
Abstract
Tick-borne viruses are an increasing global health concern due to their significant impact on humans and animals, as well as their expanding geographic distribution. Notable viruses in this group include the tick-borne encephalitis virus (TBEV), Crimean–Congo hemorrhagic fever virus (CCHFV), Heartland virus (HRTV), and Powassan virus (POWV). This review evaluates their geographic spread, clinical effects, diagnostic challenges, treatment options, and research gaps. These viruses are increasingly spreading due to climate change and shifting tick habitats. The TBEV is moving into new areas of Europe and Asia, while the CCHFV is advancing into the Balkans and Caucasus. The HRTV has become more common in the United States, and the POWV is emerging in new regions of North America. Symptoms can vary from mild fever to severe neurological and hemorrhagic conditions. Diagnostic difficulties stem from inconsistent test accuracy, and treatment options are scarce, with only a few vaccines available. Tick-borne viruses represent a significant and expanding health threat, given their diverse clinical outcomes and diagnostic difficulties. Developing more accurate and accessible diagnostic tools is critical for early identification and treatment. Additionally, creating effective vaccines will be essential to reducing the overall burden of these viruses. With the increasing spread of tick-borne viruses, enhanced surveillance, ongoing research efforts, and strategic public health interventions are necessary to effectively control their impact and prevent further outbreaks.
Introduction
Tick-borne diseases are a significant and expanding global health concern due to their widespread distribution and the severe impact they can have on human and animal health. These diseases are primarily transmitted by hard ticks from the Ixodidae family, which can host a diverse array of pathogens, including viruses, bacteria, and protozoa (CDC, 2021). Among these, tick-borne viruses (TBVs) are particularly problematic because they can cause severe, sometimes fatal illnesses (Shi et al., 2018). Notable examples of TBVs include tick-borne encephalitis virus (TBEV) (Stadler et al., 1997), Crimean–Congo hemorrhagic fever virus (CCHFV) (Sanchez et al., 2002), Heartland virus (HRTV) (McMullan et al., 2012), and Powassan virus (POWV) (Hinten et al., 2008; Brault et al., 2018).
Tick species can be broadly classified into three main groups based on their biological characteristics: hard ticks (Ixodidae), soft ticks (Argasidae), and nut grass ticks (Nuttalliellidae) (Nepveu-Traversy et al., 2024) (Fig. 1). Hard ticks, the most significant vectors of tick-borne diseases, are known for their robust, scutum-covered bodies and their ability to remain attached to hosts for extended periods while feeding. This family includes species such as Ixodes scapularis, the primary vector of Lyme disease, and Rhipicephalus sanguineus, which spreads diseases like ehrlichiosis and Rocky Mountain spotted fever. Soft ticks, in contrast, have a leathery, pliable body and generally feed for shorter periods, often transmitting pathogens like tick-borne relapsing fever (Shi et al., 2018). Finally, the Nuttalliellidae family is rare, with only a few known species that have a more limited impact on human and animal health.
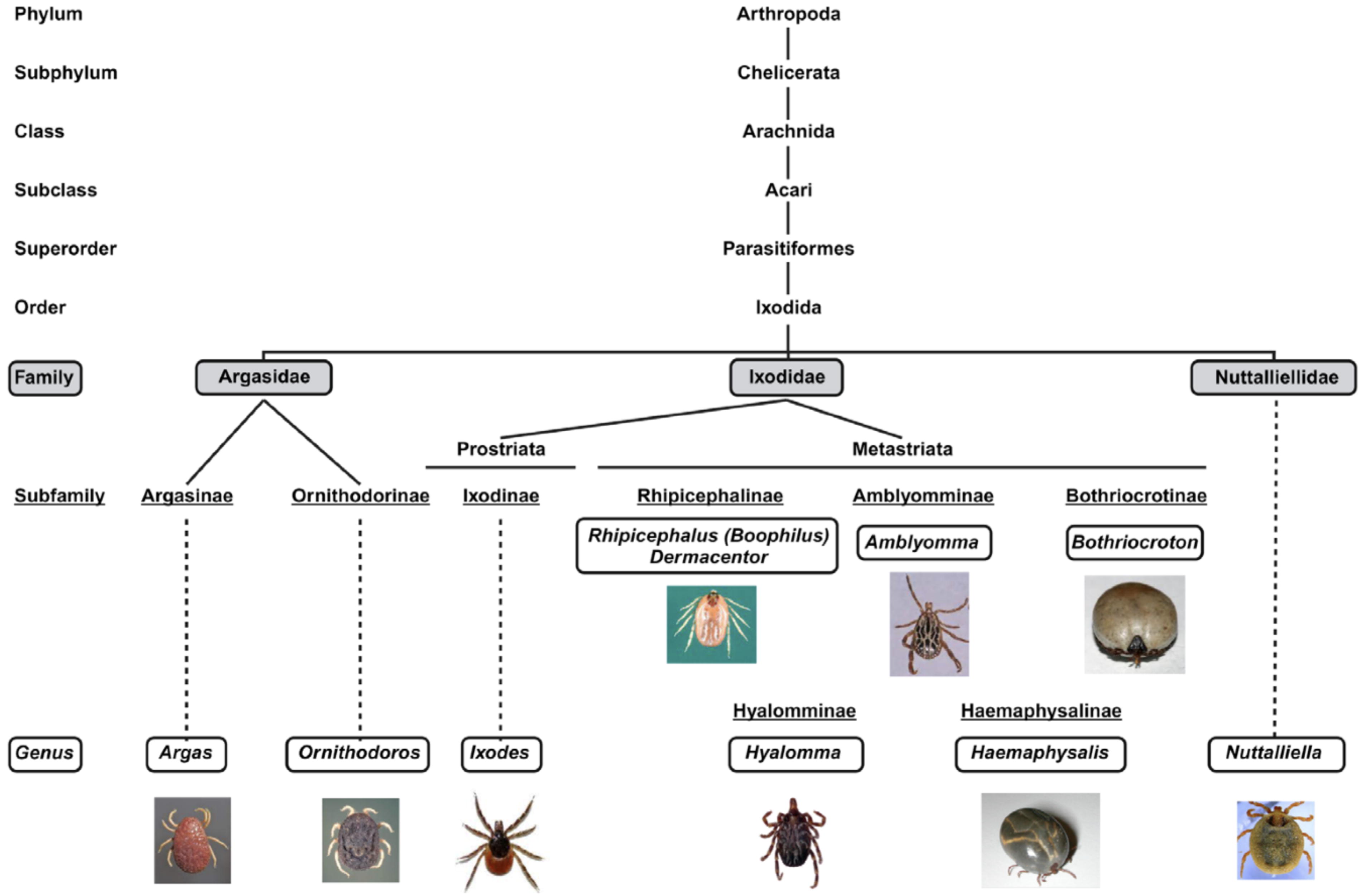
Diagram illustrating the taxonomy of ticks (NCBI taxonomy ID numbers: txid34601 [Argas], txid6937 [Ornithodoros], txid6944 [Ixodes], txid34630 [Rhipicephalus], txid34619 [Dermacentor], txid6942 [Amblyomma], txid189200 [Bothriocroton], txid34625 [Hyalomma], txid34622 [Haemaphysalis], and txid1029658 [Nuttalliella]) (Nepveu-Traversy et al., 2024).
