
Abstract
Objective:
Platform studies are an innovative clinical trial design to evaluate multiple potential therapies simultaneously using a master protocol framework for more rapid discovery of critical new disease-modifying therapies. Initially pioneered in cancer clinical trials, platform studies have more recently been adopted for new vaccine trials and other disease states. This approach has not been used for biomarker(s) validation.
Approach:
We present the development and successful implementation of a master protocol for a platform study in the National Institute of Diabetes and Digestive and Kidney Diseases Diabetic Foot Consortium (DFC) that concomitantly tests multiple biomarkers that could be used to predict diabetic foot ulcer (DFU) healing outcomes in people with DFUs.
Results:
This flexible master protocol, allowing the study of multiple biomarkers in a perpetual manner, designed to be inclusive of a broad spectrum of people with DFUs operating under the mantra “No DFU Goes Unstudied” successfully collects participant data and biospecimens for biomarker development and validation in a standardized manner across multiple DFC sites.
Innovation:
Integrating multiple biomarkers with a rich database of participants’ clinical characteristics, patient-reported outcomes, and standard of care practices at various sites collected longitudinally over 52 weeks following a pragmatic approach and thus relevant to people with DFU as seen in today’s daily practice, enable their subsequent implementation at the point of care to guide timely personalized DFU management decisions.
Conclusion:
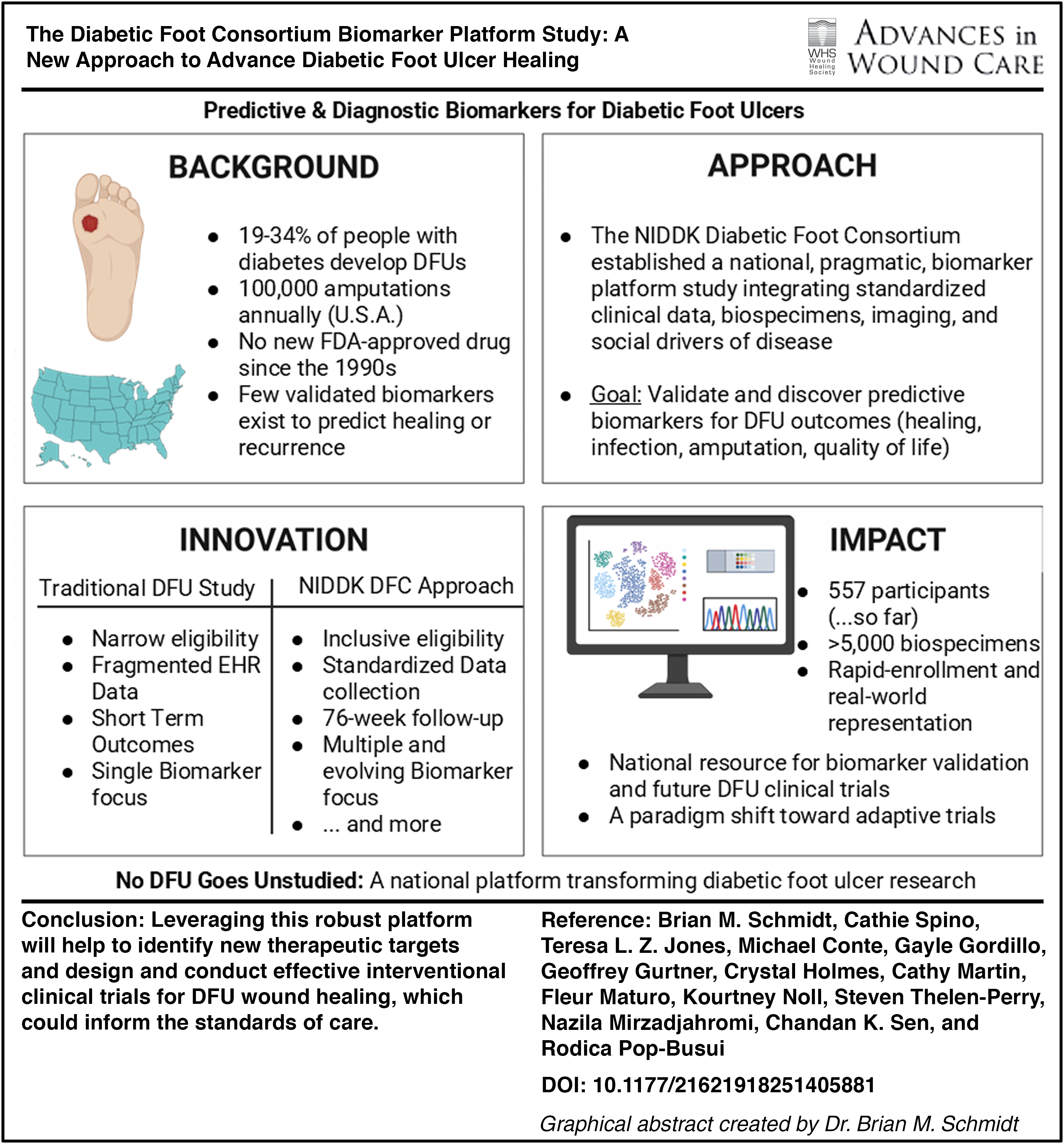
Leveraging this robust platform will help to identify new therapeutic targets and design and conduct effective interventional clinical trials for DFU wound healing, which could inform the standards of care.
