
Abstract
The COVID-19 pandemic response has been hindered by the absence of an efficient antiviral therapy for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The reason why the previous preventative approach to COVID-19 solely through vaccines has failed could be a lack of understanding of how quickly the SARS-CoV-2 virus evolves. Given the absence of specific treatments for the virus, efforts have been underway to explore treatment options. Drug repurposing involves identifying new therapeutic uses for approved drugs, proving to be a time-saving strategy with minimal risk of failure. In this study, we report the successful use of a multidrug approach in patients with COVID-19. Successful administration of multidrug therapy, such as combinations of hydroxychloroquine and azithromycin, doxycycline and ivermectin, or ivermectin, doxycycline, and azithromycin, has been reported. Multidrug therapy is effective because of the differing mechanisms of action of these drugs, and it may also mitigate the emergence of drug-resistant SARS-CoV-2 strains. The medicines were lopinavir/ritonavir (Kaletra), bamlanivimab (monoclonal antibody), glycopyrrolate-formoterol (Bevespi), ciclesonide (Alvesco), famotidine (Pepcid), and diphenhydramine (Benadryl).
Introduction
To comprehend how a disease manifests, one must understand the anatomy, physiology, and pharmacology of the body, as well as the modus operandi of the pathogen. COVID-19 targets the ACE 2 receptor of the body and, similar to other viruses such as the Middle East Respiratory Syndrome virus, infiltrates the pulmonary CD4 cells, leading to secondary atypical infections.
ACE 2 receptors are widespread in the body’s epithelia. ACE 2 enzymes activate bradykinin, resulting in increased cellular permeability. The consequence of this activation is the accumulation of fluid, which is cleared by the secretion of hyaluronic acid, particularly in the lungs, giving rise to the characteristic appearance of ground glass on X-ray and CT scans (Kouhpayeh et al., 2021; Tolouian et al., 2020) (Fig. 1).

Illustrating key locations for angiotensin converting enzyme receptors [From Mangat, 2023, used under Creative Commons CC-BY 3.0 license].
As the ACE 2 pathways become activated, patients may experience acute shortness of breath due to fluid accumulation in the alveoli. Activation of ACE 2 receptors in the pulmonary vessels can lead to a pulmonary embolism if left unaddressed (Franco-Moreno et al., 2020; Kouhpayeh et al., 2021). In the gastrointestinal system, ACE 2 activation results in fluid secretion, leading to diarrhea. Activation of ACE receptors in the olfactory neuroepithelium causes a loss of smell (Salmon Ceron et al., 2020) and subsequent loss of taste due to involvement of the facial nerve. COVID-19 can spread to the basal cisterns, causing inflammation and subsequent headaches (Seth and Kushwaha, 2020). The increased pressure in the basal cisterns can lead to elevated intracranial pressure, which may be released through the internal auditory canal into the subarachnoid space, causing enhancement of the mastoid segment of the facial nerve and mastoiditis (Frazier et al., 2020). ACE 2 inhibitors, ARB blockers, and ibuprofen can upregulate ACE 2 expression. Therefore, it is advisable to switch ACE inhibitors to alternative blood pressure medications in COVID-19 patients. In addition, patients are advised to avoid nonsteroidal anti-inflammatory drugs such as ibuprofen for fever management.
The body also has a novel cytokine signaling pathway activated by the JAK2 pathway that can be blocked by JAK 2 inhibitors (Bhalwani et al., 2021), for example, famotidine, apoquel, and baricitinib limiting the progression pathway set up by ACE2 receptor activation. As a standard, we administer famotidine 40 mg bid to delay the onset of the inflammatory response.
Background
Coronaviruses were initially discovered in 1964 by June Almeida in Glasgow. They are common commensals found in the back of the nose and throat. They have hallmark crown-type accessories externally, which harbor the spike protein to attach to the ACE receptor. Internally, COVID-19 is an RNA virus with 16 gene fragments of HIV1, HIV2, and SIV (Perez and Montagnier, 2020). COVID-19 is 1000 times more powerful in attaching to the spike protein compared with Almeida’s coronaviruses (Fig. 2).

JAK 2 pathways in relation to cytokine release COVID-19. (From Mangat, 2023, used under Creative Commons Creative Commons CC-BY 3.0 license).
Research conducted in Bergamo (Setti et al., 2020) and at Harvard (Wu et al., 2020) has demonstrated that SARS-CoV-2, the virus responsible for COVID-19, can be found on facial hair and within ventilation systems. These findings indicate that the virus can also adhere to particulate matter in the air, potentially contributing to increased rates of COVID-19 transmission in areas with higher levels of air pollution.
