
Abstract
Severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) infection is associated with proinflammatory cytokine release as mediators of host antiviral response to the infection. Cytokine persistent elevation leads to post-Coronavirus disease-2019 (COVID-19) post-COVID-19 sequela (PCS) reported in about 60% of patients affecting individual's normal life after recovery. This study evaluates relationship of cytokines and chemokines pattern during and postinfection to PCS events. Serum samples collected from 82 individuals with symptomatic, asymptomatic, or no SARS-CoV-2 infection were classified as recently or formerly infected groups according to levels of anti-2019nCoV Immunoglobulin G/Immunoglobulin M. Levels of interleukin (IL)-1α, IL-1β, IL-6, IL-8, interferon alpha (IFN-α), tumor necrosis factor alpha (TNF-α), granulocyte macrophage colony-stimulating factor (GM-CSF), and monocyte chemoattractant protein-1 were assessed via ELISA for each individual. All asymptomatic groups showed nonsignificant differences in cytokines' levels than control group. Significant elevation of IFN-α, TNF-α, and GM-CSF levels were observed in recent symptomatic, while IFN-α and TNF-α levels were significant in former symptomatic groups. We observed an association between fever with IL-1α and IFN-α levels, fatigue with TNF-α and GM-CSF, dyspnea with IFN-α, TNF-α, and GM-CSF, and chest-wheezing with GM-CSF. Individuals were surveyed 12 months postsampling for PCS events. Among 35 responders to survey, 8 (22.8%) reported PCS events, 6 of which were females. Upon studying PCS events, IL-8, IFN-α, TNF-α, and GM-CSF levels showed significant elevation in active infection, that was not seen in a resolved state of infection. Cytokines patterns suggest that either a persistent elevation in levels or damage caused during infection contributes to PCS. Although with the limited sample size, our study emphasizes the importance to conduct medical approaches targeting the associated cytokines to improve the PCS symptoms.
Introduction
The severe acute respiratory syndrome-Coronavirus-2 (SARS-CoV-2) global pandemic caused a significant threat to humans, exceeding 750 million cases and >6.8 million deaths (WHO, 2023). Coronavirus disease-2019 (COVID-19) showed a wide range of disease outcomes from a critical-severe illness that obliges medical and/or intensive care admission, a moderate symptomatic illness or a completely asymptomatic status (NIH, 2021). The immune response to SARS-CoV-2 infection leads to the activation of macrophages, natural killers, and other immune cells that express and release specific cytokines and chemokines (Keam et al., 2020). The dysregulation and hyperactivation of the correlated cytokines might trigger a cytokine storm event leading to critical stages of organ destruction and deaths (Chi et al., 2020).
Mild symptomatic and asymptomatic COVID-19 showed a different pattern of cytokine activation that correlates to the disease-associated symptoms that might be respiratory, neurological (Spudich and Nath, 2022), or gastrointestinal (Han et al., 2020). Interleukins (ILs), chemokines, and colony-stimulating factors are among the reported proinflammatory cytokines and chemokines triggered by the onset of viral infection (Chi et al., 2020). The cytokine pattern difference between symptomatic and asymptomatic infections also differs in the persistence and prolonged effect postrecovery. Tumor necrosis factor alpha (TNF-α), IL-6, IL-1β, and IL-10 were reported in symptomatic infection to be elevated postrecovery from SARS-CoV-2 that tend to increase with disease severity (Lee et al., 2020). Levels of same cytokines were reported higher in asymptomatic individual than in a recovered symptomatic patient and yet not causing any symptoms (Le Bert et al., 2021).
Nearly 60% of the patients, independent of the initial illness severity, might suffer from symptoms persistence for up to 12 months (Blomberg et al., 2021), a syndrome known as post-COVID sequela (PCS). PCS is associated with systemic inflammation that causes fatigue, joint pain, chest pain, palpitations, shortness of breath, cognitive impairment, and worsened quality of life (Logue et al., 2021), and correlates with sustained immune dysregulation that drives chronic inflammation in recovered patients (Bergamaschi et al., 2021). Studying patterns of cytokines' levels in asymptomatic groups might lead to better understanding of symptom-related, and their PCS prolonged, consequences in symptomatic infections.
