
Abstract
Zebrafish (Danio rerio) are often anesthetized by immersion in buffered tricaine methanesulfonate (MS-222). Although commonly utilized, immersion anesthesia presents a shortcoming of lethal asphyxiation with increased duration of exposures. A newer technique that circumvents this issue, known as flow anesthesia, has been adapted from larger aquatic species to zebrafish. Flow anesthesia improves safety by delivering oxygen-rich water along with the anesthetic across gill epithelium and allowing fish to be manipulated outside of water. Information on the construction of flow anesthesia apparatuses and parameters are sparse. The goal of this study was to create a flow anesthesia apparatus with materials commonly found within a research facility and to evaluate variable concentrations of MS-222 for anesthesia in zebrafish. Depth of anesthesia was monitored by quantifying respiratory rate and recording responses to physical stimulation. All concentrations of MS-222 evaluated (30−100 ppm) were successful at maintaining surgical anesthesia for up to 30 min. The anesthetic events were demonstrated to be safe, with an observed 97% survival rate. This work demonstrates refinements in zebrafish anesthesia and encourages future studies to evaluate MS-222 flow anesthesia for longer duration and evaluation of other commercially available anesthetics for efficacy in a flow anesthesia setup.
Introduction
Anesthesia is defined as the administration of a substance to chemically restrain and prevent the sensation of pain in an organism by reducing movement and nervous system function.1,2 Anesthesia is often utilized for data collection and to safely provide medical care to laboratory animals.3–5 The effects of anesthesia can be limited to a specific region or impact the organism entirely, and can range in depth from the animal being lightly sedated to general anesthesia, where the animal is unresponsive to its environment.6,7 The strength of anesthetic solutions depends on several factors such as the drug class, concentration, route of administration, and species being anesthetized.3,8,9 It is common to utilize multimodal anesthetic protocols to minimize complications while achieving desired therapeutic effects.7,10 Due to the range of physiological effects that can coincide with anesthesia administration, it is critical to select the appropriate treatment regimen to promote positive outcomes for the animal.
Anesthetic regimens are readily available for most terrestrial species utilized in biomedical and veterinary research, which provide guidance to investigative, clinical, and husbandry staff for the safe induction of anesthesia in those species. 4 In comparison, less literature is available for aquatic species, despite the increasing use of the zebrafish (Danio rerio) as a model in biomedical research.7,9–12 Immersion is the most common route of anesthetic administration in fish, wherein the drug is absorbed across the skin and gill epithelium at a rate that is species dependent.1,10,11,13 Anesthetic depth in fish is defined by various stages ranging from 1 to –4, where stage 1 is light sedation and stage 4 is just before an overdose. Stage 3 is regarded as surgical anesthesia and is characterized by the animal being unresponsive to physical contact. A decrease in respiratory rates is also observed at stage 3.1,10,11,14,15 Several drugs have been utilized for fish anesthesia including alfaxalone, benzocaine, ketamine, metomidate, isoeugenol, 2-pheoxyethanol, quinaldine, and tricaine methanesulfonate (MS-222). MS-222, the most commonly used anesthetic for fish, is the only Food and Drug Administration-approved anesthetic for zebrafish.1,8,10,11,13,16–18 MS-222 is fat soluble and can pass through lipid membranes once it is absorbed by fish. This characteristic allows for the inhibition of neuron voltage-gated sodium ion channels and prevents depolarization. This blockage of sodium channels subsequently decreases nervous system activity and prevents muscle contractions.13,16,18 Zebrafish are typically anesthetized via an immersion at concentrations of 100–150 mg/L for an induction dose of anesthetic prior to procedures being performed. 6 It is also common to utilize MS-222 for euthanasia of zebrafish at a dose of 300 mg/L or higher. 6 MS-222 is acidic and must be buffered with sodium bicarbonate prior to treatment, to prevent serious epidermal and corneal damage.6,13,16,19 Induction of anesthesia with MS-222 in zebrafish is rapid following immersion at the aforementioned doses, with the fish typically becoming unresponsive within 5 min.2,11,20 One risk that zebrafish users must consider is that MS-222 concentrations can continue to increase in the brain after reaching equilibrium in the blood, making anesthetic complications more likely when utilizing MS-222 immersion for longer periods of time.1,14 Additionally, fish lose the ability to ventilate on their own when under MS-222-induced anesthesia for long periods of time, thus requiring a continuous flow of water to be manually passed across their gills to facilitate oxygenation1,2
