
Abstract
Objective:
Lower-extremity diabetic ulcers (LEDUs) affect more than 500,000 U.S. Medicare beneficiaries each year. Dehydrated human amnionic and chorionic allografts (DHACAs) are clinically effective complements to standard of care (SoC; e.g., surgical debridement, offloading, infection, and moisture control) when treating LEDUs. However, Medicare and commercial payer coverage have restricted access to DHACAs. Our objective was to compare the effectiveness of DHACAs versus SoC among Medicare beneficiaries with LEDUs for reduction of adverse outcomes such as mortality, recurrency, and major amputation.
Approach:
We analyzed a retrospective cohort of U.S. Medicare claims for LEDUs between 2018 and 2022. LEDU claims were collapsed into episodes of care (EOC). Frequency distribution of characteristics was compared using univariate and bivariate statistics. Zero-inflated binomial regression with 1:1 nearest-neighbor propensity score matching evaluated six main outcome measures: mortality; wound recurrence; major amputation; minor amputation; emergency department (ED) utilization; and readmission.
Results:
There were 25,760 Medicare EOCs between 2018 and 2022 representing 12,880 matched samples in the DHACA and SoC cohorts. DHACAs were associated with a 20% reduction in 30-day mortality (95% confidence interval [CI]:10%, 29%), 28% reduction in risk of major amputation (95% CI: 19%, 36%), 9% reduction in ED utilization (95% CI: 3%,14%), and 8% reduction in 30-day readmission (95% CI: 2%, 13%). DHACAs were noninferior for minor amputation rates and wound recurrence compared to SoC cohort.
Conclusion:
Beneficiaries with LEDUs benefit significantly from DHACAs on multiple outcomes, including a lower risk of mortality. Providers should examine the appropriateness of DHACAs for patients with LEDU as part of wound management. Medicare and commercial payers should consider improved outcomes when defining coverage policies that restrict access to DHACAs given the observed benefits.
Keywords
INTRODUCTION
Lower-extremity diabetic ulcers (LEDUs) are the cause of significant morbidity, mortality, and health system costs to patients age 65 and older in the U.S. Medicare population. 1 The annual incidence of LEDUs grew from 406,000 to 507,000 (+24.9%) among Medicare beneficiaries between 2014 and 2019. 1 In 2019, total Medicare spending for LEDUs and associated infections exceeded $21.5 billion in direct costs. 1 Most of this expenditure could be attributed to Medicare fee-for-service costs related to outpatient services for recurring wound management. 2
William V. Padula, PhD

Efficient management of these wounds is therefore important to reduce medical costs and minimize long-term consequences associated with chronic wounds. For instance, LEDUs alone are associated with a 5-year mortality rate of 30.5%, and this jumps to between 46.2% and 56.6% for patients who undergo a minor or major amputation, respectively.3–5 Established standard of care (SoC) for these chronic wounds including sharp debridement, infection and moisture control, compression therapy, and offloading can improve health outcomes when practiced on a weekly basis.6–8 While these practices are considered efficacious and cost-effective, they may not reduce the risk of important patient consequences such as wound recurrence, amputation, and mortality. 9
Cellular and tissue products (CTPs), including dehydrated human amnionic and chorionic allografts (DHACAs), are wound coverage materials that can be used to complement SoC and improve healing of chronic wounds “to prevent the introduction, transmission, and spread of communicable diseases.”10,11 DHACAs emulate properties of skin, thereby providing an extracellular matrix, cell types such as fibroblast, epithelial cells, and stem cells, and growth factors to facilitate more efficient wound closure.12,13 DHACAs, regulated by the Food and Drug Administration (FDA) under section 361 of the Public Health Services Act and the Code of Federal Regulations Part 1270 and 1271,11,14 are required to be minimally manipulated in a way that maintains the integrity of the extracellular matrix and growth factors and the native cells of the placenta.15–17 While DHACAs are not currently considered part of SoC, several studies have demonstrated the efficacy and comparative effectiveness of these products and other classes of CTPs, generally referred to as “skin substitutes.” For example, the American Diabetes Association highlights several evidence-based adjunctive therapies that should be considered after SoC treatment has failed, specifically including CTPs such as placental-derived membranes like DHACAs. 18 A recent meta-analysis found that complete wound healing at 6 and 12 weeks and wound size reduction were significantly better following DHACA application combined with SoC, compared to SoC alone. 19 In addition, the use of DHACA in LEDUs was associated with reduced amputations, healthcare utilization, and 30-day readmissions.20,21
