
Abstract
The purpose of this review is to provide verified data on the current knowledge acquired from preclinical and clinical studies regarding topically used antimicrobial peptides (AMPs) with diabetic wound healing activity. The electronic databases were searched for articles published from 2012 to 2022. The 20 articles comparing topically used AMPs in diabetic wound healing treatment versus control treatments (placebo or active therapy) were selected. AMPs have several unique advantages in diabetic wound healing, such as a broad spectrum of antimicrobial activity even against antibiotic-resistant strains, and the capability to modulate the host's immune response and affect wound healing processes through various mechanisms of action. AMPs through antioxidant activity, stimulation of angiogenesis, keratinocytes, and fibroblast migration and proliferation may be considered an important support during conventional therapy used for diabetic wound treatment.

INTRODUCTION
Diabetic wounds and diabetic foot ulcers (DFUs) are considered to be one of the serious complications associated with type 2 diabetic mellitus (DM2). The impaired diabetic wound healing processes lead to serious complications such as a high risk of microbial infections, gangrene, limb amputations, sepsis, and even death. 1 Nowadays, widely accepted options for diabetic wound management include wound debridement, treatment of infection caused by various pathogens, dressings to facilitate a moist wound environment and exudate control, relieving pressure in foot ulcers, vascular assessment, reducing the period of prolonged inflammatory phase, medical monitoring of the remodeling phase of wound healing, prevention of recurrence of DFUs, and glycemic control. 2
DFUs are frequent and potentially devastating complications of diabetes. Patients with ischemia and infection were nearly 90 times more likely to receive a midfoot or higher amputation compared with patients in less advanced wound stages. 3 Increasing Wound, Ischemia, and Foot Infection stage is associated with a prolonged wound healing time, a higher number of surgical procedures, and an increased cost of care. 4
The infected diabetic wound heals more difficult and longer compared to an uninfected diabetic wound. Moreover, an uncontrolled infection can progress contiguously to involve the deeper soft tissues and ultimately the bone, which usually leads to lower extremity limb amputation. The most common bacteria detected in DFUs are superficially located Gram-negative bacteria (Pseudomonas aeruginosa, Escherichia coli, Proteus spp., Klebsiella spp., Acinetobacter spp., and Enterobacter spp.) and Gram-positive bacteria (methicillin-susceptible Staphylococcus aureus, methicillin-resistant S. aureus, and β-hemolytic Streptococcus), and deeply located anaerobes (Peptostreptococcus spp., Bacteroides spp., Prevotella spp., and Clostridium spp.).5–7
Bacteria such as P. aeruginosa, E. coli, Citrobacter spp., Acinetobacter spp., and S. aureus were strongly correlated with nonhealing chronic wounds, such as DFU.8,9 DFU isolates have also confirmed the presence of biofilm and multiantibiotic-resistant bacteria in the wound site of diabetic patients. 10 It was found that all the Gram-positive isolates from DFUs displayed resistance against penicillin and vancomycin, whereas the resistance of P. aeruginosa increases against the most efficient antimicrobials such as ciprofloxacin (77%) and gentamicin (69%). 11
In turn, biofilms evade the host's immune system and may be up to 1,500 times more resistant to antibiotics than planktonic cells.10,12 Bacteria within biofilms are enclosed in a network of a self-produced matrix of extracellular polymeric substances such as exopolysaccharides, proteins, extracellular DNA, and teichoic and lipoteichoic acids, which amplify the resistance to most of existing antimicrobial agents. 13 Therefore, biofilm-forming bacteria and fungi present in diabetic wound infections are less susceptible to antibiotic treatment, which translates into abnormal and prolonged wound healing. 14 Topical antimicrobial agents or systemic administration of antibiotics do not always help to reduce the risk of progressive infection; also, they do not show wound healing properties. 15 Therefore, novel and more effective therapeutic agents are essential for the treatment of diabetic wounds.