Due to the mentioned risks associated with immersion anesthesia, it is recommended that flow anesthesia be utilized when performing activities that cannot be completed within 10 min for any species of fish.1,8 Flow anesthesia works by delivering water that is dosed with anesthetic across the gill epithelium at a controlled rate, resulting in stable oxygenation and exposure to the anesthetic.8,10,12 This method has allowed researchers to perform imaging and surgical procedures on zebrafish while maintaining appropriate anesthesia for up to 2 days.12,16,20–24 Much of the emphasis in these studies has been on the construction of the flow anesthesia apparatus with respect to microscope use, rather than the investigation of what dose of anesthesia is appropriate for a certain procedure. The goal of this study was to determine if zebrafish could reach a surgical plane of anesthesia in a flow anesthesia apparatus constructed from supplies easily sourced within a research facility. In addition, we sought to evaluate various concentrations of MS-222 in flow anesthesia to determine efficacy and guide future recommendations for zebrafish anesthesia across institutions.
Methods
Setup
The flow anesthesia delivery system used in this experiment was constructed from standard supplies found in an animal research facility (Fig. 1). An 8000 series IV fluid pump (FP; BD, Chicago, IL) was used to drip anesthetic at a controlled rate to the fish, as well as a screen (MS; BD, Chicago, IL) to monitor the flow of the maintenance anesthetic agent the fish receives. To create the maintenance anesthetic solution, a fluid reservoir bag (FB; Baxter, Deerfield, IL) was created by emptying a 1 L saline bag. The saline bag was then refilled with freshly made and mixed anesthetic solution through the Luer lock port using a 50-mL Luer lock syringe (BD, Chicago, IL). Maintenance anesthetic solution creation is detailed below. The FB containing the maintenance anesthetic solution was then hung on a drip stand (DS) hook and connected to the IV FP using an infusion set (IS; BD, Chicago, IL). At the end of the IV pump infusion set, a 22-gauge TeflonTM catheter (GC; BD, Chicago, IL) was connected to insert into the fish’s mouth. The IV pump infusion set and 22-gauge catheter were then flushed to allow free flow of anesthetic solution through to the catheter. The IV pump infusion set was taped to a shoebox rat cage (Ancare, Bellmore, NY) lid that was flipped upside down and placed on top of the cage bottom which acted as a reservoir to collect the used maintenance dose anesthetic agent. Prior to each trial, a sponge was dipped in fresh fish system water and placed on top of the lid next to the taped IV pump infusion set.

Induction
Fish were initially induced into an anesthetic plane using a 150 ppm (mg/L) immersion of buffered MS-222 (Syndel, Ferndale, WA); (0.15 g MS-222, 0.30 g sodium bicarbonate [Pentair Aquatic Eco-Systems, Apopka, FL], 1000 mL fresh fish system water) in a static holding tank before starting the maintenance trial. The initial induction allowed for the appropriate positioning of the fish for the maintenance trial as nonanesthetized fish were difficult to position and risked injuring themselves. The time for induction of anesthesia was recorded for each fish and was defined as the time for fish to reach a plane of surgical anesthesia (stage 3). The time from induction to the insertion of the oral catheter and the start of the maintenance trial was also recorded.
Maintenance
Immediately after the induction immersion was completed, fish were removed from the tricaine immersion solution and placed in lateral recumbency on a freshly dipped wet sponge full of system water (Figs. 1 and 2). The flushed 22-gauge oral catheter was placed ∼3 mm into the mouth of the fish and maintenance anesthetic dose was started at a flow rate of 8.33 mL/min (500 mL/h) (Fig. 2). It is imperative to not place the catheter too far into the mouth of the fish to avoid mechanical injury and flow directly into the gastrointestinal tract. The authors aimed to place the catheter aligned with the operculum.