In this sudy, we evaluate selected proinflammatory cytokines and chemokines in individuals with mild or no symptoms due to recent or former SARS-CoV-2 infections. Also, we distinguish the related cytokines' patterns in individuals encountered with PCS within a 12-month postinfection aiming to find a proposed relationship with PCS.
Materials and Methods
Sample collection
Egyptian individuals were randomly recruited to two small-scale active surveillances conducted independently starting July 20 till August 29, 2020. All individuals (n = 135) were subjected to blood sampling and a questionnaire recording symptoms encountered since the onset of pandemic recorded in Egypt, in April
Serum anti-SARS-CoV-2 immunoglobulin detection
Serum anti-SARS-CoV-2 immunoglobulin G (IgG) and immunoglobulin M (IgM) levels were measured via SARS-CoV-2 nucleoprotein antigen-specific ELISA assay using precoated human anti-2019nCoV(N)IgG and anti-2019nCoV(N)IgM plates (FineTest; Wuhan Fine Biotech Co., LTD, China).
Quantification of serum cytokines levels
IL-1α, IL-1β, IL-6, IL-8, interferon alpha (IFN)-α, TNF-α, granulocyte macrophage colony-stimulating factor (GM-CSF), and monocyte chemoattractant protein-1 (MCP-1) levels were assessed using relevant precoated ELISA plates (SunLong Biotech Co., LTD, China) according to the manufacturer's guidelines. Absorbance measured at 450 nm and a reference at 620 nm filters, concentrations were calculated in either picograms (pg) or nanograms (ng)/mL using standards provided in the kits. Individuals suffering from hepatitis B or C viruses, or following an immunotherapy were excluded if their cytokines' levels outlie the interquartile range of grouped data.
Statistical analysis
Analysis started by evaluating the groups' distributions normality using the Shapiro–Wilk test then the Bartlett test to evaluate variance homogeneity. Accordingly, normally distributed/homogenate-variance data were analyzed using the following parametric tests: One-way ANOVA for ≥3 groups mean comparison; upon significance, it was followed by Tukey's post hoc test, and independent t-test for two groups comparison. Alternative nonparametric tests were Kruskal–Wallis test for ≥3 groups comparison; upon significance, it was followed by Dunn's post hoc test, and Mann–Whitney U-test for two groups comparison. Fisher's Exact test was used to assess the association between females PCS. Relationships between cytokine levels in individuals with PCS were assessed through Spearman's rank correlation coefficient and coefficient of determination (R 2). A p-value <0.05 was considered significant.
Data were analyzed and visualized on a Jupyter Notebook using Python Version 3.8.3 and the following libraries: for data manipulation, Pandas 1.0.5 (McKinney, 2010) and NumPy 1.22.2 (Harris et al., 2020); for statistical analysis, SciPy v. 1.5.0 (Virtanen et al., 2020) and Scikit_posthocs v. 0.7.0 (Terpilowski, 2019); and for visualization, Matplotlib v. 3.2.2 (Hunter, 2007) and Seaborn v. 0.11.0 (Waskom, 2021).
Results
Sample selection and categorization using anti-SARS-CoV-2 IgG and IgM levels
To select individuals who encountered SARS-CoV-2 infection, serum anti-2019nCoV IgG level was assessed. Individuals tested anti-IgG-positive were included in the study (n = 82), further categorized into groups defined according to reported symptoms and anti-2019nCoV IgG/IgM levels as following: recent symptomatic (RS; n = 26); anti-IgG+/anti-IgM+/symptoms+, recent asymptomatic (RA; n = 16); anti-IgG+/anti-IgM+/symptoms−, former symptomatic (FS; n = 31); anti-IgG+/anti-IgM−/symptoms+, former asymptomatic (FA; n = 5); and anti-IgG+/anti-IgM−/symptoms−. Negative control individuals (Neg.; n = 4) were defined as anti-IgG−/anti-IgM−/symptoms− with no exposure to infected individuals until the day of sample collection (Table 1 summarizes individuals' data).
