
Abstract
Objective:
Drugs regulating hypoxia-inducible factor (HIF)-1α have not been investigated for wound healing in lymphedema. Therefore, we examined the effects of drug modulation of HIF-1α activity for wound healing in our previously developed mouse model of nonirradiated hind limb lymphedema.
Approach:
Mouse hind limb lymphedema models (n = 17) and a sham group (n = 6) were created using 8- to 10-week-old male C57BL/6N mice. Mice with hind limb lymphedema were randomized into experimental groups receiving roxadustat, 3-(5′-hydroxymethyl-2′-furyl)-1-benzylindazole (YC-1), or dimethyl sulfoxide and were given intraperitoneal injections every 2 days for up to 2 weeks. Four days after the surgery, an 8-mm diameter full-thickness skin wound was created in the hind limb. The number of days required for wound closure and the percentage of wounds closed were measured. Skin samples taken at wound creation were evaluated by histological and molecular analysis.
Results:
Administration of roxadustat accelerated wound healing, whereas YC-1 delayed it, with a significant decrease and increase in skin thickness, respectively. The relative mRNA expression of Hif1α, matrix metalloproteinase-3, and interleukin-6 was significantly higher in the roxadustat group and that of metalloproteinase-9 was significantly lower in the roxadustat group compared with the control group.
Innovation:
This study is the first to demonstrate delayed wound healing in a mouse model of hind limb lymphedema and the first to demonstrate the promotion of significant wound healing through the use of roxadustat.
Conclusion:
Roxadustat exerts wound-healing effects and may promote the regulation of extracellular matrix remodeling via gene expression in hind limb lymphedema wound models.
INTRODUCTION
Hypoxia-inducible factor (HIF) activates the transcription of genes involved in the cell’s response to hypoxic conditions. It has a heterodimeric structure comprising HIF-1α, which is sensitive to oxygen, and HIF-1β, which is constitutively expressed. 1 The HIF-1α subunit, which has an important regulatory role, was discovered in 1992 by Semenza et al., 2 and its structure and regulatory mechanism have been further elucidated in recent years. Under normoxia, HIF-1α undergoes hydroxylation by prolyl hydroxylases (PHDs), ubiquitination by von Hippel–Lindau protein, and rapid degradation by proteasomes. However, under hypoxia, hydroxylation by PHDs does not occur, and HIF-1α is stabilized without degradation. It then binds to HIF-1β and activates various target genes by binding to the nuclear hypoxia response element. 3 Among the diverse target genes are transcriptionally activated genes related to cell proliferation, erythropoiesis, angiogenesis, extracellular matrix metabolism, glucose metabolism, iron metabolism, and so on.4,5
Taku Maeda, MD, PhD

Roxadustat, also known by its chemical name FG-4592, is a HIF-PHD inhibitor that stabilizes HIF-1α, 6 and 3-(5′-hydroxymethyl-2′-furyl)-1-benzylindazole (YC-1) is a small molecule HIF-1α inhibitor. 7 Roxadustat has been developed as a novel orally active therapeutic agent for renal anemia in patients with chronic kidney disease. 8 Moreover, roxadustat has been reported to have therapeutic potential in diabetes-related diseases such as cardiomyopathy, nephropathy, retinal damage, and impaired wound healing. 9 We previously reported that roxadustat improved a mouse hind limb lymphedema model through the promotion of lymphangiogenesis. 10
Wound tissues become hypoxic due to vascular injury and increased oxygen demand. Relative hypoxia leads to the stabilization of HIF, which is involved in multiple steps in the wound-healing process, including angiogenesis, proliferation and migration of fibroblasts, recruitment of inflammatory cells, differentiation of myofibroblasts, and metabolic reprogramming. 11 The use of roxadustat to induce stabilization of HIF-1α has been shown to promote the healing of skin wounds in a mouse model, 12 as well as refractory skin wounds in a diabetic rat model. 6 However, the impact of drug-induced stabilization or inhibition of HIF-1α on refractory wounds in lymphedema has not been investigated. Because we have previously demonstrated the therapeutic potential of roxadustat in lymphedema, 10 we focused on wound healing in lymphedema during treatment using roxadustat.
Therefore, in the present study, we examine the effects of drug-induced modulation of HIF-1α activity for wound healing, using the mouse model of hind limb lymphedema developed in our previous study. 13
CLINICAL PROBLEM ADDRESSED
In clinical practice, patients with lymphedema are prone to wound formation due to impaired skin barrier function, 14 as well as delayed wound healing, which frequently leads to complications such as cellulitis that may be difficult to treat. When lymphatic fluid transport is impaired, wound healing is reported to be prolonged due to complex pathological conditions such as cellular damage caused by osmotic abnormalities, immunocompromise, infection, and fibrosis.15,16 The development of effective treatment methods for wounds in lymphedema is thus desirable from the perspective of treating associated symptoms.
MATERIALS AND METHODS
Animals
The animal experiments in this study were conducted with approval of the Hokkaido University Institutional Animal Care and Use Committee (approval number 20–0147). Male C57BL/6N mice (n = 23), aged 8–10 weeks, were purchased from Japan SLC (Hamamatsu, Japan) and kept in a room maintained at 24°C, under a 12-h light/12-h dark cycle with free access to food and water. A random number table was used to divide mice into four groups as follows: the sham group (n = 6), roxadustat group (n = 6), YC-1 group (n = 5), and control group (n = 6).