Cathie Spino, ScD
INTRODUCTION
Diabetic foot ulcers (DFUs) have an estimated global burden of 19–34% of people with diabetes worldwide. 1 More than 1.6 million people are diagnosed with a DFU, and >100,000 amputations secondary to a nonhealing or infected DFU are performed each year in the United States. 2 People with DFUs face the burden of long-term treatments, a 20–30% risk of nonhealing and a 60% risk of infection.1,3,4 The considerable advances in understanding the biology of diabetic wound healing have not translated to effective therapies with the last drug therapy approved by the U.S. Food and Drug Administration (FDA) in the late 1990s. 5 The paucity of validated biomarkers for DFU healing that can be used in clinical trials for targeted entry criteria and monitoring therapy effectiveness has contributed to the difficulties of DFU therapy development. Another factor is clinical trial design that often has very narrow inclusion criteria, which make recruitment difficult and the results less relevant and generalizable for the broader DFU population.
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)-funded Diabetic Foot Consortium (DFC) was established to improve the clinical study of DFUs by building a clinical research network to validate and develop DFU biomarkers with the eventual goal of conducting clinical trials for innovative DFU therapies. The DFC consists of multiple academic clinical sites, a Data Coordinating Center (DCC), and biomarker analysis units. 6 The DFC is committed to and has achieved recruitment of people with DFUs that reflects the diversity of Americans suffering from DFUs, as currently seen in daily practice, including those from rural and/or underserved locations. 7 In addition, the DFC expanded its research scope to include studying the role of social drivers of diabetic foot disease (SDDFD), such as food insecurity, housing instability, limited health literacy, and poor social support, as well as by engaging with a broad spectrum of communities and wound care stakeholders.
The DFC initiated and completed two biomarker studies using the traditional approach of a single protocol for each biomarker. The c-myc study evaluated whether the nuclear localization of c-myc and phosphorylated glucocorticoid receptor could predict DFU healing. 8 The transepithelial water loss (TEWL) study tested whether the measurement of TEWL could predict DFU wound recurrence. 9 The DFC also initiated a biorepository protocol to collect biosamples from each of these protocols. From these experiences and the NIDDK funding announcement for studies to develop biomarkers using the DFC infrastructure, the DFC decided to pursue a platform approach 6 —the Predictive and Diagnostic Biomarkers for Diabetic Foot Ulcers: Open Wound Master Study (NCT06104969)—to capitalize on this clinical study design, to better leverage DFC resources, and to achieve the vision of “No DFU Goes Unstudied.”
Master protocols, initially pioneered in cancer clinical trials, are defined as “one overarching protocol designed to answer multiple questions”10–15 with multiple substudies. They are well suited for biomarker studies where the data and biosamples collected in a common protocol can be distributed for multiple biomarker investigations of a single disease. Their use in a clinical research network, such as the DFC, allows for extensive substudies within the master protocol framework to optimally understand biomarker performance characteristics and to propose biomarker cutoff values to characterize good and poor clinical outcomes. Therefore, this innovative and rigorous approach represents a paradigm shift for DFU studies and provides a robust framework to support new and personalized clinical care practices and improve the care of all people with DFUs.
CLINICAL PROBLEMS ADDRESSED
The Open DFU Platform Study evaluates a highly relevant clinical problem, given the high prevalence and serious consequences of the DFU through several features that address challenges in DFU research.
Examples of recent additions to the master protocol are a substudy on pedal medial artery calcification scores as a predictor for wound healing that requires collection and reading of foot X-rays, as well as incorporating biophysical sensors to measure wound temperature, oxygen saturation, and wound impedance, and adding new CRFs to collect major adverse cardiovascular events (new clinical data) for a subset of participants.34–42 This is just another example on how the flexibility of this platform study design can address multiple scientific questions simultaneously, incorporate pilot studies, and reduce the time, cost, and sample size required to reach definitive conclusions as compared with individual “umbrella-style” designed studies that are traditional for trials in this space (i.e., for trials of multiple drugs in one disease) and allows for adaptation to meet the demands of future scientific discovery.
MATERIALS AND METHODS
The DFC master protocol was designed with a high level of pragmatism and the ability to enroll the vast majority of DFUs participants, as seen in daily practice. It is thus poised to answer multiple scientific and clinical questions simultaneously and adapt to make the most efficient use of study funds and participants. By collecting a large set of biospecimens in a standardized fashion and characterizing many participants and DFU features, it has the potential to inform and facilitate future clinical trials.