Sample Definition and Frequency of Symptoms Among Symptomatic Individuals
Anti-IgG/IgM levels of each group were compared statistically to explore the reliability of the preselection/categorization criteria. Individuals grouped as recent and former infection status showed significant anti-2019nCoV IgG levels difference (Fig. 1A) in both symptomatic (p < 0.001) and asymptomatic (p = 0.026) groups. While individuals categorized in the same infection status group showed no significant difference in anti-2019nCoVIgM (p = 0.115; Fig. 1B) and IgG levels comparing RS/RA and FS/FA groups (p = 0.408, and 0.276; Fig. 1C, D, respectively). The homogeneity between individuals of the same group increased the confidence in using anti-IgM levels in infection status differentiation.

Distribution of anti-SARS-CoV-2 IgG and IgM levels in different groups: Distribution and statistical significance of specific anti-IgG and IgM levels used in group definition.
Comparing cytokines levels in RS versus asymptomatic infections
Cytokines levels of RS versus RA groups were compared to evaluate the differences of a recent (active/incompletely resolved) infection in relationship to a symptomatic outcome. First, each group was compared to the control group, all cytokine levels in RA (p > 0.05; “B” in Table 2), and levels of IL-1β, IL-6, IL-8, and MCP-1 (p > 0.05, “A” in Table 2) in RS showed nonsignificant difference to control group, therefore, the latter cytokines showed no difference to the control in both groups in our sampling.
Pairwise Post Hoc Test Comparison Resulted p-Values
Statistical significance of the changes between recent and former group to negative control and recent versus FS groups.
Statistically significant difference; bold values; statistically nonsignificant difference; cytokines initiated with “a” denotes pairwise post hoc Dunn's test while other cytokines were evaluated by pairwise post hoc Tukey's test; NA is not applicable for calculation.
GM-CSF, granulocyte macrophage colony-stimulating factor; FS, former symptomatic group; IFN-α, interferon alpha; IL, interleukin; MCP-1, Monocyte chemoattractant protein-1; RS, recent symptomatic group; TNF-α, tumor necrosis factor alpha.