Mouse model and drug administration
The mice were used to establish a model of hind limb lymphedema, as previously reported. 13 Experiments were performed under general anesthesia with 2.5% isoflurane inhalation. Briefly, a circumferential incision was made in the left inguinal region, followed by resection of the inguinal lymph node and surrounding fat pad. The subcutaneous tissue was dissected to expose the left popliteal lymph node area. The node’s afferent and efferent lymphatic vessels were ligated with 10–0 nylon, and the left popliteal lymph node and surrounding fatty tissue were removed. A rectangular silicone splint with a width of 3 mm was fabricated using a 1-mm-thick silicone sheet (Tigers Polymer, Osaka, Japan). This silicone splint was suture-fixed to the skin and muscle of the left groin with 6–0 nylon to create the hind limb lymphedema model. A sham group with only a skin incision around the entire left groin was also created.
Four days after the surgery performed to establish the lymphedema model or the sham with skin incision, a full-thickness skin wound with a diameter of 8 mm was created using a dermal punch (Kai Industries, Seki, Japan) at a site 6 mm distal from the silicone splint on the left hind limb in the lymphedema models or at the same lesion in the sham group (defined day 0 for wounds). The excised skin and subcutaneous tissues were collected for histology and RNA isolation.
Roxadustat and HIF-1α antagonist YC-1 were purchased from Selleck Chemicals (Houston, TX). The roxadustat group received 0.05 mL of roxadustat 25 mg/kg in solvent dimethyl sulfoxide (DMSO; Fujifilm Wako Pure Chemical, Osaka, Japan), 6 the YC-1 group received 0.05 mL of YC-1 30 mg/kg in DMSO, 17 and the control group received 0.05 mL of DMSO intraperitoneally every 2 days for up to 2 weeks, including the day of the surgery performed to establish the lymphedema model. The sham group received 0.05 mL of DMSO intraperitoneally every 2 days for up to 2 weeks, including the day of the surgery creating the skin incision (Fig. 1).
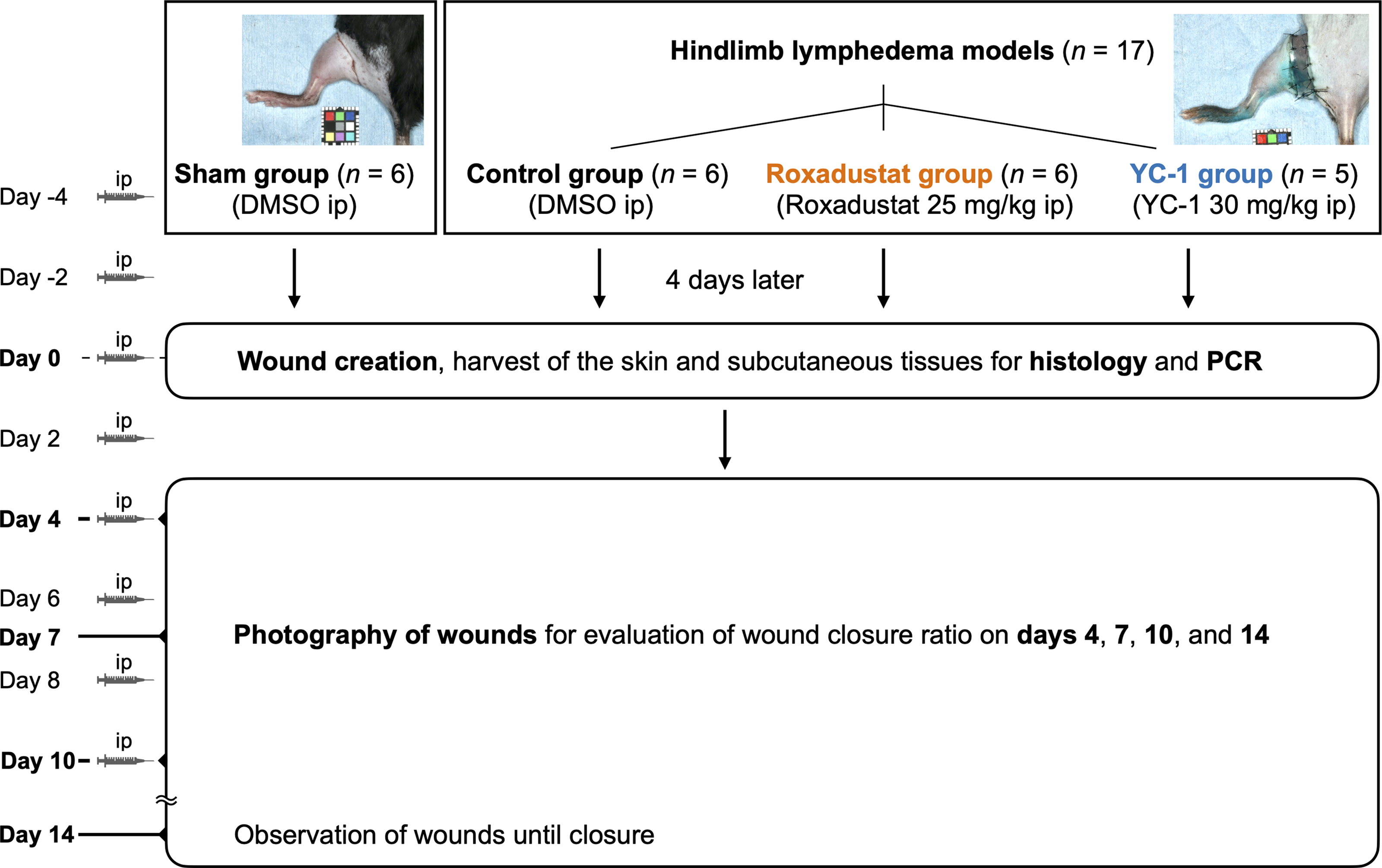
Schematic of the study design. Groupings, n, and time points for drug administration and evaluation. Day 0 was defined as the day of wound creation. ip, intraperitoneal injection.