Antimicrobial peptides (AMPs), small molecular weight membrane-active peptides with a broad spectrum of activity against various microorganisms (bacteria, yeasts, and fungi), may be attractive therapeutic agents in diabetic wound infection.16,17 These small peptides are essential components of human innate immunity and contribute to the first line of defense against wound infection.18,19 AMPs disrupt the membrane integrity or inhibit the cellular functions of bacteria, viruses, and fungi. 20
AMPs can block DNA replication and disrupt RNA and protein synthesis, which in turn lead to bacterial cell wall lysis. 21 AMPs can act through the production of reactive oxygen species (ROS) and mitochondrial dysfunction, thus leading to microbial cell apoptosis.22,23 Furthermore, AMPs have been considered a potential therapeutic source due to their different mechanisms of action, broad-spectrum properties, and antibiofilm potential, in comparison with conventionally used antibiotics.24–27 The LL37 has been shown to have antimicrobial and antibiofilm activity against multiple Gram-positive and Gram-negative human pathogens.18,28,29
Human β defensins (hβD)-2 was shown to be effective in eliminating biofilms formed by E. coli, 30 P. aeruginosa, 31 and S. aureus. 32 Furthermore, AMPs are implicated both in defense against bacterial infections and in the wound healing process.33,34 AMPs have immunomodulatory activity,35,36 angiogenic activity, 37 and antioxidant activity, 38 and stimulates epidermal growth factors (EGFs), 39 and keratinocyte and fibroblast proliferation and migration, 40 influencing the wound healing process. Some AMPs, such as human LL37 cathelicidin,41,42 recombinant peptide PLL-37 (derived from LL-37 with the N-terminal proline), 41 hβD, 43 and human AP-57, 44 have confirmed wound healing activity. A large number of articles described AMPs as promising wound healing agents,33,34 but only a few of them focus on AMPs for diabetic wound healing or infected diabetic wound.
The purpose of this review is to provide verified data on the current knowledge acquired from preclinical and clinical studies regarding topically used AMPs with diabetic wound healing activity. Moreover, the antimicrobial activity of AMPs used for diabetic wound infections, and various cellular and molecular mechanisms of their actions will also be described.
METHODS
Search strategy
The PubMed, Scopus, and Google Scholar databases were searched for articles published from 2012 to present. Search terms included “antimicrobial peptides for topical treatment of diabetic wounds,” “antimicrobial peptides for topical treatment of diabetic foot ulcers,” and “antimicrobial peptides used in diabetic infection.” References from reviews about AMPs used for the topical treatment of diabetic wounds were searched for additional articles and case reports. A manual search was also conducted based on citations in the published literature.
Inclusion and exclusion criteria
The results of the animal- and human-based studies on topically used AMPs in diabetic wound healing versus control treatments (placebo or active therapy) were selected. Other ways of administration (e.g., oral, systemic) of AMPs in diabetic wound healing than the topical were excluded from the study. Also, AMP wound healing activities other than diabetic wound healing were excluded from the study. Publications describing ischemia were excluded from the study. Moreover, publications in languages other than English were excluded. Finally, 20 articles that meet the criteria were used for the review (Fig. 1).

Search strategy used to identify relevant articles.
AMPs USED FOR DIABETIC WOUND INFECTIONS