Analysis of bronchoalveolar lavage samples from COVID-19 patients has revealed heightened concentrations of hyaluronic acid, attributed to the upregulation of hyaluronan synthases and the downregulation of hyaluronidase (Garvin et al., 2020). In conjunction with increased lung permeability resulting from bradykinin release, hyaluronic acid facilitates fluid absorption.
Consequently, elevated levels of hyaluronic acid may impede gas exchange and contribute to alveolar damage, particularly in cases involving inappropriate ventilator settings. Notably, the United States has observed the highest mortality rate associated with COVID-19 (Fig. 3).

Cross section through COVID-19 virus. Coronaviruses are a large family of viruses that include the common cold, severe acute respiratory syndrome (SARS), and the novel coronavirus responsible for a global pandemic in 2020. This model shows the structure of pathogens in the coronavirus family. [From Mangat, 2023, used under Creative Commons Creative Commons CC-BY 3.0 license].
COVID-19 treatment
If left unchecked, COVID-19 progresses through a biphasic course, ultimately leading to pulmonary embolism. The initial phase, termed the viremic phase, typically lasts 7–10 days (see Fig. 4), during which a four-phase therapeutic approach can effectively reduce viral load. Common symptoms include fever, sore throat, fatigue, bodily aches, anorexia, loss of smell/taste, nausea, and diarrhea.
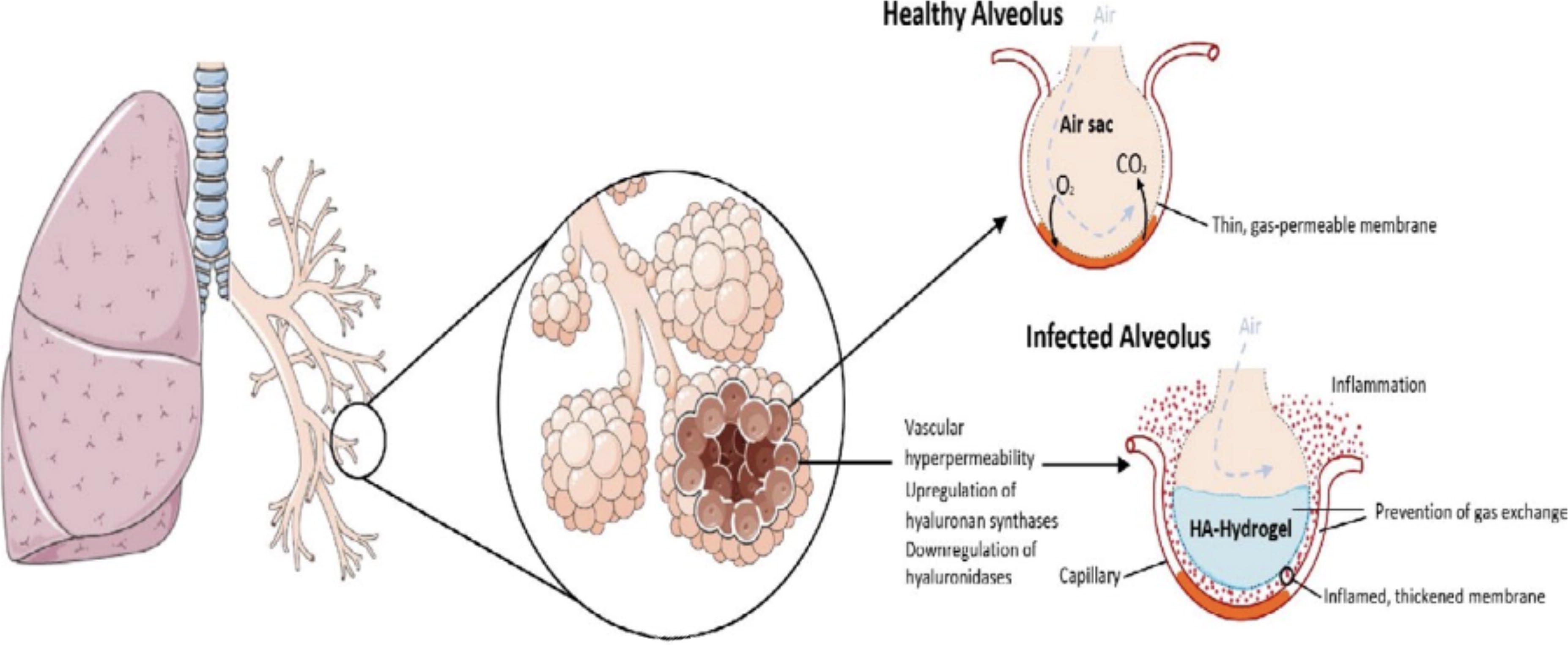
Diagram Illustrating Hyaluronic deposition during COVID-19 [From Mangat, 2023, used under Creative Commons Creative Commons CC-BY 3.0 license].