Evaluation of wound healing in the hind limb lymphedema
The wounds were observed daily, and the number of days until wound closure was recorded. Wound images were captured using a single-lens reflex camera (EOS Kiss X8i; Canon, Tokyo, Japan) equipped with a macro lens (EF 50 mm f/2.5 Compact Macro Lens; Canon) and a close-up strobe (Macro Ring Lite MR-14EX; Canon) on days 0, 4, 7, 10, and 14. The wound area was analyzed using ImageJ software (National Institutes of Health, Bethesda, MD), and the percentage of wound closure was calculated using the following formula: wound closure ratio = [1 − (remaining ulcer area/initial ulcer area)] × 100%.
Evaluation of hind limb lymphedema
The skin and subcutaneous tissues excised during wound creation were immersed in 4% paraformaldehyde phosphate buffer solution (Fujifilm Wako Pure Chemical) and fixed (n = 5 or 6 per group). A whole-slide scanner (NanoZoomer Digital Pathology; Hamamatsu Photonics, Shizuoka, Japan) was used to capture digital images of the slides, which were then visualized using NDP.view2 software (Hamamatsu Photonics).
The degree of edema was evaluated by measuring the skin thickness on hematoxylin and eosin-stained slide sections. With reference to a previous report, 13 the distance from the skin surface to the border between the dermal and subcutaneous fat layers was measured as skin thickness. The distance from the skin surface to the bottom of the basal cells was measured as epidermal thickness. After the specimens were randomized, two examiners (excluding the first author) measured the thickness of the skin in each group by observation, using NDP.view2 software.
Gross lymphedema was assessed from photographs of the hind limb wound images captured on days 0, 4, 7, 10, and 14.
Evaluation of mRNA expression in the hind limb lymphedema
The skin and subcutaneous tissues excised during wound creation were cryopreserved. Extraction of total RNA from the cryopreserved tissues (n = 4 per group) was performed using QIAshredder, RNeasy Fibrous Tissue Mini Kit, and RNase-Free DNase Set (all from Qiagen, Hilden, Germany). Subsequently, reverse transcription was performed to generate cDNA, using High-Capacity RNA-to-cDNA Kit (Applied Biosystems, Foster City, CA). Then, real-time quantitative reverse transcription polymerase chain reaction (PCR) was performed using StepOnePlus Real-Time PCR System (Applied Biosystems) and Power SYBR Green Master Mix (Applied Biosystems), and the ΔΔCt method was applied to calculate the relative levels of PCR products. 13 Each sample was examined in triplicate. A list of the primers used for reverse transcription PCR is presented in Table 1.
Reverse-transcription polymerase chain reaction primer sequences and product size
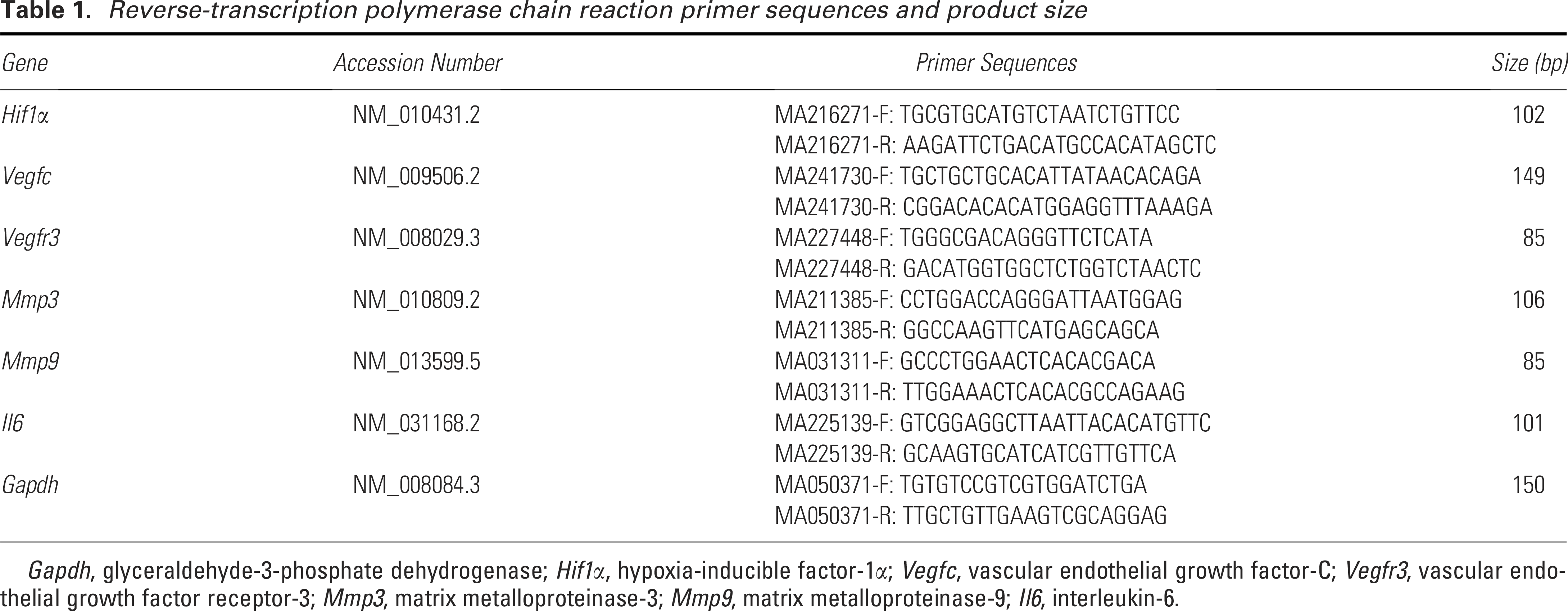
Gapdh, glyceraldehyde-3-phosphate dehydrogenase; Hif1α, hypoxia-inducible factor-1α; Vegfc, vascular endothelial growth factor-C; Vegfr3, vascular endothelial growth factor receptor-3; Mmp3, matrix metalloproteinase-3; Mmp9, matrix metalloproteinase-9; Il6, interleukin-6.
