
Abstract
The percentage of head and neck cancer (HNC) positive for human papillomavirus (HPV) is unknown in most parts of India. How toll-like receptors (TLRs) affect the adaptive immune response in HNC is also mainly unknown. We here assessed the expressions of HPV DNA, p16, inflammation, and TLRs in oral squamous cell carcinoma (OC) and oropharyngeal squamous cell carcinoma (OPC). Patients with OC (n = 31) and OPC (n = 41), diagnosed during 2017–2018 at the Malabar Cancer Centre (tertiary cancer center), Kerala, India, were included in the study. Immunohistochemistry was performed on tumor specimens against p16, TLR3, TLR7, TLR8, TLR9, CD4, and CD8. Quantitate polymerase chain reaction for 14 high-risk HPVs (HPV16/18/31/33/35/39/45/51/52/56/58/59/66/68) was performed. Seven out of 31 OC (22.6%) were p16+ but only 3.2% (1/31) of OC were positive for HPV DNA. While 24.4% (10/41) of OPC were p16+, HPV DNA was found in only one P16+ OPC and in no P16− OPC. TLR3, TLR7, TLR8, and TLR9 were expressed both in OC and in OPC. The expression of TLR7 was significantly higher in OPC compared with OC. TLR8 expression was correlated with and TLR7 tended to be correlated with the inflammatory score in OPC (r = 0.56, p < 0.05 and r = 0.52, p = 0.08, respectively). In conclusion, the role of HPV in OC and OPC is minor, and p16 constitutes a poor biomarker for HPV positivity in Kerala, India. Intracellular TLRs are correlated with the degree of inflammation in OPC but not in OC and may potentially constitute a medical target in the therapy of HNC in the future.
Introduction
Oral squamous cell carcinoma (OC) constitutes the predominant part of all head and neck cancer (HNC). OC is frequently preceded by precursor lesions designated oral potentially malignant disorders (OPMDs) (Ganesh et al., 2018). Common OPMDs, with a prevalence of ∼1%, are leukoplakia and oral lichen planus (Ganesh et al., 2018). In India, oral submucous fibrosis (OSMF) is also an OPMD frequently registered (Murthy et al., 2022). Consumption of alcohol and tobacco are important risk factors for the development of OPMDs and OC (Muwonge et al., 2008; Singh et al., 2021; Singh et al., 2018). In India and in other countries in Asia, chewing of the betel quid is common and associated with a significant increased risk of OSMF and OC (Guha et al., 2014; Murthy et al., 2022; Singh et al., 2018).
Human papillomavirus (HPV) infections are associated with the development of oropharyngeal squamous cell carcinoma (OPC). In western countries, the number of HPV-associated OPC has increased dramatically (Nasman et al., 2020). For example, more than two-thirds of all OPC in Sweden are, today, associated with HPV (Nasman et al., 2020). However, the prevalence of HPV positivity in OPC seems to vary globally depending on populations. We recently showed that the prevalence of p16-positivity in OPC was only 8% in patients recovered at the Malabar Cancer Centre, Thalassery, Kerala, in southern India (Pandiar et al., 2021). In contrast to OPC, the association between OPMD/OC and HPV infections is less clear (Simoens et al., 2021; Sundberg et al., 2019).
Toll-like receptors (TLRs) constitute important members of the innate immune system and respond to damage-associated molecular patterns and pathogen-associated molecular patterns. TLRs are not only expressed in epithelia and immune cells but also on tumor cells. TLRs may regulate different functions of tumor cells, including proliferation, invasion, and regulation of the immune response (Huang et al., 2008). There are 10 described TLRs in man. TLRs are either expressed on the plasma membrane or intracellularly in the membrane of endosomes. TLR3, TLR7, TLR8, and TLR9 are expressed in endosomes and are activated by double-stranded RNA, single-stranded-RNA (ssRNA), uridine-rich or uridine/guanosine-rich ssRNA, and unmethylated CpG DNA, respectively (Mielcarska et al., 2020).