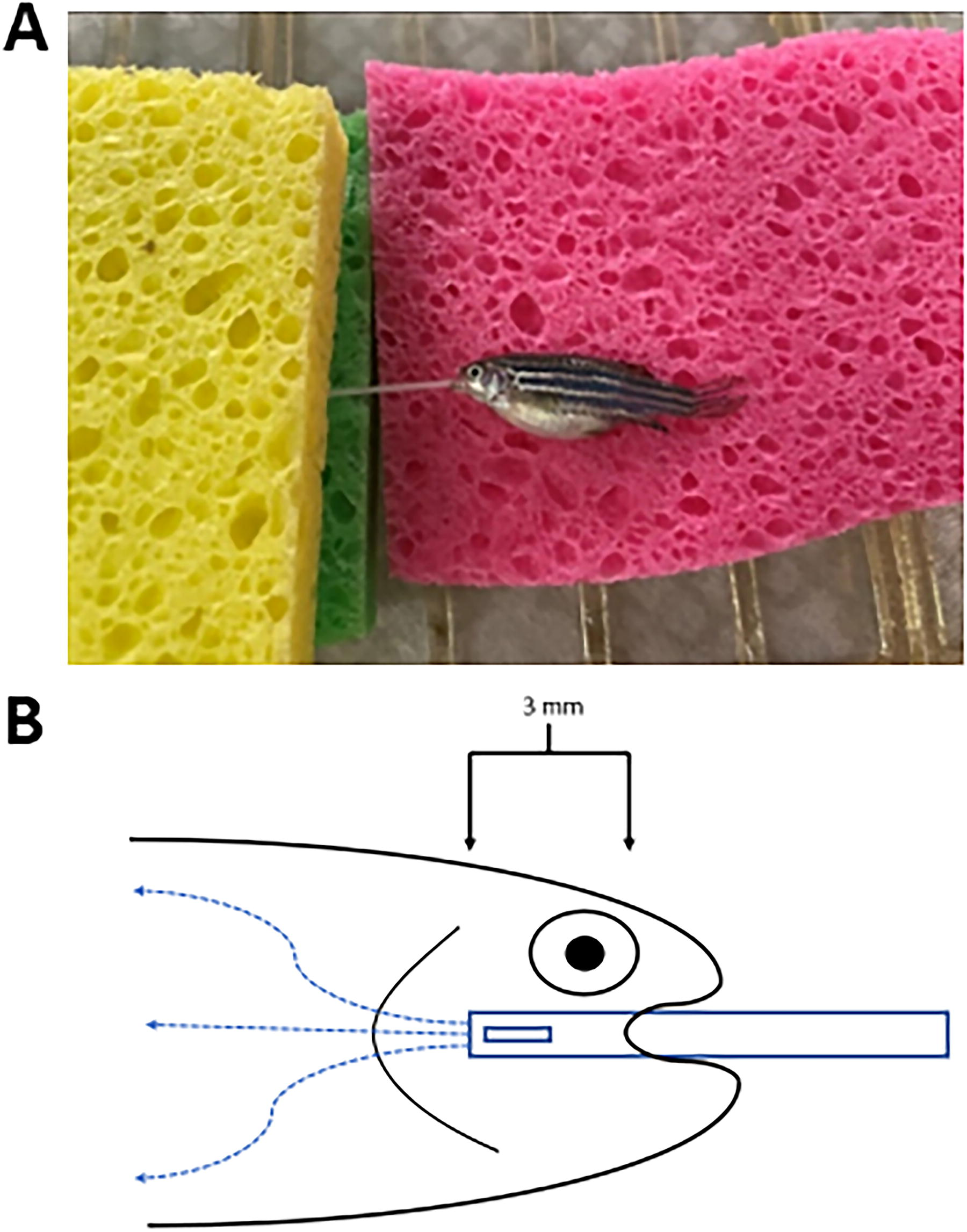
During each trial, fish were continuously monitored to ensure the oral catheter positioning was sustained within the allocated position in the mouth, and operculum movement continued. Immediately after each fish had the oral catheter initially placed in their mouth, operculum rates were recorded for 1 min to establish a baseline rate. Operculum rates were then recorded every 10 min until the end of the trial. Immediately after each operculum rate was recorded, responses to external stimuli were assessed by applying pressure to the tail with forceps and fish received a gentle spray of system water using a spray bottle to keep them moist. Depth of anesthesia was evaluated during the 30-min period by calculating operculum rate (beats/min) and recording the fish’s responses to external stimuli (Figs. 4 and 5). Flow rate for each trial remained at 8.33 mL/min (500 mL/h) and individual trials ran for 30 min. A total of 40 adult Tübingen long fin strain zebrafish initially obtained from Zebrafish International Resource Center were used with 10 adults (5 males and 5 females) tested at each of the following maintenance doses: 30, 50, 70, and 100 ppm (N = 40) (Table 1).