Eligibility
Briefly, the master protocol is open to all individuals with an Open DFU with few exclusion criteria (Table 1). These eligibility criteria maximize the opportunity for patients with DFUs to participate in the study during their clinical visit. The rationale behind having broad inclusion criteria is to evaluate any type of DFU across the spectrum of care, including infection and osteomyelitis. The few exclusion criteria include the presence of gangrene, WIfI ischemia grade 3, planned revascularization, and ongoing participation in a DFU clinical trial because these may confound the protocol’s outcomes on DFU healing. 44
Inclusion and exclusion criteria
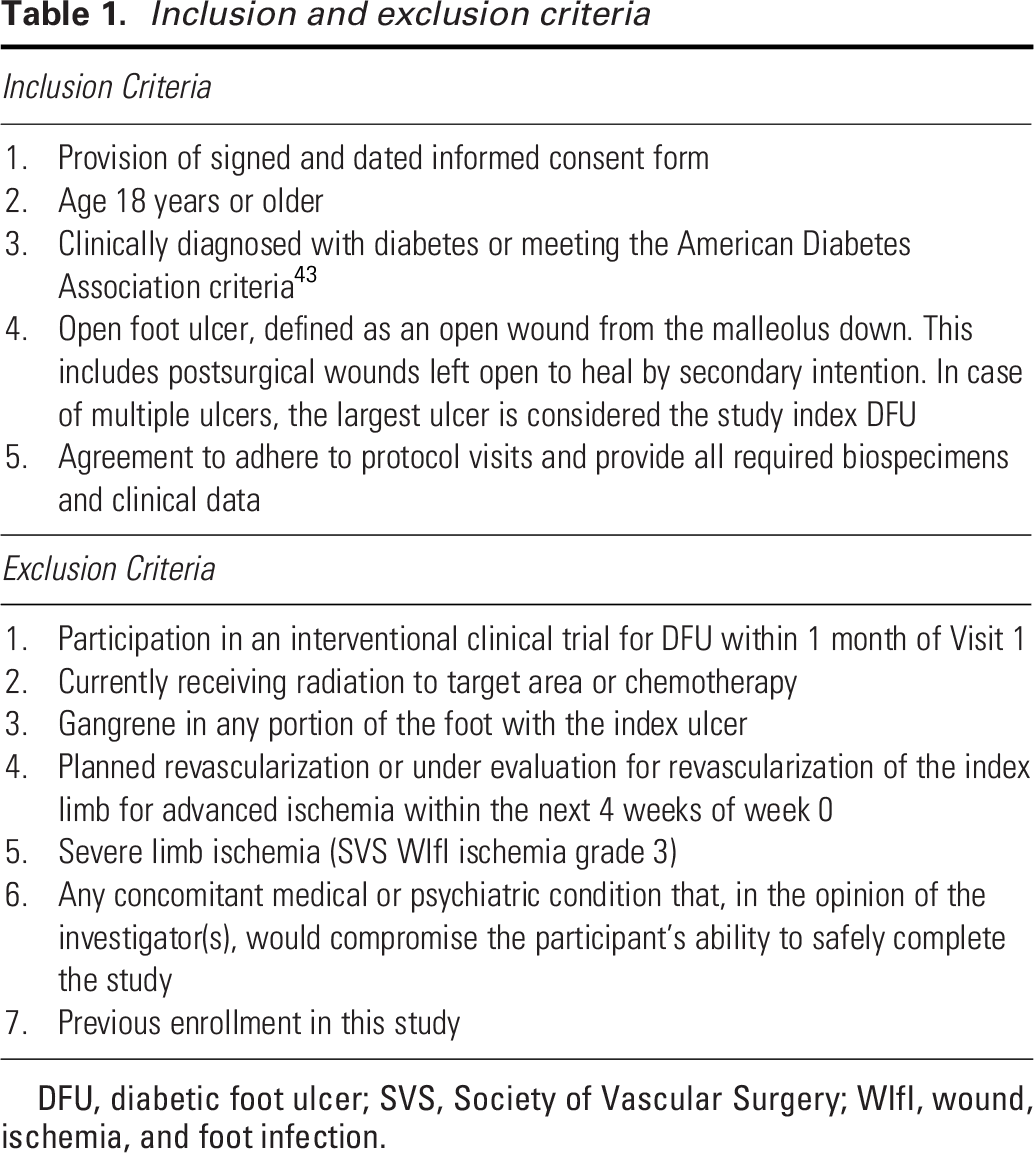
DFU, diabetic foot ulcer; SVS, Society of Vascular Surgery; WIfI, wound, ischemia, and foot infection.
