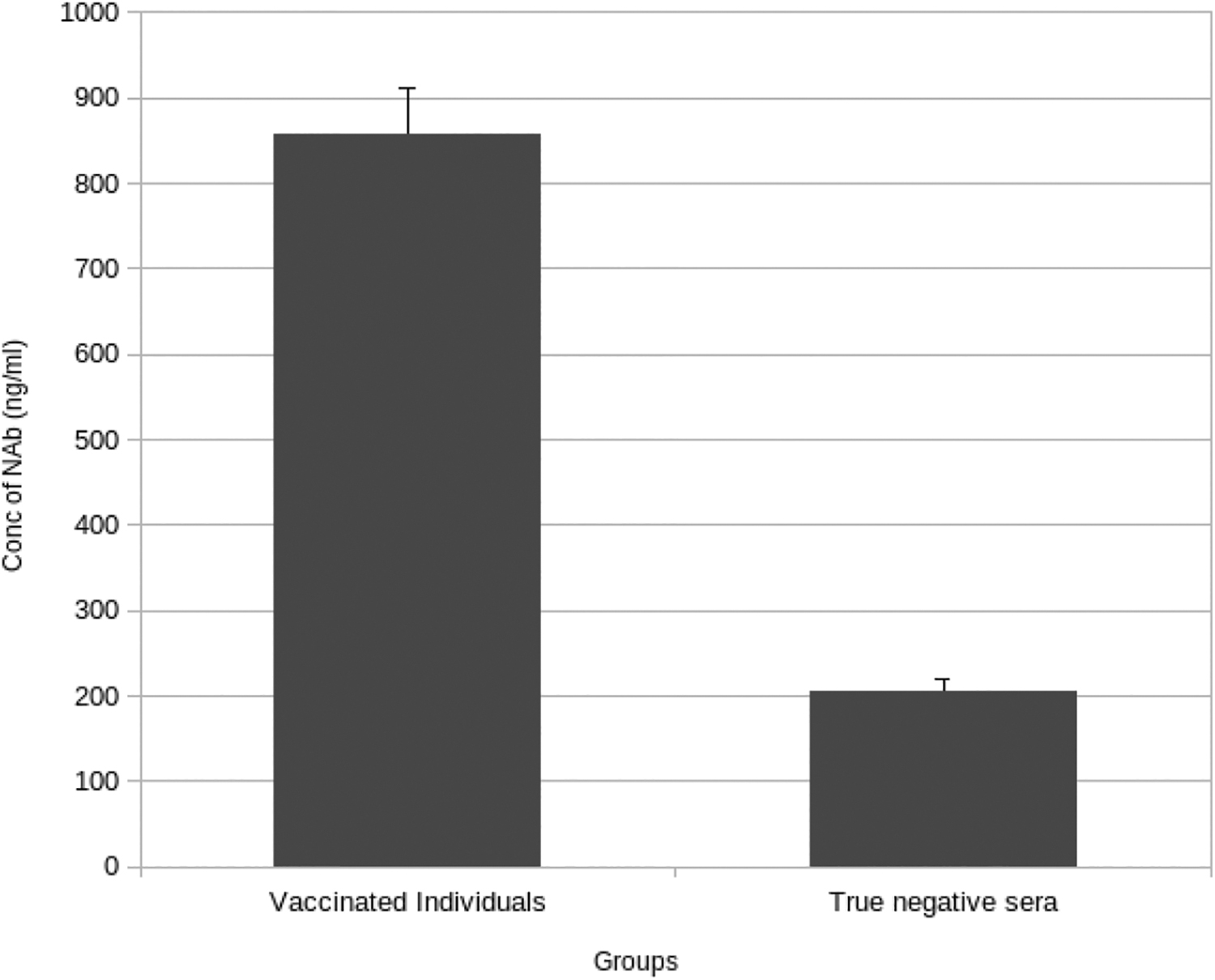
Semiquantitative analysis of mean concentration of NAb of 50 vaccinated and 50 true negative samples was evaluated using the standard plot shown in figure 1a (OD vs. NAb concentration). The NAb concentration analyzed using in house ELISA kit of the vaccinated and/or naturally infected subjects was compared with the true negative sera samples. Cutoff 350 ng/mL considered as negative test result. ELISA, Enzyme Linked Immunosorbent Assay.
Correlation of % inhibition by in-house NAb ELISA with cPass kit
The data obtained for percent inhibition were correlated with cPass data, and the Pearson correlation coefficient (R) was observed as 0.716, which was highly significant (p < 0.001).
Sensitivity and specificity
To determine the sensitivity as well as the specificity of the NAb-ELISA, we thereby tested 50 serum samples collected from COVID-19 vaccinated and or naturally infected recovered subjects using our developed NAb-ELISA, out of 50 samples tested for the presence of NAb, 48 were positive (Table 1). Further, to examine the specificity of the NAb-ELISA, we tested 50 SARS-CoV-2-negative sera (collected before December 2019). The lack of a positive result in SARS-CoV-2 negative sera suggested 100% specificity, (Table 2). Next, 50 serum samples from COVID-19-vaccinated and/or naturally infected and recovered subjects and 10 true negative samples were tested using the NAb-ELISA and cPass kit.