Within each box, the central horizontal line represents a median value. Boxes extend to the 25th and 75th percentiles of each group’s distribution values. Vertical extending whiskers denote the minimum and maximum value of each group’s range. Timeline for induction of anesthesia in male (n = 20) and female (n = 20) zebrafish (D. rerio) with 150 ppm MS-222 immersion.

Within each box, the central horizontal line represents a median value. Boxes extend to the 25th and 75th percentile of each group’s distribution values. Vertical extending whiskers denote the minimum and maximum value of each group’s range. Opercular rates of sedated zebrafish (Danio rerio) at 0, 10, 20, and 30 min after oral catheterization and initiation of maintenance dose at 30, 50, 70, 100 ppm concentrations of MS-222 (N = 4, n = 10; F = female, M = male, # = time posttrial start opercular rate was taken).
Weight, Percent Survival, Time to Induction (Average ± SD), and Recovery Time (Average ± SD) for Male (M) and Female (F) Zebrafish (Danio rerio) from 30, 50, 70, and 100 ppm MS-222 Maintenance Treatments
Recovery
After 30 min, the final operculum rate and stimuli response tests were conducted. Anesthetic flow from the IV pump was then stopped and the oral catheter was removed from the fish. Fish were then transferred into individual 1-L breeding tanks (Aquaneering®, San Diego, CA) filled with fresh system water and were continuously monitored until recovered. Fish were considered recovered when equilibrium was achieved, and normal swimming behavior resumed. Recovery time from placement into the recovery tank and total recovery time were recorded. After the fish recovered from the maintenance dose, they were individually transferred to 1.8-L Aquaneering tanks and placed back on system with appropriate water flow. Fish were assessed at 24- and 48-h postrecovery to evaluate safety of the anesthetic event.
Histopathology
Samples were fixed in formalin for 24–48 h and then transferred to the processor for a 28-h run. The dehydration steps were as follows: 70% ethanol for 1 h, 80% ethanol for 1 h, 95% ethanol for 1 h, 100% ethanol—two changes for 1 h 30 min, and one change for 2 h. For the clearing steps, two xylene changes were performed for 2 h and 30 min each, and one change for 3 h. Paraffin embedding involved three changes, each for 4 h. Samples were embedded at the end of the run. Blocks were sectioned at 5–10 micron thickness, one section per slide. Slides were then stained with Hematoxylin and Eosin on a Leica ST5020 (Leica, Deerfield, IL). Slides were cover slipped with Permount (Fisher Scientific, Waltham, MA) using #1.5 thickness cover glass.
System parameters
Zebrafish were kept on an Aquaneering® recirculating life support system at a pH of 7.2–7.5, conductivity of 450–600 (μS/cm), temperature between 26.0 and 27.5°C (78.8–81.3°F), and with a 10% daily water exchange. The aquatic facility is maintained under a 14:10 light:dark cycle.