Statistical analysis
Statistical analysis was performed using JMP ver. 18.1.0 (SAS Institute, Inc., Cary, NC). The multiple group tests were performed using one-way analysis of variance followed by the Tukey–Kramer multiple comparisons test. The results are expressed as mean ± standard deviation. A value of p < 0.05 was considered to indicate a significant difference.
RESULTS
Roxadustat accelerated wound healing in the hind limb lymphedema
The length of time required for wound closure was significantly prolonged (p < 0.01) in the control group (12.7 ± 0.8 days), roxadustat group (10.7 ± 1.0 days), and YC-1 group (15.6 ± 0.5 days) compared with the sham group (8.3 ± 1.0 days), but was significantly shorter in the roxadustat group (p < 0.01) and significantly longer in the YC-1 group (p < 0.01) compared with the control group (Fig. 2A, B).
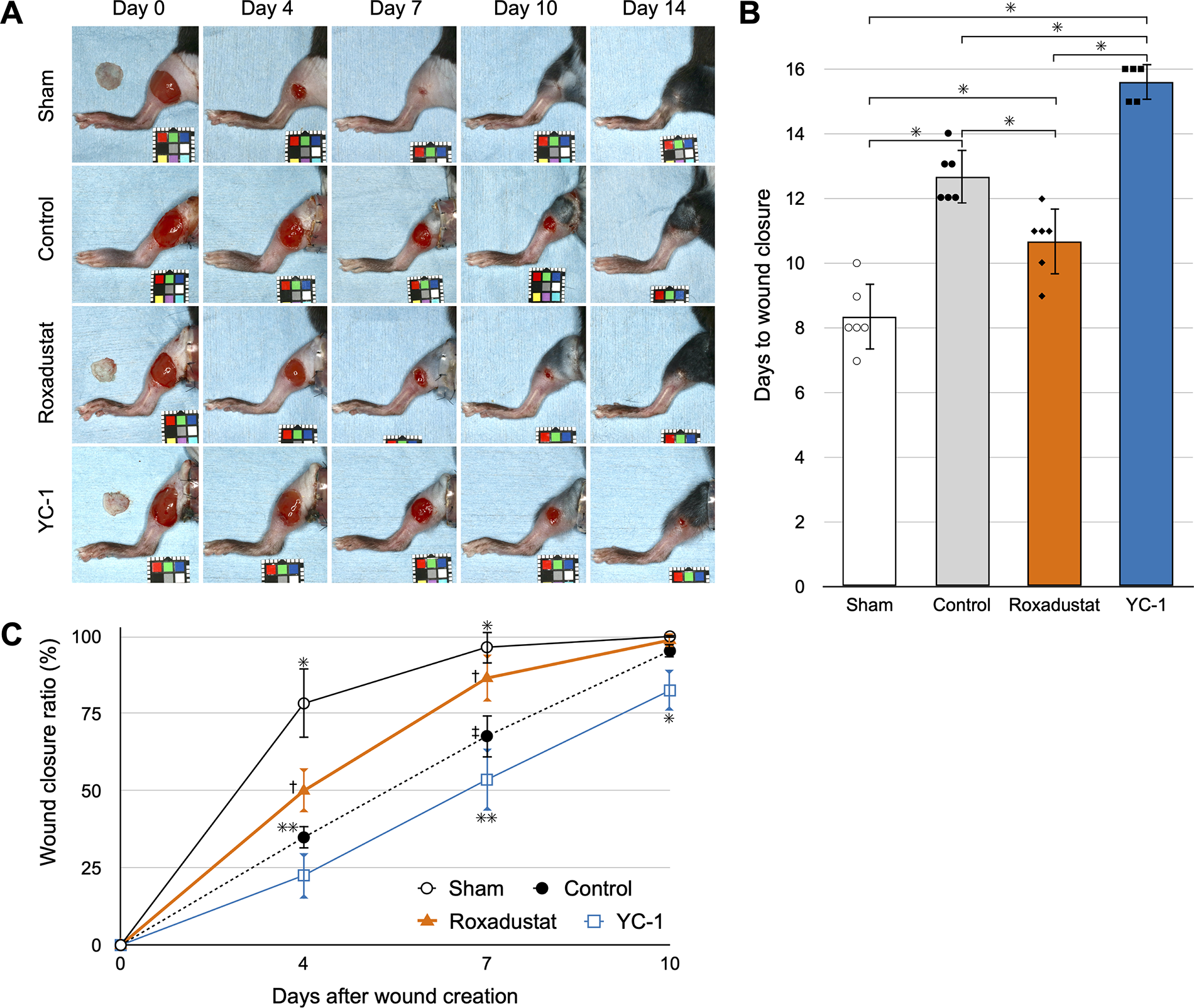
On day 4 after wound creation, the percentage of wound closure was significantly lower (p < 0.01) in the control group (34.9% ± 7.2%), roxadustat group (50.0% ± 3.7%), and YC-1 group (22.6% ± 7.4%) compared with the sham group (78.3% ± 11.3%). The roxadustat group showed a significant increase compared with the control group (p < 0.05), whereas the YC-1 group showed no significant difference (Fig. 2A, C).