Despite their improved efficacy and effectiveness at supporting wound closure among LEDU patients, the reimbursement landscape for DHACAs has challenged their uptake as a consistent complement to SoC. Like SoC, DHACAs are applied recurringly in tandem with debridement. 8 A chronic wound with the complex nature of an LEDU could require 12 weeks or more of debridement and reapplication of DHACA. 8 However, the U.S. Centers for Medicare & Medicaid Services (CMS) has published a proposed local coverage determination (LCD) limiting the number of applications of any CTP graft to eight applications within 12 weeks of the first application. 22 This proposed LCD may minimize the likelihood of success for patients at risk to incur more complex wounds and places providers in the position of balancing patient-centered care and clinical discretion with reimbursement decisions that may not provide coverage for a patient throughout their care pathway. 23 This coverage determination will also likely be mimicked by U.S. commercial payers who cover more than 50% of Medicare beneficiaries in the country, as well as other patients with LEDU under the age of 65.
Thus, while there has been a growing body of evidence on the clinical efficacy of DHACAs related to wound closure,24,25 continual, updated evidence on the comparative real-world effectiveness of DHACAs in the Medicare population may benefit both patients and providers by informing the evidence reviewed and considered by CMS and commercial payers as part of ongoing coverage decisions. To this aim, we conducted comparative effectiveness research on LEDUs using DHACAs compared to SoC among U.S. Medicare beneficiaries leveraging the most current real-world evidence available (2018–2022). Studying this elderly population not only serves to inform Medicare on the clinical utility of DHACAs but also provides data on the comparative effectiveness for these beneficiaries.26,27
MATERIALS AND METHODS
Study design
We analyzed a retrospective observational cohort of Medicare beneficiaries with LEDUs treated with a DHACA or SoC between 2018 and 2022 using claims data from the Medicare Limited Data Sets (2018–2022). Medicare claims from 2022 were the most recent data currently available from CMS at the time of the study. Medicare beneficiaries in the inpatient, outpatient, and skilled nursing facility (SNF) settings with an LEDU during the study timeframe were included.
Novel clinical interventions
DHACAs evaluated in this study included amniotic and chorionic placental membrane allografts. A full list of products can be found in Supplementary Table S1.
Study population
Medicare beneficiaries with LEDU were included in the cohort if they met the following criteria: (1) one inpatient or two outpatient visits with an International Classification of Disease, 10th Revision (ICD-10 CM) code for diabetes at least 30 days apart (i.e., E0800 through E139); (2) an ICD-10 CM code for lower-extremity pressure ulcer (i.e., L89.X); (3) an ICD-10 CM code confirming the pressure ulcer was of diabetic etiology (i.e., E10.621); (4) a chronic wound lasting at least 4 weeks; (5) did not have a ICD-10 CM code for venous leg ulcer; and (6) received care in the United States. Similar to prior studies, all claims were clustered into episodes of care (EOC) such that claims for the same wound episode were captured together. The first claim for a wound initiated the EOC, and subsequent claims without a 90-day gap from the initial or subsequent claim were collapsed to form the EOC. 20 A beneficiary having a claim meeting the above criteria but 90 days from a prior claim would initiate a new LEDU EOC. EOCs that received a DHACA or simple wound debridement, hereafter classified as no advanced treatment (i.e., SoC), were included in the cohort. EOCs that received a non-DHACA CTP or alternative therapies (i.e., negative pressure wound therapy [NPWT], hyperbaric oxygen therapy [HBOT]), identified using Healthcare Common Procedural Coding System and/or CPT codes, were excluded (Fig. 1).