The global significance of TBVs is highlighted by their diverse geographical distribution and their substantial impact on public health. For example, TBEV is endemic in parts of Europe and Asia, with its range expanding into new areas due to climate change and shifts in tick populations (Estrada-Peña et al., 2017; Nuttall, 2022; Tsoumani et al., 2023). Similarly, CCHFV, which is prevalent in Africa, the Middle East, and parts of Asia, has been linked to outbreaks with high mortality rates (Sanchez et al., 2006; Lippi et al., 2021). The geographic spread of these viruses underscores the importance of robust surveillance and public health strategies to address the growing risk (Lippi et al., 2021; Pulkkinen et al., 2022).
Understanding TBVs is critical for several reasons. These viruses can present with a broad spectrum of clinical symptoms, ranging from mild febrile illnesses to severe conditions such as encephalitis and hemorrhagic fever, which complicates diagnosis and treatment (Dai et al., 2018; CDC, 2021). Diagnostic challenges are prevalent due to symptom overlap with other diseases and variability in clinical presentation (Yean et al., 2024). Although some TBVs (Kovalev and Mukhacheva, 2017), like TBEV, have effective vaccines, many do not, highlighting the need for continued research into effective treatments and preventive measures (WHO, 2023). Moreover, the expanding geographic range of these viruses necessitates ongoing research and public health interventions to mitigate their impact (Lippi et al., 2021).
This systematic review aims to achieve several key objectives concerning TBVs. First, it seeks to evaluate the geographical distribution of these viruses, with a focus on identifying regions with high incidence rates and emerging areas of concern. Second, the review will examine the clinical impact of TBVs, analyzing their manifestations, severity, and outcomes, including symptom profiles and potential complications. Third, the review will identify diagnostic challenges, discussing the accuracy, availability, and limitations of current diagnostic methods for these infections. Additionally, it will review the treatment options available for tick-borne viral infections, summarizing current antiviral therapies, supportive care, and the status of vaccine development. Finally, the review will highlight research gaps, identifying areas where further studies are needed to improve understanding, diagnosis, treatment, and prevention of TBVs. By addressing these objectives, the review aims to provide a comprehensive, evidence-based overview to inform future research and public health strategies.
Overview of TBVs
TBVs can be classified into several families and genera, each associated with different clinical manifestations and geographic distributions. Major families of TBVs include Flaviviridae, Bunyaviridae, and Nairoviridae (Pustijanac et al., 2023) (Table 1).
Summary of Tick-Borne Viruses
The Flaviviridae family includes several important TBVs. Notable members are the TBEV and the Kyasanur forest disease virus (KFDV). TBEV is the causative agent of tick-borne encephalitis, which primarily affects the central nervous system and can lead to severe neurological complications (Stadler et al., 1997; Pustijanac et al., 2023). KFDV, on the other hand, is found in India and causes fever and hemorrhagic manifestations. This family is characterized by enveloped viruses with single-stranded RNA genomes (Pulkkinen et al., 2022; Pustijanac et al., 2023).
The Bunyaviridae family includes viruses such as the CCHFV and the Rift Valley fever virus (RVFV). CCHFV is known for causing severe hemorrhagic fever with high mortality rates, and it is endemic in parts of Africa, the Middle East, and Asia (Sanchez et al., 2002; Sanchez et al., 2006; Shi et al., 2018). RVFV, primarily affecting livestock, can also infect humans and cause febrile illness and hemorrhagic fever. Bunyaviruses are also enveloped, with segmented RNA genomes (Shi et al., 2018).
The Nairoviridae family includes the KFDV, which, as mentioned, is associated with severe febrile and hemorrhagic illnesses in India. Nairoviruses are characterized by their segmented RNA genomes and their ability to cause significant hemorrhagic fevers (Shi et al., 2018).
Geographic Distribution of TBVs
TBVs exhibit a varied geographic distribution depending on the virus type and geographical region (Table 1). This section evaluates the prevalence and geographic distribution of major TBVs, focusing on areas with high incidence and emerging regions of concern (Fig. 2).

Geographical distribution of primary tick vectors and tick-borne pathogens. Green numbers represent the tick vectors, violet numbers denote the tick-borne bacteria and protozoa, and orange numbers indicate tick-borne viruses (Nepveu-Traversy et al., 2024).
TBEV is a prominent tick-borne pathogen, predominantly found in Europe and Asia (Dai et al., 2018). The highest prevalence rates are reported in countries such as Austria, Estonia, Latvia, Lithuania, Poland, and Russia, where TBEV is endemic and contributes significantly to neurological disease burden (Kovalev and Mukhacheva, 2017; Pustijanac et al., 2023). Recent studies indicate an expansion of TBEV into new regions, including Scandinavia and parts of Central Europe, likely due to climate change and shifting tick populations (Pustijanac et al., 2023). In these areas, TBEV incidence has been rising, underscoring the need for enhanced surveillance and vaccination efforts.