Studies suggest that HPV infection may reduce the innate immune response in cervical cancer by upregulating TLR4 and downregulating TLR2/TLR7 (Guleria et al., 2019). TLR5 and TLR7 are also expressed differently in HPV-positive and HPV-negative tongue base cancer (Haeggblom et al., 2019). High expression of TLR5 and low expression of TLR7 were associated with poor survival in HPV-positive OPC (Jouhi et al., 2017). In squamous cell carcinoma of the tongue high expression of TLR5 was associated with increased recurrence rate (Kauppila et al., 2013). Furthermore, TLR9 is less expressed in Epstein–Barr virus (EBV)-positive OPC compared with EBV-negative OPC (Stepien et al., 2021).
Immunotherapy in the form of immune checkpoint inhibitors targeting programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1) has led to a paradigm shift in the treatment of many cancer forms. Immunotherapy plays a role in the treatment against HNC; however, only one out of five patients who progressed on platinum-containing therapy was helped by PD-1/PD-L1 targeted therapy (Muro et al., 2016). Stimulation of TLR7 and TLR9 on plasmacytoid CD303+ dendritic cells gives rise to a type 1 interferon response, and drugs targeting TLR7 and TLR9 have been explored in cancer therapy (Chiang and Kandalaft, 2018). Local injection of CpG targeting TLR9 after surgery of early-stage melanoma may improve recurrence-free survival (Koster et al., 2017).
Intratumoral administration of the TLR7/TLR8 agonist 3M-052 increased the number of tumor-infiltrating lymphocytes (TILs), reduced the tumor size, and decreased the number of lung metastases in an animal model of triple-negative breast cancer (Zanker et al., 2020). The TLR8 agonist motolimod has been tested in combination with chemotherapy in metastatic OC (Ferris et al., 2018). The study was negative for survival but in subgroup analysis, motolimod appeared to have effects in HPV-positive OPC. In animal models of OC, targeting TLR9 may lead to increased survival and potentiation of PD-1 targeted therapy (Cheng et al., 2020). Consequently, TLR targeted therapy may potentially be used combined with PD-1/PD-L1 targeted therapy in the future.
In view of the dramatic increase in HPV-positive HNC in western countries we presently assessed the degree of p16 positivity and HPV DNA positivity in a contemporary cohort of HNC in the Kerala region, India. Moreover, we assessed whether TLRs may trigger adaptive immune responses in OC and OPC.
Materials and Methods
The study included patients (N = 72) with biopsy-proven squamous cell carcinoma of the oral cavity and oropharynx, diagnosed during the period January 2017 to December 2018. The samples also had to fulfill the quality control standards required for immunohistochemistry (IHC) and quantitative polymerase chain reaction (qPCR) at the Divisions of Oncopathology and Molecular Oncology of Malabar Cancer Centre (tertiary cancer center), Thalassery, Kerala, India. Ten patients with oropharyngeal carcinoma were retrospectively included from our previous cohort (2012–2017) (Pandiar et al., 2021). Patients included in the study had not undergone chemotherapy or radiotherapy before biopsy. Demographical data were retrieved from the medical charts of the patients.
IHC for p16 protein and PCR for HPV DNA subtype were performed on all 72 cases to ascertain the presence or absence of HPV. In the next set of experiments, in a subset of samples (due to lack of biopsy material), 18 OC and 21 OPC (10 P16+ and 11 P16−) were assessed with IHC for the expression of TLR3, TLR7, TLR8, and TLR9 and for helper T cells (CD4) and cytotoxic T cells (CD8). Moreover, the degree of inflammation was assessed.
DNA extraction
Four to five sections of 10 μm were taken in a 1.5 mL centrifuge tube, and deparaffinization was done using xylene. Further DNA isolation was done using QIAamp DNA FFPE Tissue Kit (Qiagen, Hilden, Germany) according to the protocol of the manufacturer. The final elution was done using 50 μL of nuclease free water.