AMPs have several unique advantages in diabetic wound healing, such as a broad spectrum of antimicrobial activity even against antibiotic-resistant strains and their capability to modulate the host immune response. 45 AMPs are currently being applied as promising therapies against polymicrobial-infected chronic wounds such as DFUs. 46 Some AMPs showed antimicrobial activity against Gram-positive and Gram-negative bacteria isolated from diabetic wounds (Table 1). Hydrogel with Jelleine-1 and 8-Bromoadenosine-3′,5′-cyclic monophosphate, 50 and human neutrophil peptide-1 (HNP-1) and hβD-1 in combination with cefotaxime, as well as HNP-1 and hβD-1 encapsulated in niosomes 49 showed antibacterial activity against MRSA isolated from diabetic wounds. Tet-213- and silver nanoparticles-loaded porous silicon microparticles showed antibacterial activity against S. aureus. 53
Antimicrobial activity of antimicrobial peptides used for diabetic foot ulcer
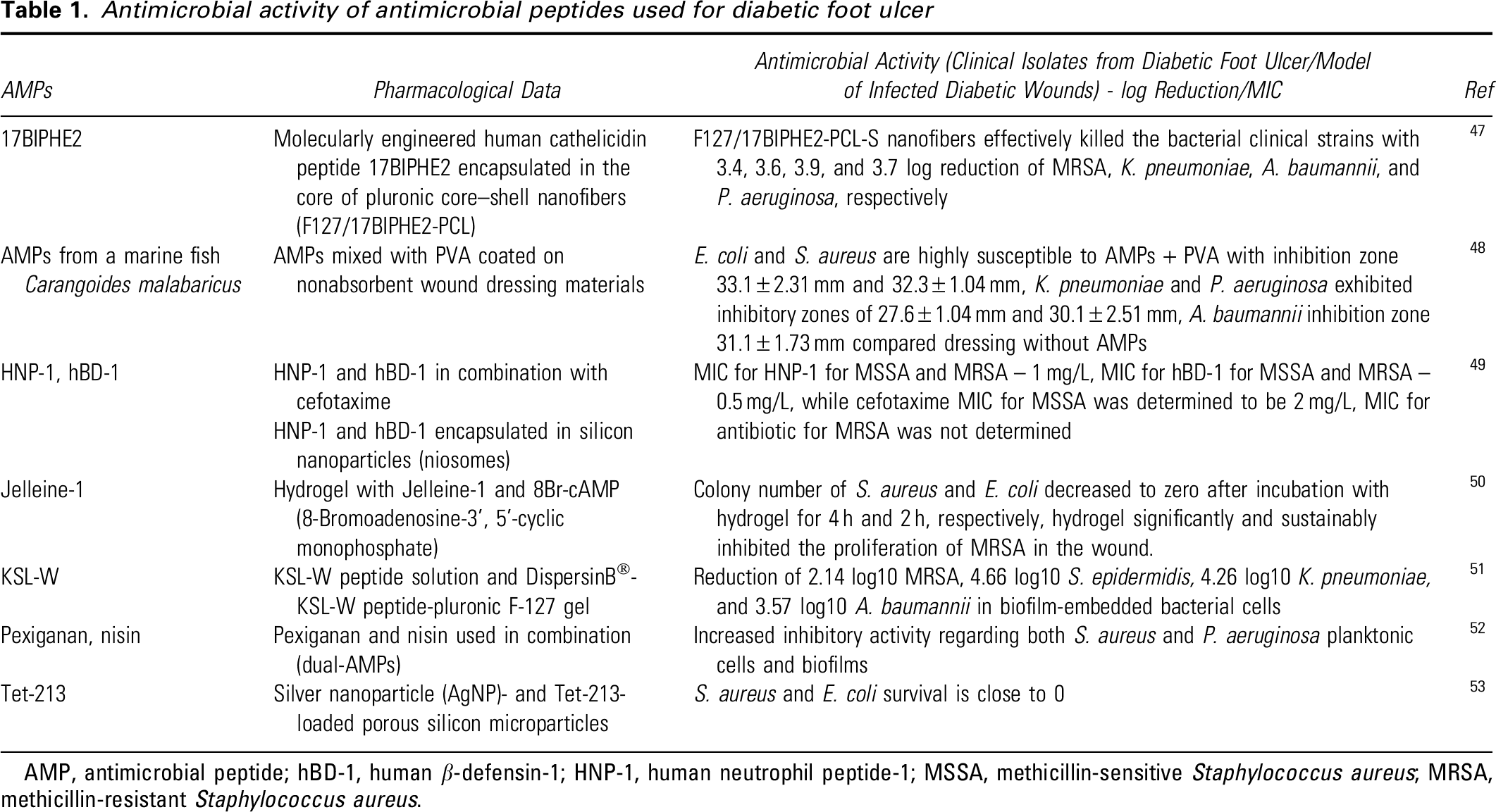
AMP, antimicrobial peptide; hBD-1, human β-defensin-1; HNP-1, human neutrophil peptide-1; MSSA, methicillin-sensitive Staphylococcus aureus; MRSA, methicillin-resistant Staphylococcus aureus.
Pexiganan and nisin used in combination (dual AMPs) showed antimicrobial activity against planktonic and biofilm of S. aureus and P. aeruginosa isolated from diabetic foot infections (DFIs). 52 Also, a hydrogel with cecropin showed antibacterial activity against S. aureus and P. aeruginosa from infected wounds in diabetes. 54 Human cathelicidin peptide 17BIPHE2 encapsulated in the core of pluronic core–shell nanofibers showed antibacterial activity against MRSA, K. pneumoniae, A. baumannii, and P. aeruginosa isolated from chronic wounds. 47
AMPs from a marine fish Carangoides malabaricus mixed with PVA coated on nonabsorbent wound dressing materials showed antibacterial activity against E. coli, K. pneumoniae, A. baumannii, S. aureus, P. aeruginosa, 48 while KSL-W peptide solution and DispersinB®-KSL-W peptide-pluronic F-127 gel against S. epidermidis, K. pneumoniae, P. aeruginosa, and A. baumannii from diabetic wound infection. 51 Furthermore, it was shown that in some antibiotics, clarithromycin significantly improves LL37-mediated antibacterial activity and wound healing capacity of fibroblasts in well-controlled T2D patients through upregulation of LL37 on neutrophil extracellular traps. 55
AMPs USED FOR DIABETIC WOUND HEALING
Animal-based studies
The most described animal studies are based on diabetes induced by streptozotocin (STZ), a cytostatic antibiotic produced by Streptomyces achromogenes, used clinically as a chemotherapeutic agent in the treatment of pancreatic β cell carcinoma. 56 It was shown that damaged pancreatic β cells, resulting in hypoinsulinemia and hyperglycemia, induced type 1 and 2 diabetes in rodents.57–59 Only one reported study has been conducted on leptin receptor-deficient diabetic mice (57BLKS-LepR, db/db). 60 The db/db mice are used as model diabetes type 2 and demonstrate chronic hyperglycemia and pancreatic beta cell atrophy, and come to be hypoinsulinemic. 61
Wound healing activity of AMPs conducted on animals with induced diabetes is mainly based on the excision wound model or punch biopsy model through the removal of some part of the skin at the depth of the epidermis and upper dermis (partial thickness or split-thickness wound) or both epidermis and dermis up to the fascia or subcutaneous tissue (full-thickness wound). 62 Excision wounds can be observed during diabetic wounds. Therefore, the excision wound model allows the observation of wound re-epithelialization and wound contraction during topical treatment.