CCHFV is predominantly found in Africa, the Middle East, and parts of Asia. High incidence rates are reported in countries such as Turkey, Iran, and parts of sub-Saharan Africa, where outbreaks of CCHFV have been documented with severe hemorrhagic symptoms and significant mortality (Shtanko et al., 2014; Eslava et al., 2024). Recent surveillance data reveal an increasing number of cases in new regions, including parts of the Balkans and the Caucasus, where the virus has recently been identified, signaling an expanding geographic range (Estrada and De Guzman, 2011; Eslava et al., 2024). This trend highlights the importance of improving diagnostic capabilities and public health responses in these emerging areas.
HRTV was first identified in the United States, specifically in Missouri and Tennessee. The prevalence of HRTV is relatively lower compared to TBEV and CCHFV but has been documented in several other states, including Kentucky and Arkansas (McMullan et al., 2012; Brault et al., 2018). HRTV is primarily reported in rural and forested areas, with an apparent expansion in its geographic range over the past decade. This expansion is attributed to changes in tick habitat and vector ecology, necessitating further research into the virus’s epidemiology and risk factors (Clarke et al., 2018; Brault et al., 2018).
POWV is primarily found in North America, particularly in the northeastern United States and parts of Canada. Recent data indicate an increasing incidence of POWV infections, with reports emerging from regions previously considered nonendemic, such as the Midwest and southern Canada (Hinten et al., 2008; Yang et al., 2022). The rise in POWV cases is linked to the spread of its primary tick vectors, such as Ixodes scapularis, and the expansion of their habitat due to changing environmental conditions (Anderson and Armstrong, 2012; Yang et al., 2022). This geographic expansion necessitates increased vigilance and preventive measures in newly affected areas.
Several regions are emerging as areas of concern due to the expanding geographic range of TBVs. Climate change, shifts in tick populations, and changes in land use are contributing to the spread of these viruses into new areas. For instance, the expansion of TBEV into Scandinavia and Central Europe, the detection of CCHFV in the Balkans and Caucasus, and the rise in POWV cases in previously unaffected areas of North America all highlight the need for adaptive surveillance and control strategies (Pesko et al., 2010).
The Interplay of Climate, Hosts, and Land Use in Tick Population Dynamics
The growing concern over TBVs and their expanding geographic range can be largely attributed to the complex interplay of environmental factors, particularly climate change, shifts in tick populations, and changes in land use (Lippi et al., 2021; Perumalsamy et al., 2024) (Fig. 3). The current evidence shows that these factors not only affect the distribution of ticks but also alter the dynamics of TBV transmission, making it crucial to examine the ecology of ticks more closely (Eslava et al., 2024). This is especially important in understanding the mechanisms behind the spread of these viruses and forecasting potential outbreaks.
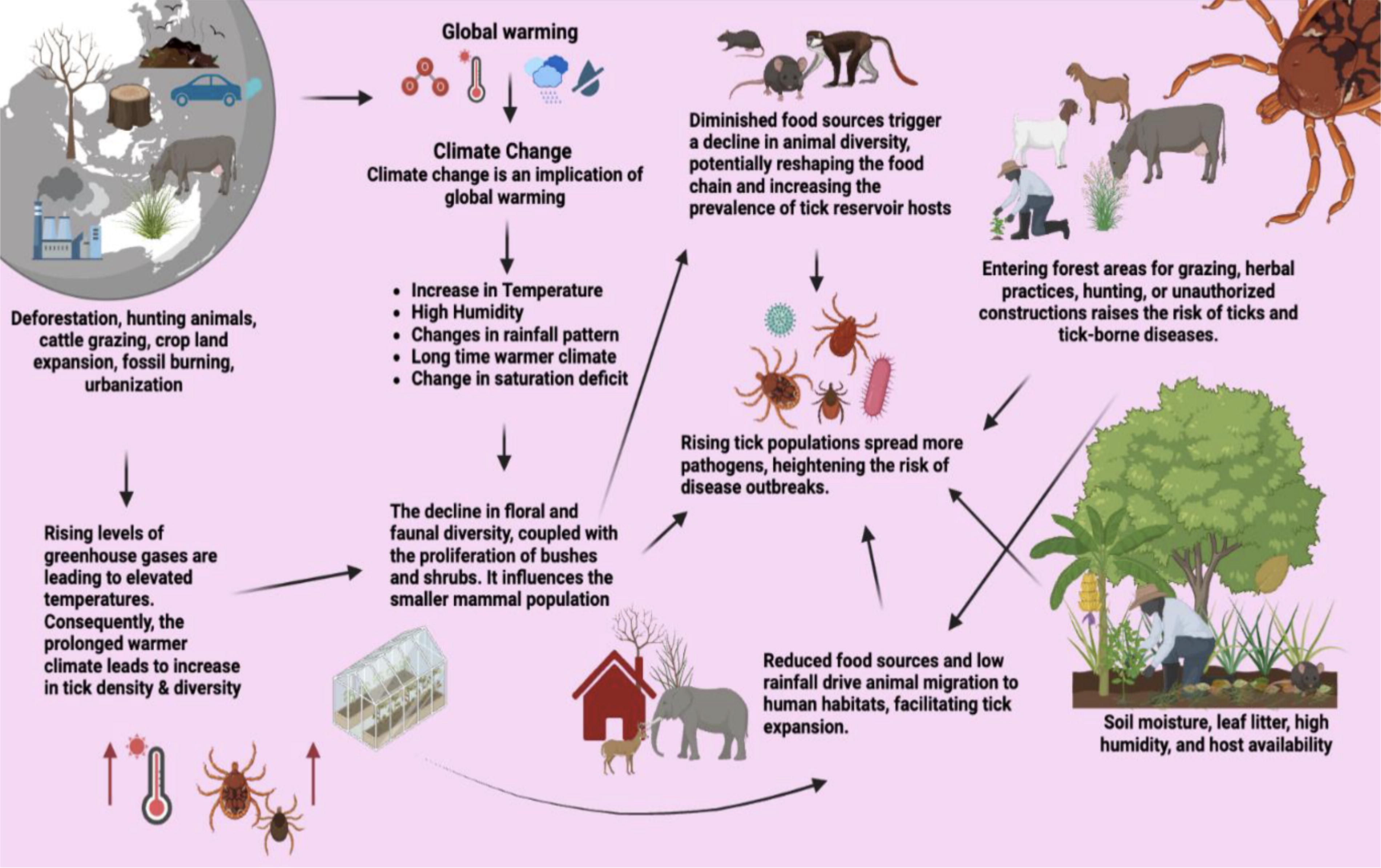
A schematic representation highlights the geographical expansion of ticks, underscoring the significant role played by global warming and climate change in facilitating this spread. It illustrates the impact of climate change on tick habitats and distribution, emphasizing the connection between the loss of floral and faunal diversity and the subsequent increase in tick populations. The figure elucidates the interrelationship between climate change and human activities, emphasizing how anthropogenic factors contribute to the proliferation of ticks. This visual representation offers a comprehensive overview of the intricate dynamics among environmental changes, human activities, and the escalating prevalence of ticks in various regions.
