
Abstract
Rural-to-urban migration is increasingly common among youths in developing countries and could affect sexual activities with consequences for premarital pregnancies. We use life history data collected in Kisumu, Kenya, to investigate how the timing and number of rural-to-urban moves are associated with premarital pregnancy. Among sexually experienced young women aged 18 to 24 (N = 226), 60 percent had moved at least once in the past 10 years and 38 percent had experienced a premarital pregnancy. Results of the event history analysis show that those who experienced one or two moves were at increased risk for premarital pregnancy compared to nonmovers. Also at increased risk were movers whose most recent move occurred in the past 7 to 12 months. Finally, those whose last move occurred at age 13 or younger were also at an elevated risk. Migration brings about specific risks and needs for youths, including the need for sexual and reproductive health education and services, which should be made available and accessible to new urban residents.
With an increasing age at first marriage across sub-Saharan Africa, the context of sexual initiation in many countries has shifted from marriage to premarital relationships (Mensch, Grant, and Blanc 2006). This development has been accompanied by an increase in the years that young women are at risk for premarital birth (Hattori and Larsen 2007; National Research Council and Institute of Medicine 2005). Premarital pregnancy and childbearing can influence the achievement and timing of other key transitions to adulthood and alter young women’s life trajectories in the longer term. In particular, research in sub-Saharan Africa has linked premarital pregnancy and birth to early termination of education, lower long-term earning potential, decreased opportunities for union formation, and experiences of discrimination and stigmatization (Amobi and Igwegbe 2004; Grant and Hallman 2008; Hattori and Larsen 2007; National Research Council and Institute of Medicine 2005; Nzioka 2004; Zwang and Garenne 2008). 1 In most of sub-Saharan Africa, the social and economic consequences of a premarital birth occur in the absence of a state social welfare infrastructure for poor or unwed mothers. 2
Migration from rural to urban areas is an increasingly common experience for youths in sub-Saharan Africa, and previous research has documented associations between such residential changes and sexual and reproductive outcomes, including sexual initiation, HIV/AIDS, and fertility (Luke et al. 2012; Mberu and White 2011; Mberu 2008; White et al. 2008; Yang 2004). Nonetheless, there has been scant research to date on links between migration and premarital pregnancy. There are multiple pathways through which rural-to-urban migration can be posited to increase the likelihood of premarital pregnancy for young women. Residential change itself is often a disruptive event in young women’s lives, which could be accompanied by difficulties in adapting to new social environments and integrating into supportive peer networks (Goldberg forthcoming). Migration to urban areas in particular also exposes individuals to new ideas, more permissive social norms, and access to a wider pool of potential sexual partners (Brockerhoff and Biddlecom 1999; Wolffers et al. 2002). In addition, migration can provide increased opportunities for independence from parents and other caregivers, which can decrease social control. These circumstances may lead to engaging in new relationships and unsafe sexual activities, such as early sexual initiation, more frequent sex, or less condom and contraceptive use, which can in turn increase the risk of premarital pregnancy. Finally, urban areas in sub-Saharan Africa generally offer access to a wider range of high-quality health services than do rural areas, which can also affect premarital pregnancy. For example, greater access to and use of contraceptive methods could lessen the risk of conception, while the availability of safe abortion services could decrease the negative implications of a premarital pregnancy.
Most previous quantitative studies of migration are cross-sectional and compare migrants to nonmigrants at one point in time (e.g., Brockerhoff and Biddlecom 1999; Lurie 2006). It is increasingly recognized that migration is a complex process that often involves multiple residential changes during adolescence and young adulthood (Luke et al. 2012; Mberu and White 2011). Few studies contain data regarding the various dimensions of migration—such as the timing and number of residential changes—that would enable exploration of migrants and their behaviors as they age and assimilate. Our study overcomes this limitation by using retrospective life history calendar data, containing monthly information on residential moves and pregnancy during a 10-year period, from young people in Kisumu, Kenya.
Within sub-Saharan Africa, Kenya has one of the highest rates of premarital pregnancy (Magadi, Agwanda, and Obare 2007). As elsewhere in the region, a large percentage of these pregnancies are unintended. Among Kenyan adolescents aged 15 to 19, 47 percent of pregnancies were reported as unplanned (unwanted or mistimed) in 2007 (Kenya National Bureau of Statistics, and IFC Macro 2010). In this study, we examine linkages between rural-to-urban migration and premarital pregnancy in Kisumu, the third largest city in Kenya and the capital of Nyanza Province. In this area of the country, rates of nonmarital pregnancy among young women are the highest in the country, and rates of contraceptive use are low (Oindo 2002). Statistics for Nyanza Province show that among never-married girls, more than 13 percent of those aged 15 to 19 have ever been pregnant, and 45 percent of those 15 to 24 have never used a contraceptive method (Population Council 2010). Previous research in Kisumu has documented the influence of early pregnancy on young women’s life course transitions, including dropping out of secondary school (Clark, Kabiru, and Mathur 2010). Kisumu, with an estimated population of 350,000, is also a primary destination for large streams of internal and international migrants in western Kenya. An economic hub and the site of many schools and colleges, Kisumu attracts a range of young people seeking employment and educational opportunities. Given its importance as a migration destination and the poor reproductive and sexual health outcomes for youths, Kisumu is an important location for investigating the linkages between migration and premarital pregnancy.