AMPs alone (Table 2) and AMP-loaded dressings (Table 3) showed diabetic wound healing activity in animal-based studies. Lysozyme-AMP fusion protein, 38 IBP5, 63 LFcinB, 64 and RP55765 markedly accelerated diabetic wound healing. In turn, IDR-1018 demonstrated significantly accelerated wound healing in S. aureus-infected porcine and nondiabetic, but not in diabetic murine wounds. 60 It seems that IDR-1018 promotes wound healing independent of direct antibacterial activity. It is anticipated that the wound-healing activities of IDR-1018 can be attributed to the modulation of host immune pathways, which are suppressed in diabetic wounds and provide further evidence of the multiple immunomodulatory activities of IDR-1018. Moreover, IDR-1018 induced faster wound closure than LL-37 and HB-107.
Antimicrobial peptides used for diabetic wound healing, animal-based studies

CAT, catalase; COX-2, cyclooxygenase-2; EGF, epidermal growth factor; FGF-2, fibroblast growth factor-2; GSH, glutathione; ICAM-1, intercellular adhesion molecule; IL-6, interleukin 6; MAPK, mitogen-activated protein kinase; MRSA, methicillin-resistant Staphylococcus aureus; p-Akt, phosphorylated serine/threonine kinases; p-ERK, phosphorylated extracellular signal-regulated kinase; SOD, superoxide dismutase; STZ, streptozotocin; TNF-α, tumor necrosis factor-α; VEGF, vascular endothelial growth factor.
Antimicrobial peptides loaded dressings used for diabetic wound healing, animal-based studies

IL-6, interleukin 6; MRSA, methicillin-resistant Staphylococcus aureus; p38 MAPK, p38 mitogen-activated protein kinase.
Topical applications of AMPs loaded in various dressings seem to be a good alternative for infected wound or assisting in tissue regeneration. 66 Some studies are focused on AMP-loaded dressing used for diabetic wound healing in animal-based studies (Table 3). Wound dressings based on nanofibers with scaffolding architecture replicate the characteristics of the skin, a large surface area to volume ratio to allow cell adhesion and exudates absorbing capacity, tunable porous structure for easy flow nutrient infiltration and gas exchange, encapsulation of drug for achieving their controlled release, they appear to be desirable properties for dressings used in wound healing.71,72 Moreover, nanofiber scaffolds reduce the frequency of dressing changes and minimize patients' discomfort.
IP-1 incorporated in nanocomposites 67 and W379-incorporated nanofiber aerogels with macrochannels 70 enhanced diabetic wound healing and antibacterial activity in wound infections. Also, a novel gene delivery system based on the AMP (LL37) grafted ultra-small gold nanoparticles (AuNPs@LL37) for the topical treatment of diabetic wounds with or without bacterial infection, showed a promising effect. 68 Moreover, AuNPs@LL37 combined with VEGF plasmids promoted angiogenesis and inhibited MRSA infection in diabetic wounds, resulting in accelerated wound closure rates, faster re-epithelialization, improved granulation tissue formation, and high VEGF expression. This active agent showed higher antibacterial ability than the free AMPs and the cationic AuNPs alone in vitro and in vivo due to synergistic effects.
Also, LL37-conjugated gold nanoparticles (LL37NPs) immobilized in polyurethane-based wound dressings (PU-adhesive-LL37NPs) prevent bacterial infections (S. aureus, E. coli, and P. aeruginosa) and facilitate wound healing by tissue contact, inducing re-epithelialization and anti-inflammatory processes in diabetic conditions. 69 Hydrogel with oxidized dextran (ODEX), AMP-modified hyaluronic acid (HA-AMP), and platelet-rich plasma (PRP) (ODEX/HA-AMP/PRP) significantly improve diabetic wound healing and antibacterial activity against S. aureus and P. aeruginosa in the infected diabetic wound. 54 AMP-loaded dressings and AMP drug delivery to the target site is an innovative approach to enhance the therapeutic efficacy in the healing of diabetic wound infection (Fig. 2). This section will certainly be expanded in the future.

AMP-loaded dressing for diabetic wound healing. AMP, antimicrobial peptide.