Flow diagram of study sample selection for lower-extremity diabetic foot ulcers (LEDU) receiving dehydrated human amnionic and chorionic allografts (DHACAs) or nonadvanced therapy (NAT) for SoC from the Medicare Limited Dataset, 2018–2022.
Exposures and main outcome measures
This analysis included several sociodemographic characteristics, such as age (continuous), sex (Male/Female), race (White/non-White), and geography based on the Centers for Disease Control and Prevention Geographic Regions (North, Midwest, South, West). Clinical characteristics controlled for included healthcare setting (Inpatient, Outpatient, SNF) based on initial LEDU claim, and Charlson comorbidity index (CCI) to account for severity of illness. 28 History of diabetic foot ulcer (DFU) for each patient was identified using ICD-10 CM code (Z86.31) if patient received at least one ICD-10 code prior to the start of EOC.
We examined six outcome measures for this study: 30-day mortality; wound recurrence; major amputation; minor amputation; emergency department (ED) utilization; and hospital 30-day readmission. All outcomes were assessed either during the length of the EOC or up to a timeframe (e.g., 30 days) after EOC end. Thirty-day mortality was defined as death occurring within or up to 30 days after an EOC. Recurrence was defined as a recurrent LEDU between 6 months and 1 year post-EOC with at least one other ICD-10 code, apart from confirmation of diabetic etiology, from previous LEDU EOC present in the recurrent EOC. Major amputation was defined as amputations above the ankle, while minor amputation was defined as below the ankle and could occur anytime during the length of EOC. ICD-10 CM and CPT codes were utilized to identify major and minor amputations occurring during and up to the end of the EOC. ED utilization was defined as at least one ED visit occurring during the EOC. Readmission was defined as a hospital 30-day readmission during the EOC where the patient had at least one claim that indicated inpatient stay.
Statistical approach
Frequency distribution of clinical and demographic variables was examined by treatment groups (DHACA versus SoC) using univariate and bivariate statistics. Continuous variables were evaluated using a student’s t-test, and categorical variables were evaluated using chi-square test of independence. Zero-inflated binomial regression was used to evaluate 30-day mortality, wound recurrence, and major and minor amputations as the frequency of outcomes was small. Logistic regression was used to evaluate ED utilization and 30-day readmission. The DHACA and SoC cohorts were matched by propensity score (PS) for age, sex, race, year, region, dual eligibility, CCI, peripheral arterial disease, and length of EOC. We examined several PS-matched models including nearest-neighbor, kernel, and radius PS matching. One to one PS-matching using the nearest-neighbor method with a caliper set to 0.001 was selected because it achieved the most comparable cohort for analyses. All analyses were tested at the 95% confidence level and completed using STATA 17.0 (Texas, USA).
RESULTS
Patient characteristics
We identified 202,417 EOCs among 161,803 unique beneficiaries between 2018 and 2022 (Fig. 1). Of these EOCs, 6.4% received DHACAs (N = 12,901 EOCs among 10,155 beneficiaries). The majority of the EOCs were among males (64.4%), individuals who were White (79.5%), and individuals living in the South region (41.5%). Approximately 6% of the cohort had a history of DFU. The study arms were similar across most demographic characteristics with some differences between DHACA and SoC EOCs identified in dual-eligibility status (i.e., Medicare and Medicaid eligible beneficiaries) and diagnosed peripheral arterial disease (Table 1). Distribution of outcomes in the unmatched cohort can be seen in Table 2.
