
Abstract
Evaluating the impact of cardiac surgery on humoral and cellular immunity in pediatric congenital heart disease patients with prior Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection or vaccination is crucial for postoperative care planning. This study enrolled 61 pediatric patients undergoing cardiac surgery with cardiopulmonary bypass at a single institution. Measurements were taken before the operation, immediately postoperation, and during the first follow-up examination at least 1 month later. The evaluations included SARS-CoV-2-specific immunoglobulin G (IgG) and neutralizing antibodies for humoral immunity assessment, as well as specific and nonspecific T-cell immune responses to gauge T-cellular immunity and functionality. The results demonstrated that the serum titers of IgG and neutralizing antibodies remained comparable postsurgery to preoperative levels. Nevertheless, significant decreases in specific and nonspecific T-cell immune responses, along with a decline in CD3+ T-cell numbers, were observed immediately following surgery. This was followed by a gradual recovery of immune response to preoperative levels approximately 1 month later. These findings suggest that in the first month following cardiac surgery in pediatric patients, residual specific antibodies, potentially derived from the original production or plasma transfusion, may provide partial protection against COVID-19 infection. Subsequently, T-cellular immunity gradually recovers and resumes its protective role. The study provides important insights into the dynamics of immune recovery following cardiac surgery in this vulnerable patient population, which may be essential for optimizing postoperative management and reducing the risk of COVID-19 infection.
Introduction
The coronavirus SARS-CoV-2, the causative agent of the COVID-19 pandemic, has posed significant challenges in managing infected patients with underlying health conditions, including pediatric patients with congenital heart disease (CHD). Surgical repair is the primary treatment for most congenital birth defects and is crucial for prolonging the life expectancy of pediatric CHD patients. The coexistence of COVID-19 infection and the need for surgical intervention requires careful consideration to ensure optimal outcomes while minimizing the risk of complications (Gupta et al., 2022; Shehata et al., 2020).
For CHD children who have been infected or vaccinated previously, their preexisting specific immunity, encompassing both humoral and T-cellular immunity, is considered the vital defense against the SARS-CoV-2 virus to prevent reinfections and mitigate the risk of severe illness (Ruedas-Lopez et al., 2020; Zhang et al., 2022). However, surgical procedures can disrupt physiological status—especially cardiopulmonary bypass (CPB), a common technique in cardiac surgery known to induce an inflammatory response and depress host defenses (Justus et al., 2019; Larmann and Theilmeier, 2004; Rodriguez-Lopez et al., 2022; Tárnok and Schneider, 2001). The abnormal immune system may affect the immune response against SARS-CoV-2 generated through infection or vaccination. During the epidemic, the cardiac surgeons wondered if the cardiac surgery might disturb the preexisting specific immunity, potentially compromising its protective efficacy. Several previous studies have shown that COVID-19-vaccinated CHD adult patients undergoing surgery with CPB experienced a reduction in SARS-CoV-2 antibody titers immediately postsurgery, which persisted for up to a month (Hayashi et al., 2022; Simsek et al., 2022; Strobel et al., 2023). Moreover, the global T-cell subset count, which is associated with the adaptive immune system, was found to decrease postoperatively in both adult and pediatric patients undergoing CPB operations (Akbas et al., 2002; Habermehl et al., 2003; Tajima et al., 1993). While these studies provide valuable insights into the impact of cardiac surgery on immunity in adult patients, there is limited research exploring the extent and persistence of both specific humoral and T-cellular immunity in pediatric CHD patients with cardiac surgery.
This study aimed to evaluate the preexisting humoral and T-cellular immunity against SARS-CoV-2 in CHD children following cardiac surgery. The titers of IgG and neutralizing antibody against SARS-CoV-2 were measured to assess the humoral immunity. In addition, a standardized whole-blood interferon-gamma release assay (IGRA) (Mouton et al., 2021; Saade et al., 2022) was performed to determine the specific-released interferon-gamma (IFN-γ), a key cytokine secreted by antigen-specific T cells, in order to assess both the SARS-CoV-2-specific T-cellular immunity and global T-cell functionality at the same time. This study aimed to aid clinicians in comprehending the impact of cardiac surgery on the preexisting immunity in pediatric CHD patients, thereby potentially guiding strategies for the prevention of postoperative infections and the optimization of booster vaccination protocols.