Calculation of maximum anesthetic exposure potential
To better compare the dosing regimens using a standardized approach, we calculated the total amount of drug that the fish received by multiplying the concentration of the anesthetic by the flow rate, and then by the duration of the treatment; induction dose of anesthesia was excluded from this calculation (Table 2). For convenience, the authors deemed this value as maximum anesthetic exposure potential (MAEP); the MAEP values for this study are displayed in Table 2.
Proposed Formula for the Maximum Anesthesia Exposure Potential (MAEP) for Calculating the Total Potential Exposure to Anesthetic via Flow Anesthesia and MAEP Values Derived from This Study and Existing Literature
Statistical analysis
Our data was analyzed using GraphPad Prism (version 10.3.1) software and significance was considered when a p value of <0.05 was achieved. Normality of data across all groups was assessed using the Shapiro−Wilk test. Differences in time to induction between male and female groups were evaluated using a two-tailed t-test. Opercular rates between sexes at identical time points and doses were analyzed using a Mann−Whitney U test. To assess changes in opercular rates relative to initial values, a Friedman test was conducted. To determine differences in recovery time across varying MS-222 dosages, a Kruskal−Wallis test was performed. Recovery times between sexes were compared using a two-tailed t-test for groups exposed to 30, 50, or 70 ppm MS-222, while a Mann−Whitney U test was used for the 100 ppm group. Descriptive statistics were calculated for weight, percent survival, time to induction, and recovery time for all groups.
Results
Surgical anesthesia was induced for all fish in the study at a concentration of 150 ppm MS-222 (Fig. 3). While males reached the state of surgical anesthesia faster than females (Avg = 51.4 s vs. 56.4 s), the difference was not significant (p > 0.05). Anesthesia was successfully maintained for 30 min across all concentrations (Figs. 4 and 5). Operculum rates decreased as the trials progressed within all groups except for the males receiving a dose of 50 ppm; this group had higher operculum rates at the second and third checkpoints than at the first (Fig. 4). Opercular rates were significantly lower at all timepoints for both males and females when compared to the initial rates (p < 0.0001). Differences in opercular rates between gender were insignificant at all time points. Initial operculum rate was compared to the time it took to place the oral catheter in individual fish and no significance was found.
Nearly all dosage groups up to 70 ppm had at least one fish respond to the initial reflex timepoint at 10 min (Fig. 5). Only 2 out of 10 fishes reacted to the stimuli by the final timepoint at the lowest concentration, while there were zero reactions after the first timepoint at concentrations greater than 50 ppm. The 100 ppm groups did not respond to any of the reflex checks. All fish from the 30, 50, and 70 ppm groups fully recovered from their anesthetic exposure (Table 1). A single fish from the 100 ppm group did not recover which resulted in 90% survival from our highest concentration, and 97.5% overall survival (Table 1). As expected, a higher dosage of MS-222 resulted in longer recovery times (Fig. 6). The recovery time for the 30 and 50 ppm groups was significantly less than for the 100 ppm group (p < 0.0001 and p = 0.0165, respectively). Recovery time within the 30 ppm concentration was very similar across sexes, only differing by ∼1 s (Fig. 6). Males took longer than females to recover at concentrations of 50 and 70 ppm, although there was no significance (p = 0.1352 and 0.6499; Fig. 6). Recovery was noticeably longer for females than for males at a concentration of 100 ppm, although values did not approach significance (p = 0.1111) (Fig. 6).