Unfortunately, some studies described above have not only shown the potential therapeutic activity of AMPs in diabetic wound healing but also pointed out the limitations of the research. The lysozyme-AMP fusion protein study was limited by the small sample size, and some mechanisms, such as neuropathy, were not illuminated. 38 Finally, time was relatively short from the preparation of the diabetic wound to treatment with the lysozyme-AMP fusion protein, so the use of fusion protein in DFU treatment could not be fully shown.
IDR-1018 did not demonstrate any effect on diabetic (type-II) wound healing, suggesting the wound healing-promoting mechanism is absent or suppressed in diabetic wounds, while a positive impact on wound healing in nondiabetic mice was observed. 60 It was also shown that LFcinB promoted epithelial closure in ex vivo wound healing model of primary porcine keratinocytes, which was accompanied by the subsequent increase in epithelial cell proliferation, whereas in in vitro model, ii did not. 64 The obtained results are not clear, and the authors tend to further investigation.
Human-based studies
There are only a few clinical trials describing the influence of AMPs on diabetic wound healing (Table 4). The human studies reported were performed in the context of DFUs, which are chronic, nonhealing wounds that are frequently associated with peripheral vascular disease and neuropathy. 76 Moreover, DFUs, especially when they become infected, are a leading cause of morbidity and may lead to amputation. Treatment of DFUs usually requires wound debridement, glycemic control, and surgical interventions. 77 It was shown that SR-037975 and scorpion AMP 74 reduced DFU wound area, while pexiganan acetate cream application was clinically comparable to an oral antibiotic (ofloxacin) therapy in treating diabetic patients with a mildly infected foot ulcer. 73 Moreover, pexiganan acetate cream might reduce the risk of selecting antimicrobial-resistant bacteria.
Antimicrobial peptides used for diabetic wound healing, human-based studies

The incidence of amputation (2%–3%) did not differ significantly between pexiganan and ofloxacin treatment groups. The pexiganan cream 0.8% (Locilex®; Dipexium Pharmaceuticals, Inc.) has been registered in two pivotal phase III clinical trials, OneStep-1 and OneStep-2: randomized, double-blind, multicenter, placebo-controlled studies as antibacterial candidates for DFIs. 78 Locilex was applied twice daily for 14 days in patients with mild DFIs and did not meet the primary efficacy endpoint versus vehicle plus standard of care in wound closure rate. in addition, Locilex failed to meet the secondary endpoint of demonstrating a higher rate of bacterial eradication.
Moreover, FirstString Research, Inc., also developed a Granexin® Gel that contains the synthetic aCT1 peptide for treating DFUs. 79 This formulation was under phase III until May 2020 and has since been terminated without safety or efficacy concerns. Finally, only a few AMPs have obtained FDA approval for the treatment of bacterial skin infections or acute wounds, including Neosporin® (gramicidin), Cubicin® (daptomycin), Vancocin® HCl (vancomycin), Orbactiv® (oritavancin), Dalvance® (dalbavancin), and Vibativ® (telavancin). 80
MECHANISM of ACTION of AMPs in DIABETIC WOUNDS
Wound healing difficulties in diabetes patients are related to chronic inflammation, impaired production of cytokines and growth factors, reduction of nitric oxide, microvascular complications, impaired keratinocytes, and fibroblast migration and proliferation, abnormal matrix metalloproteinase, excessive proteolytic enzymes activity, tissue oxidative stress, and bacterial infection. 81 It was also shown that the expression of AMPs in chronic wounds is significantly reduced and contributes to the impairment of wound healing. 82
Hozzein et al. 83 showed that expression of β defensin-2 was significantly reduced in diabetic mice. Gonzalez-Curiel et al. 84 determined that patients with DM2 express lower levels of LL37 and hβD-2 genes in peripheral blood cells, which could explain the higher susceptibility to DFU infections. It was also showed that patients with DFUs (grade 2–4 according to the Wagner's classification) and patients with venous calf ulcers present insufficient expression of hβD-2 in comparison to normal skin, suggesting the pathological role of this protein in the chronicity of ulcers. 85 Also, RNase 7 downregulation can make DM2 patients prone to infections and impaired wound healing. 86 RNase 7 levels were decreased in DM2 patients with or without DFU compared with skin from healthy donors.
Moreover, most DM2 patients are treated with drugs (glyburide, metformin, or insulin) to reduce glycemia and results showed that metformin reduces the expression of RNase 7 in in vitro treated keratinocytes, suggesting that the chronic use of metformin should be evaluated in DFU patients. Conversely, Rivas-Santiago et al. 87 have demonstrated that hβDs were overexpressed in biopsies from patients with DFUs (grade 3 according to Wagner's classification), whereas LL37 has low or no expression in comparison with biopsies from healthy skin donors. Moreover, when primary cell cultures from these biopsies were infected with S. aureus, epidermal cells from diabetic ulcers showed lower LL37 expression compared with cell cultures from healthy donors' skin.