Climate Change and TBVs
Climate change has a profound impact on the life cycles of ticks and the pathogens they carry. Warmer temperatures, fluctuating precipitation patterns, and the lengthening of favorable seasons for tick activity are contributing to the expansion of tick populations into regions that were once inhospitable (Tsoumani et al., 2023). As temperatures rise, areas that were previously too cold to support ticks, such as higher latitudes or altitudes, are becoming more hospitable (Lippi et al., 2021). This is particularly evident in parts of Northern Europe and North America, where tick species such as Ixodes scapularis (which transmits Lyme disease) and Ixodes ricinus (responsible for diseases like tick-borne encephalitis) are moving into new territories. As ticks spread into these new areas, the risk of TBV transmission increases. In addition to temperature, changing precipitation patterns are affecting the moisture levels in ecosystems, influencing tick survival rates and their ability to reproduce (Tsoumani et al., 2023).
These environmental changes are not only driving the geographic spread of ticks but also altering the timing of their activity. Tick populations are becoming more abundant and active for longer periods throughout the year, increasing the likelihood of human exposure (Nuttall, 2022). In particular, climate-induced shifts in the seasonal patterns of ticks can result in an extended period of virus circulation, heightening the risk of outbreaks. As warmer and wetter conditions favor tick survival, areas previously considered low risk for TBVs may now see an increase in cases, prompting the need for better predictive models to track these trends (Madison-Antenucci et al., 2020).
Tick Ecology and Population Cycles
The ecology of ticks is a critical area of research that has seen substantial development in North America and Europe. Researchers have focused extensively on how environmental factors, such as temperature, humidity, and habitat availability, shape tick populations and influence the timing of their life cycles (Lippi et al., 2021). For instance, studies have shown that different tick species have varying temperature thresholds for survival and reproduction, which can significantly affect the abundance and distribution of ticks in any given region. In addition, the availability of hosts (such as small mammals, birds, and larger wildlife) plays a pivotal role in tick population dynamics (Amicizia et al., 2013). When land use changes—such as deforestation or urbanization—disrupt these ecosystems, the interactions between ticks, their hosts, and the viruses they carry can be altered in unpredictable ways.
Climate change is exacerbating these effects, and one of the most concerning outcomes is the disruption of established tick population cycles (CDC, 2021). For example, in some regions, the arrival of warmer temperatures may cause ticks to emerge earlier in the season and stay active longer into the fall, allowing for extended periods of viral circulation (Brault et al., 2018). This, in turn, increases the chances of humans and animals coming into contact with infected ticks, facilitating the transmission of diseases such as Lyme disease, babesiosis, and tick-borne encephalitis (Madison-Antenucci et al., 2020). The disruption of natural tick cycles may also result in the overlap of multiple tick generations in a single season, leading to an increased risk of viral amplification and transmission (Madison-Antenucci et al., 2020).
The Role of Land Use and Hosts in Viral Circulation
Changes in land use, including urbanization and the expansion of agricultural areas, are altering tick habitats in ways that further influence the transmission of TBVs. As human populations encroach on previously wild habitats, human-tick interactions increase, making suburban and urban areas hotspots for tick-borne diseases (Brault et al., 2018). Additionally, land use changes can affect the abundance and diversity of wildlife species that serve as hosts for ticks. For instance, a rise in populations of certain animals, such as deer or rodents, can provide ticks with a greater number of hosts, facilitating the spread of viruses in the tick population (Eslava et al., 2024). This host-driven effect is particularly important when considering the role of large vertebrates in sustaining tick populations and enhancing the circulation of viruses in both urban and sylvatic (wild) cycles (Yean et al., 2024).
In rural or sylvatic cycles, where interactions between wild animals and ticks are more common, climate change and land use shifts can similarly impact the dynamics of TBV circulation. For example, forest fragmentation can create edges that are more conducive to tick survival while also increasing human exposure to tick habitats. Understanding how land use changes affect the abundance and distribution of hosts, along with how this interacts with tick population dynamics, is crucial for predicting the emergence and spread of TBVs (Estrada-Peña et al., 2017).
The Need for Better Tracking and Predictive Models
Given the increasing threat posed by the spread of TBVs, it is critical to track tick populations and their associated viruses more carefully. Surveillance systems that monitor tick populations, their hosts, and the viral pathogens they carry are vital in identifying emerging risks and preventing outbreaks (Takahashi et al., 2014). This is particularly important in regions where TBVs are emerging or have yet to be studied in depth, such as in parts of Africa, the Middle East, and Asia (Eslava et al., 2024). In these regions, tick populations and the viruses they carry may follow different cycles, influenced by distinct climatic and ecological factors. For instance, the Hyalomma ticks in the Middle East are vectors for Crimean–Congo hemorrhagic fever, and changes in land use and climate could influence the spread of this disease across borders. Similarly, tick-borne diseases in parts of sub-Saharan Africa, such as African tick-bite fever, may be affected by climate changes that alter the range and activity of the ticks involved (Shi et al., 2018).
Incorporating information about tick population cycles in these regions and understanding their interactions with climate, land use, and hosts will be crucial for improving the prediction of TBV outbreaks. Developing comprehensive models that account for the varying factors influencing tick populations, viral circulation, and disease transmission will enhance the ability of public health systems to respond proactively to emerging threats.
Clinical Consequences of TBVs
The clinical impact of TBVs varies significantly depending on the specific virus and the affected individual. Each virus presents a distinct symptom profile, with manifestations ranging from mild flu-like symptoms to severe, life-threatening conditions.