Then by comparing RS/RA groups, all except IL-1α levels significantly differ (p = 0.067; Fig. 2A), as the levels of IL-1β, IL-6, IL-8, and MCP-1 (p < 0.0001, p = 0.047, 0.043, and 0.0276; Fig. 2B–D, H, respectively) were of no difference to the control, then only IFN-α, TNF-α, and GM-CSF levels showed significant elevation in RS over RA (all p < 0.0001; Fig. 1E–G, respectively) and control group (“A” in Table 2).
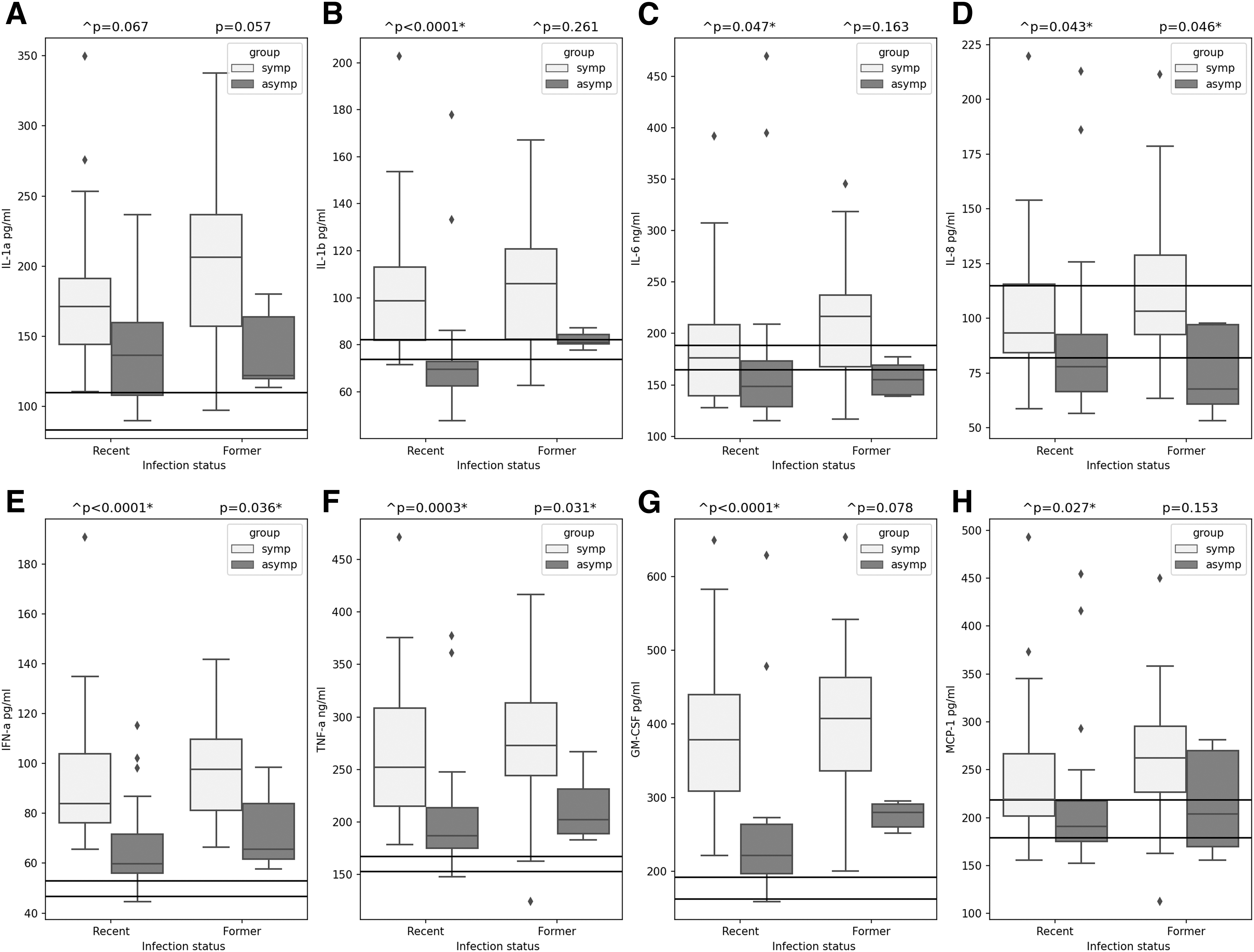
Distribution of cytokine levels in recent and former infection status comparing symptomatic and asymptomatic individuals: Cytokine levels represented as concentration (pico- or nanogram) per milliter on Y-axis, infection group on x-axis, horizontal upper line represents the max of the relative cytokine quantification in the negative control group while horizontal lower line represents its median. Recent symptomatic group n = 26, recent asymptomatic n = 16, former symptomatic n = 31, and former asymptomatic group n = 5. (Significance value initiated with “^” denotes a Kruskal–Wallis test while other cytokines were evaluated by one-way ANOVA test).
Comparing cytokines levels in FS versus asymptomatic infections
Cytokine levels of FS versus FA groups were compared to evaluate the differences of a former (resolved) infection in relationship to a symptomatic outcome during infection. All cytokine levels in FA group (p > 0.05, “D” in Table 2) and levels of both IL-6 and IL-8 in FS showed nonsignificant difference from control group (“C” in Table 2).
Comparing FS/FA groups, levels of IL-1α, IL-1β, IL-6, GM-CSF, and MCP-1 showed nonsignificant difference between groups (p = 0.057, 0.261, 0.163, 0.078, and 0.153; Fig. 2A–C, G, H, respectively). In FS groupIL-8, IFN-α and TNF-α levels were significantly different (p = 0.046, 0.036, and 0.031; Fig. 2D–F, respectively), but as IL-8 level were of no difference to control group, then only IFN-α and TNF-α levels were considered significantly elevated in FS over FA groups.
Elevated cytokine levels' association with reported symptoms in RA infection group
Levels of IFN-α, TNF-α, and GM-CSF cytokines that showed significant elevation in RS group were assessed for possible association with reported symptoms (Table 3). Significant association of fever with IFN-α level (p = 0.047), fatigue with TNF-α and GM-CSF levels (p = 0.042 and 0.006, respectively), and dyspnea with IFN-α, TNF-α, and GM-CSF levels (p = 0.046, 0.016, and 0.001, respectively) while wheezing was associated only with GM-CSF levels (p = 0.027).