Unadjusted characteristics of lower-extremity diabetic ulcers per episode of care by treatment received (N = 202,417 EOCs)
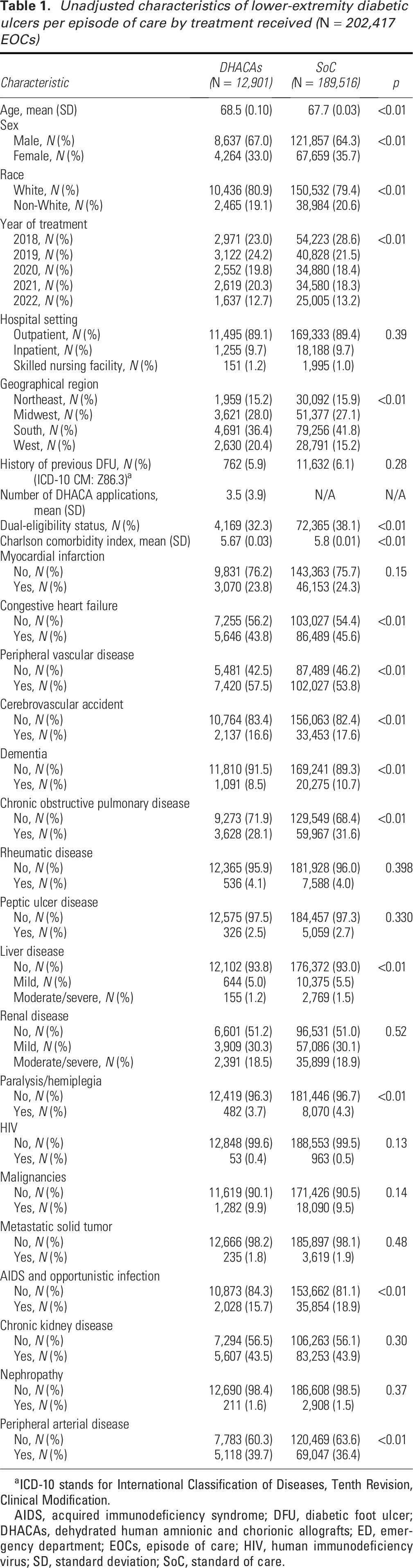
ICD-10 stands for International Classification of Diseases, Tenth Revision, Clinical Modification.
AIDS, acquired immunodeficiency syndrome; DFU, diabetic foot ulcer; DHACAs, dehydrated human amnionic and chorionic allografts; ED, emergency department; EOCs, episode of care; HIV, human immunodeficiency virus; SD, standard deviation; SoC, standard of care.
Unadjusted outcomes of lower-extremity diabetic ulcers per episode of care by treatment received (N = 202,417 EOCs)

Comparative effectiveness of DHACAs versus SoC
We PS-matched 25,760 EOCs with 12,880 EOCs in each group, among 10,136 beneficiaries receiving DHACA and 10,052 receiving SoC (Table 3). The proportion of matched DHACA EOCs was 99.8% (12,880/12,901 EOCs). The PS-matched groups were similar across sociodemographic and clinical characteristics and comorbidities. Table 4 presents relative risk reductions (RRR) derived from multivariable regression for each main outcome measure in the PS-matched cohort. There was 20% RRR in 30-day mortality among DHACA EOCs compared to SoC EOCs (RRR = 0.80, 95% CI: 0.71–0.90). The use of DHACAs was associated with a 28% decreased risk of major amputations (RRR = 0.72, 95% CI: 0.64–0.81), 9% decreased risk of ED visits (RRR = 0.91, 95% CI: 0.86–0.97), and 8% reduction in 30-day readmissions (RRR = 0.92, 95% 0.87–0.98) compared to SoC. These findings amounted to an absolute risk reduction of 0.6% for 30-day mortality, 1.5% for major amputations, 1.8% for ED utilization, and 1.3% for 30-day readmission.
Characteristics by 1-to-1 propensity score-matched cohort (N = 12,880 EOCs per cohort)

ICD-10 stands for International Classification of Diseases, Tenth Revision, Clinical Modification.
Key results of 1-to-1 propensity score-matched cohort (N = 12,880 per cohort) across 25,760 total episodes of care, 2018–2022

DHACA stands for dehydrated human amnionic and chorionic allograft.