Quantitative polymerase chain reaction
Quantity and purity of the DNA extractions were analyzed by loading 1 μL of DNA onto the NanoDrop spectrophotometer (Thermo Fisher Scientific, MA), where purity analysis was performed using ultraviolet absorbance 260/280 ratio and 260/230 ratio and quantitation using absorption at 260 nm. TRUPCR® high-risk (HR)-HPV with 16/18 Genotyping Kit (CE IVD; 3B BlackBio Biotech India Ltd., Bhopal, India) is a Real-Time Amplification test for the qualitative detection of HPV DNA in clinical samples. Extracted DNA from samples was amplified using real time amplification and detected using fluorescent reporter dye probes specific for 14 HR-HPV genotypes, that is, HPV16/18/31/33/35/39/45/51/52/56/58/59/66 and HPV68. The kit includes Master Mix and primer-probe mix for the specific amplification of E6/E7 region of the HPV, as well as a positive and a negative control to confirm the integrity of the kit reagents.
Three independent reactions ran parallel in three tubes of this kit. The first reaction detects any of the HR-HPV genotypes 16, 31, 33, 35, 52, 58, 51, 56, and 66 (FAM channel). The second reaction detects any of the HR-HPV genotypes 18, 45, and 59 (FAM channel) along with genotyping of HPV 18 (HEX) and Endogenous Internal Control (TEXAS RED). This allows exclusion of unreliable results. The third reaction detects either HR-HPV genotype 39 or 68 (FAM) along with genotyping of HPV16 (TEXAS RED). After preparing the reaction, the PCR program was set up as mentioned in the kit protocol. A sample showing a proper S-shaped curve with a Ct-value of <37 was considered as positive. Any sample without an S-shaped curve or with a Ct-value >37 was considered as negative.
Immunohistochemistry
IHC on tumor specimens detecting p16 (n = 72), TLR3 (n = 29), TLR7 (n = 29), TLR8 (n = 32), TLR9 (n = 32), and CD4 versus CD8 (n = 27) was performed. Paraffin-embedded tumor sections (3 μm) were heated to 60°C for 1 h and then kept overnight at 37°C. The next day the sections were deparaffinized in xylene and 100% ethanol and rehydrated by placing the sections in running tap water followed by washes in tris-base buffer (TBS; pH = 7.4). The sections were placed in ethylenediaminetetraacetic acid buffer solution and boiled in a pressure cooker.
After cooling, the sections were placed in distilled water followed by TBS washes. The sections were then covered with peroxide block (PathnSitu, Hyderabad, India). The primary antibody was then placed on the sections for 1 h. This was followed by adding polyexcel target binder (PathnSitu) for 30 min incubation followed by washing with TBS. The sections were then covered with polyexcel poly horseradish peroxidase (PathnSitu) for 10 min followed by washes in TBS and tap water. The sections were then covered with StunnDAB working solution (PathnSitu) and incubated for 5 min at room temperature. Finally, the sections were counterstained with hematoxylin followed by washes in running tap water and dehydrated in increasing concentrations of ethanol (70–100%) and xylene. At the end, the sections were mounted in DPX (Pallav Chemicals & Solvents Pvt. Ltd., Tarapur, India).
Assessment of IHC staining
Positivity of p16 for OPC was defined as a strong and diffuse nuclear and cytoplasmic staining in >70% of tumor cells (World Health Organization, 2017). Since no WHO defined criteria for p16 positivity in the oral cavity exists, p16 positivity was defined as when faint diffuse or strong p16 staining occurred in more than 40% of the tumor cells (Table 1 and Supplementary Fig. S1). TLR staining was scored low (1), moderate, or strong (3) for combined cytoplasmatic and nuclear staining. The ratio between CD8:CD4 was scored as −1 if CD8<CD4, as 0 if CD8 = CD4, and as 1 if CD8>CD4. The degree of inflammation was based on the following criteria for interpretation: Mild <50% (score 1): if the inflammatory infiltrate was less than 50% of the area of one high power field; moderate 50–75% (score 2): if the inflammatory infiltrate was between 50% and 75% of the area of one high power field; and marked >75% (score 3): if the inflammatory infiltrate was more than 75% of the area of one high power field.