Comparison of Cytokines Level in Relationship to Coronavirus Disease-2019 Symptoms Reported in Recent Symptomatic Infection Group (n = 26)
The table includes p-values of the statistically significant difference of cytokine levels in presence and absence of the symptom evaluated using Mann–Whitney U-test.
ns, nonsignificant.
Comparing significantly elevated cytokines' levels of symptomatic individuals in recent versus former infections
The symptoms associated with elevated IFN-α, TNF-α, and GM-CSF levels in RS were among those reported in individuals suffering from PCS. The elevation of IFN-α and TNF-α levels in FS group raised the question of whether it was comparably elevated in recent versus former infection. Comparing RS/FS groups of IFN-α, TNF-α or GM-CSF levels showed nonsignificant difference (p = 0.08, 0.152, and 0.341, respectively, “E” in Table 2). This comparable elevation was further questioned in relationship to PCS development.
Comparing cytokines levels of individuals with versus without PCS
To explore the cytokine level patterns in individuals experienced PCS events, we studied the groups in accordance to PCS outcome. Individuals participated in PCS questionnaire were 35 out of the 78 of recently or formerly infected individuals. Only 8/35 (22.8%) reported PCS with symptoms summarized in Table 4. Females were 6/8 cases, but neither females nor males were significantly associated with PCS (p = 0.291 and 0.378, respectively). Reported PCS symptoms were fatigue of unexplained discomfort and lessened activity, brain fog, concentration issues, and shortness of breath.
Frequency of Post-COVID-19 Sequela Events in Surveyed Individuals 12-Months Postsampling and the Reported Symptoms
F, female; M, male; PCS, post-COVID sequela.
Figure 3 shows the comparison of RS/FS cytokine levels in relationship to PCS. In RS group, IL-8, IFN-α, TNF-α, and GM-CSF levels showed significant elevation in individuals encountered with PCS (p = 0.032, 0.036, 0.028, and 0.028; Fig. 3D–G, respectively). It is now obvious that RS IL-8 levels nonsignificance difference to control (p = 0.821, “A” in Table 2) was attributed to individuals with no PCS (Fig. 3D). IFN-α and TNF-α levels showed significant correlation (r 2 > 0.78; p < 0.05; Fig. 4) in RS PCS.