On day 7, the percentage of wound closure was significantly decreased (p < 0.01) in the control group (67.7 ± 7.5%) and YC-1 group (53.6 ± 10.3%) compared with the sham group (96.5 ± 5.2%). The percentage of wound closure in the roxadustat group (86.5 ± 7.0%) was significantly increased compared with the control group (p < 0.01), while that in the YC-1 group was significantly decreased (p < 0.05) (Fig. 2A, C).
On day 10, the percentage of wound closure was significantly decreased (p < 0.01) in the YC-1 group (82.4 ± 6.6%) compared with the sham group (100%), control group (95.2 ± 2.1%), and roxadustat group (98.8 ± 2.4%) (Fig. 2A, C).
In addition, compared with the control group, the roxadustat group showed a gross decrease in edema, whereas the YC-1 group showed increased edema. This finding was observed from the time of wound creation to wound closure (Fig. 2A).
Roxadustat decreased skin thickness in the hind limb lymphedema
The mean skin thickness was 197 ± 11.2, 279 ± 8.3, 215 ± 38.8, and 323 ± 13.2 μm in the sham, control, roxadustat, and YC-1 groups, respectively. Compared with the sham group, the control group showed a significant increase in skin thickness (p < 0.01). Compared with the control group, the roxadustat group showed a significant decrease in skin thickness (p < 0.01), and the YC-1 group showed a significant increase in skin thickness (p < 0.05) (Fig. 3A, B).
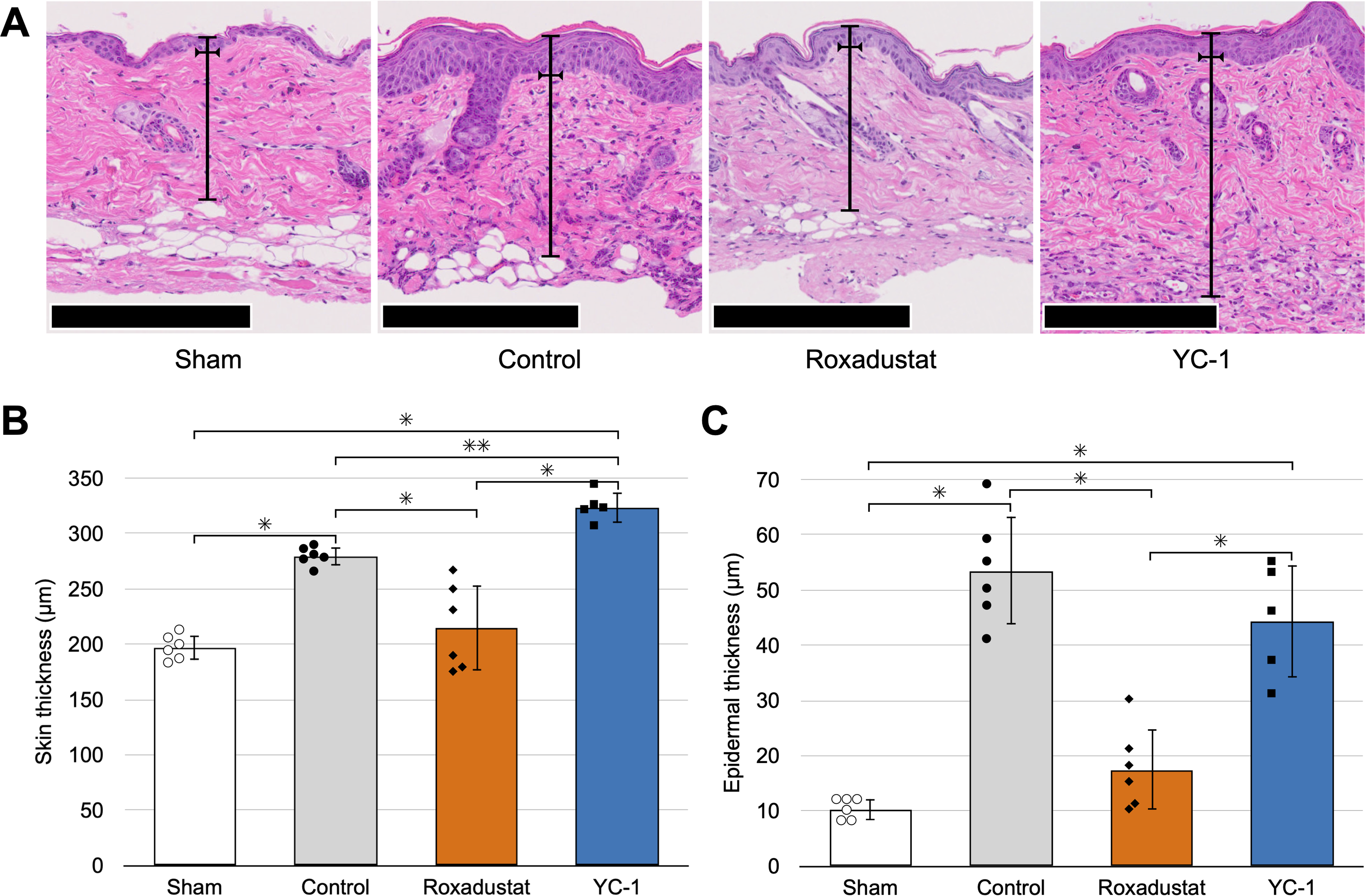
The mean epidermal thickness was 10.3 ± 1.9, 53.5 ± 9.8, 17.5 ± 7.4, and 44.4 ± 10.2 μm in the sham, control, roxadustat, and YC-1 groups, respectively. A similar trend was observed in the epidermal thickness. Compared with the sham group, the control and YC-1 groups showed a significant increase in epidermal thickness (p < 0.01). Compared with the control group, the roxadustat group showed a significant decrease in epidermal thickness (p < 0.01) (Fig. 3A, C).