These results suggest that defensin production in DFUs seems to not be enough to promote proper wound healing, while the low or lack of production of cathelicidin might contribute to the pathogenesis of DFUs. Interesting is the fact that the expression levels of human α defensins HNP1, HNP3, and HNP4 were significantly higher in the wound center than at the edge of DFUs. 88 Moreover, human α defensins through hemoglobin A1C (HbA1c), which significantly promoted IL-8 expression, aggravated the inflammatory response in patients leading to poor healing of DFUs.
AMPs applied topically on diabetic wound act through different mechanisms of action, including antimicrobial, anti-inflammatory, and antioxidant activity, stimulation of angiogenesis, production of cytokines and growth factors, keratinocytes, and fibroblast proliferation and migration. Therefore, AMPs may be considered an important support during conventional therapy used for diabetic wound treatment (Fig. 3).

AMPs for diabetic wound healing – mechanism of action.
Inflammatory cell response
AMPs are defined as host defense peptides because of their essential role in constituting the innate immunity system. 89 The influence of AMPs on the skin's immune system has been confirmed.90,91 Human cathelicidin presents a receptor-mediated chemotactic activity, and activation of immune cells occurs through the formyl-peptide-like receptor-1 (FPRL-1), G-protein-coupled receptors, the nucleotide receptor P2X7, and Toll-like receptor (TLR) signaling. 92 Also, hβDs stimulate keratinocytes to produce proinflammatory cytokines and chemokines such as interleukin IL-6, IL-10, monocyte chemoattractant protein-1, and macrophage inflammatory protein-3a and mediate keratinocyte migration and proliferation. 93
Moreover, it has been demonstrated that hβD3 through the inhibition of TLR signaling pathways in immune cells leads to transcriptional repression of the proinflammatory genes. 94 HβDs help in combating insulin resistance by inhibiting the production of glucocorticoids, reducing chronic inflammation by acting through the TLR signaling pathway, and provoking cell migration, proliferation, angiogenesis, and stabilization of fibroblasts and keratinocytes, ultimately resulting in diabetic wound closure. 95 The lysozyme-AMP fusion protein promotes diabetic wound size reduction by improving anti-inflammation through decreased levels of proinflammatory cytokines (IL-6 and TNF-α) content, and expression of COX-2. 38
Bovine lactoferricin (LFcinB) improved wound healing in diabetic mice through decreased M1-to-M2 macrophage ratios, suggesting the downregulation of inflammation in diabetic wounds. 64 LL37 peptide immobilized in polyurethane (PU)-based wound dressings showed lower macrophage infiltration in the diabetic wounds as well as low expression of proinflammatory cytokines such as TNF-α and IL-6 after 6 days of treatment, indicating that they act as an anti-inflammatory dressing. 69 Cecropin hydrogel inhibited proinflammatory factors (TNF-α, IL-1β, and IL-6) and enhanced anti-inflammatory factors (TGF-β1) in infected wounds in diabetes. 54
Free radicals and oxidative stress
Oxidative stress is caused by an increase in free radicals such as ROS and/or reactive nitrogen species in the body, which leads to intercellular biochemical dysregulation of the redox status. 96 An imbalance of free radicals and antioxidants [superoxide dismutase (SOD), catalase (CAT), and glutathione (GSH)] in the body results in the overproduction of ROS, which lead to cell/tissue damage and generate inflammation, neuropathy, ischemic lesion, topical infection, and in consequence, delayed diabetic wound healing. 97 Therefore, decreasing ROS levels through antioxidative systems may reduce oxidative stress-induced damage and improve diabetic wound healing. The lysozyme-AMP fusion protein accelerated wound healing through reduced oxidative stress by increasing activities of antioxidant enzymes, including SOD, glutathione peroxidase (GSH-Px), CAT, and decreased lipid peroxide content in serum (STZ)-induced diabetic rats. 38
Growth factor production
Growth factors such as transforming growth factor (TGF), EGF, fibroblast growth factor (FGF), insulin-like growth factor (IGF), keratinocyte growth factor (KGF), platelet-derived growth factor (PDGF), and vascular endothelial growth factor (VEGF) are necessary for wound healing. 98 It was shown that the downregulation of growth factor receptors and rapid degradation of growth factor lead to delayed wound healing in diabetics. 99 The reduced concentration of TGF-β, 100 EGF,101,102 FGF-7, 103 and KGF 104 has been reported in diabetic wound and their influence on the delays in wound healing was also confirmed. It was also shown that the growth factors, IGF-1 and TGF-α, induce the expression of AMPs such as hCAP-18/LL-37 and hβD-3 in human keratinocytes. 105
Lysozyme-AMP fusion protein increases the expression of VEGF and FGF-2 in granulation tissues in STZ-induced diabetic rats. 38 LL-37-grafted ultra-small gold nanoparticles (AuNPs@LL37) promotes the expression of VEGF in diabetic wounds with bacterial infection. 68 AMP-IBP5 increases VEGF in keratinocytes in diabetic wounds. 63 Moreover, AMP-IBP5-induced activity was mediated by the EGF receptor, signal transducer and activator of transcription 1 and 3, and mitogen-activated protein kinase (MAPK) pathways.