Distribution of cytokine levels in symptomatic individuals encountered with versus no PCS: Cytokine levels represented as concentration (pico- or nanogram) per milliter on Y-axis, infection group on x-axis, horizontal upper line represents the max of the relative cytokine quantification in the negative control group while horizontal lower line represents its median. Recent infection status with PCS group n = 3, no PCS group n = 8; former infection status with PCS group n = 5; no PCS group n = 7. (Statistical significance was evaluated using Mann–Whitney U-test).
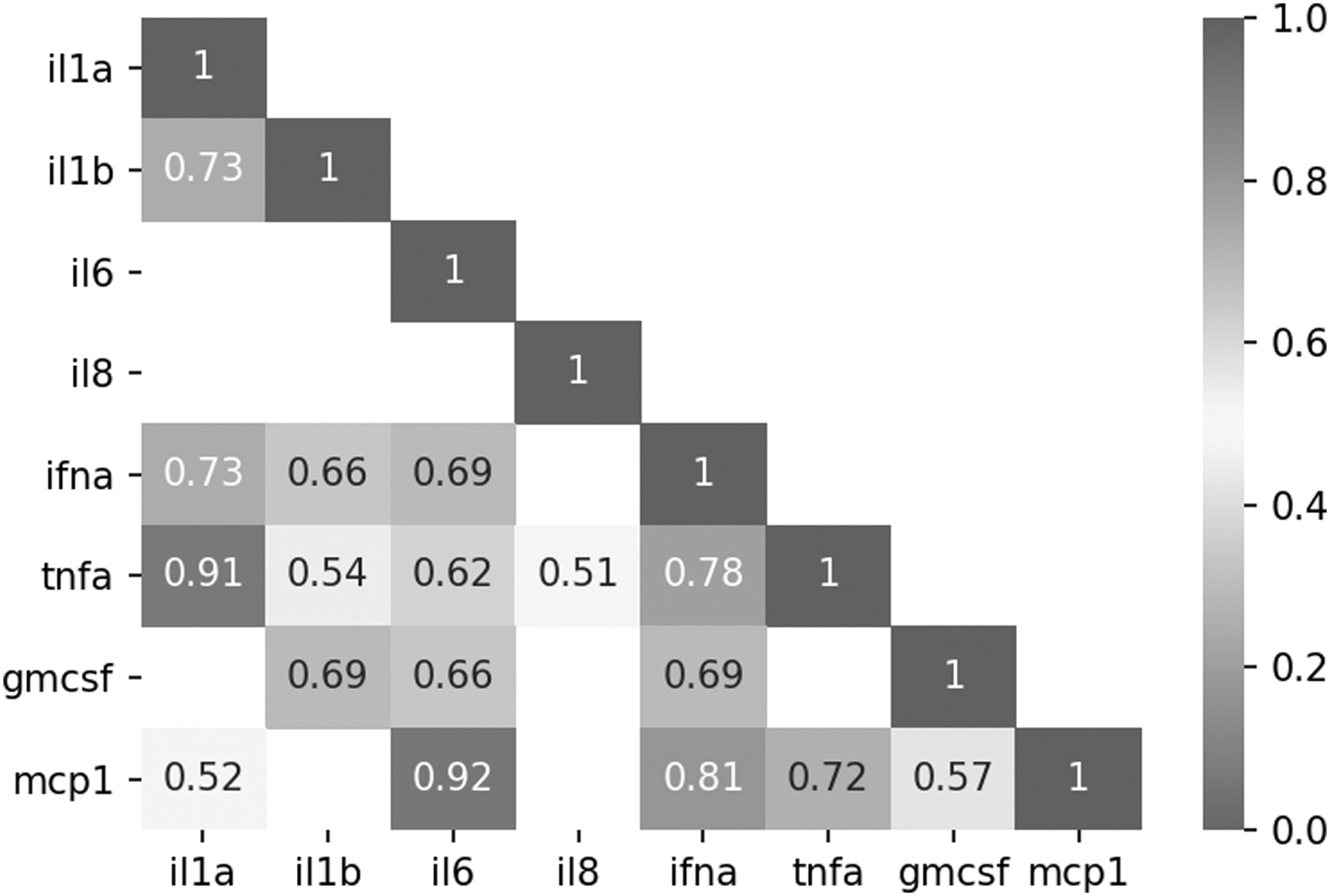
Spearman's correlation matrix calculated for cytokine levels in individuals encountered PCS. Correlation matrix represented as rank coefficient of determination R 2 of significant p-values <0.05.
In FS group, all cytokines showed nonsignificant difference (p > 0.05; Fig. 3) in accordance to PCS; however, the low number of samples might not represent the real distribution correctly. Figure 3 shows that cytokine levels decrease in former versus recent infection and that PCS might not relate to persistent elevation but to the consequences of highly elevated levels during infection (RS).
Discussion
Cytokines and chemokines play a vital role in SARS-CoV-2 infection clearance and prolonged immunity against reinfection (Rabaan et al., 2021). On the contrary, this protective immune response can also trigger pathological localized and systemic inflammatory events (Le Bert et al., 2021).
In our study, we focused on mild symptomatic and asymptomatic infections, through random recruitment to include asymptomatic individuals. Defining the infection onset or recovery through viral detection did not fit the asymptomatic infection as it cannot be estimated by patients test negative by reverse transcription-polymerase chain reactions. This was overcome by taking advantage of anti-IgM levels reported to be detected up to 1.5 months postonset of SARS-CoV-2 infection (Zhou et al., 2021).
Infection status was defined as possible recent or former infection status upon sampling using virus-specific anti-IgM levels. Anti-IgM levels indicated an onset of around 1.5 months of a recent unrecovered infection upon sampling, while its absence indicates a >1.5 months onset of former or recovered infection. A significant elevation in anti-IgG levels was observed in defined recent over former infection groups, which aligns with the tendency in anti-IgG levels to decrease postrecovery, regardless of symptoms (Khaitan et al., 2022; Long et al., 2020). This significant difference and decline in former infection group increased the confidence in the IgM-based group definition for further analysis.