Materials and Methods
Study population and design
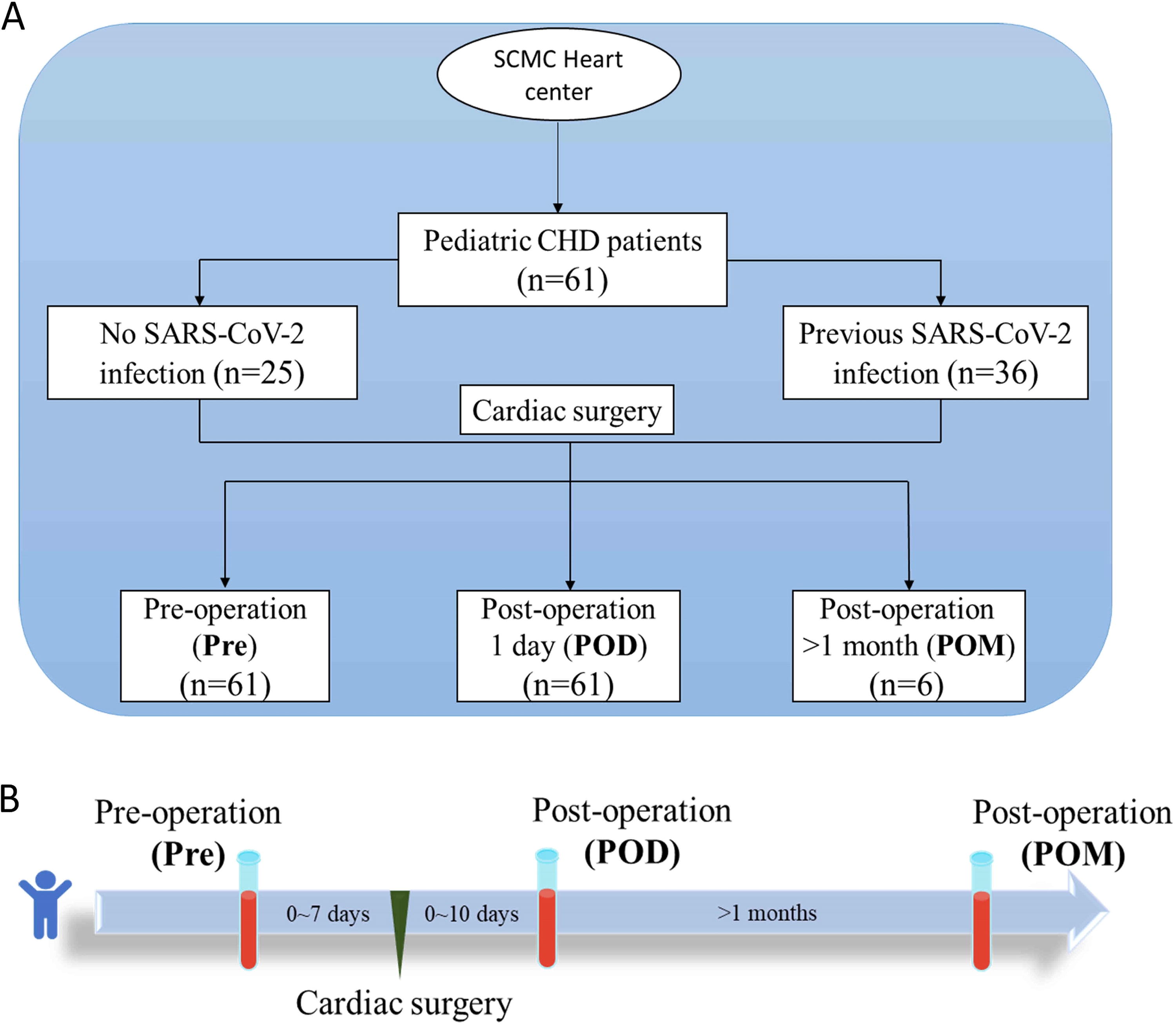
This single-center study was conducted at the Heart Center of Shanghai Children’s Medical Center between March and September 2023. A total of 61 pediatric patients with CHD who were admitted for cardiac surgery with CPB operation were recruited and enrolled in the analysis (Fig. 1A). Based on self-reported COVID-19 RT-PCR results upon admission, there were 25 patients who were considered as negative for the virus and 36 patients who had previously been infected within the past 6 months. Blood samples were collected from these patients at three distinct time points: within 7 days prior to the operation (Pre), during the hospital stay (within 10 days) immediately following the operation (POD), and during the first follow-up examination, which occurred at least 1-month postoperation (POM) (Fig. 1B). However, due to loss to follow-up, only six subjects were available for analysis at the POM time point. An age-matched control group consisted of children who had undergone allogeneic blood stem cell transplantation more than 2 years ago (median interquartile range [IQR] = 25.6 [24.3, 33.4] months) and had not received any medications (Supplementary Table S1). Following evaluation by hematologists, these children were determined to exhibit a relatively immunocompetent status (de Koning et al., 2016; Dekker et al., 2020).
Enrollment and sampling.
The enrolled pediatric patients’ characteristics, including age, sex, date of surgery, specific surgical procedures, and CD3+ T-cell counts obtained from flow cytometry, were collected from electronic patient records. Information regarding SARS-CoV-2 infection and vaccination with at least one dose of inactivated vaccines (CoronaVac/BBIBP-CorV) was obtained and verified through communication with the guardians of each pediatric patient. Most participants were last vaccinated more than 1 year ago.
Humoral immunity assessment