The subsequent phase involves a host-mediated response characterized by cytokine storm and thrombosis, necessitating the continuation of medications from the initial phase alongside high-dose steroids and supplementary treatments to mitigate the cytokine storm and thrombotic events. Unfortunately, studies have been conducted utilizing antiviral agents without adequately dosed steroids during this phase of the disease, suggesting a limited understanding of its pathophysiology.
The COVID-19 injury, along with clinical signs and phases of disease progression, is summarized in Figure 4 above.
Most of the time, treating most severe viral infections involves early intervention with multiple therapeutic agents. This strategy has not been implemented in clinical trials for COVID-19 conducted by governmental or industrial sponsors. Given that the COVID-19 syndrome is characterized by rapid viral proliferation, cytokine-mediated organ damage, and dysfunction, as well as endothelial injury leading to platelet aggregation and thrombosis (see Fig. 5), it is unrealistic to expect a single drug or antibody to address all of these pathological manifestations effectively.
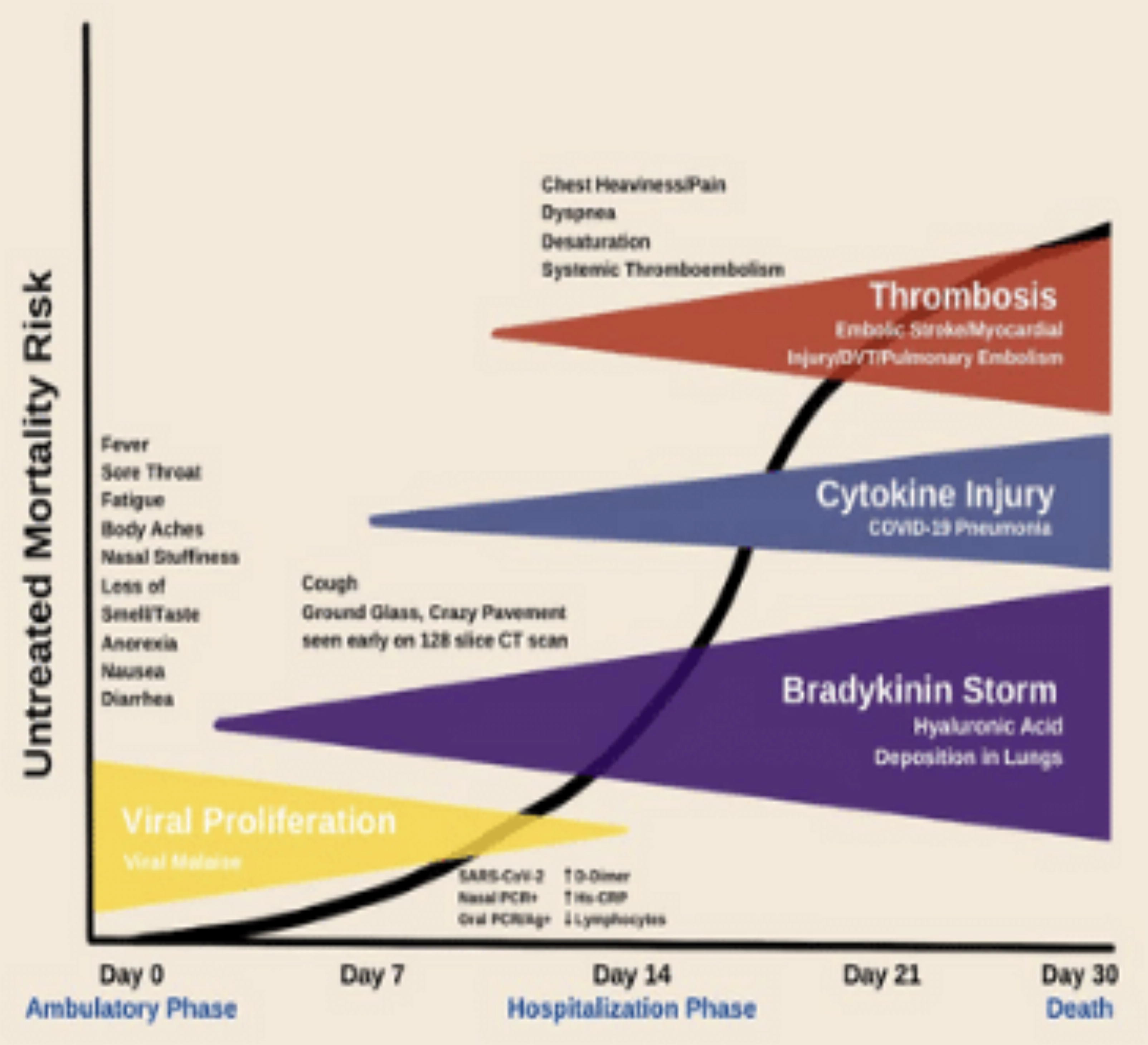
Phases of Disease Progression Following Untreated COVID-19 injury. Major dimensions of COVID-19 infection that call for a multidrug strategy in the early ambulatory period with available medications, including anti-infectives (hydroxychloroquine, ivermectin, azithromycin, doxycycline), corticosteroids, and antiplatelet drugs and anticoagulants. The phases of the infection and their time-course allow for the sequenced multidrug approach to be utilized with the goal of reducing hospitalization and death. (Adapted from: https://www.imrpress.com/journal/RCM/21/4/10.31083/j.rcm.2020.04.264/htm, used under Creative Commons CC-BY license).