Criteria for Interpretation of p16 Immunohistochemistry Staining in Oral Squamous Cell Carcinoma and Oropharyngeal Squamous Cell Carcinoma in the Oral Cavity
OC, oral squamous cell carcinoma; OPC, oropharyngeal squamous cell carcinoma.
Antibodies
Mouse monoclonal to CD8 (C8/468; PathnSitu), mouse monoclonal to p16 (INK4a, G175-405; Emergo, Netherland), mouse monoclonal to TLR9 (1:200, WH0054106M3; Sigma-Aldrich, St. Louis, MO). Polyexcel target binder (secondary antibody; PathnSitu), rabbit monoclonal to CD4 (EP204; PathnSitu), rabbit polyclonal to TLR3 (1:200, ab62566; Abcam, Cambridge, United Kingdom), rabbit polyclonal to TLR7 (1:200, PA5-95046; Thermo Fisher Scientific), and rabbit polyclonal to TLR8 (1:200, PA5-102413; Thermo Fisher Scientific).
Statistics
We used a sample size calculation based on the prevalence of HPV positive oral cancer (∼20%) and oropharyngeal cancer (20%) in India. The sample size was fixed as n = 30 for oral cavity and n = 30 for oropharynx, based on the power of the study calculated as n = z2P(1 − P)/d2 where n = number of samples, z = statistics for a level of confidence, and P = expected prevalence or proportion (in proportion of one; if 10%, d = 0.1%, d = precision). This total sample size for OC and OPC (n = 60) for the present study, calculated using the above equation, had expected proportion of 10% precision at 95% confidence interval.
As we planned to use formalin fixed paraffin embedded (FFPE blocks) for the detection of HPV DNA by PCR and given the fact that probably only 60% of the samples may pass the quality control of the isolated DNA, it would have been ideal to take 50% more samples to meet the target. The chi-square test was used to compare categorical data and the Mann–Whitney U test for continuous values. The Pearson correlation test was used for comparison between linear associations between immunohistochemical expressional patterns. Statistical significance was set to p < 0.05.
Results
The demographic details of patients and pathological data of the tumors are displayed in Tables 2 and 3. In brief, the proportion of male to female was 2:1, and the mean age of patients was 61 ± 1.4 years (median age 65). The OC was 45.2% well, 45.2% moderately, and 9.7% poorly differentiated where tumors originating in the tongue dominated in the cohort. OPC was keratinized in 87.8% and nonkeratinized in 12.2% of cases. While the ratio between men and women in the cohort was balanced for OPC, the ratio between men and women for OC was 9:1 (p < 0.001, Table 3). Smoking, alcohol use, and chewing areca nut and tobacco were common habits and occurred to the same degree in patients with OC and patients with OPC (Tables 3 and 4). Chewing of tobacco and/or areca nut occurred in 51.6% of OC patients and 36.6% of OPC patients (p = 0.20).
Demographics and Tumor Characteristics
Among “no data” there were 14 patients who were chewers, however, what was chewed was not recorded.
Demographics and Pathology in Oral Squamous Cell Carcinoma and Oropharyngeal Squamous Cell Carcinoma
The bold value indicates where significance is attained in the tables.
Among “no data” there were seven patients who were chewers, however, what was chewed was not recorded.
HPV, human papillomavirus.
Correlations in Oral Squamous Cell Carcinoma
The bold value indicates where significance is attained in the tables.
TLR, toll-like receptor.