To assess humoral immunity, serum samples were tested for SARS-CoV-2-specific IgG and neutralizing antibodies (Nab) using chemiluminescence immunoassay (CLIA) (Suzhou Hybiome Biomedical Engineering Co., Ltd.). IgG was detected via indirect CLIA: serum samples were mixed with recombinant SARS-CoV-2 antigen to form immune complexes, which were immobilized on magnetic particles, labeled with acridinium ester-conjugated antihuman IgG, and quantified by chemiluminescence. A relative light unit ratio value above 1 S/CO (sample luminescence value/cutoff value), as defined by the manufacturer, was considered positive for IgG. Nab was measured by competitive CLIA: biotinylated SARS-CoV-2 RBD antigen bound to Nab, followed by acridinium ester-labeled ACE2 antigen competition and magnetic separation. The chemiluminescence intensity is inversely correlated with Nab levels. A threshold for positive Nab was determined by constructing a receiver operating characteristic curve, comparing the uninfected and unvaccinated group with the positive group, resulting in an optimized cutoff value of 63.8 IU/mL (Supplementary Fig. S1). Both IgG and Nab testing procedures were performed on the AE-180 fully automated CLIA analyzer (Suzhou Hybiome Biomedical Engineering Co., Ltd.).
Cellular immunity assessment
The SARS-CoV-2 specific T-cell response was monitored using the VIDAS® solution kits (bioMérieux). In brief, fresh heparinized whole-blood samples were stimulated with a stimulation reagent containing restricted SARS-CoV-2 peptide pools (AG) (VIDAS STIMMTM COVID RUO-bioMérieux). Meanwhile, a blood sample with a blank stimulation reagent served as a negative control (NIL), while a sample with a mitogen-containing reagent acted as a positive control (MIT) (Caruso et al., 1997; Lim et al., 1998) (VIDAS STIMM BASIC RUO-bioMérieux). All three stimulation reagents were prepared from freeze-dried powder by adding sterile deionized water to achieve a concentration of 200 μg/mL. The mixed samples were then incubated at 37°C under 5% CO2 for 22 h. After incubation, the supernatant of each sample was collected to measure the concentration of IFN-γ (VIDAS IFNg RUO-bioMérieux) based on a two-step sandwich enzyme immunoassay method with final fluorescence detection (ELFA) by using the miniVIDAS platform (bioMérieux). According to the kit instructions, the threshold of positivity for IFN-γ was set at 0.08 IU/mL (Mouton et al., 2021; Saade et al., 2022). A sample was considered reactive to SARS-CoV-2 if the IFN-γ concentration of the NIL was below 0.08 IU/mL and the AG was above the threshold, or if the difference between AG and NIL (AG − NIL) was above the threshold.