TBEV commonly causes a biphasic illness (Fig. 4). The initial phase typically includes flu-like symptoms such as fever, headache, muscle aches, and fatigue, which often resolve within a week (De Graaf et al., 2016; Pustijanac et al., 2023). This is followed by a second phase characterized by severe neurological symptoms, including meningitis, encephalitis, and myelitis. The severity of neurological symptoms can range from mild cognitive impairment to severe motor dysfunction and coma. Complications can be profound, with long-term sequelae including persistent cognitive deficits and motor disabilities in a significant proportion of survivors (Füzik et al., 2018; Pustijanac et al., 2023).

Overview of the classical biphasic disease pattern of human TBEV infection. TBEV, tick-borne encephalitis virus.
CCHFV is associated with severe hemorrhagic fever, presenting with high fever, headache, myalgia, and abdominal pain. As the disease progresses, patients may develop bleeding manifestations such as petechiae, ecchymosis, and gastrointestinal bleeding, which can lead to severe hemorrhagic shock (Spengler et al., 2016; Eslava et al. 2024). Mortality rates for CCHFV can be high, with fatality rates ranging from 10% to 40%, depending on the outbreak and the patient’s health status. Survivors may experience long-term effects, including chronic fatigue and joint pain (Palomar et al., 2017).
HRTV typically presents with acute febrile illness, characterized by fever, fatigue, and myalgia. More severe cases can involve gastrointestinal symptoms such as nausea, vomiting, and diarrhea, along with symptoms of thrombocytopenia and leukopenia (Takahashi et al., 2014; Brault et al., 2018). Although the overall mortality rate for HRTV is relatively low, the disease can result in prolonged recovery times and significant impacts on quality of life. Long-term effects may include persistent fatigue and joint pain, with some patients reporting ongoing health issues months after infection (Kim et al., 2013; Brault et al., 2018).
POWV is known for causing neurological disease, which can manifest as encephalitis or meningoencephalitis. Initial symptoms often include fever, headache, and nausea, which can rapidly progress to severe neurological symptoms such as confusion, seizures, and motor impairment (Pesko et al., 2010; Yang et al., 2022). The disease has a higher incidence of long-term complications compared to other TBVs, with many survivors experiencing significant residual effects such as cognitive deficits, motor dysfunction, and chronic neurological symptoms. The mortality rate for POWV is relatively low but can result in severe long-term outcomes (Anderson and Armstrong, 2012; Yang et al., 2022).
Complications associated with TBVs are often severe and can result in significant long-term health issues. For instance, TBEV can lead to chronic neurological problems, including cognitive impairments and motor dysfunction, which can affect daily living and quality of life (El Khoury et al., 2013; Pustijanac et al., 2023). CCHFV can cause severe hemorrhagic manifestations with long-lasting effects such as chronic joint pain and fatigue, which can significantly impact a patient’s quality of life even after recovery (Eslava et al., 2024). HRTV and POWV infections can result in prolonged recovery periods and chronic health issues, including persistent fatigue, joint pain, and neurological sequelae (Brault et al., 2018; Yang et al., 2022).
The clinical impact of TBVs is substantial, with manifestations ranging from mild to severe and complications that can lead to long-term health issues (Fig. 5). The severity and outcomes of these infections highlight the need for effective prevention, prompt diagnosis, and management strategies to mitigate their impact on affected individuals.
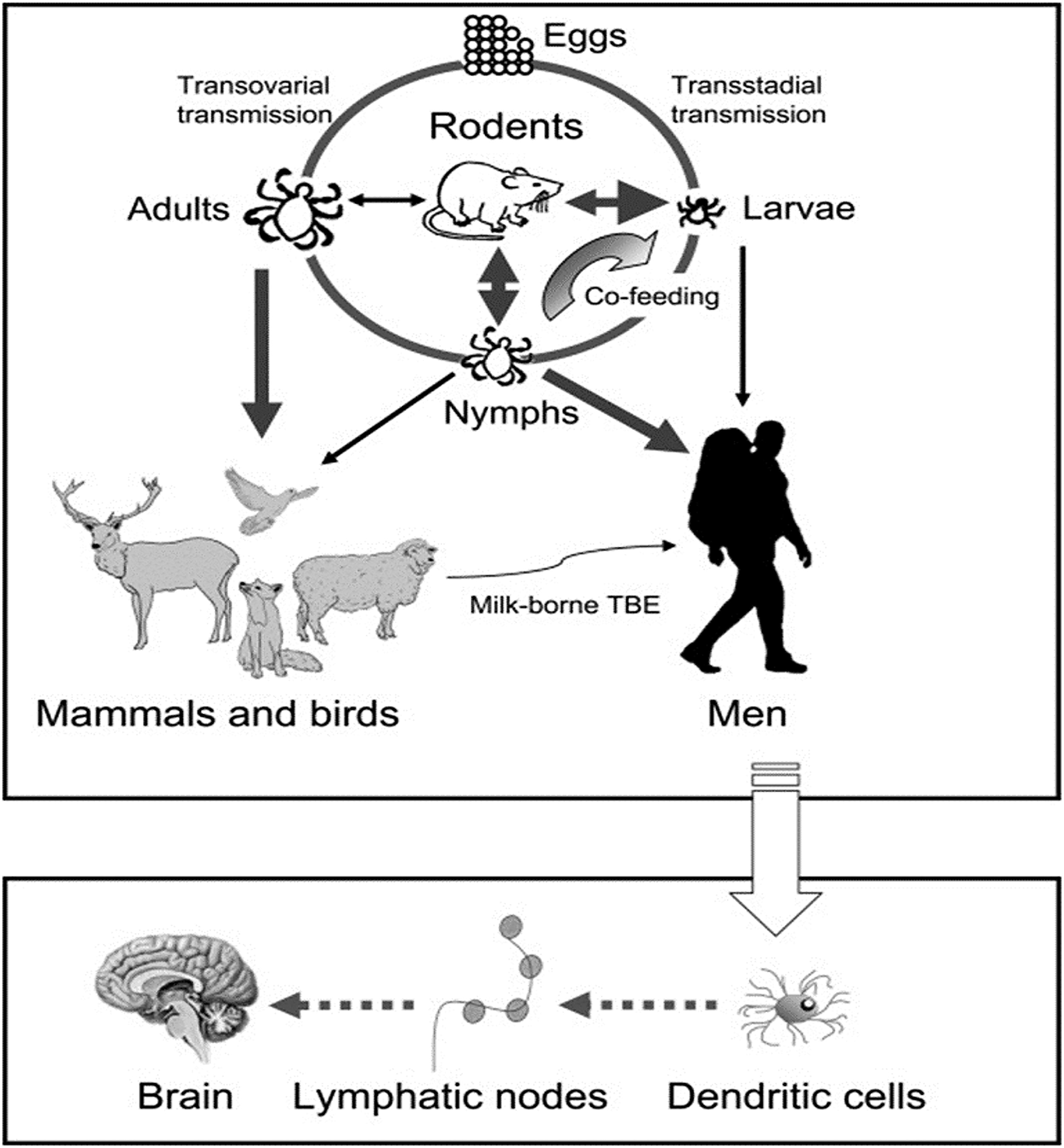
Transmission and clinical consequences of tick-borne encephalitis virus.