P16 and HPV DNA
Seven out of 31 OC (22.6%) were p16 positive (i.e., nuclear and cytoplasmic staining in >40% of tumor cells) but only 3.2% (1/31) of OC was positive for HPV16 DNA. While 24.4% (10/41) of OPC was positive for p16, HPV16 DNA was found in only one P16-positive OPC and in no P16-negative OPC. HPV-positive OPC constituted therefore only 2.4% of all OPC (Table 3).
Inflammation and TLR expressions in OC and OPC
The inflammatory score was higher and the ratio CD8/CD4 tended to be higher in OC compared with OPC (p = 0.04 and p = 0.051, respectively, Fig. 1a–c). TLR3, TLR7, TLR8, and TLR9 were expressed both in OC and in OPC (Fig. 2a, b). The expression of TLR7 was significantly higher in OPC compared with OC (p = 0.030; Fig. 2b). In OC, the expressions of TLR3, TLR7, TLR8, and TLR9 were neither correlated with the inflammatory score nor the balance between CD4+ and CD8+ lymphocytes (Table 4). TLR8 expression was correlated with and TLR7 tended to be correlated with the inflammatory score in OPC (r = 0.56, p = 0.039, n = 14 and r = 0.52, p = 0.08, n = 12, respectively; Table 5).
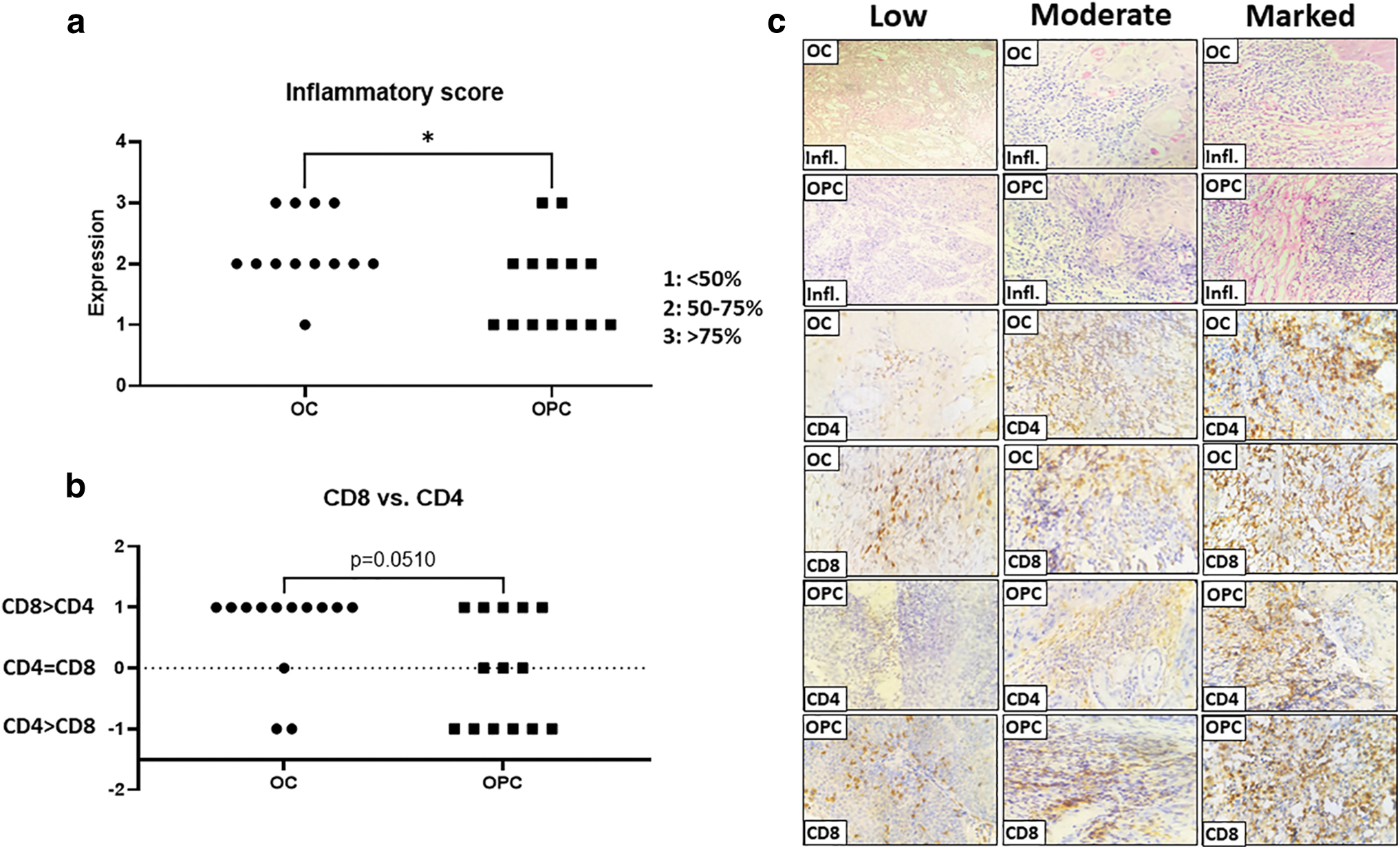
The inflammatory score in OC and OPC

Plot over the expression of TLR3, TLR7, TLR8, and TLR9 in OC and OPC
Correlations in Oropharyngeal Squamous Cell Carcinoma
The bold value indicates where significance is attained in the tables.
Correlation is significant at the 0.05 level (two tailed).
Discussion
In the present study we show that HPV does not seem to be an important player neither in OC nor in OPC in the Kerala region in India. We also show that TLR7 may potentially trigger an inflammatory response in OPC.
p16 positivity was found in 7 out of 31 cases of OC (22.6%) but only 1 out of these 7 p16-positive cases was also positive for HPV DNA (14%). This indicates that p16 does not seem to be a reliable biomarker for HPV positivity for OC. This finding is consistent with findings from the Swedish cohort of patients with