In addition to the SARS-CoV-2 specific T-cell response, the nonspecific T-cell response, reflecting global T-cell functionality, was also measured. A concentration of 100 μg/mL MIT (VIDAS STIMM BASIC RUO-bioMérieux) was used as a stimulant for nonspecific T-cell activation in this study. The incubation conditions for nonspecific stimulation were the same as those for specific stimulation. Following incubation, the relative fluorescent value of the nonspecific-released IFN-γ was measured using the miniVIDAS platform. This allowed for the assessment of the level of specific T-cell response and nonspecific T-cell response in the samples at the same time.
Statistical analysis
The demographic characteristics of the enrolled patients were summarized using the median and interquartile range for continuous data, while absolute values and percentages were used for categorical data. The results were presented as individual values and using boxplots, which depict the 25th to 75th percentile range along with the median. The chi-squared test was used for analyzing qualitative variables. The Mann–Whitney test was employed to compare continuous variables, such as IgG and neutralizing antibody titers, as well as specific- and nonspecific-released IFN-γ concentrations between uninfected and convalescent subjects. Wilcoxon signed-rank test was used to measure the difference between the groups at the Pre, POD, and POM time points. Further, the comparison of CD3+ T-cell counts of CHD children at the POD time point was compared with that of the control group. Pearson correlation analysis was used to assess the correlation between nonspecific-released IFN-γ and cell numbers or age. A p-value <0.05 was considered statistically significant. The statistical analyses were conducted using OriginPro2017 (OriginLab Corporation) for Windows which was also utilized to generate graphs and visualize the results.
Ethical statement
The study was approved by the institutional review board and the Ethics Committee of Shanghai Children’s Medical Center (SCMCIRB-K2022115-1). Written informed consent was obtained from all participating patients and/or their parents.
Results
Clinical characteristics
This observational clinical study enrolled 61 pediatric patients. They were categorized as 16 patients with no history of COVID-19 infection or vaccination (non), 34 patients with one history of infection or vaccination (C/V), and 11 patients with a history of both infection and vaccination (C&V) (Table 1). The C&V group showed a significantly older age compared to non and C/V groups. In other respects including gender, postinfection interval time, Risk Adjustment for Congenital Heart Surgery score, CPB and clamp duration time, and amount of transfusion plasma, there was no significant difference among the three groups. Anti-inflammatory medications such as methylprednisolone or ulinastatin were administered in all patients to mitigate operative inflammation. Four patients in the C/V group did not receive plasma transfusion (Table 1).
Clinical Characteristics of the Enrolled Patients
C/V, one history of infection or vaccination; C&V, with history of both infection and vaccination; IQR, interquartile range; Non, no history of infection or vaccination; RACHS, Risk Adjustment for Congenital Heart Surgery.
Specific humoral and T-cellular immunity against SARS-CoV-2
In this study, humoral immunity against SARS-CoV-2 was assessed by measuring antibody titers of IgG (Fig. 2A) and Nab (Fig. 2B). At the Pre time point, vaccinated convalescent patients (C&V group) exhibited significantly higher antibody titers for both IgG and Nab compared to those with a history of only infection or vaccination alone (C/V group). Patients with no history of infection or vaccination (nongroup) demonstrated the lowest levels of IgG and Nab. At the POD time point, there were fluctuations in the antibody titers compared to the Pre time point. Particularly, the low antibody titers observed at Pre time point, especially in nongroup, increased significantly at the POD time point. In contrast, the highest titers in C&V patients showed a downward trend but remained the highest among the three groups. Subsequently, at the POM time point, the patient’s antibody titers showed no significant changes compared to the POD time point, despite the limited number of cases.