Diagnostic Approaches and Challenges in Tick-Borne Viral Infections
The accurate diagnosis of TBVs is critical for effective patient management and treatment, yet it is fraught with challenges due to the diversity of these viruses and the limitations of current diagnostic methods.
TBEV is typically diagnosed through serological and molecular methods. Serological tests, including enzyme-linked immunosorbent assays (ELISA) and indirect immunofluorescence assays (IFA), detect TBEV-specific antibodies (IgM and IgG) in the blood. These tests are valuable for diagnosing TBEV, particularly in the later stages of the disease when antibody levels are elevated (Holmgren and Forsgren, 1990; Yean et al., 2024). However, their accuracy can be compromised early in the infection when antibodies are not yet detectable, leading to potential false negatives. On the other hand, polymerase chain reaction (PCR) assays can detect TBEV RNA in cerebrospinal fluid (CSF) or blood, offering high sensitivity and specificity (Haglund et al., 2003; Yean et al., 2024). Despite this, PCR can be limited by the timing of sample collection and the low concentration of viral RNA in some cases.
For CCHFV, serological tests detecting specific IgM and IgG antibodies are commonly used. These tests, performed using ELISA, are effective but can sometimes yield false positives due to cross-reactivity with other flaviviruses (Mazzola and Kelly-Cirino, 2019). PCR methods, including reverse-transcription PCR (RT-PCR), can detect CCHFV RNA in blood, CSF, and tissue samples, providing high sensitivity and specificity (Zivcec et al., 2017; Mazzola and Kelly-Cirino, 2019). However, PCR assays require specialized equipment and expertise, and the accuracy can be influenced by the timing of the test relative to the infection stage (Koehler et al., 2018).
HRTV diagnosis relies on serological methods, such as ELISA, to detect specific antibodies. While these tests are available, they may not be widely accessible and can be limited by cross-reactivity with other arboviruses (Madison-Antenucci et al., 2020; Basile et al., 2021). PCR assays are used to detect HRTV RNA in blood and other bodily fluids, offering high sensitivity. However, the lack of standardized PCR tests and the virus’s relatively recent discovery can pose challenges in diagnosing HRTV effectively (Savage et al., 2013; Yean et al., 2024). Additionally, early-stage infections with low viral loads can complicate accurate diagnosis.
POWV is diagnosed through serological tests that detect antibodies in serum or CSF using ELISA or IFA (Dupuis et al., 2013). These methods are useful for confirming infection but can be impacted by cross-reactivity with other flaviviruses, leading to potential diagnostic confusion (Nofchissey et al., 2013; Yang et al., 2022). PCR techniques can also be employed to detect POWV RNA in CSF and blood, providing high sensitivity. However, the effectiveness of PCR can be limited by the timing of the sample collection and the variability in viral load (Yean et al., 2024).
The availability and accessibility of diagnostic tests for TBVs vary significantly across different regions. In areas where these viruses are endemic, diagnostic facilities are often well-equipped, and tests are more readily available. Conversely, in regions where TBVs are emerging or less common, there may be limited access to specialized diagnostic tests. This disparity can lead to delays in diagnosis and challenges in managing outbreaks effectively (El Khoury et al., 2013; Mazzola and Kelly-Cirino, 2019).
Treatment and Management Strategies for Tick-Borne Viral Infections
Treatment options for tick-borne viral infections are currently limited, with most management strategies focusing on supportive care rather than antiviral therapies. For TBEV, there are no specific antiviral drugs available. The primary approach remains supportive care, which includes managing symptoms and providing supportive measures (Amicizia et al., 2013; Pustijanac et al., 2023). Ribavirin, an antiviral drug effective against some flaviviruses, has not shown substantial efficacy against TBEV, limiting its utility for this infection (Andreotti, 2006; Pustijanac et al., 2023).
Similarly, for CCHFV, ribavirin is the most commonly used antiviral medication (Zivcec et al., 2018). Clinical studies suggest that ribavirin can reduce mortality and improve outcomes if administered early in the course of the illness (Dowall et al., 2017; Eslava et al., 2024). Despite its potential benefits, ribavirin’s use is often constrained by its side effects and the need for timely intervention, which may not always be feasible.
In the case of HRTV, no specific antiviral treatments are available. The management of HRTV infections relies on supportive care to address symptoms and provide hydration (Brault et al., 2018; Fujii et al., 2022). As with other TBVs, research into effective antiviral therapies for HRTV is ongoing, but no targeted treatments have been established (Rodrigues et al., 2021).
For POWV, there are no approved antiviral drugs. Treatment for POWV infections is also supportive, focusing on alleviating symptoms and addressing complications that arise (Vanblargan et al., 2021; Yang et al., 2022). This supportive approach is consistent with the management of other tick-borne viral infections where specific antiviral options are lacking.
Supportive care is a critical component in the management of tick-borne viral infections. This care includes ensuring proper hydration and maintaining electrolyte balance, which is crucial for managing the often severe symptoms associated with these infections (Yang et al., 2022). Symptomatic treatment involves the use of analgesics and antipyretics to manage fever and pain, with additional interventions such as antiepileptic drugs being necessary for severe neurological involvement (Yang et al., 2022).