For ambulatory patients exhibiting recognized signs and symptoms of COVID-19 on the first day (see Fig. 5), often before oral antigen testing, three therapeutic principles should be applied (Centers for Disease Control and Prevention, 2020): 1) combination anti-infective therapy to inhibit viral replication, 2) corticosteroids to regulate cytokine storm, and 3) antiplatelet agents/antithrombotic therapy to prevent and manage vascular thrombosis.
Step 1 phase zero treatment
The objective during phase zero is to reduce viral load and inhibit the adherence of the spike protein to the ACE 2 receptor. (Fig. 6) This goal is achieved by administering nasal rinses targeting the posterior nasal/throat area with normal saline. This approach is straightforward and highly effective because SARS-CoV-2 primarily resides in the posterior nasal/throat region. Furthermore, inhalers containing agents such as glycopyrrolate (e.g., Bevespi/Breztri) or ipratropium bromide are utilized to desiccate respiratory secretions.

Approaches in targeting COVID-19 prior to spike protein activation. (From Mangat, 2023, used under Creative Commons Creative Commons CC-BY 3.0 license).
In addition, inhalers with both antiviral and steroid properties, such as Alvesco and Pulmicort, can be used concurrently with a desiccating inhaler.
Step 1 phase 1 treatment
The objective of this stage is to hinder the binding of the SARS-CoV-2 spike protein to ACE 2 receptors and alleviate the bradykinin storm. While monoclonal antibodies effectively prevent binding, viral load may take 2–6 days to decline altogether. Therefore, careful monitoring for thromboembolic events is imperative. The administration of diphenhydramine or cetirizine, both second-generation antihistamines, can mitigate the bradykinin storm (Fig. 7).

Drug mechanism of action. Sequential multidrug treatment algorithm for ambulatory acute COVID-19-like and confirmed COVID-19 illness. ACE2, angiotensin receptor 2; TMPRSS2, transmembrane serine protease 2. (Adapted from: https://www.imrpress.com/journal/RCM/21/4/10.31083/j.rcm.2020.04.264/htm, used under Creative Commons CC-BY license).
Step 1 phase 2 treatment
This stage recognizes the attachment of the spike protein of COVID-19 to the ACE 2 receptor and the subsequent targeting of viral multiplication by various drugs. These drugs include hydroxychloroquine, which encapsulates COVID-19, as well as protease inhibitors such as lopinavir/ritonavir, nirmatrelvir/ritonavir, and remdesivir, which target viral replication. Remdesivir should be avoided in patients with renal impairment and limited to no more than two doses due to its renal toxicity. Nirmatrelvir/ritonavir pose risks of multiple drug interactions, necessitating cessation of concurrent medications when used. Moreover, there is a growing occurrence of failure with nirmatrelvir/ritonavir as the virus undergoes mutations (Epling et al., 2023).
In addition, ivermectin can be utilized as it inhibits RNA replicase and serves as a transmembrane serine protease 2 inhibitor, impeding the attachment of the immature spike protein following viral replication. It is customary to use both a protease inhibitor and hydroxychloroquine simultaneously to expedite the reduction of viral load, although this multidrug approach can prolong the mitigation of variant resistance viruses.
We recommend supplementing with a daily dosage of 12 mg for individuals with reliable access to ivermectin. Higher doses may induce adverse effects such as dizziness, tachycardia, uveitis, and keratitis, leading to decreased visual acuity. It is crucial to recognize that COVID-19 is characterized by significant inflammation, and daily administration of 325 mg aspirin mitigates the risk of vascular occlusive disease.
Step 1 phase 3 treatment
This context aims to halt the advancement toward cytokine storm utilizing JAK 2 inhibitors such as famotidine, apoquel, and baricitinib. Administration of famotidine at 80 mg daily effectively suppresses the cytokine storm pathway.