Specific humoral immunity against SARS-CoV-2. The antibody titers of IgG
In addition to humoral immunity, the T-cell immune response to SARS-CoV-2 was assessed by measuring the concentration of IFN-γ released by specific T cells at three time points (Fig. 3). At the Pre time point, the nongroup exhibited the weakest response, with mostly samples being nonreactive. The C/V group showed an increased reactive T-cell response level. The strongest specific T-cell immune response was observed in C&V patients. These observations at the Pre time point align with the humoral immunity findings. However, at the POD time point, unlike the sustained specific antibody response, almost all subjects showed nonreactive specific T-cell response. Interestingly, the T-cell response recovered at the POM time point, reaching a similar level to that observed at the Pre time point. Overall, the specific T-cell immune response exhibited a significant decrease followed by recovery over time after surgery, a trend not observed in humoral immunity findings.

Specific T-cellular immunity against SARS-CoV-2. The concentration of IFN-γ reflected the SARS-CoV-2 specific T-cell immune response at Pre, POD, and POM time points. Non represented uninfected and nonvaccinated, C/V represented convalescent or vaccinated, and C&V represented convalescent and vaccinated. The vertical axis was logarithmic scale for clarity. The dashed line represented the threshold of positivity. The significance levels of corresponding population at two time points (POD vs. Pre, POM vs. POD) were marked above the boxplot. *p < 0.05, ***p < 0.001. IFN-γ, interferon-gamma.
Global T-cell functionality
To assess the impact of cardiac surgery on global T-cell function, we evaluated the nonspecific T-cell immune response alongside the specific T-cell immune response in CHD children undergoing cardiac surgery with CPB (Fig. 4A). Our results demonstrated that, at the preoperative (Pre) time point, the enrolled pediatric CHD patients displayed a significantly lower level of nonspecific-released IFN-γ compared to the control group, indicating a compromised global T-cell functionality even before surgery. At the POD time point, a significant decline in global T-cell functionality was observed among all subjects, which gradually recovered to preoperative levels by the postoperative month (POM) time point. This trend in global T-cell function mirrored the variations in specific T-cell immunity. Consistent with the findings for global T-cell functionality, a significantly lower level of the CD3+ T-cell counts (Fig. 4B) was observed in all subjects compared to the control group at the POD time point. Further, the global T-cell functionality of pediatric CHD patients at the POD point and control group exhibited a high correlation with their CD3+ T-cell numbers (Fig. 4C). These findings suggest that after surgery, CHD patients exhibited a T-cellular immune suppressed status, reflected by both reduced T-cell numbers and compromised T-cell function.

Global T-cell functionality.
Since cellular immune function can be influenced by age, global T-cell functionality was further evaluated across different age groups. A moderate correlation between global T-cell functionality and age was evident (Supplementary Fig. S2A). Notably, children above 3 years old exhibited higher levels of global T-cell functionality compared to those below 3 years old at all three test points (Supplementary Fig. S2B). However, no significant differences were found in the SARS-CoV-2-specific T-cell immune response between patients above and below 3 years old (Supplementary Fig. S3).
Discussion
As SARS-CoV-2 has become a common respiratory tract infectious agent and new variants of the virus continue to emerge, it is crucial for pediatric CHD patients undergoing cardiac surgery to maintain a persistent and robust humoral and cellular immune response. This is essential for protecting against the virus, preventing reinfections or severe infections during hospitalization, and ensuring a smooth postoperative recovery.