Data elements collected at study visits
At the baseline visit, a comprehensive set of data is collected on demographics, medical and wound history, quality of life, social factors, physical exam, and wound images. Wound debridement tissue, fluid and dressings, as well as blood are collected at baseline and at the week 4 visit; urine collection, although optional given potential participants’ burden, is also recommended for collection at baseline and at the week 4 visit. Participants are evaluated at week 2 and week 4 and monthly thereafter until week 52 or complete wound closure, which is defined as skin re-epithelization without drainage or dressing requirements at two consecutive visits 2 weeks apart. 45 In addition, as suggested by the Observational Safety Monitoring Board for the DFC, we included follow-up on index DFC wound recurrence in participants who healed at week 78. The protocol collects extensive participant data, including demographics, laboratory data, medications, comorbidities, SDDFD, and PROs, providing a comprehensive profile of DFU participants (see Fig. 1). PROs collected through the master protocol, including measures of neuropathy, sleep disturbance, and quality of life, can inform the design of future clinical trials by identifying patient-centered endpoints and guiding individualized intervention strategies. SDDFD data may be incorporated into predictive models by stratifying participants by socioeconomic, geographic, and social support factors, allowing for weighting of these variables to better understand disparities in DFU healing and to develop personalized care pathways.
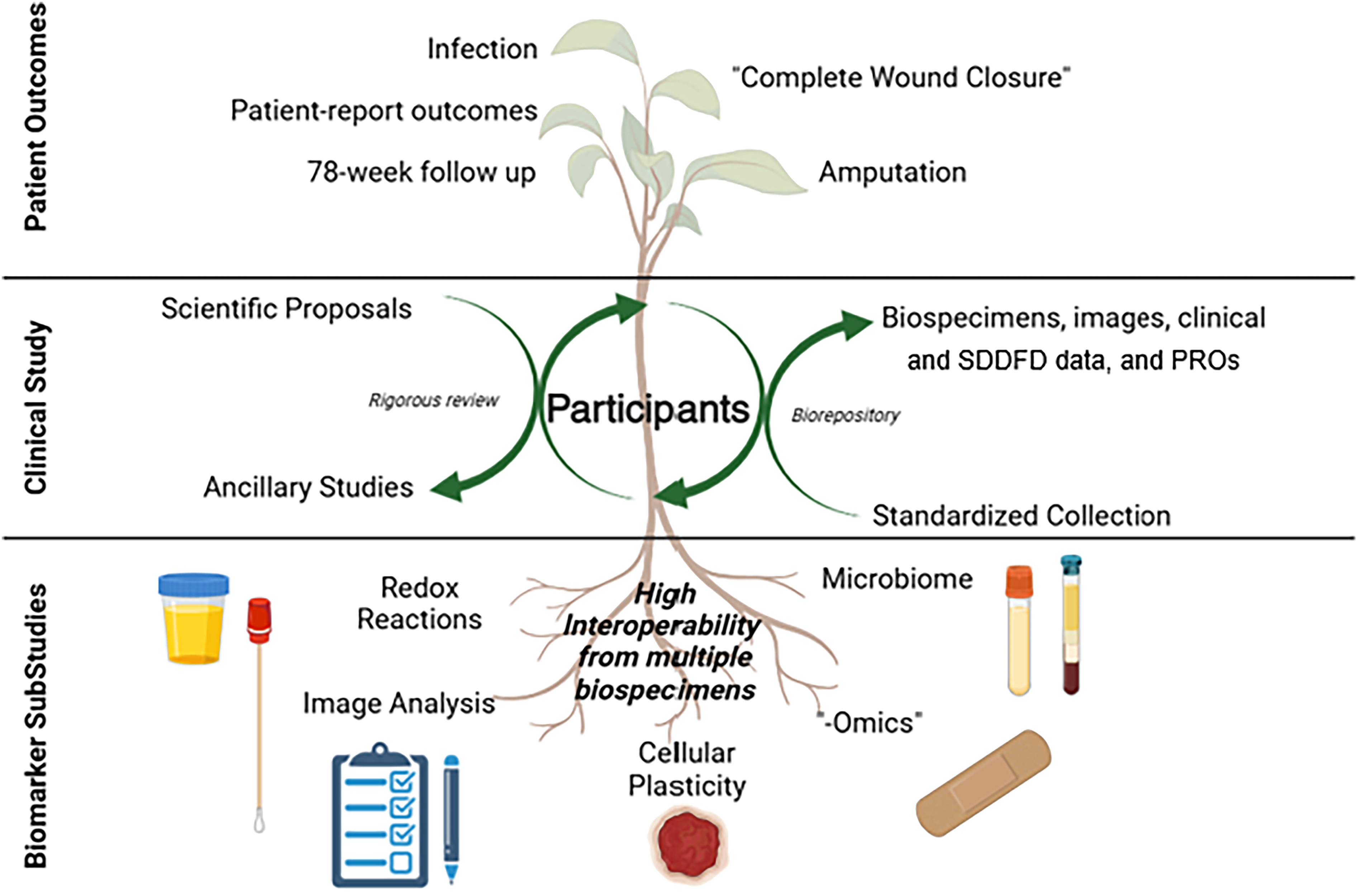
Organizational elements of the Diabetic Foot Consortium’s “Predictive and Diagnostic Biomarkers for Diabetic Foot Ulcers: Open Wound Master Study.” DFU, diabetic foot ulcer; Omics, branches of science; PRO, patient-reported outcome; SDDFD, social drivers of diabetic foot disease.