Step 2 phase 4 treatment
This manifests after a duration of 10 days or in individuals who have received suboptimal treatment earlier. The objective is to mitigate inflammation through the administration of high-dose steroids, such as prednisone at 60 mg twice daily, and to address any thromboembolic conditions with apixaban. Oxygen supplementation is often necessary, and Cura signa has developed an oxygen concentrator capable of delivering 10 L of continuous oxygen outside of hospital settings, surpassing the standard 6 L of continuous flow typically available in hospitals. Interleukin 7 blockers, such as tocilizumab, are used at this stage to suppress the cytokine storm. Notably, the past President of the United States authorized the release of this medication to the United Kingdom for the COVID-19 treatment of the then-Prime Minister (Balogun, 2021).
Furthermore, as we progress, the risk of atypical bacterial infections and atypical viruses rises, necessitating the use of clarithromycin levofloxacin or valacyclovir.
Considering the clinical challenge of delineating individual phases, we implement a treatment strategy comprising a 10-day regimen that includes all the listed drugs administered from the initial patient encounter.
Cases
Case description 1
In the first case report, a 44-year-old male presented himself after attending a Christmas family gathering. His past medical history included type 1 diabetes for 39 years, with a body mass index of 36 kg/m2, and a history of sleep apnea and acute respiratory distress syndrome in 2004. He reported experiencing the following symptoms: intermittent dry cough over the past 7 days, sore throat over the last 3 days, diarrhea lasting 1–2 days, constant headache persisting for the past 5 days, new-onset shortness of breath with a pulse oximetry reading of 95% accompanied by fever for 1 day, without chills, and loss of taste and smell for the past 5 days. After a COVID PCR test returned positive, we started him on a treatment regimen comprising lopinavir/ritonavir, hydroxychloroquine, aspirin, clarithromycin, Benadryl, and a Medrol dose pack.
Subsequently, we referred the patient to a monoclonal antibody center, where he received a bamlanivimab infusion on day 9. After infusion, the staff assured him that everything was satisfactory and indicated that they would contact him in a week. However, the patient did not adhere to the recommended daily checks. He returned to our clinic facility on day 14, reporting shortness of breath upon climbing one flight of stairs. A CT angiogram of the chest confirmed the presence of a pulmonary embolism. In addition, a CT scan revealed multiple ground glass opacities in both lungs, consistent with COVID-19 pneumonitis (See Fig. 8). Despite recommendations for hospitalization, the patient refused, citing fears related to his sister’s placement on a ventilator in the ICU.

Computed tomography angiogram of patient with COVID-19 pneumonitis. *Arrow points to site of pulmonary embolism (from Dr. Arvinder Uppal M.D., used with permission).
We started treatment with apixaban 10 mg twice daily for pulmonary embolism, Famotidine 40 mg once daily, intravenous (IV) solumedrol 60 mg twice daily for 5 days followed by a prednisone taper, IV ceftriaxone 2 g once daily for 5 days followed by oral clarithromycin 500 mg twice daily, and the use of incentive spirometry.
Ten days after the monoclonal antibody infusion, the patient developed fever and chills, prompting the initiation of treatment with Valtrex 1 g thrice daily for 7 days. The chills resolved after 24 h.
The patient returned to work 3 weeks after the initial COVID infection. His sister returned home 4 weeks after the initial COVID-19 infection, requiring supplemental oxygen.
Case description 2
A 67-year-old female horse dressage trainer, weighing 115 lbs., presents herself 12 days after a positive COVID test result. Her medical history includes a significant asthma diagnosis.
She had previously consulted with a physician who prescribed amoxicillin–clavulanate 875 mg–125 mg and prednisone 60 mg once daily for a span of 10 days. Despite the treatment regimen, she remained acutely short of breath and tested positive for COVID-19.
Initiated treatment includes the following: Aspirin 325 mg Lopinavir/ritonavir 200–50, two tablets twice daily for a total of 40 tablets Hydroxychloroquine 200 mg, two tablets twice daily for 40 tablets Prednisone 60 mg twice daily Clarithromycin 500 mg twice daily Famotidine 40 mg twice daily Benadryl 25 mg in the morning and cetirizine 10 mg at night Breztri and Alvesco, two puffs twice daily In addition, a CT angiogram of the chest was ordered using a 128-slice scanner.
The CT angiogram of the chest confirmed the presence of an early right lower lobe pulmonary embolus, along with a globular ground glass appearance in both lung fields indicative of COVID-19 pneumonitis and scarring of both lung bases.
Subsequently, the patient was commenced on Eliquis 10 mg twice daily for 1 week and administered IV ceftriaxone 2 g and solumedrol 60 mg twice daily for 5 days.
On the 18th day post-COVID diagnosis, the patient experienced a yeast infection and onset of oral herpes. Treatment consisted of valacyclovir 1 g thrice daily for 1 week and fluconazole 150 mg once daily.