Keratinocyte and fibroblast proliferation and migration
During the proliferative phase of wound healing, keratinocytes, fibroblasts, and endothelial cells proliferate, migrate, and differentiate, which enable the formation of granulation tissue, restores surface integrity, and promotes wounds closure. 106 In the epidermis, bacterial contact and inflammation stimulate keratinocytes to produce hCAP18/LL-37.107,108 Moreover, cathelicidin hCAP18/LL-37 upregulated at the skin wound site induces keratinocyte migration by epidermal growth factor receptor (EGFR) transactivation and STAT3 phosphorylation. 109
Also, hβD-2 supports the proliferation, migration, and differentiation of dermal fibroblasts and epidermal keratinocytes. 93 W379, AMP incorporated nanofiber aerogels with microchannel enhance skin cell migration, granulation tissue formation, and re-epithelialization through activation of p38 MAPK signaling pathway. 70 LL37 peptide immobilized in polyurethane-based wound dressings enhanced wound healing and re-epithelialization in diabetic mice. 69 AuNPs@LL37/pDNAs (AuNPs@LL37 combined with VEGF plasmids) accelerate wound closure rates through faster re-epithelialization and improved granulation tissue formation. 68 IP-1-functionalized cerium oxide nanoparticles incorporated with reduced graphene oxide nanocomposites enhance rapid keratinocyte proliferation and migration leading to wound closure. 67
Angiogenesis
Angiogenesis is an essential part of the wound healing process, consisting of the formation of a new capillary network (microvascular) in response to hypoxia or other stimuli in diabetics. 110 The hypoxic conditions in diabetes induce macrophages to secrete proangiogenic growth factors such as VEGF, FGF, PDGF, and cytokines, TGF-β and IL-1, involved in the control of various aspects of angiogenesis.111,112 VEGF and PDGF are one of the most important angiogenic factors in wounds.
Various studies have suggested that VEGF and PDGF can accelerate wound healing by increasing vessel formation. 113 VEGF production lies downstream of hypoxia and hyperglycemia. Hypoxia activates hypoxia-inducible factor-1 (HIF-1), a transcriptional activator that promotes angiogenesis by upregulating target genes such as VEGF-A. 114 Hyperglycemia can also induce indirect VEGF overexpression mediated by TGF-β. 115 Moreover, the levels of angiogenic factors are downregulated in nonhealing chronic wounds. 116 The upregulation of FGF and PDGF is associated with angiogenesis in diabetes and stimulates wound healing in diabetic mice. 117 Some AMPs induce angiogenesis. It was shown that LL-37 promotes angiogenesis by activating FPRL1 expressed on endothelial cells. 37
The hβD-3 accelerates wound healing by enhancing the secretion of angiogenic growth factors such as FGF, PDGF, and VEGF, and induced the migration and proliferation of human fibroblasts through FGFR1/JAK2/STAT3 signaling pathways. 118 Also, the secretion of angiogenin, a potent stimulator of angiogenesis, was dose-dependently increased by hβD-1, hβD-2, hβD-3, and hβD-4, and this secretion was mediated by the activation of EGFR, Src family kinase, c-Jun N-terminal kinase (JNK), p38, and nuclear factor-kappa B (NF-κB) signaling pathways. 119 Lysozyme-AMP fusion protein promotes diabetic wound size reduction through increased levels of proangiogenic cytokines (VEGF and ICAM-1), and expression of VEGF, FGF-2, p-ERK, and p-Akt protein in granulation tissues. 38 AMP-IBP5 markedly accelerated wound healing, increased the expression of angiogenic factors, and promoted vessel formation in diabetic mice. 63
It was found that AMP-IBP5 rescued the high glucose-induced attenuation of proliferation and migration, as well as the production of angiogenin and VEGF in keratinocytes. The AMP-IBP5-induced activity was mediated by the EGFR, signal transducer and activator of transcription 1 and 3, and MAPK pathways, as indicated by the inhibitory effects of pathway-specific inhibitors. Also, W379-incorporated nanofiber aerogels with microchannel greatly enhance vascularization through activation of p38 MAPK signaling pathway. 70 LFcinB, 64 AuNPs@LL37/pDNAs, 68 and cecropin hydrogel 54 improved diabetic wound healing by promoting angiogenesis and expression of VEGF.