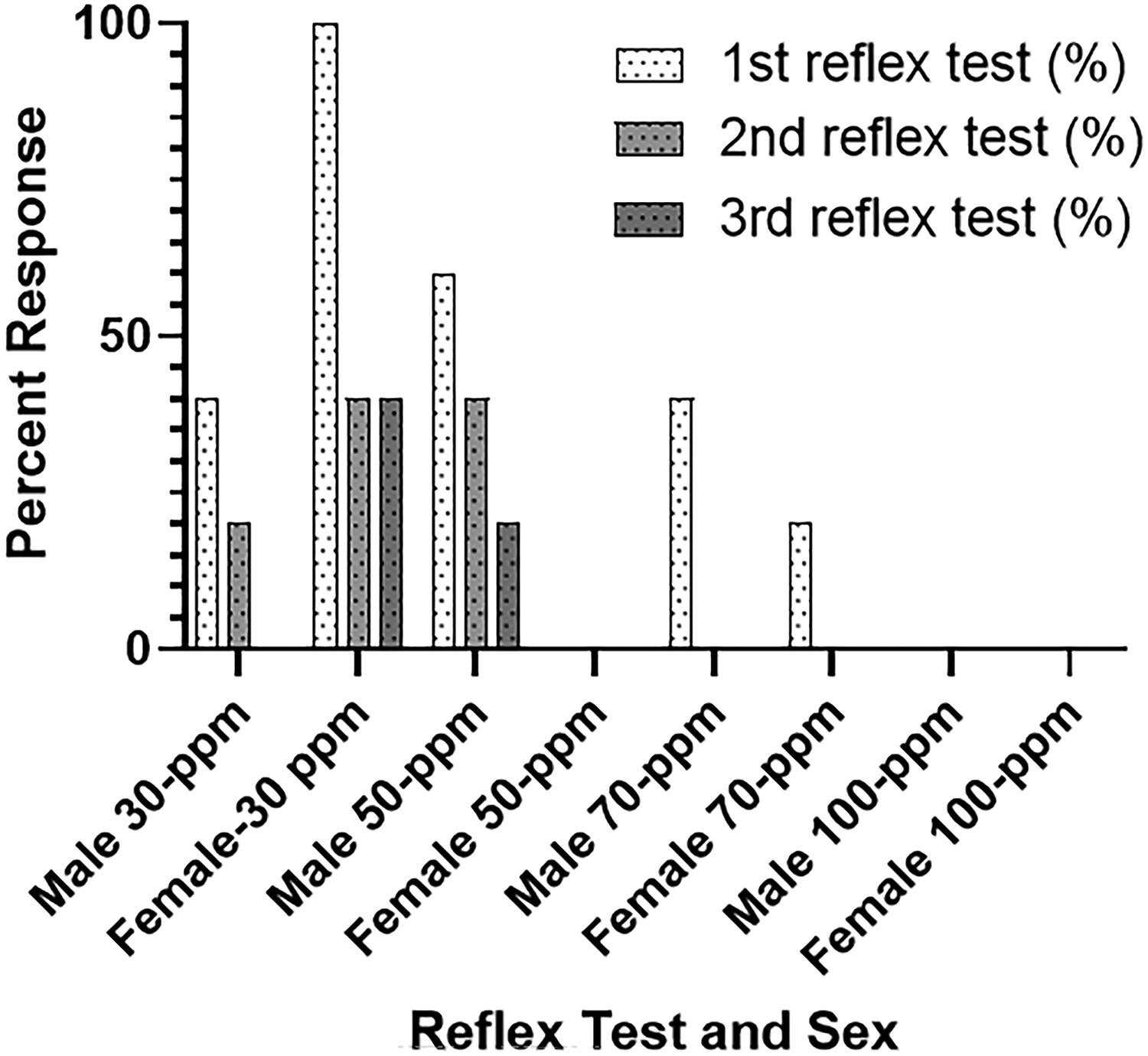
Proportion of zebrafish (D. rerio) that responded to external stimuli during reflex checks (N = 4, n = 10; F = female, M = male, #, time posttrial start opercular rate was taken).

Within each box, the central horizontal line represents a median value. Boxes extend to the 25th and 75th percentile of each group’s distribution values. Vertical extending whiskers denote the minimum and maximum value of each group’s range. Recovery time of male (N = 4, n = 5) and female (N = 4, n = 5) zebrafish (D. rerio) under 30, 50, 70, and 100 ppm of MS-222 maintenance solution.