Oxygen saturation levels were restored to 95%, with home oxygen at 2 L initiated. By the 20th day post-COVID diagnosis, oxygen saturation reached 97%. On the 21st day, the solumedrol dosage was reduced to 60 mg once daily.
By the 22nd day post-COVID diagnosis, oxygen saturation reached 98%, with continued treatment involving incentive spirometry and clarithromycin 500 mg twice daily. Over 6 weeks, steroid dosage was gradually reduced, and oxygen therapy was discontinued.
Three months later, a repeat CT angiogram conducted utilizing the same 128-slice scanner confirmed the resolution of the pulmonary embolus and pneumonitis.
Case description 3
A 59-year-old male patient, post-heart transplant and under immunosuppressive therapy, with a medical history, including insulin-dependent diabetes and sleep apnea, developed symptoms of sore throat, fever, and chills after exposure to his children who tested positive for COVID-19. Following a positive COVID-19 test, the patient was admitted to the transplant unit, where he received four doses of remdesivir, with close monitoring of renal function. Discharged 5 days later, he presented with a bronchitis cough, accompanied by the production of green phlegm, low-grade fever, and chills. Treatment was promptly initiated with lopinavir/ritonavir, HCQ, clarithromycin, Benadryl, and a Pulmicort inhaler. Within 10 days, the patient’s chest was clear, and he remained asymptomatic.
Correlation Analysis