Cardiac surgery, particularly the frequent use of CPB, can significantly impact the patient’s immune system, influencing humoral immunity levels (Bufkin et al., 1995; Lante et al., 2005; Lesouhaitier et al., 2024). Previous studies have reported a significant reduction in SARS-CoV-2-specific IgG levels in vaccinated adult CHD patients undergoing cardiac surgery with CPB (Hayashi et al., 2022; Simsek et al., 2022; Strobel et al., 2023). Consistent with these findings, our study observed a decline in SARS-CoV-2 antibody levels in pediatric CHD patients with high preoperative titers after surgery (C&V patients in Fig. 2). Hemodilution and increased volume of distribution due to the extracorporeal circulation might lead to lower the concentration of antibodies (Khuri et al., 1992; Siminelakis et al., 1996). Surprisingly, for the majority of pediatric CHD patients with low preexisting titers in this study (non and C/V patients in Fig. 2), an upward trend was observed in their postoperative SARS-CoV-2 antibody levels. One possible explanation for the varying observations could be the blood transfusion procedure performed during surgery. Given the widespread COVID-19 vaccination among the Chinese population and a nationwide infection outbreak several months prior to sample collection, blood donors were likely to have moderate levels of SARS-CoV-2 antibodies (Goldberg et al., 2023). This may have minimized the impact of hemodilution on the original antibody titers in patients with moderate or low levels. Consequently, CHD patients with low antibody levels, particularly those who were uninfected and nonvaccinated, may have experienced a surge in their blood’s SARS-CoV-2 antibodies following surgery. To verify this hypothesis, we compared four C/V patients who did not receive blood transfusions during surgery with other C/V patients (n = 22). We found that CHD patients without plasma transfusion showed consistently low antibody titer at Pre and POD time points, while a significant increase in antibody titers was observed in most patients who received plasma transfusion at their POD time point (Supplementary Fig. S4), indicating a potential effect of plasma transfusion on the antibody levels. Notably, the increased antibody levels included not only total IgG but also functional antibodies, as demonstrated by elevated SARS-CoV-2 RBD antigen-binding Nab (Fig. 2B). Prior evidence indicates that passively transferred IgG antibodies have a half-life of 3–4 weeks (Thibault et al., 2016), and transfusion of SARS-CoV-2 antibodies can reduce disease severity in infected individuals (Abraham, 2020; Rajendran et al., 2020). These findings suggest that the infused antibodies may provide temporary protection during the critical postoperative recovery phase. In summary, the combined effects of surgical procedures, CPB, and the unique influence of blood transfusions during the pandemic period may have contributed to a complex dynamic of SARS-CoV-2 antibody levels in this study.
It is worth mentioning that this study could be the pioneer in utilizing a standardized whole-blood IGRA to evaluate both the specific and nonspecific T-cellular functionality of CHD children. The results revealed that, contrary to humoral immunity, there was a marked decline in specific T-cellular immunity against SARS-CoV-2 immediately following cardiac surgery, which gradually recovered over time. This trend was also observed in global T-cell functionality. Since the approach involved analyzing T-cell function from fixed volumes of whole blood, the reduction in interferon production levels may reflect both a decrease in the functional capacity of individual T cells and a reduction in T-cell counts per unit volume. Previous studies have reported a numerical reduction in T-cell subsets after cardiac surgery with CPB. For instance, Tajima et al. and Akbas et al. observed significant declines in CD3+, CD4+, and CD8+ T cells in adult patients following cardiac surgery with CPB (Akbas et al., 2002; Tajima et al., 1993). This reduction may be attributed to T-cell consumption caused by increased immune activity due to blood-foreign material interactions, as well as hemodilution, which decreases the total number of T cells. Similarly, Yamaguchi et al. and Habermehl et al. reported significant decreases in T-cell subpopulations in children after cardiac surgery with CPB. Habermehl et al. suggested that this could result from leukocyte loss in the membrane-oxygenator or within organs, the use of leukocyte-depleted packed red cells, or a combination of these factors (Habermehl et al., 2003; Yamaguchi et al., 2000). Consistent with these findings, our results observed a significant postoperative decrease in CD3+ T-cell counts, with global T-cell functionality strongly correlating with CD3+ numbers, indicating that reduced T-cell subsets impair functionality. In addition to the reduction in cell numbers, cardiac surgery may also directly impact cellular immune function. Surgical stress is considered a key factor contributing to cellular immunosuppression (Ogawa et al., 2000). Hogan et al. reported that both physical and psychological surgical stress can increase the release of glucocorticoids, such as cortisol from the adrenal gland, which are known to suppress both T-lymphocyte proliferation and maturity (Hogan et al., 2011). Additionally, the use of anti-inflammatory medications, such as methylprednisolone during the operation, may also temporarily inhibit the T-cell immunity. Fortunately, both SARS-CoV-2 specific T-cell immunity and global T-cell functionality gradually recovered within approximately 1 month, indicating that the temporary postoperative T-cellular immune deficiency can be restored over time. In conclusion, considering the postoperative changes in humoral and cellular immunity, it could be inferred that postoperative convalescents may still maintain some protection against COVID-19 infection throughout the convalescent period.