Roxadustat upregulated Hif1α, Vegfc and Vegfr3 in the hindlimb lymphedema
The relative mRNA expression levels of Hif1α, vascular endothelial growth factor-C (Vegfc), and vascular endothelial growth factor receptor-3 (Vegfr3) were significantly higher in the roxadustat group compared with the control and YC-1 groups (p < 0.05, p < 0.01, and p < 0.01, respectively). However, these expression levels did not differ significantly between the sham and control group (Fig. 4).
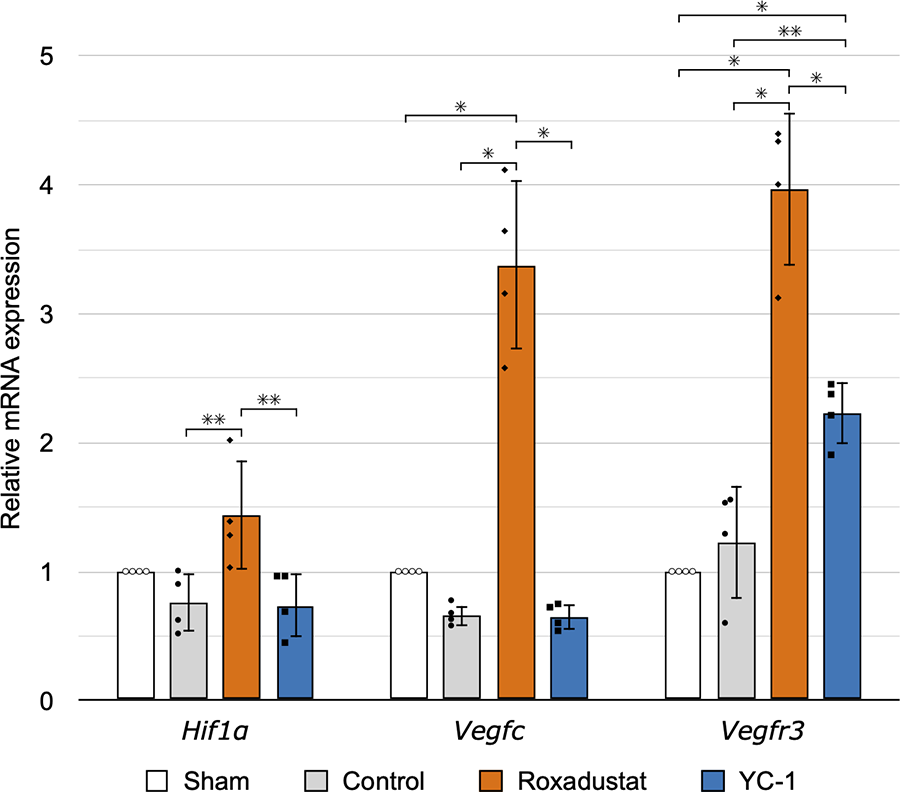
The relative mRNA expression levels of hypoxia-inducible factor-1α (Hif1α), vascular endothelial growth factor-C (Vegfc), and vascular endothelial growth factor receptor-3 (Vegfr3) in skin and subcutaneous tissues excised during wound creation 4 days after the surgery performed to establish the lymphedema model or the sham with skin incision. Data are shown as the mean ± standard deviation. n = 4, *p < 0.01 and **p < 0.05.
Roxadustat upregulated Mmp3 and downregulated Mmp9 in the hindlimb lymphedema
The relative mRNA expression levels of matrix metalloproteinase-3 (Mmp3) and Mmp9 were significantly higher in the control group compared with the sham group (p < 0.01); that of Mmp3 were significantly higher in the roxadustat group compared with the control and YC-1 groups (p < 0.01), whereas that of Mmp9 were significantly lower in the roxadustat and YC-1 groups compared with the control group (Fig. 5; p < 0.01).

The relative mRNA expression levels of matrix metalloproteinase-3 (Mmp3) and Mmp9 in skin and subcutaneous tissues excised during wound creation 4 days after the surgery performed to establish the lymphedema model or the sham with skin incision. Data are shown as the mean ± standard deviation. n = 4, *p < 0.01 and **p < 0.05.
Roxadustat upregulated Il6 in the hindlimb lymphedema
The relative mRNA expression level of interleukin-6 (Il6) was significantly higher in the roxadustat group compared with other groups (p < 0.01) and was significantly higher in the YC-1 group compared with the sham and control groups (Fig. 6; p < 0.01 and p < 0.05, respectively).