We investigated the impact of different treatments on COVID-19 by analyzing the correlation between the number of symptoms and the duration of medication administration. The graph illustrates the relationship between the number of symptoms and the number of days each medicine was administered. (Fig. 9) The medications utilized were as follows: Alvesco (AlvDays); ciclesonide, Bevespi (BevDays); glycopyrrolate and formoterol, Benadryl (BenDays); diphenhydramine, famotidine (FamDays); antihistamine, Kaletra (KalDays); lopinavir/ritonavir, monoclonal antibodies (mABDays); and bamlanivimab. Symptoms were fever and chills. In a cohort of 26 patients, eight individuals (30.8%) received treatment comprising lopinavir/ritonavir, bamlanivimab, glycopyrrolate-formoterol, ciclesonide, and diphenhydramine. Notably, patients exhibited prompt amelioration of COVID-19 symptoms within a timeframe of 3–5 days. Subsequently, correlation coefficients were calculated for each medication in relation to the number of symptoms experienced by patients. A negative correlation coefficient signified a swifter resolution of symptoms.
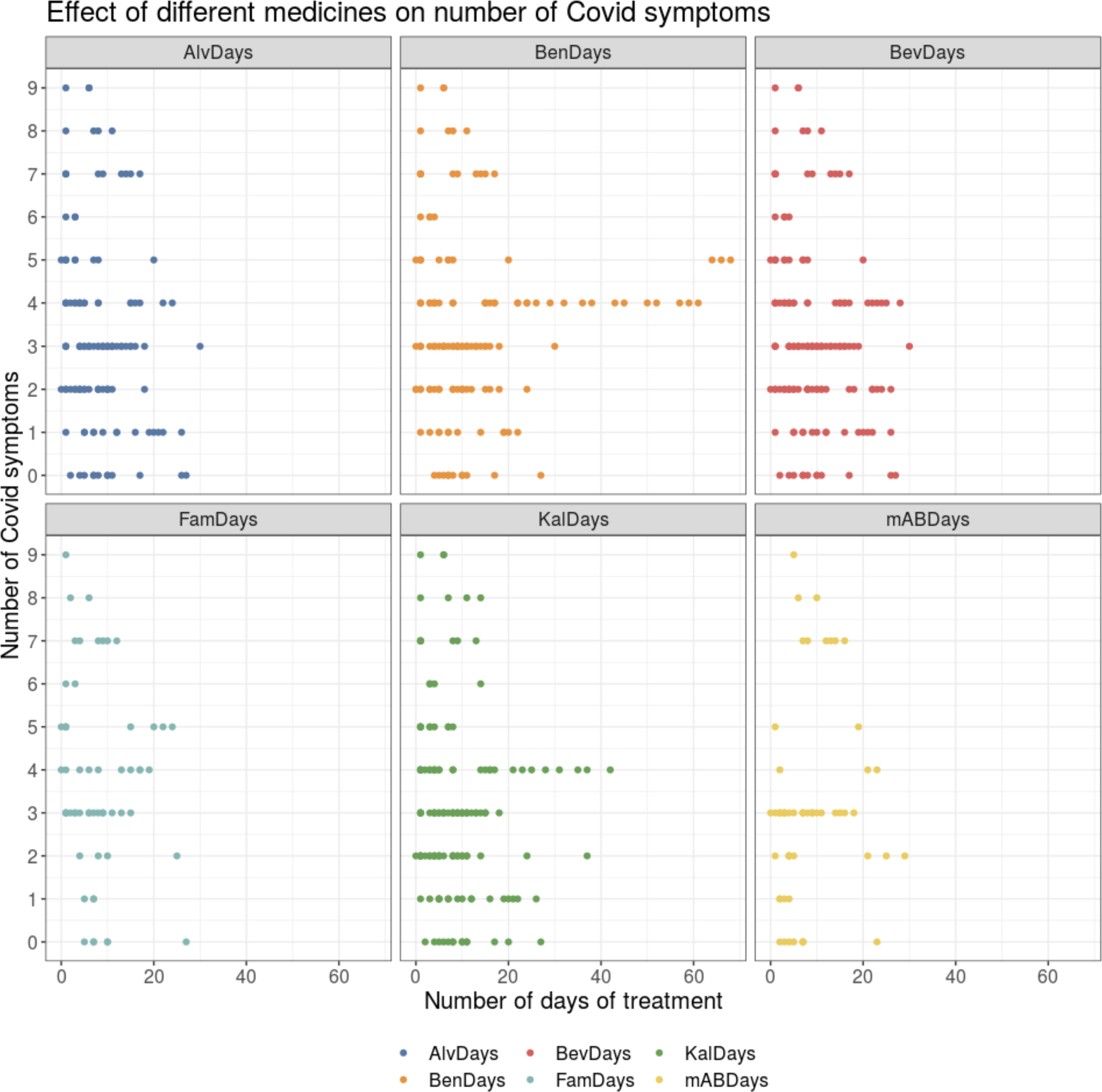
Effect of different medicines on the average duration of COVID-19 symptoms.
What can be inferred from the number of days a medicine was given?
Based on the raw data, it is evident that the duration of treatment corresponds to the number of days until symptoms were observed (except for one patient). The subsequent plot indicates that most treatments cease after 20 days, suggesting that this duration may be a reasonable period for treatment continuation. (Fig. 10)
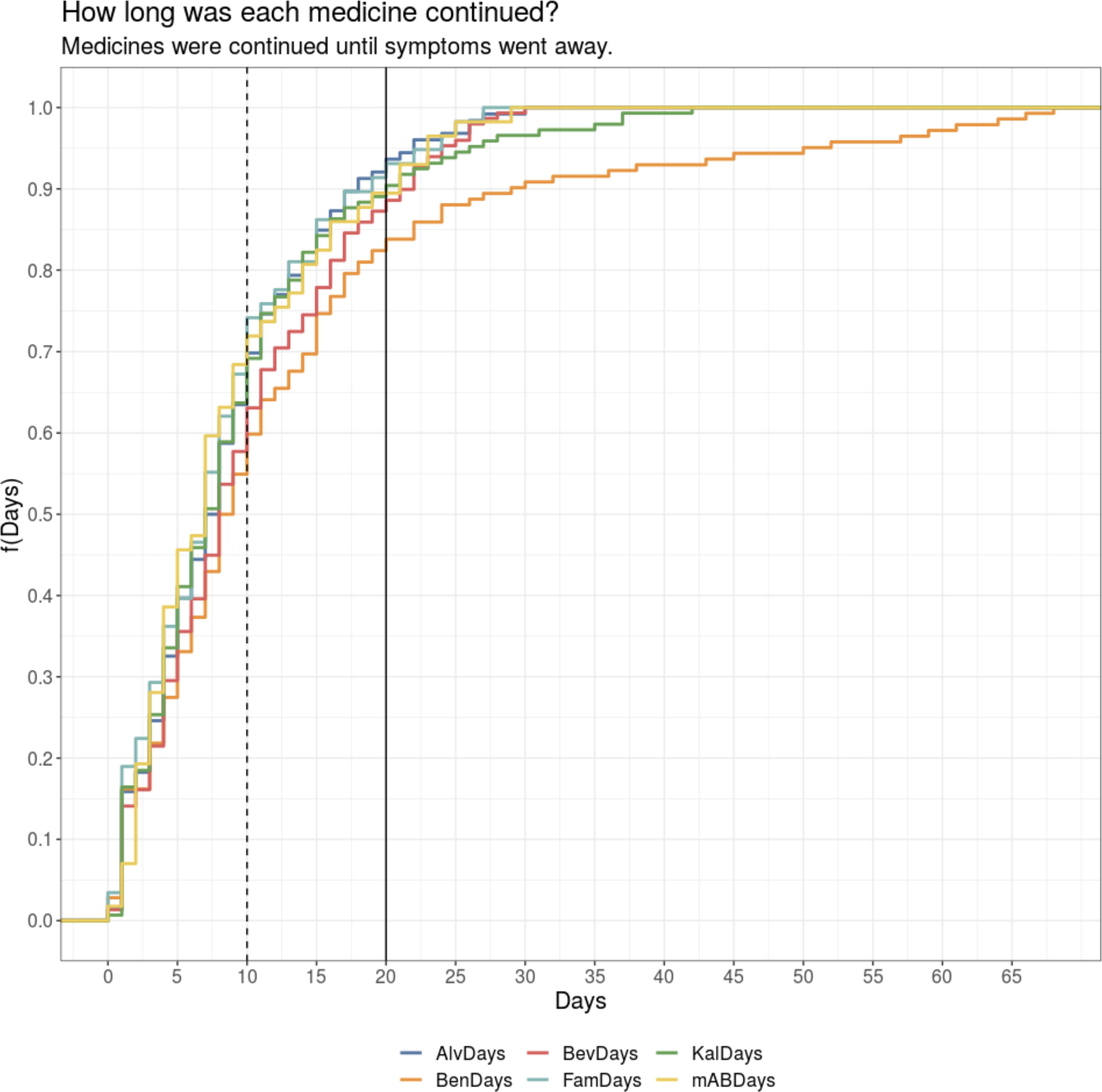
Duration of medication continuation.