Serum levels of eight inflammatory and proinflammatory cytokines and chemokines; IL-1α, IL-1β, IL-6, IL-8, IFN-α, TNF-α, GM-CSF, and MCP-1 were assessed. Asymptomatic groups showed no difference than controls, which aligns with previous observations where asymptomatic infection was believed to mount an immune response that successfully clear infection under elevated, yet, proportionately coordinated proinflammatory and anti-inflammatory cytokines (Chan et al., 2021; Le Bert et al., 2021).
In recent infection status, IFN-α, TNF-α, and GM-CSF levels showed a significant elevation in symptomatic over asymptomatic groups. The observed elevation of IFN-α and TNF-α levels was previously reported with a comparable unelevated GM-CSF levels (Soares-Schanoski et al., 2022; Tripathy et al., 2021), with a possible relationship between dysregulated IFN-α and disease severity (Hadjadj et al., 2020). In contrast to our findings, multiple studies showed IFN-I levels elevation in asymptomatic (Bencze et al., 2022; Masood et al., 2021) over symptomatic infections.
Studying former infection groups, the cytokine levels were expected to show a decline to near-normal levels, however, both IFN-α and TNF-α levels showed a significant elevation in FS over FA group. This raised a question whether this elevation is an attribute to symptomatic groups that was declined in former than recent infections. RS and FS groups showed nonsignificant difference between IFN-α, TNF-α, and GM-CSF levels postulating a possible persistence in elevation. As observations were not longitudinal with no direct relationship between individuals in the two groups, we cannot conclude a persistence in elevation of cytokine level. However, the comparable elevation might reflect a possible prolonged effect of IFN-α and TNF-α levels in case of symptomatic infection beyond recovery.
Elevated cytokines in RS and FS groups showed significant association to reported symptoms, fever was associated with IFN-α, which aligns with its reported pyrogenic effect of IFN-α in diseases other than COVID-19 infection (Haşlak et al., 2023; Netea et al., 2000). Fatigue association with elevated TNF-α levels aligns with multiple reports in COVID-19 and PCS cases (Ceban et al., 2022), besides a strong correlation to cases of chronic fatigue syndrome (Yang et al., 2019). GM-CSF was associated with fatigue with no prior reports, but it is known as a key inflammatory factor in COVID-19 (Thwaites et al., 2021).
Dyspnea and chest wheezing were associated with GM-CSF aligning with its effect on increasing the activated neutrophils' prolonged recruitment leading to substantial lung tissue injury (Kudlak et al., 2013). Dyspnea was associated with IFN-α levels that was reported to interfere with lung epithelial tissue recovery (Major et al., 2020). Dyspnea association with TNF-α levels was not previously reported as observed in the present study.
The reported symptoms associated with cytokine elevation are among those reported in PCS, including fatigue, dyspnea, anosmia, chest pain, myalgia, sleep, and cognitive disorders (Assaf et al., 2020; Dicpinigaitis and Canning, 2020; Havervall et al., 2021; NIH, 2021). The significant elevation of IFN-α and TNF-α in RS groups that is not decreased in FS group showing association to symptoms common in PCS events in our data led to questions. The levels in FS group of those with no PCS are hypothesized to decline with symptoms relief; thereby should have affected the FS distribution compared to RS group. Then, if there is a possible persistent elevation why not all individuals suffer from PCS. This suggested that either RS or FS groups, if dissected according to PCS development, could include hidden subgroups with different behavior.
Individuals reported that experiencing PCS symptoms along a 12 months' range postsampling were 22.8% (8 individuals) of all responders and 34.7% of symptomatic individuals. This prevalence is less than that previously reported in Egypt of about 80% encountering PCS (Abdelhafiz et al., 2022). However, a prevalence of 27.8 up to 73% of individuals encountered with PCS up to 9 months of observation were reported (Malkova et al., 2021). PCS-related symptoms reported were fatigue, brain fog, and shortness of breath, all align with previous reports in Egypt (Aiash et al., 2021).