OC and leukoplakia (Sundberg et al., 2019). Our results are also in line with studies from Mangalore in the Karnataka state in South India where no case of HPV DNA positivity was found in OC (Bandhary et al., 2018). A similar degree of p16 positivity (10 out of 41 cases) was also found in OPC, which is similar to the one reported from Visakhapatnam on the east coast of India (Sabu et al., 2019). However, we found that only 1 case out of 41 cases (2.4%) was positive for HPV DNA. The low degree of HPV DNA positivity is consistent with previous studies from South India (Bandhary et al., 2018). While high concordance between p16 and HPV DNA positivity in OPC cohorts has been reported from Belgium, Norway, Sweden, and Korea (Carpen et al., 2018; Fossum et al., 2017; Kim et al., 2020; Simoens et al., 2022), high discordance has instead been reported from studies in South Africa and Thailand (Arsa et al., 2021; Dapaah et al., 2022). p16 is used as a surrogate biomarker for HPV positivity in OPC in the Western world (Amin et al., 2017).
Studies show that p16+ OPC has better clinical outcome after treatment (Ang et al., 2010). Retrospective studies suggest that dose de-escalation of radiotherapy can be performed in HPV-positive OPC without affecting overall survival (Gabani et al., 2019). However, the sensitivity of p16 as a biomarker for HPV is low, and the prognostic significance for p16 positivity has been questioned for other sites such as the uvula, soft palate, and pharyngeal wall (Hammarstedt et al., 2021). Studies show that patients with p16+/HPV− OPC have worse clinical outcome than patients with p16+/HPV+ OPC (Nauta et al., 2018). How p16 should be used as prognosticator in other continents outside the Western world is unknown. We suggest that p16+/HPV− OPC constitutes a subgroup more common outside of the Western World. The origin of patients may therefore be of importance in the clinical decision of any down-escalation of chemoradiotherapy.