Endpoints
Several key endpoints are assessed that include (Table 2): proportion of participants with complete wound healing (as defined above) by week 52; proportion of participants who develop infections of the index DFU among those with no infections at baseline; proportion of participants who have an amputation of the limb associated with the index DFU; time to healing; and a broad battery of PROS including change in baseline to later of 52 week or confirmation visit in SF-12 Physical and Mental domain scores, 26 Diabetic Foot Ulcer Short Form subscores, 24 and PROMIS Sleep Disturbance scores, 25 see Figure 2 for the study schema and the Supplementary Tables S1 and S2 for protocol and endpoint details.
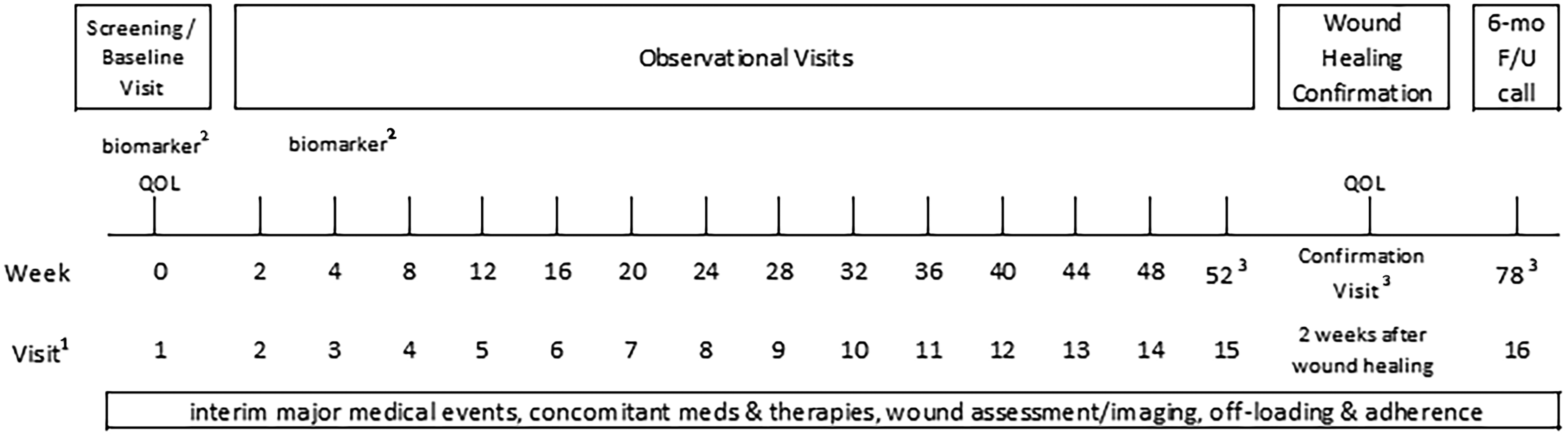
Study schema for the platform study of open diabetic foot ulcers. 1Most study visits are in-person clinic visits, except as otherwise indicated in the protocol. 2Biomarkers include blood, wound fluid, wound dressings, wound debridement (as clinically indicated), and urine (optional but encouraged). 3For participants whose DFUs have healed prior to week 52, a phone call or video visit should occur at week 52 and 78 to assess recurrence and wound status. For participants whose DFUs have healed at week 52, a phone call or video visit should occur at week 78 to assess recurrence. For participants whose DFUs have not healed by 52 weeks, a 6-month phone call or video visit should occur to assess healing and wound status. DFU, diabetic foot ulcer; F/U, follow-up; meds, medications; QOL, quality of life.