Correlation between number of symptoms and day medicine was given
A modest inverse correlation is observed between certain medications and the quantity of symptoms, consistent with the anticipated trajectory in which symptom reduction aligns with treatment progression. Conversely, a minor positive correlation is noted between Benadryl administration and symptom count, a trend that persists across the analysis of Benadryl’s impact on symptomatology. ## correlation between KalDays and symptoms is −0.1407 ## correlation between BevDays and symptoms is −0.227 ## correlation between AlvDays and symptoms is −0.2191 ## correlation between BenDays and symptoms is 0.0353 ## correlation between mABDays and symptoms is 0.1429 ## correlation between FamDays and symptoms is −0.1554
Discussion
The emergence of the SARS-CoV-2 outbreak represents a unique event occurring once in a century, yet it has not been effectively addressed through the adoption of a multirepurposed drug strategy, similar to that utilized in tuberculosis treatment. The initial phase of viral replication, resembling symptoms of influenza, presents a critical window of opportunity for potentially mitigating the risk of more severe outcomes among high-risk individuals. Valuable time is lost due to the adoption of a passive “wait and see” approach, which lacks antiviral treatment as the condition progresses, potentially leading to unnecessary hospitalizations, increased morbidity, and mortality. Following infection, the sole means of preventing hospitalization in high-risk individuals involves the initiation of treatment before the onset of symptoms that would typically prompt paramedic calls or emergency room visits.
COVID has killed over a million people in the United States, the Fauci approach of “stay at home for 2 weeks and return to your physician if there is a problem” loses the valuable opportunity of stopping the progression of this condition in the viremic phase. Second, this approach gives time for the virus to take hold and increase the risk of long-term COVID-19 damage.
COVID-19 infection is a three-step disease, the initial phase within the first 10 days of infection is viremic, but as time progresses beyond day 10, we approach the period where the body produces a highly inflammatory reaction requiring high-dose steroids along with the antiviral therapy to arrest the disease progression. In recent studies, even though immunosuppressive therapy has shown promising results for control of the cytokine storm syndrome in severe cases of COVID-19, it is also well documented that immunosuppressive agents (e.g., corticosteroids and cytokine blockers) increase the risk of opportunistic infections.
It is, therefore, critical to be aware of the fact that COVID-19 induces immunosuppression, causing the rise of atypical bacterial pneumonia, viral pneumonia, and fungal infections that need to be taken into account and treated accordingly.
Not all drugs are created equal; this current administration has let go of monoclonal antibodies, which have shown a lower mortality rate than nirmatrelvir/ritonavir and paid premium costs. There has been increased failure of nirmatrelvir/ritonavir as the virus continued to mutate. Remdesivir has been shown to have serious nephrogenic possibilities to single kidney patients and those in renal failure. In the United States, it is still administered as a front-line treatment, whereas in other countries it has been stopped. To prevent resistance, we should adopt a multidrug approach and understand the downstream risks of atypical bacterial, viral pneumonia with fungal infections and treat early.
Conclusion
Initiating therapy promptly with a regimen comprising repurposed medications such as Kaletra, Bevespi (glycopyrrolate-formoterol), Alvesco (ciclesonide), Benadryl (diphenhydramine), monoclonal antibodies (bamlanivimab), and Pepcid (famotidine) disrupts the viral replication cycle and mitigates against the likelihood of cytokine storm onset. There is a need to look in the mirror and understand that our willful ignorance is the cause of the million dead in the United States today. We need to stop living in fear, be bold and treat COVID aggressively, and avoid long-term complications.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.