We directly compared the MAEP values used in this study, respectively 7.5 − 24.99, to parameters published in Xu et al. and Castranova et al. where they used MS-222 with only flow anesthesia and produced MAEP values for their studies.12,20 Their MAEP values were 2246.4 mg delivered over 48 h and 907.2 mg delivered over 20 h, respectively (Table 2). To the authors’ knowledge, survival in the present study (97.5% across all concentrations) was higher than all other reported survival in studies using flow anesthesia in zebrafish. It is important to note that the current study utilized the lowest concentrations of anesthesia and did not attempt to extend the treatment as long as some of the published work.12,16,20
On histopathologic evaluation, all samples were of adequate diagnostic quality with minimal to rarely, mild autolysis. No differences were noted between concentration groups on histopathologic evaluation. The only abnormalities noted were interpreted as nonpathological age-related or incidental findings.
Discussion
Utilization of flow anesthesia is based on the application of continuous anesthetic directly to the gills of the fish and is a relatively new technology, first reported in the 1990s.1,14,25 Flow anesthesia allows for a more appropriate delivery of anesthesia for procedures of longer duration, and it is recommended that this method should be used for any activity longer than 10 min.1,8 Zebrafish have been successfully maintained under flow anesthesia by multiple groups for imaging purposes.12,16,20–24 Details of the anesthetic preparation vary or are underreported, making it challenging to adapt protocols for institutional use. Here, our goal was to evaluate a range of concentrations of MS-222 delivered via flow anesthesia to allow researchers to select the lowest effective dose compatible with experimental procedures and to optimize fish welfare.
Johnston et al. were the first to report on flow anesthesia in zebrafish. Anesthesia was maintained with a dose of 160 mg/L (160 ppm) of MS-222 via oral intubation at a flow rate of 1 mL/min. 21 Xu et al. induced anesthesia in zebrafish with MS-222 at a concentration of ∼173 mg/L (173 ppm) and then utilized a flow anesthesia setup at a dose of 130 mg/L (130 ppm) to maintain anesthesia for 48 h. 20 Xu et al. recommended a minimum flow rate of 5.5–6 mL/min. 20 Castranova et al. utilized a dose of 126 mg/L (126 ppm) of MS-222 at a flow rate of 6 mL/min for 20 h and had a survival rate of 77%. 12 Wynd et al. was the only group to utilize flow anesthesia in zebrafish with a drug other than MS-222. 16 In this study they utilized benzocaine at a concentration of 35 mg/L (35 ppm) following induction of anesthesia with 200 mg/L (200 ppm). 16 This concentration was effective at maintaining zebrafish under anesthesia; however, the survival rate was 14.3% when administered their dose for 8 h. Wynd et al. then adapted their protocol to include a 330 s dose of system water following a 870 s dose of the benzocaine and increased survival to 71.4% at 8 h. This method was successful at keeping a zebrafish under anesthesia for 24 h. In comparison, the current study utilized a broader range of MS-222 concentrations from 30 to 100 mg/L at a flow rate of 8.33 mL/min to maintain a surgical plane of anesthesia after being induced with an immersion at 150 ppm. These parameters were established to anesthetize fish for 30 min which is often sufficient to perform most procedures or imaging studies needed in adult animals.
The MAEP values in our study ranged from 7.5 mg in our 30 ppm group to 24.99 mg in our highest concentration of 100 ppm; all treatments in the current study lasted ∼30 min. Flow rate was higher in the present study than other reported values. This flow rate was deemed necessary for maintaining anesthesia in the fish when transferring from the anesthetic immersion solution as initial trials with a lower flow at the same concentrations were not sufficient for maintaining the anesthetic plane. Histological analysis showed no adverse effects associated with the increased flow rate in this study relative to other published flow rates in zebrafish anesthesia.