Core primary and secondary endpoints
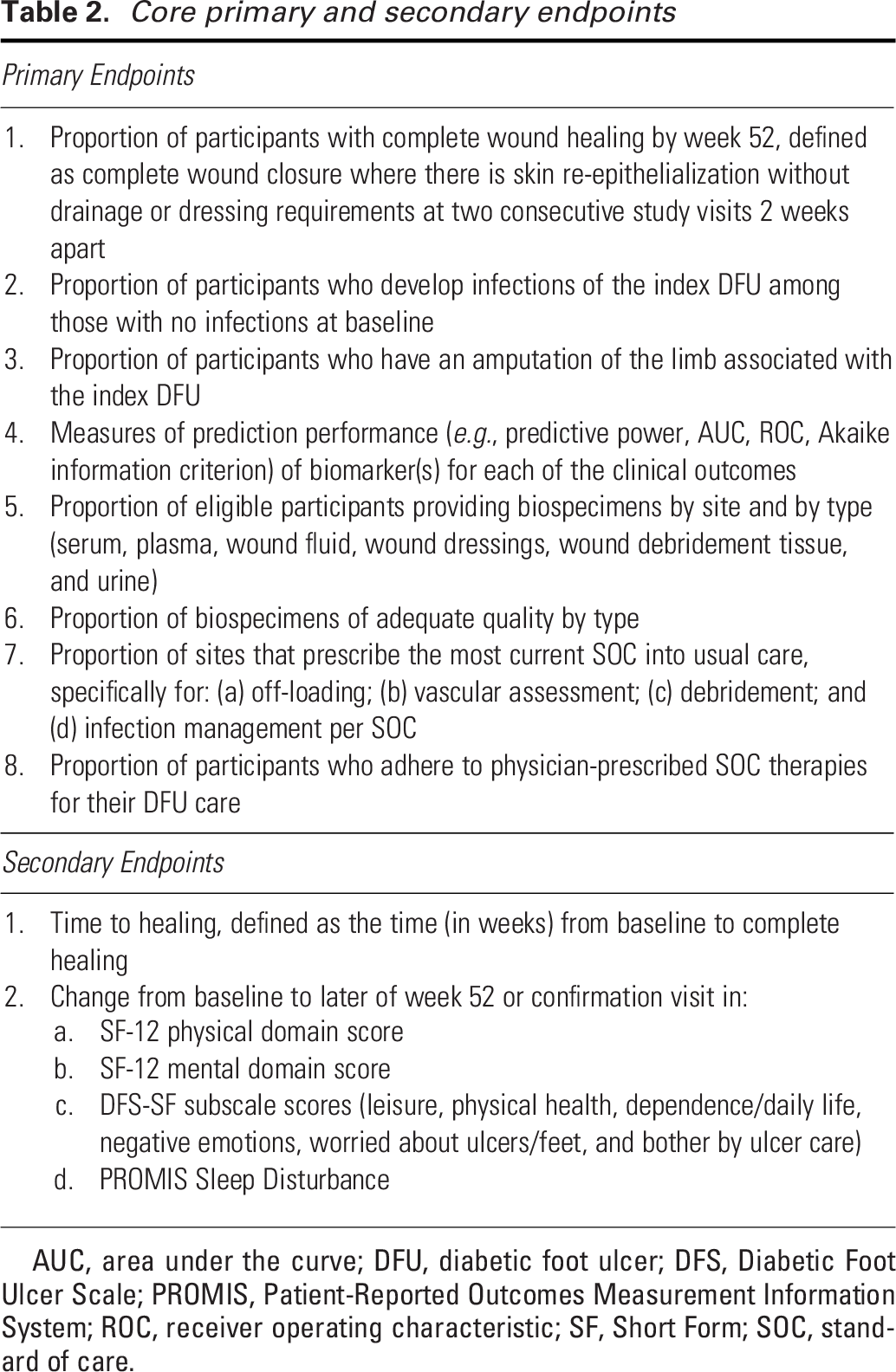
AUC, area under the curve; DFU, diabetic foot ulcer; DFS, Diabetic Foot Ulcer Scale; PROMIS, Patient-Reported Outcomes Measurement Information System; ROC, receiver operating characteristic; SF, Short Form; SOC, standard of care.
RESULTS
Seven clinical sites have been activated in the Open DFU Platform Study: University of California San Francisco, UM, University of Pittsburgh, University of Arizona, Beth Israel Deaconess Medical Center, Northwell Health, and University of Southern California. Since the first participant was enrolled in June 2023, DFC enrollment has reached 557 DFU participants and yielded over 5,000 biospecimens as of July 2025 (Table 3). Sixteen percent of participants have completed the study per protocol, of which 7% completed the 6-month follow-up call (week 72). Participants have completed 3,135 visits for which clinical research coordinators have entered 25,110 CRFs, with more than 75% entered within 3 days and an overall median timeliness of data entry of 0 days (i.e., data were entered on the date of the visit). These clinical research data and biospecimens are currently used in one K23 grant, five R61/R33 grants, five ancillary studies, three supplements, six ancillary analyses, and one substudy. The work done to date across the biomarker validation projects included in the master protocol has resulted in 11 presented abstracts at national and international meetings and 7 manuscripts. Thus, in <2 years since the first participant enrollment, the DFC master protocol has provided the foundation for abstracts and manuscripts that deliver critical insights into biomarkers and healing in a diverse set of DFU individuals.