All 50 serum samples from COVID-19-vaccinated and/or naturally infected and recovered subjects were found to be positive in the GenScript cPass test, while 48 sera samples tested positive using the in-house NAb ELISA method. The comparative data of both the kits are graphically represented in Figure 3. All 10 true negative sera samples were negative in both the test methods (Fig. 4). Compared to cPAss kit, the sensitivity of in-house NAb-ELISA was 96% (95% confidence intervals of 86.29–99.51) and specificity was 100% (95% confidence intervals of 69.15–100.00) (Table 3).

Comparison of percent inhibition of in-house ELISA kit with the GenScript cPass™ SARS-CoV-2 Neutralization Antibody Detection kit (grey line is of in-house ELISA result and dark grey line is of cPass kit, n = 50).
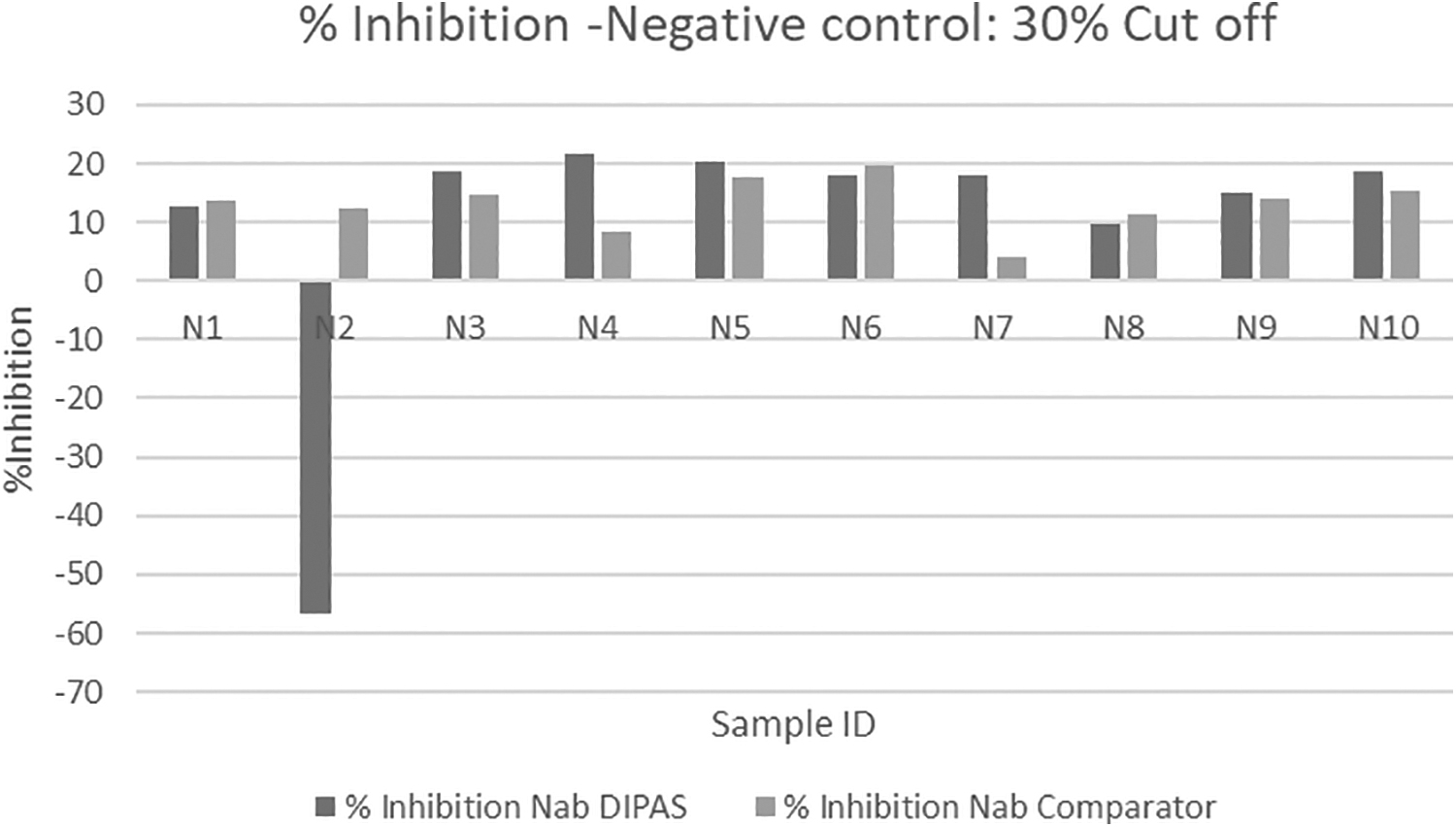
Serum samples of true negative subjects were analyzed and compared with FDA-approved cPass kit for NAb (n = 10). FDA, Food and Drug Administration.
Evaluation of Sensitivity and Specificity of In-House Neutralizing Antibody ELISA Kit with Comparator GenScript's cPass Kit
Sensitivity = (True positive/true positive+false negative) × 100
= (48/48 + 2) × 100 = 96%.