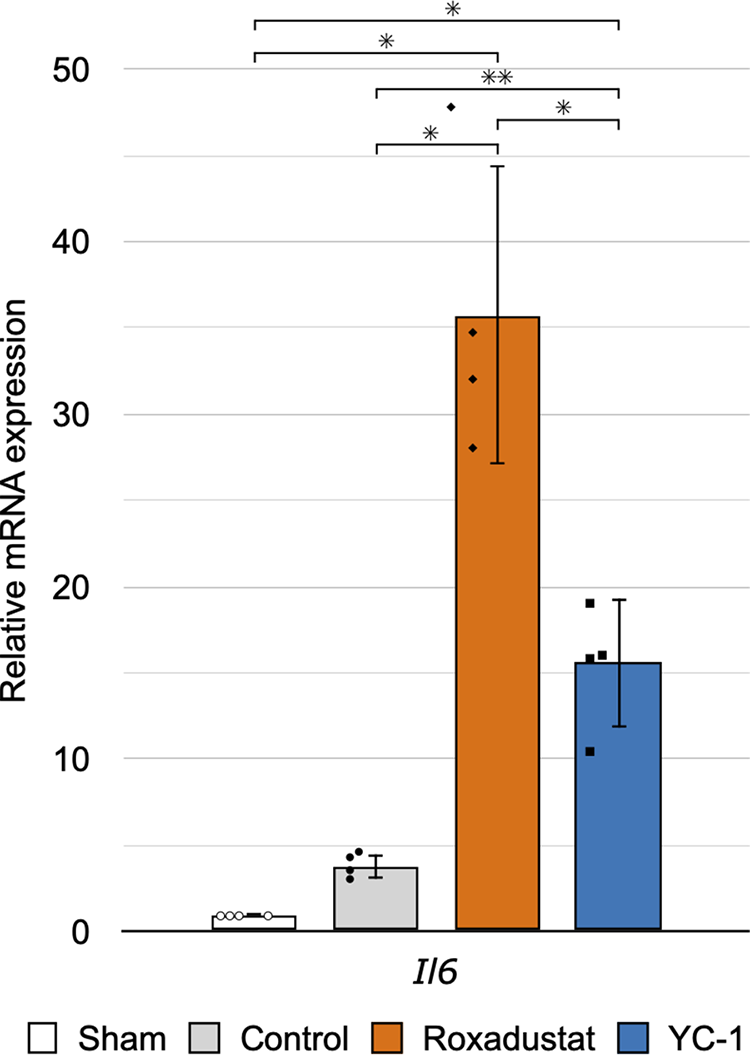
The relative mRNA expression level of interleukin-6 (Il6) in skin and subcutaneous tissues excised during wound creation 4 days after the surgery performed to establish the lymphedema model or the sham with skin incision. Data are shown as the mean ± standard deviation. n = 4, *p < 0.01 and **p < 0.05.
DISCUSSION
Lymphedema models have been created in rabbit ears 18 and mouse tails,7,19 but those models did not involve lymph node excision and did not approximate the pathophysiology of lymphedema in humans. Thus, there has been a need to develop animal models that reflect the dynamics of lymphedema in a more clinically relevant manner.20,21 We developed a model of lymphedema in the hind limbs of mice to study the pathogenesis of lymphatic dysfunction, with the aim of generating a more clinically relevant lymphedema model. 13 The model used in the present study anatomically mimics human lymphedema and is more suitable for wound healing studies compared with our previous mouse model of hind limb lymphedema 22 because it does not require consideration of radiation effects.
A previous study created a mouse model of hind limb lymphedema, using a method different from that in the present study; in that model, a full-thickness skin wound with a diameter of 4 mm was created in the hind limb on the day after the surgery performed to establish the lymphedema model to study the dynamics of lymphatic flow in wound healing, but there was no delayed wound healing due to lymphedema. 23 In the model, the inguinal lymph node and surrounding tissue were excised when creating the mouse hind limb lymphedema, but the popliteal lymph node was not. In addition, the model did not treat the shallow lymph vessels by irradiation or splinting, resulting in a shorter duration of edema. 23 Furthermore, the relatively short wound-healing period due to the 4-mm diameter wound might have precluded a significant difference. 23 To our knowledge, the present study is the first to demonstrate delayed wound healing in a mouse model of hind limb lymphedema through the creation of a full-thickness skin wound with a diameter of 8 mm, which was the maximum size that could be evaluated two-dimensionally in photographs.
In our previous study using the same mouse lymphedema model as in the present study, edema peaked at 4 days after the surgery and persisted for about 1 month, and fluorescent lymphangiography showed that lymphatic flow stasis persisted for about 6 months. 13 Administration of roxadustat and YC-1 to the above wound models accelerated and delayed wound healing, respectively. At the same time, from the prewounding point at 4 days after the surgery to wound healing, the roxadustat group showed improvements in gross edema and significantly decreased skin thickness, whereas the YC-1 group showed worsening of gross edema and significantly increased skin thickness.
HIF-1α coordinates lymphangiogenesis during wound healing as an early response mechanism to hypoxia, inflammation, and lymphatic fluid stasis. 7 Although few studies have investigated the use of HIF-related agents in lymphedema, it was reported that administration of YC-1 in a mouse tail lymphedema model exacerbated edema and decreased lymphangiogenic factors such as VEGF-C, 7 similar to the results of the present study. VEGF-C promotes lymphatic regeneration in the context of wound repair in the mouse tail lymphedema model via VEGFR-3 signaling.7,19 We have previously shown that roxadustat increases mRNA expression of lymphangiogenic factors such as Prospero homeobox 1, Vegfc, and Vegfr3, as well as the number of lymphatic vessels, and also decreases the circumference of the hind limb and improves lymphatic stasis in the mouse model of hind limb lymphedema. 10 In the present study, although the assessment of lymphedema was not quantified due to the presence of the wound, lymphedema also tended to be improved in the roxadustat group, consistent with these results.
Consistent with our previous report in which the skin samples were obtained at 7 days after the surgery performed to establish the lymphedema model, 10 PCR results showed significant increases in Hif1α, Vegfc, and Vegfr3 in the roxadustat group compared with the control group, whereas the YC-1 group showed significantly decreased Vegfr3 compared with the control group, and nonsignificantly decreased Vegfc, consistent with a previous report. 7 Although we previously demonstrated increased expression of VEGF-C and VEGFR-3 in the control group compared with the sham group at 1 to 3 weeks after the surgery performed to establish the lymphedema model, 13 in the present study, the skin and subcutaneous tissues were excised at 4 days after the surgery, which may have been too early to properly evaluate Vegfc and Vegfr3 expression in this hind limb lymphedema model.