Baseline characteristics in the Diabetic Foot Ulcers Open DFU Platform Study. All eligible participants
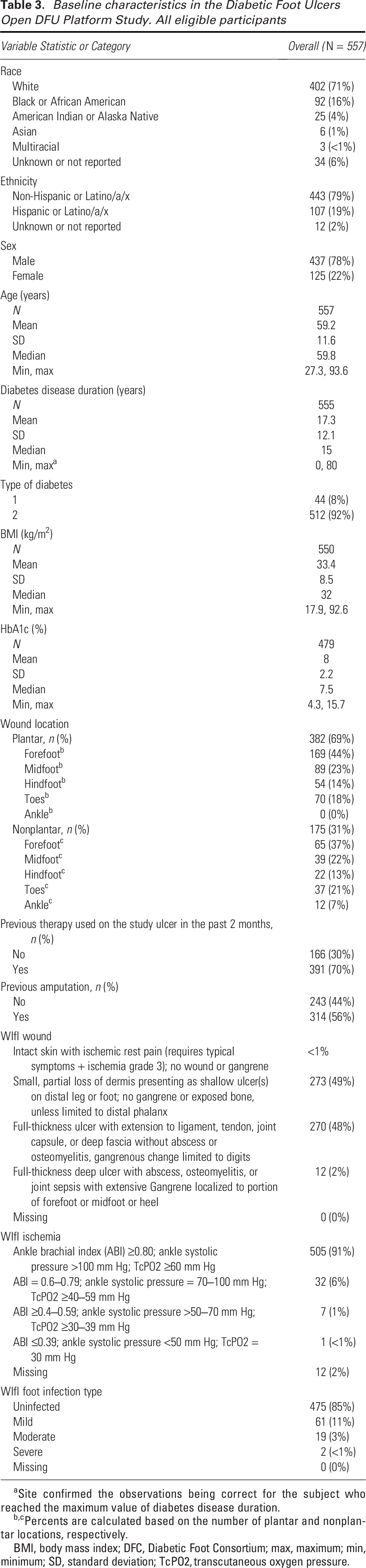
Site confirmed the observations being correct for the subject who reached the maximum value of diabetes disease duration.
Percents are calculated based on the number of plantar and nonplantar locations, respectively.
BMI, body mass index; DFC, Diabetic Foot Consortium; max, maximum; min, minimum; SD, standard deviation; TcPO2, transcutaneous oxygen pressure.
DISCUSSION
Two types of innovation are hallmarks of master protocols: the use of a trial network with infrastructure in place to streamline trial logistics, improve data quality, and facilitate data collection and sharing; and the use of a common protocol that incorporates novel statistical approaches to study design and data analysis, enabling a broader set of objectives to be met more effectively and timely than would be possible in independent trials. 11 The DFC master protocol includes both and represents a paradigm shift in the approach to clinical study of DFUs by being inclusive of all DFU patients—significant strengths of this design. Rather than studying a single question (e.g., does a product lead to improved healing time, or does this biomarker predict complete wound healing) or a specific patient population (e.g., Wagner grade 1 DFU), our biomarker platform study approach studies the whole spectrum of DFUs (see Supplementary Fig. S2). The infrastructure developed in the NIDDK DFC and now the Open DFU master protocol can be used to address multiple questions in parallel and be nimble to incorporate new questions as biomarkers and therapies advance. In taking a pragmatic approach to the SOC being followed in distinct and diverse geographic locations, our robust and standardized ICF, data collection, and safety reporting processes position us to address future efforts, such as embedding clinical trials within usual health care and creating learning health care systems. DFUs with their accompanying infections and amputations are common, costly, and deadly, and we hope that the adaptive biomarker platform study approach detailed here can be an exemplar for future investigations of other chronic disease states.
Case vignette
“A 62-year-old man with type 2 diabetes presents with a 2.5 cm plantar ulcer of 6 weeks’ duration on his right foot. Baseline assessment using a validated biomarker panel at the point of care featuring an elevated inflammation index and upregulated CCL28 chemokines identifies him as a high-risk non-healer. Using this information, the clinician applies more intensive personalized care earlier by initiating advanced wound therapies that include the use of cellular and tissue-based products immediately, continued aggressive off-loading with a DH off-loading shoe given the patient’s requirement to drive for work, and coordinating multidisciplinary follow-up, which included assessment with vascular and infectious diseases specialists. As a result, the ulcer demonstrates accelerated healing and closes by week 15, avoiding infection or further invasive interventions. This scenario illustrates how predictive biomarkers could enable timely, personalized interventions to promote wound healing and prevent complications.”
Limitations
Although the platform approach has many advantages, there are some limitations. Broad inclusion criteria and multiple substudies necessitate rigorous regulatory and ethical oversight, including comprehensive informed consent and monitoring for participant safety. Potential variability introduced by site-specific SOC practices is mitigated through standardized data collection, central training, and analytical methods that account for site and treatment heterogeneity. It requires sufficient funding to support the development and maintenance of the research infrastructure, and it is not well suited for individual center clinical trials. In addition, if proposed substudies are sufficiently different from the current platform design, it may be more efficient to start additional studies—whether traditional or alternative platform studies—rather than adapt the current platform study. For example, new endpoints such as ulcer-free days in remission 46 would likely require a change in the schedule of study visits to reflect the SOC differences from open to closed wound to recurrence and differences in collection methods (e.g., coordinator vs. patient) that would not fit easily into our current platform study design. New clinical outcomes that reframe the characterization of DFUs as healed or recurrent wounds within a framework of remission (as used in cancer care) could anchor biomarker discovery and validation to meaningful patient-centered outcomes, with the potential to ensure that advances translate into durable improvements in daily life and long-term health. The DFC encourages proposals to investigate such new scientific directions in collaboration with DFC investigators; more information about the proposal process is available at https://diabeticfootconsortium.org/researchers/.