We did not observe a statistically significant difference in risk of minor amputation (RRR = 0.95, 95% CI: 0.88–1.02) between those receiving DHACA and SoC. In addition, we did not observe a significant difference in risk of wound recurrence (RRR = 0.86, 95% CI: 0.71–1.04) in the matched cohort, but did observe a statistically significant difference without matching, when only applying direct adjustment for sociodemographic and clinical characteristics in the statistical model (Supplementary Table SA1).
DISCUSSION
We evaluated the comparative effectiveness of DHACAs associated with LEDU wound management, relative to SoC in a large, nationally representative sample of Medicare beneficiaries over 5 years. To our knowledge, this is the most current analysis of real-world evidence among U.S. Medicare beneficiaries with LEDUs. We found that treatment with DHACAs was associated with significant reductions in 30-day mortality, major amputations, ED utilization, and 30-day readmissions (Fig. 2). Other statistical analyses imply trends favoring DHACA for wound recurrence and minor amputation as well, although not statistically significant using our PS-matched methodology. These findings are consistent with previous studies highlighting the effectiveness of DHACAs and other CTPs for LEDU wound management, wound closure, and reduced rates of amputation and mortality.13,14,24–27,29,30

The comparative effectiveness of dehydrated human amnionic and chorionic allografts (DHACA) versus SoC for lower-extremity diabetic ulcer treatment in a propensity score-match cohort in the U.S. Medicare population, 2018–2022 (N = 25,760). *Statistically significant difference between comparators in a propensity score-matched cohort (p < 0.05). **Statistically significant difference between comparators in an unmatched, direct-adjusted cohort (p < 0.05).
One difference in our study was a higher proportion of minor amputations among beneficiaries than in other reported studies.20,31 This difference might be due to the inclusion criteria used in this study (compared to the definition of run-in periods in other studies 20 ) and the omission of EOCs based on episode length of patient death, with other studies selecting healthier populations. 31 However, this estimate is in line with work suggesting that up to half of infected LEDUs require minor or major amputations.32,33 This study, which included a sicker population, nevertheless demonstrated the efficacy of DHACA products demonstrating this use of DHACA for hard-to-heal wounds can avoid the downstream morbidity associated with LEDUs.
Improved wound closure also impacts the economic burden of wounds. Patients with LEDU with amputations have a 5-year mortality akin to patients with cancer. 4 Further, as of 2015, the national annual economic burden attributable to LEDU management was comparable to the total direct costs of cancer management at ∼$80 billion.4,7 Prior studies illustrate reductions in amputations associated with conserving costs related to wound care. 20 Some estimates suggest that 49–85% of amputations caused by LEDU are preventable, and DHACAs could reduce such amputation rates in up to 42% of cases.20,34 In addition, cost-effectiveness analysis has shown that DHACAs dominate SoC by reducing hospital utilization and amputations, which in turn lead to reduced overall costs of care in the Medicare population. 31 These findings highlight the clinical and economic benefits of these products for Medicare patients with LEDU in both the short and long term. This compendium of research suggests that utilization of DHACAs alongside high-quality wound management procedures that emphasize adequate surgical debridement, infection prevention and treatment, and offloading as well as proper diabetes management improve chronic wound healing and reduce overall costs associated with adverse clinical outcomes.
Limitations
There were several limitations. First, the study population was determined to have an LEDU based on the cohort identification criteria of ICD-10 codes on Medicare claims, which are limited by the accuracy of provider coding. Beneficiaries classified as receiving DHACAs were assumed to have the DHACA applied to the corresponding LEDU claim. Absent clinical data, we were unable to rule out the possibility of DHACA application to a concurrent pressure injury, arterial ulcer, or other type of chronic wound; however, this would conservatively bias results toward the null. Similarly, we could not differentiate whether there were multiple LEDUs per beneficiary that were co-occurring, and therefore whether an EOC is capturing a single wound or multiple wounds.