In this study, it was observed that CHD children exhibited weaker global T-cell functionality prior to surgery compared to immunocompetent children. Pediatric CHD patients are generally of a younger age, and age is known to be associated with immune system development and function (Simon et al., 2015; Valiathan et al., 2016). In the subgroup analysis, children above 3 years old exhibited stronger T-cell functionality compared to those below 3 years old. Additionally, it should be noted that certain CHDs may cause immunodeficiency (Radford and Thong, 1988; Singampalli et al., 2021). Interestingly, when assessing the SARS-CoV-2-specific T-cellular response, no significant difference was observed between the two age groups. While prior studies have reported lower COVID-19 T-cellular responses in children compared to adults following infection (Cohen et al., 2021; Pierce et al., 2020), our study and several others have found similar levels of COVID-19 T-cellular response across different age groups of children (Tian et al., 2022; Tsang et al., 2021). These observations suggested that the age difference in children may affect the baseline level of global T-cellular response but not the induction level of specific T-cellular immunity.
This study has several potential limitations that should be acknowledged. First, the inconvenience of long-distance round-trip led to follow-up losses for many participants, resulting in a reduced sample size at the POM point. This reduction limits our ability to conduct a thorough analysis and make comparisons with earlier time points. Further, the donor used for the transfusion probably contained COVID-19 antibodies, which might interfere with assessing the real impact of surgery on preexisting antibodies. Additionally, the testing methods used in our study, including SARS-CoV-2-specific IgG, neutralizing antibody, and IGRA kits, may require further optimization for pediatric patients, although this limitation does not impact the validity of our main findings. Our analysis remains robust in comparing different groups across three time points to identify potential trends of each parameter. Lastly, due to the difficulty in collecting blood from healthy children, the control group in the present study consisted of relatively immunocompetent individuals. Future studies should include healthy child controls to verify these results.
Conclusions
Among pediatric CHD patients undergoing cardiac surgery, it was found that some preexisting specific antibodies were retained in the majority of pediatric CHD patients following surgery. Simultaneously, a transient decrease in SARS-CoV-2-specific T-cell immunity and global T-cell functionality was noted during the early postoperative period, with recovery occurring approximately 1 month after surgery. These findings demonstrate the impact of cardiac surgery on preexisting specific immunity and global T-cell immunity in CHD patients, providing valuable insights for postoperative care strategies in these patients.
Footnotes
Acknowledgments
The authors would like to thank the patients and their parents for their support and participation in this study.
Authors’ Contributions
Conceptualization: Y.P., L.M., A.F., F.B., Q.C., J.L., and Z.X. Methodology: Y.P., L.M., A.F., F.B., D.L., and C.G. Formal analysis and data curation: Y.P., L.M., J.L., and Z.X. Investigation: Y.P., A.Z., Y.C., and M.Z. Resources and writing—review and editing: A.F., F.B., J.L., and Z.X. Writing—original draft preparation: Y.P. and L.M. Visualization: L.M. Supervision: J.L. and Z.X. Project administration: J.L. and Z.X. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
L.M., A.F., F.B., and J.L. are bioMérieux employees. D.L. and C.G. are Suzhou Hybiome employees. The remaining authors declare no commercial or financial conflict of interest.
Funding Information
This research received no external funding.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.