Females were 6/8 of reported PCS events, but was not statistically associated in our study, some reports associate PCS with females (Bai et al., 2022), while others reported that there was no difference between males and females (Moreno-Pérez et al., 2021). Despite that disease severity increases in males, the stronger immune response in females might increase the disease consequences of mild infections (Mohamed et al., 2021).
Cytokine levels in RS and FS groups according to PCS showed an interesting pattern. RS group showed an elevation in IL-8, IFN-α, TNF-α, and GM-CSF levels in individuals going to encounter PCS dividing the distribution of symptomatic individuals completely (Fig. 3), which was not persistent in FS group with a tendency to be lower in PCS group. This obvious elevation during infection might cause more tissue damage in PCS groups that was suggested by a study showing that the damage caused by abundance and elevation of immune cells during infection resulting in cell exhaustion and thereby slow the tissue damage repair with prolonged consequences (Williams et al., 2022). Therefore, the cytokine deficiencies due to exhaustion slow down repair, hence prolonged consequences and not persistence of elevated cytokines.
Studies also reported elevated cytokines related to PCS events. Persistently elevated IFN-α levels was reported in PCS contributing in cognitive decline and pain-related manifestations (Tan et al., 2022). In a study on hamsters, SARS-CoV-2 induced central nervous system-wide type-I IFN responses and brain region-specific transcriptional alterations that persisted beyond one month following acute infection (Frere et al., 2022) contributing in increased risk of neurological and neuropsychiatric disorders (Huang et al., 2021; Taquet et al., 2021).
Persistently elevated TNF-α was reported in PCS cases (Schultheiß et al., 2022), while contributing in fatigue, myalgia, and joint pain triggered by its IL-6 induction (Cronstein, 2007). TNF-α contributes to hippocampus local inflammation resulting in cognitive-behavioral changes (Bortolato et al., 2015), memory consolidation, and a state called “sickness behavior” (Gemma et al., 2005). TNF-α is linked to inflammatory bowel syndrome (IBS), as one of its major causes, while anti-TNF-α is a common IBS treatment nowadays (Perše and Unkovič, 2020). GM-CSF was not reported, to our knowledge, with PCS events. However, besides its role in dyspnea, it triggers neurotoxic molecules production related to active multiple sclerosis lesions in the brain (Lee et al., 2020).
However, our study was challenged by limitations, among which the low sample size due to the limited access to well-characterized samples was further delimited by the randomness in sampling to target asymptomatic individuals. Also, follow-up for PCS status caused a further decrease in the number of samples studied with a dependence on self-reporting that might bias the results.
Conclusion
Herein reported a significant elevation in IFN-α, TNF-α, and GM-CSF levels in mild symptomatic over asymptomatic infections, that are associated with symptoms reported in PCS events. Upon studying PCS events, IL-8, IFN-α, TNF-α, and GM-CSF levels showed significant elevation in active infection that was not elevated in a resolved state of infection. Cytokine patterns suggests that either a persistent elevation in levels or due to the damage caused during infection contributes in PCS. Our study emphasizes the importance of conducting research targeting the reported cytokines for the treatment and improvement of PCS, especially in risk groups of recurrent overlapping infections.
Ethics Approval
The study was approved by the Medical Research Ethics Committee at the National Research Centre (Approval reference No. 20166). The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Footnotes
Authors' Contributions
M.M.B. wrote the grant that funded the work, designed the study, discussed the experimental design and the results of the work with all coauthors and put the structure of the article. M.H.N., R.N., and D.N.A.E. supervised filling the questionnaires and interviewed July-surveillance individuals. K.A., W.A.H, F.M.E., and S.R. provided the sera from August-surveillance for SARS-CoV-2 patients. M.H.N., R.N., and D.N.A.E. performed the ELISA assays for IgM/IgG. R.N. performed the ELISA for cytokines detections, did the statistical analysis using a Jupyter notebook with a Python 3.8.3 work environment. R.N. wrote the draft of the article that was discussed and edited by M.M.B. All authors have read, discussed the final version of the article, and agreed to the submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Research Center, Egypt under Mandatory Grant: MP120803.