Second, SoC is not uniformly defined in chronic wounds and normally consists of infection and moisture management, debridement, and offloading/compression with no advanced treatments. However, as these are real-world data, there is no visibility into what each patient received as SoC and the extent or quality of such interventions, such as compliance with use of offloading devices. Furthermore, there is no visibility in whether optimal SoC was applied and whether it was applied evenly between the cohorts. Similarly, this analysis could not account for the efficacy of treatment for underlying diabetes or venous insufficiency, nor can we infer the strength of association between LEDU in the study population and concomitant peripheral vascular disease. By convention, adequate vascular flow should be achieved, including by revascularization procedures, before application of a CTP.
Third, though the data utilized in this study included the COVID-19 pandemic, the number of observations in 2020 was similar to other years. It is unclear whether the COVID-19 pandemic potentially resulted in treatment variability that affects these results. As is the nature of observational research, other unobserved interruptions or irregularities could introduce the potential for confounding.
Fourth, there is the potential that unobserved confounding and differences between groups may remain despite PS matching on a robust set of demographic and clinical characteristics, including comorbidities. For example, those beneficiaries receiving DHACAs may receive more aggressive treatment in general for their underlying comorbidities, though this would likely bias the results toward the null hypothesis. Last, these results may have limited generalizability outside of the U.S. Medicare population, such as patients under the age of 65. 35
Conclusions
The wound care field would benefit from future research exploring the comparative effectiveness of DHACA for non-Medicare or ex-U.S. patients, and over longer time horizons, to aid in understanding the generalizability of these findings. Additional studies comparing DHACA products—such as head-to-head clinical trials or comparative effectiveness research with real-world evidence—that include a longer assessment window for recurrence, mortality, and amputation rates would improve our understanding of the clinical benefits and consistency of outcomes across CTPs. Real-world evidence studies provide added confidence in the use of these products for LEDUs, which have been shown in meta-analysis of small studies to result in more complete wound closure 19 and provide decision makers added information when determining the clinical benefit of DHACAs and their coverage policies.
In conclusion, this real-world analysis of Medicare beneficiaries found that DHACAs are associated with superior outcomes compared to SoC in the management of LEDU. These results, and numerous other studies, suggest caution in defining coverage policies that severely restrict access to DHACAs. Since Medicare is the largest single payer in the United States, its coverage determination will influence the coverage policies of commercial payers and could have an impact on the field of care and the national supply of DHACAs. Policy and decision makers can weigh the emerging clinical and economic evidence for DHACAs to balance access and cost considerations in their coverage policies to ensure that effective wound care is available to patients with LEDUs.
KEY FINDINGS
DHACAs products emulate properties of skin and are used, in addition to SoC (e.g., wound debridement), for the treatment of LEDU in Medicare patients. Treatment with DHACAs was associated with significant reductions in 30-day mortality, major amputations, ED utilization, and 30-day readmissions. This real-world analysis of Medicare beneficiaries found that DHACAs are associated with superior outcomes compared to SoC in the management of LEDU and provide added confidence in the use of these products for LEDUs.
AUTHORS’ CONTRIBUTIONS
W.V.P. conceived and designed the study, provided clinical and methodological guidance, supervised data acquisition and analysis, interpreted results, and drafted and edited the article (lead). S.R. conceived and designed the study, conducted data curation and analysis, and drafted and edited the article (equal). B.G.C. contributed to study design, data acquisition and management, analytical approach, interpretation of results, and edited the article (equal). F.C. contributed to study design, data acquisition, and management and analytic approach (equal). P.S. contributed to data acquisition and management (supporting). K.R.H. provided clinical expertise, interpretation of results, and edited the article (supporting/senior). All authors critically reviewed and approved the final version of the article.
Footnotes
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors have no disclosures, and no ghostwriters were employed.
ACKNOWLEDGMENTS AND FUNDING SOURCES
Unrestricted funding was provided by Legacy Medical Consultants via Rubrum Advising. Stage Analytics serves as a technical consultant to Rubrum Advising. W.V.P. declares personal fees and equity holdings from Stage Analytics.