In OC, the inflammatory score was higher compared with the inflammatory score in OPC. There was a predominance of CD8+ lymphocytes compared to CD4+ lymphocytes in OC and the dominance strongly tended to be larger compared to OPC. The number of CD8+ lymphocytes is higher in OC compared with leukoplakia, and CD8+ TILs are associated with a favorable prognosis in OC (Boxberg et al., 2019; Missale et al., 2021; Ohman et al., 2012). While TLRs were not associated with the degree of inflammation and the CD8:CD4 ratio, the expression of TLR7 was higher in OPC than in OC. TLR7 tended to be and TLR8 expression was positively correlated with the degree of inflammation in OPC. In tongue base cancer, CD8+ TILs were associated with TLR5 but not with TLR7 (Jouhi et al., 2017). Intratumoral administration of TLR7/8 agonists may expand CD8+ TILs in mice and induce potent antitumoral effects in different animal models of cancer, including HNC (Lu et al., 2019; Rolig et al., 2022; Wang et al., 2021; Zuniga et al., 2022). Several studies are ongoing assessing the clinical efficacy of TLR7/TLR8 agonists in cancer treatment (Frega et al., 2020).
A restriction of the study is the limited number of individuals assessed. The power may have been too low to fully assess the involvement of TLRs in OC and OPC. The study was also most likely underpowered to assess any differences between OC and OPC in the prevalence of smoking, alcohol use, and tobacco and areca nut chewing. Moreover, the study was conducted in one single center.
In conclusion, HPV infection is not an important factor in the development of HNC, and p16 is not a good surrogate marker for HPV positivity in the Kerala region in India. We suggest that p16+/HPV− OPC constitutes a different group of tumors from p16+/HPV+ and p16−/HPV− tumors and which may be considered in treatment decisions. TLR8 is correlated with the degree of inflammation in OPC. Future trials assessing whether TLR7/TLR8 agonists may be used in the therapy of HNC are warranted.
Footnotes
Acknowledgments
The authors thank Sreelakshmi Panthalath Gangadharan, Malabar Cancer Centre, for help with data collection and Jayesh Saha, Malabar Cancer Centre, for help with qPCR.
Data Availability Statement
Additional data can be acquired by submitting a written request to the Institute of Clinical Sciences, Sahlgrenska Academy at the University of Gothenburg, Medicinaregatan 3A Göteborg SE-413 90, Sweden. E-mail: klinvet@gu.se
Ethics Approval Statement
The study was approved by the Institutional Ethics Committee, Malabar Cancer Centre (No. 161/IEC-ERC/13/MCC/21-1-2020/35).
Patient Consent Statement
Informed consent was waived by the Institutional Ethics Committee, Malabar Cancer Centre.
Authors' Contributions
Study concepts: S.K.N., D.R., S.S., G.K., B.H., D.G.; Study design: S.K.N., D.R., S.S., G.K., B.H., D.G.; Data acquisition: S.K.N., D.R., S.S.; Data analysis and interpretation: S.K.N., D.R., S.S., D.G.; Statistical analysis: S.K.N., S.S., D.G.; Article preparation: S.K.N., S.S., D.G.; Article editing: S.K.N., D.R., S.S., G.K., B.H., D.G.; Article review: S.K.N., D.R., S.S., G.K., B.H., D.G.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Director General of Indian Council of Medical Research, Department of Health Research, Ministry of Health and Family Welfare, Government of India sanctioned the budget allotment of Rs. 1,201,160/- as grant-in aid for the Project titled “Assessment of key immune factors in pathogenesis of HPV associated oral and oropharyngeal squamous cell carcinoma” under Dr. Sangeetha K. Nayanar, Malabar Cancer Centre, Thalassery, India. Moreover, the study was sponsored by the King Gustav V Jubilee Clinic Cancer Research Foundation, Gothenburg, Sweden [grant number no: 2021:352].
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.