Wound healing involves a complex series of interactions among cells, the extracellular matrix (ECM), microenvironments, and molecular signals. 4 Chronic wounds are characterized by persistent inflammation, excessive proteolytic activity from MMPs, compromised ECM deposition, and the lack of a proliferative phase. 24 HIF-1α activity is impaired in diabetes characterized by impaired wound healing. 25 Fibroblast-restricted HIF-1α knockout mice are reported to exhibit delayed wound healing. 26 Drugs that block HIF-1α hydroxylation have been found to be beneficial in improving wound healing in diabetic mice. 27 Among the HIF-PHD inhibitors, intraperitoneally administered roxadustat is reported to promote angiogenesis via activation of the HIF-1α/VEGF signaling pathway, leading to improved wound healing in diabetic rats 6 or enhanced skin flap survival in rats. 28 HIF-1α is a master regulator that controls the expression of various growth factors and cytokines that organize the different phases of wound healing, including inflammation, angiogenesis, and reepithelialization. 12
MMP3 is known to be an early responder to tissue injury, and during the inflammatory phase of wound healing, it plays an active regulatory role by degrading the ECM and inducing leukocyte infiltration, thereby promoting the anti-inflammatory response and transitioning to the proliferative phase.29,30 In addition, it has been reported that the expression of MMP3 may be regulated by HIF-1α.31,32 MMP9 is also involved in the reorganization of the ECM during the wound-healing process as a primary gelatinase, and its overexpression in the wound microenvironment weakens granulation tissue formation and inactivating growth factors, thereby inhibiting wound healing in diabetic rats. 33 Overexpression of MMP9 has also been reported in more severe and infected diabetic foot ulcers compared with nondiabetic controls in humans. 34 The inflammatory phase of wound healing is administered by macrophage-derived reactive oxygen species, 11 which are known to upregulate MMP9. 35
The multifaceted cytokine IL-6 is also involved in wound healing, and studies have reported delays or impairment of wound healing in IL-6 knockout mice.36,37 In addition, HIF-1α upregulates IL-6 expression by binding to its promoter region, thereby promoting inflammation and cell proliferation. 29
In the present study, we found that mRNA expression of Mmp3 and Mmp9 was significantly increased in the control group compared with the sham group. The mRNA expression of Il6 also increased, but the difference was not significant. Given that MMP3 and MMP9 are ECM remodeling genes,29,33 the observed increase in their mRNA expression may indicate acute inflammation in lymphedema. In addition, the mRNA expression of Hif1α, Mmp3, and Il6 was significantly increased in the roxadustat group compared with the control and YC-1 groups, whereas the expression of Mmp9 was significantly suppressed compared with the control group. Roxadustat may upregulate MMP3 and IL-6 through the induction of HIF-1α, thereby promoting wound healing in lymphedema. Overexpression of MMP9 is known to inhibit wound healing, and roxadustat may suppress the overexpression of MMP9 in lymphedema and contribute to ECM remodeling. Similarly, it has been reported that hyperbaric oxygen therapy promotes wound healing by decreasing MMP9 in diabetic mice. 38
In conclusion, the findings of the present study indicate that roxadustat plays a role in the regulation of ECM-remodeling gene expression in hind limb lymphedema wound models and exerts wound-healing effects during the inflammatory and proliferative phases. The findings of this study suggest that the lymphedema-improving effect of roxadustat also has an impact on the promotion of wound healing.
There are several limitations and important issues that should be considered regarding the findings of this study. First, the mouse model of hind limb lymphedema examined in this study does not address chronic lymphedema as observed in humans. Second, wound healing is affected by various factors in lymphedema, including the wound size and the mechanical stress applied to the wound. Third, wound healing in mice has been reported to be more prone to wound contraction and less prone to granulation and epidermal formation compared with humans, 39 and skin stretching due to circumferential changes in hind limb circumference might have a significant effect on wound healing without wound stenting. Fourth, to evaluate wound healing in lymphedema during the drug treatment of lymphedema, drug administration was initiated 4 days before wound creation, so the baseline condition of the wound differed according to the group. Finally, the skin and subcutaneous tissues were harvested only at the time of wound creation, and thus, mRNA expression was not evaluated over time. Further research is necessary to clarify the mechanism of action of roxadustat for wound healing in lymphedema.
KEY FINDINGS
Delayed wound healing was demonstrated in a mouse model of hind limb lymphedema. Roxadustat promoted wound healing, whereas the HIF-1α inhibitor YC-1 delayed it. Roxadustat regulated the mRNA expression of Mmp3, Mmp9, and Il6, which were involved in wound healing.
INNOVATION
The lack of standardized and optimized animal models of lymphedema has hindered research into the dynamics of lymphedema and its complications, including delayed wound healing.13,20 Because there is no curative treatment for these complications, new treatments are urgently needed. In this study, we used a radiation-free mouse model of hind limb lymphedema to show that wound healing in lymphedema is delayed compared with that in nonlymphedema and that wound healing is accelerated by the administration of roxadustat, a HIF-1α stabilizing agent. Drug therapy for wound healing in lymphedema has not been investigated previously, and these findings may contribute to advances in drug therapy.
Footnotes
ACKNOWLEDGMENT AND FUNDING SOURCES
The authors would like to thank Kohei Oashi and Daisuke Iwasaki for advice regarding this study. This study was funded by the
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.