In severe cases, particularly those involving encephalitis or hemorrhagic manifestations, intensive monitoring and care may be required. This can include the provision of ventilatory support, renal replacement therapy, and other critical care measures as needed to manage the complications associated with these infections (Brault et al., 2018).
Emerging therapies for tick-borne viral infections include novel approaches such as monoclonal antibodies and small-molecule antivirals (Tsuruta et al., 2018). Research into monoclonal antibodies aims to develop targeted treatments that neutralize the virus directly. These therapies have shown promise in preclinical studies but are not yet available for clinical use (Pantaleo et al., 2022; Pustijanac et al., 2023). Similarly, small-molecule antivirals, which target viral enzymes or replication processes, are under investigation. These potential treatments could offer new therapeutic options in the future, but as of now, they remain in the experimental phase (Chen et al., 2015; Pustijanac et al., 2023).
Vaccination is a key preventive strategy for tick-borne viral infections. For TBEV, several effective vaccines are available in Europe and parts of Asia (Rumyantsev et al., 2006). These vaccines have proven effective in significantly reducing the incidence of TBEV infection and are recommended for individuals living in or traveling to endemic areas (Schmaljohn et al., 1997; Eslava et al., 2024).
Currently, there is no licensed vaccine for CCHFV, although vaccine development is ongoing (Fig. 6). Several candidate vaccines are in various stages of preclinical and clinical development, but none have yet been approved for widespread use (Tipu, 2016; Dowall et al., 2017).

Emerging therapies for tick-borne viral infections include novel approaches such as monoclonal antibodies and small-molecule antivirals.
No vaccines are available for HRTV or POWV. Research into vaccine development for these viruses is still in the early stages, with no licensed vaccines currently available (Choi et al., 2020; Brault et al., 2018).
Preventive measures for tick-borne viral infections include personal protection strategies such as using insect repellents containing DEET, wearing long-sleeved clothing, and performing tick checks after outdoor activities (Taylor et al., 2021; Pustijanac et al., 2023). Environmental management, including reducing tick habitats and maintaining clear areas around residential properties, can also help minimize the risk of tick bites (Rodrigues et al., 2021; Tsoumani et al., 2023). Public education on tick-borne diseases, their prevention, and early symptoms is essential for reducing the incidence of these infections and ensuring prompt medical attention when needed (WHO, 2023).
Research Gaps in the Study of TBVs
One significant research gap in the field of TBVs is the detailed understanding of their pathogenesis. While there is a general understanding of the clinical manifestations of these infections, the molecular and cellular mechanisms by which these viruses cause disease remain poorly elucidated (Amicizia et al., 2013). Research needs to focus on the specific interactions between TBVs and host cells, including how viral proteins facilitate immune evasion and tissue damage (Zivcec et al., 2018). For instance, uncovering the roles of particular viral proteins in disrupting host immune responses could provide new targets for antiviral therapies (Shi et al., 2018).
In addition, the evolving nature of TBVs due to environmental changes and their impact on viral evolution is another critical area needing further exploration (De Graaf et al., 2016). With climate change and habitat alterations potentially leading to new viral strains, there is a need for longitudinal studies that track genetic variations in TBVs. Such research could help predict future outbreaks and assess how these changes affect viral transmission, virulence, and host interactions (Füzik et al., 2018; Nuttall, 2022; Tsoumani et al., 2023).
Current diagnostic methods for TBVs, such as serological tests and PCR, have notable limitations, including issues with accuracy and accessibility. One pressing gap is the development of rapid, point-of-care diagnostic tests that are both highly sensitive and specific (Holmgren and Forsgren, 1990). Such tests would greatly enhance the ability to diagnose tick-borne viral infections promptly, particularly in regions with limited healthcare resources (Haglund et al., 2003). Research should focus on creating diagnostic platforms that can deliver accurate results quickly, making them more widely available (Mazzola and Kelly-Cirino, 2019).
Another challenge is overcoming cross-reactivity and false positives associated with existing diagnostic assays. Serological tests, for instance, often suffer from cross-reactivity with other viruses, which can lead to inaccurate diagnoses (Mazzola and Kelly-Cirino, 2019). There is a need for improved diagnostic assays that minimize these issues, potentially through the development of more specific tests or algorithms that incorporate multiple testing modalities (Koehler et al., 2018; Shi et al., 2018).
The lack of specific antiviral treatments for many TBVs represents a significant research gap (Dowall et al., 2017). While some antiviral drugs, such as ribavirin, have shown effectiveness against certain viruses, no approved antiviral therapies exist for many tick-borne infections. Research should prioritize the discovery and development of new antiviral agents that target the specific mechanisms of these viruses (Rodrigues et al., 2021). High-throughput screening for antiviral compounds and the development of targeted therapies based on viral molecular biology could lead to new treatment options (WHO, 2023).
Emerging therapies, such as monoclonal antibodies and small-molecule antivirals, also require further investigation (Vanblargan et al., 2021). Although these therapies hold potential, they need rigorous clinical testing to establish their safety and efficacy. Well-designed clinical trials are essential to evaluate these new therapies, optimize treatment regimens, and assess long-term outcomes (Andreotti, 2006; WHO, 2023).
Vaccine development for TBVs is another critical area needing attention. Effective vaccines exist for some TBVs like TBEV (Zivcec et al., 2018), but there is a significant gap for other viruses such as CCHFV, HRTV, and POWV. Research should focus on developing vaccines for these viruses, identifying suitable antigens, adjuvants, and delivery methods. Additionally, understanding vaccine-induced immunity, including the duration of protection and potential for cross-protection, is crucial for improving preventive strategies (Lippi et al., 2021; Yang et al., 2022).
Preventive measures beyond vaccination also need evaluation. Research should assess the effectiveness of various strategies, including environmental management and public education campaigns, in reducing tick-borne virus incidence (Yang et al., 2022). This includes evaluating tick control programs, the efficacy of personal protective measures, and the integration of educational efforts into public health strategies (Lippi et al., 2021).