Despite having different anesthetic concentrations and flow rates, the amount of MS-222 received by fish in the first 30 min in Xu et al. and Castranova et al. was similar to what fish received in our 30-min trials according to MAEP.12,20 The current study was successful at utilizing a lower concentration of anesthetic solution and a higher flow rate than previously published work to maintain anesthesia in zebrafish with high survival. Utilizing lower concentrations of anesthetic solution can improve the survivability of fish, reduce recovery times, and possibly prevent long-term health effects fish may experience at higher concentrations. The overall decline in operculum rates and lack of response to external stimulation as the trials progressed confirmed that the fish remained in a surgical plane of anesthesia (stage 3). Initial operculum rates were high and have been observed by others in the field at the initiation of fish anesthesia.11,14 Additionally, the time it took for oral catheterization of the fish for maintenance anesthesia did not impact on the initial operculum rate. Assessment of the surgical plane is a possible source of human error that could impact the variability in initial operculum rate and success of the overall anesthetic procedure, as the induction of anesthesia is rapid and can vary between individual fish when using MS-222. 11 It is worth noting that the increased mean recovery time in the female 100 ppm group compared to the other groups could be attributed to an individual fish and points to the impact of individual variability and anesthetic recovery times. The authors hypothesize that body composition of fish plays a role in anesthetic recovery times, as higher body compositions and increased lipids will affect drug clearance time for lipid-soluble drugs, such as MS-222.13,16,18 This may also explain why males at 50 ppm showed increased opercular rates at later timepoints when compared to initial opercular rates. Future studies focusing on recovery times from anesthetic procedures using fish with varying body compositions can elucidate the relationship between anesthetic clearance time and individual fish variability.
Conclusions
This study was successful at maintaining surgical anesthesia in zebrafish, with supplies commonly found in a research facility, at lower concentrations of MS-222 than previously reported. Based on the high survival rate and lack of histological pathology findings in our study, we find that MS-222 flow anesthesia concentrations between 30 and 100 ppm can be safely utilized in zebrafish for up to 30 min. We also present a way for researchers to calculate and compare anesthetic values, using the MAEP, to help compare across past studies and refine the best procedures of anesthetic use. This formula can help users determine anesthetic concentrations and flow rates of new anesthetic drugs via flow anesthesia by comparing anesthetic values to other routes of administration (e.g., immersion) and standardizing treatment. Further investigations are needed to determine the safety of flow anesthesia for periods longer than 30 min, to evaluate the efficacy of other anesthetics in our flow anesthesia setup, and to evaluate the effect of flow rates on zebrafish health and welfare postanesthetic exposure.
Animal Ethics Statement
All applicable international, national, and institutional guidelines for the care and use of animals were followed. All procedures involving animals were performed in accordance with the ethical standards of the Institutional Animal Care and Use Committee at the Abigail Wexner Research Institute at Nationwide Children’s Hospital. The facility is Office of Laboratory Animal Welfare-assured, USDA-registered, and accredited by AAALAC International.
Footnotes
Acknowledgments
The authors acknowledge Kristen Joyce and Ashley Artrip for their help with obtaining supplies and Joshua Zens for help with the initial plan and set up of the flow through anesthesia apparatus.
Authors’ Contributions
A.G.K.: Experimental design/conceptualization, literature review, article preparation, and data acquisition/interpretation/curation. L.R.B.: Experimental design/conceptualization, article preparation, statistical/data analysis, and data acquisition/curation. L.T.F.: Data interpretation, reviewing, and editing of article. M.B.P.: Reviewing and editing of article, article preparation, data interpretation, and statistical analysis. R.A.M.: Experimental design, reviewing and editing of article, and data acquisition/curation. M.W.: Histological analysis, article preparation, and data interpretation. G.C.K.: Reviewing and editing of article. C.B.A-Z.: Reviewing and editing of article. L.A.F.: Reviewing and editing of article, article preparation, data acquisition/curation, and data interpretation.
Disclosure Statement
The authors declare no competing or financial interests.
Funding Information
This work was supported by funding from the Animal Resources Core at the Abigail Wexner Research Institute at Nationwide Children’s Hospital, startup funds granted to G.C.K. from the Abigail Wexner Research Institute at Nationwide Children's Hospital, and the Department of Pathology at Midwestern University College of Veterinary Medicine.