In summary, the Predictive and Diagnostic Biomarkers for Diabetic Foot Ulcers Open Wound Master Study offers significant advantages for accelerating effective biomarker(s) validation and complex data integration for advanced modeling for wound healing, improving study efficiency, particularly in a complex and heterogeneous disease such as DFUs. The knowledge garnered from this study poises us to help design new interventional trials and personalized care approaches. The DFC team is actively monitoring and refining its implementation, including carefully considering logistical, regulatory, and statistical challenges to ensure validity, reproducibility, and success.
INNOVATION
With up to 5,000 U.S. participants followed for up to 78 weeks, the study is the largest to provide prospective data on DFU healing in real-world settings. The Open DFU Platform Study broader inclusion criteria (including individuals with infections or osteomyelitis) increase its relevance. The flexible protocol accommodates new substudies. Integration with SOC practices reduces participant burden. The use of the WIfI classification system18,44 replaces outdated risk prediction models. Multiple prespecified biomarkers (Table 4), wound imaging, and clinical data are standardized and integrated using advanced statistical approaches, enhancing predictive capabilities, and enabling evaluations of novel biological healing pathways.
Prespecified biomarkers studied in the Diabetic Foot Ulcers Open DFU Platform Study
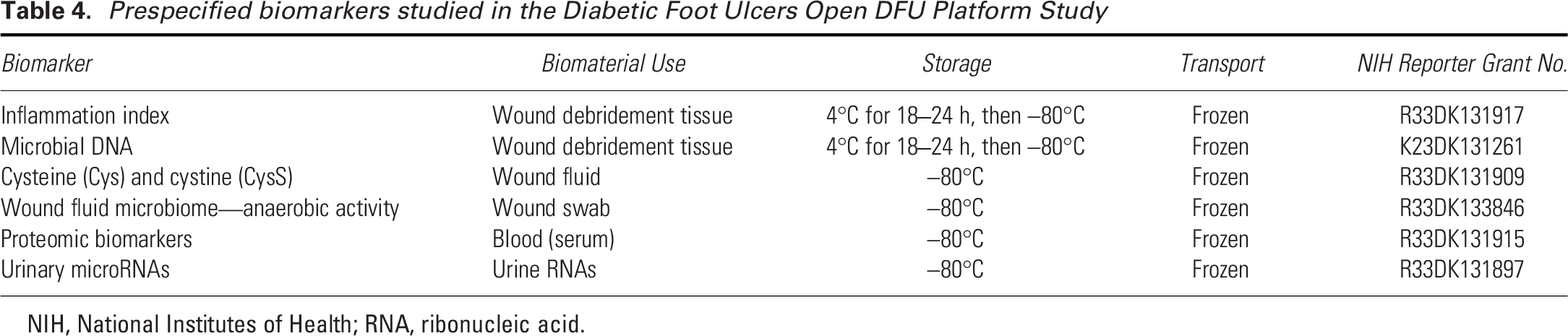
NIH, National Institutes of Health; RNA, ribonucleic acid.
KEY FINDINGS
Platform studies are an innovative clinical trial design to evaluate multiple potential therapies simultaneously. The DFC has successfully applied the platform study approach to biomarkers of DFU healing by implementing and continuing to enroll participants in the first-ever master protocol for DFUs. Over 500 participants have been enrolled, and thousands of unique data points, including links to biospecimens, are now available as a result of this national effort.
ACKNOWLEDGEMENTS AND FUNDING SOURCES
The authors would like to thank all the participants with DFU who have generously given their time to participate in DFC studies. The authors thank the NIDDK Project Officers, Henry Burch, MD and Yan Li, PhD, for study guidance, as well as all investigators, coordinators, and data coordinating staff listed in the Supplemental Acknowledgments.
This study was conducted by the NIH-sponsored DFC supported through Grant IDs U01DK119100, U01DK119083, U01DK119094, U01DK119099, and U24DK122927 of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK).
AUTHORS’ CONFIRMATIONS
B.S.: Writing—original draft, writing—review and editing, supervision, and funding acquisition. C.S.: Conceptualization, methodology, formal analysis, writing—review and editing, supervision, and funding acquisition. R.P.-B.: Conceptualization, methodology, writing—review and editing, supervision, and funding acquisition. C.S., B.S., and R.P.B. designed the MP. B.S. and R.P.B. drafted the article. B.S., C.S., R.P.B., M.K., G.G., and T.L.Z.J. participated in finalizing the MP. All authors have reviewed and approved the final version of the article.
AUTHOR DISCLOSURE AND GHOSTWRITING STATEMENT
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article. The content of this article was expressly written by the authors, and no ghostwriters were used.
Footnotes
ABOUT THE AUTHORS
Supplemental Material
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.