ADVANTAGES AND DISADVANTAGES of AMP USE in CLINICAL APPLICATION - FUTURE ASPECTS
AMPs display advantages over conventional antibiotics to combat various skin infections and potential immunomodulatory properties. 91 They have a broad spectrum of microbial activity and through different modes of action, limited emergence of resistance.120–122 Moreover, synergistic interactions with conventional antibiotics could eliminate the threat of multidrug-resistant bacteria. 45 Unfortunately, in most cases, AMPs have failed clinical trials.80,123,124 Challenges to the clinical application of AMPs include cytotoxic effects, limited stability under physiological conditions, and problems related to peptide bioavailability and efficacy.123,125 Several AMPs cause hemolytic and/or cytotoxic effects at antimicrobial concentrations, limiting their wider utilization.126,127
Polymyxins are crucial antimicrobials to eradicate MDR Gram-negative bacteria, but they may cause nephrotoxicity and neurotoxicity at antimicrobial concentrations. 128 Toxicity and increased hemolytic activity of AMPs are related to high hydrophobicity. 129 Control of hydrophobicity and charge can reduce the toxicity of AMPs. Also, AMP susceptibility to proteolytic degradation, loss of antimicrobial activity in the presence of serum or physiological concentration of salts, anionic proteins and polysaccharides found in the biological fluids, and alkaline pH of wounds limits their antimicrobial activity and wound healing effects.130–133 Some AMPs lose their activities under the physiological salt conditions due to the loss of electrostatic interactions between peptides and the cell membrane. 134 Most AMPs have lower activity in serum because they bind to serum proteins such as albumin and lipoproteins. 135
Moreover, the linear structure of AMPs can be easily attacked by host proteases and peptidases present in blood serum and wound exudate leading to their proteolysis and deactivation. 123 Also, poor stability to gastric pH and susceptibility to proteolytic enzymes make oral administration much more difficult. 136 Therefore, topical administration is often used rather than intravenous or oral administration. 137 However, it was shown that LL-37 is unstable in the DFU microenvironment. 138 Adding to the above, one of the greatest challenges to effective clinical applications of AMPs is their bioavailability. AMPs have much better permeation into tissues and are considerably more stable, less prone to trigger immune/allergic reactions, and significantly cheaper to produce, which underpin the extensive research that has been devoted to finding strategies to improve their bioavailability. 139
To overcome the shortcomings of AMPs, several other strategies have been designed such as chemical modifications of AMP structure (terminal modification, cyclization, replacement of one or more residues with nonproteinogenic amino acid, replacing peptide bonds with other chemical groups, and elimination of one or more residues) to increase AMP metabolic stability and lipophilicity, and use different delivery systems (liposomes, ethosomes, transferosomes, cubosomes, nanostructured lipid carriers, solid lipid nanoparticles, and biopolymers) toward enhanced permeability to obtain more effective and safer AMPs as potential drug candidates.122,140 The development of optimized topical delivery systems with high AMP stability and bioavailability is necessary to maximize the antimicrobial and wound healing effects. Certainly, the AMP research field is still largely unexplored, and great advancement can be expected in the future.
CONCLUSION
AMPs appear to be promising therapeutic agents for diabetic wound healing. AMPs showed a broad spectrum of antimicrobial activity with low resistance rates, display pivotal immunomodulatory activity, and affect cell migration and proliferation, as well as angiogenesis. Numerous animal-based studies and few clinical trials are confirming the activity of AMPs in the stimulation of diabetic wound healing. Topical applications of AMPs loaded in various dressings seem to be a good alternative for the treatment of diabetic wounds.
AMPs are considered to have a high potential in not only eradicating microorganisms but also in promoting wound healing by stimulating re-epithelialization, angiogenesis, collagen, and granulation tissue formation in diabetic wounds. Therefore, AMPs may be considered important support during conventional therapy or even as a substitute for synthetic drugs used for diabetic wound treatment. The creation of an AMP delivery system with prohealing properties would be an important advance in the healing of diabetic wounds and would improve the lives of patients.
Footnotes
AUTHORs' CONTRIBUTION
Conceptualization, A.H.; methodology, A.H. and A.P.H.; writing - original draft preparation and visualization, A.H.; writing - review and editing, A.P.H.; and supervision, A.P.H.. All authors have read and agreed to the published version of the article.
ACKNOWLEDGMENTS AND FUNDING SOURCES
No funding was received for this article.
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. The content of this article was expressly written by the author(s) listed. No ghostwriter was used to write this article.