Discussion
The prevalence and geographic distribution of TBVs present a complex and evolving picture. TBEV, for example, remains highly endemic in specific regions of Europe and Asia, aligning with areas where tick populations are dense and climatic conditions are favorable for tick survival (Dai et al., 2018; Yean et al., 2024). Recent studies highlight a worrying trend of TBEV spreading into new geographic areas previously considered low risk, driven by factors such as climate change and shifting land use patterns (Kovalev and Mukhacheva, 2017; Yean et al., 2024). This suggests a potential increase in incidence rates and a need for enhanced surveillance in emerging regions.
CCHFV exhibits high prevalence in Africa, the Middle East, and parts of Asia, with its distribution closely linked to tick habitats and agricultural practices (Shtanko et al., 2014; Eslava et al., 2024). However, as human activities and climatic conditions evolve, there is an increasing risk of CCHFV spreading to new areas. This geographic expansion underscores the importance of ongoing monitoring and preventive measures to address potential outbreaks in previously unaffected regions (Estrada and De Guzman, 2011).
In the United States, viruses like HRTV and POWV are emerging concerns. HRTV has been reported in the Midwest, while POWV is increasingly noted in the northeastern regions (McMullan et al., 2012; Brault et al., 2018). Despite the lower prevalence compared to TBEV and CCHFV, the emergence of these viruses indicates a need for targeted public health strategies and increased awareness in these areas. Comprehensive surveillance and research are essential to map out the full extent of these viruses’ geographic distribution and to identify new at-risk regions (Clarke et al., 2018).
The clinical impact of TBVs varies widely, reflecting their diverse pathogenic mechanisms. TBEV can lead to a spectrum of neurological outcomes, ranging from mild symptoms to severe encephalitis, with potential long-term effects such as cognitive deficits and motor impairment (De Graaf et al., 2016; Yean et al., 2024). The variability in clinical severity highlights the need for a nuanced understanding of the virus’s impact on different populations and the importance of early intervention to mitigate severe outcomes (Füzik et al., 2018).
CCHFV is associated with a high mortality rate, particularly due to its potential to cause severe hemorrhagic manifestations and multiorgan failure (Spengler et al., 2016; Eslava et al., 2024). The severity of CCHFV infections often correlates with delayed diagnosis and limited availability of supportive care, emphasizing the need for improved clinical management and timely medical intervention to improve patient outcomes (Palomar et al., 2017).
HRTV and POWV also present significant clinical challenges (Pesko et al., 2010; Takahashi et al., 2014). HRTV can cause a range of symptoms from mild fever to severe multiorgan dysfunction (Kim et al., 2013).
POWV is known for its potential to cause encephalitis with serious long-term neurological consequences (Brault et al., 2018). The diversity in symptom profiles and disease outcomes underscores the necessity for tailored diagnostic and treatment approaches, as well as continued research into the long-term effects of these infections (Anderson and Armstrong, 2012).
Diagnostic challenges for TBVs are multifaceted, involving issues of accuracy, accessibility, and timeliness. Serological tests, while valuable, often suffer from cross-reactivity with other viruses, leading to false positives and complicating accurate diagnosis (Holmgren and Forsgren, 1990; Mazzola and Kelly-Cirino, 2019). This issue highlights the need for more specific diagnostic assays and improved algorithms that can distinguish between different tick-borne pathogens.
PCR-based methods offer greater specificity but are limited by the timing of sample collection and the presence of the virus in the body (Zivcec et al., 2017; Mazzola and Kelly-Cirino, 2019). There is an urgent need for rapid, point-of-care diagnostic tests that can provide accurate results quickly. Such advancements would significantly enhance the ability to diagnose tick-borne viral infections early, allowing for more effective treatment and potentially reducing the risk of severe disease outcomes (Haglund et al., 2003).
Integrating new technologies, such as multiplex assays and advancements in bioinformatics, could improve diagnostic accuracy and efficiency (Savage et al., 2013). These tools would enable the simultaneous detection of multiple TBVs, facilitating a more comprehensive diagnostic approach (Mazzola and Kelly-Cirino, 2019; Basile et al., 2021).
The current treatment landscape for tick-borne viral infections is limited, with most infections managed through supportive care rather than specific antiviral therapies. For instance, while ribavirin has shown some efficacy against CCHFV (Andreotti, 2006), there are no widely approved antiviral drugs for many other TBVs (CDC, 2021). This gap underscores the need for ongoing research into new antiviral agents that target specific viral mechanisms.
Emerging therapies, such as monoclonal antibodies and small-molecule antivirals, hold promise but require further clinical validation (Zivcec et al., 2018; WHO, 2023). These therapies could offer more targeted treatment options and improve patient outcomes, but rigorous clinical trials are necessary to establish their safety and effectiveness.
Vaccination is a key preventive strategy for certain TBVs, such as TBEV, for which effective vaccines are available in some regions (WHO, 2023). However, there is a notable gap in vaccine availability for other TBVs, such as CCHFV, HRTV, and POWV (Spengler et al., 2016; Palomar et al., 2017; Takahashi et al., 2014; Kim et al., 2013). Research into vaccine development for these viruses is crucial for preventing future outbreaks and reducing the overall burden of disease.
Beyond vaccination, other preventive measures such as tick control programs and public education campaigns play an essential role in reducing tick-borne virus incidence (CDC, 2021). Evaluating the effectiveness of these measures and integrating them into public health strategies will be vital for controlling the spread of TBVs.
Conclusion and Recommendations
To effectively manage and mitigate the impact of TBVs, a multifaceted approach is essential. Enhanced global surveillance and monitoring are crucial to tracking virus prevalence and geographic spread. Developing rapid, accurate diagnostic tools will facilitate timely detection and treatment. Advancements in antiviral therapies and vaccines are needed to improve patient outcomes and prevent infections. Additionally, implementing comprehensive preventive measures and strengthening research collaborations will support the ongoing fight against these emerging threats. Addressing these areas will be key to reducing the burden of tick-borne diseases and protecting public health.
Footnotes
Author’s Contributions
The author was responsible for all aspects of the research, including conceptualization, methodology, data collection, analysis, and manuscript preparation.
Author Disclosure Statement
In this review, the author declares no competing interests, indicating they have no affiliations or financial involvement that could potentially sway their findings.
Funding Information
No funding was received for this article.