Specificity = (True negative/true negative+false positive) × 100
= (10/10 + 0) × 100 = 100%.
Discussion
The humoral immune response against any viral infection leads to the production of NAbs that can prevent the viruses from infecting cells (Addetia et al., 2020; Huang et al., 2020). For the detection of NAbs against the infectious virus, viral plaque reduction and neutralization test is the gold standard method, which requires a live virus and laboratory setting of biosafety level 3 or 4 for performing the experiment (Okba et al., 2020; Pieri et al., 2022).
In the current study, we have developed a SARS-CoV-2 NAb ELISA to detect NAbs against SARS-CoV-2 using purified proteins. The assay is based on the interaction of the SARS-CoV-2 RBD with the host ACE2 receptor (hACE2) (Lan et al., 2020; Liu et al., 2022; Tai et al., 2020). The use of purified hACE2 protein-coated ELISA plates and biotin-conjugated RBD allows this test kit to assess the presence of NAbs that block the interaction of RBD-Biotin with hACE2 with high correlation to the GenScript's cPass kit (Lan et al., 2020; Tan et al., 2020).
In this study, we have compared the FDA-approved cPass kit for Neutralizing antibodies with an in-house-developed neutralizing antibody ELISA kit. The sensitivity and specificity of the in-house-developed ELISA kit were 96% and 100%, respectively, when compared with FDA-approved cPass kit. NAbs are essentially very important for virus clearance and protection of the host against SARS-CoV-2 (Pang et al., 2021). As mentioned earlier, only NAbs are known to inhibit the entry of virus inside the host cells, therefore, it becomes essential to quantitate the presence of NAbs after vaccination as the level of circulating NAbs is directly correlated to survival as well as virus control in vaccinated or infected patients (Dispensiri et al., 2021). The gold standard method of testing NAbs requires BSL-3/4 facility, which poses a risk to scientific researchers (Li et al., 2022). Therefore, a safe and reliable method needs to be developed for NAbs for the prevention of SARS-CoV-2 infection.
Tan et al. (2020) developed a surrogate SARS-CoV-2 (surrogate VNT) neutralization test that was based upon the antibody-mediated blockade of the ACE2–S protein interaction. It was approved by FDA and can be used as an alternative method for determining NAbs. Herein, we developed an ELISA method to test the presence of NAbs in the serum by making a standard curve of known concentration of NAbs and its reaction with S1-RBD biotin and negative control and sera samples of vaccinated individuals for the rapid detection of NAbs. In our method, the level of NAbs can also be determined semiquantitatively, indicating the level of NAb present in serum.
The in-house-developed neutralizing antibody ELISA kit's performance in terms of percent inhibition was compared with FDA-approved GenScript cPass kit and correlation analysis gave a Pearson coefficient value (R) of 0.716, which was significant (p < 0.001). However, when the concentration of NAb and percent inhibition of in-house-developed NAb ELISA was correlated, the Pearson coefficient R-value was only 0.3, although it was significant (p < 0.04). The gold standard method for detection of neutralizing antibody (Plaque reduction neutralization test) is always superior over any other alternate method for detection of NAbs. A comparative analysis of advantages and disadvantages of the in-house ELISA-based assay, FDA-approved GenScript's cPass assay and pseudotyped virus-based neutralization assays are elucidated in Table 4
Advantages and Disadvantages of Neutralization Assays
FDA, Food and Drug Administration.
In summary, our study reveals that the NAb ELISA detection assay is able to detect NAbs in human serum samples. Also, it is at par with FDA-approved GenScript cPass kit. The ELISA-based NAb testing kit developed in our laboratory can also semiquantitively measure the level of NAb in the serum. The ELISA-based NAb estimation will help in estimating the prevalence of NAbs and humoral immunity. Although the in-house-developed ELISA kit can be used for mass screening of individuals for the presence of NAbs, however, this method has some limitations, a sample containing a lower level of NAbs (<350 ng/mL) will be considered as negative, as the cutoff value for the test is 30%. Further, this method cannot assess the assay performance against variants of concern because we lack sequence data and strain typing on the subjects from which the sera were collected.
At the late stage of the pandemic, we know that the immunity induced by vaccination against SARS-CoV-2 results in improved outcomes following infection, which include reduced symptoms and severity of disease and reduced hospitalization rates (McLean et al., 2022). The analysis of NAb levels against SARS-CoV-2 using this ELISA method may be useful in determining the immune protection status at the population level.
Footnotes
Acknowledgment
The authors thank Ms. Asha D. Kushwaha, Ms. Jyotsana Bakshi, and Ms. Smriti Sudha for their support.
Authors' Contributions
Conceptualization, K.P.M., M.S., and D.S.; methodology: K.P.M., M.S., and D.S.; resources and materials: K.P.M., M.S., D.S., and S.N.S. Data analysis: K.P.M.; article writing: K.P.M.; editing: K.P.M., M.S., D.S., and S.N.S. All authors have read and agreed to the published version of the article.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by Defence Institute of Physiology and Allied Sciences, Delhi.