Previous Research
A large body of work has examined the determinants of premarital pregnancy in sub-Saharan Africa (e.g., Ajayi et al. 1991; Ondimu 1997; Toroitich-Ruto 1997). Though little research has investigated links between migration and premarital pregnancy, several studies have investigated the role of residence. Research in Nyanza Province, Kenya, finds that rural residence is associated with a significantly lower likelihood of initiating childbearing for teenage girls than is urban residence (Magadi and Agwanda 2009), and similar results are found in Namibia (Garenne and Zwang 2006). These studies focus on residence in a particular type of place (here, an urban area) at one moment in time, however. Since migration is a process, and one that often consists of spells in various locations, examination of associations between migration and youths’ behavior should ideally follow individuals across locations over the life course (Elder 1994). It is also likely that the association between migration and a given behavior depends on the timing of residential change, including the age at which migration occurred and the length of time that has passed since the move.
In this study, we examine several dimensions of migration during the early life course. First, we consider the number of residential moves lasting one month or more undertaken by young women. Scholars hypothesize that frequent residential change may create a sense of transiency and psychological stress and increase the likelihood of engaging in premarital sex and, therefore, increase the chances of premarital pregnancy (Stack 1994). On the other hand, young women who make repeated residential changes may become more resilient to these disruptions over time with no increased risk of premarital sex and pregnancy for those who move repeatedly (Luke et al. 2012).
Second, we examine age at residential change. Moves in late childhood and early adolescence could pose more adjustment difficulties than moves that occur at later ages, when young people have acquired skills and experiences that allow them to more safely navigate the disruptions that accompany migration. Furthermore, residential change during early adolescence can be expected to coincide with the major emotional and physical changes associated with puberty, which could be particularly detrimental for young girls, making them more vulnerable to early sexual activity and premarital pregnancy (Luke et al. 2012).
Finally, we consider how recently a move occurred. In their efforts to assimilate, adolescents and young adults who have recently changed residences may become involved in activities or associate with peer groups that encourage delinquency or early sexual activity (South, Haynie, and Bose 2005). On the other hand, caregivers may be attentive to the difficulties associated with adapting to a new environment in the short term and may supervise young people more closely during this period, thus restricting their sexual activities (Luke et al. 2012).
Data and Methods
This article draws on detailed life history data from the Urban Life among Youth in Kisumu Project, conducted in 2007. The study employed a novel survey instrument called the Relationship History Calendar (RHC). The RHC is a foldout grid in which monthly information on each topic is recorded in a timeline format over a 10-year retrospective period (January 1998 to June/July 2007). Respondents were between the ages of 18 and 24 at the time of the interview and, therefore, between 8 and 14 at the start of the RHC. Like other life history calendars, the RHC gathers information on respondents’ fertility, employment, schooling, and migration (or residence) histories (Axinn, Pearce, and Ghimire 1999). Place of residence (district within Nyanza Province, other province in Kenya, or country) and its designation as urban or rural are recorded for each month. In addition to these life course domains, respondents provide detailed information on each of their romantic and sexual partnerships, including the type of relationship and frequency of sexual intercourse in each relationship.
The survey sample was drawn by contacting every other household in forty-five randomly selected urban enumeration areas in Kisumu town. Men and women ages 18 to 24 in the selected households were eligible to be interviewed. One respondent was randomly chosen per household, and he or she was randomly assigned to receive either the RHC or a more standard demographic survey. The overall response rate for the study was 94.9 percent. A comparison of the quality of the data gathered by each type of survey instrument found that, overall, the RHC collected equally consistent and comparable data relative to the standard survey, with less social desirability bias found in the reporting of sexual behaviors. Further details of the study design and quality of the RHC data are available elsewhere (Luke, Clark, and Zulu 2011).
The present study examines the potential role of migration in young women’s transition to first premarital conception, conditional on having experienced sexual activity. Of the 286 female respondents interviewed with the RHC, those who had never initiated sexual intercourse by the end of the 10-year calendar period are excluded from the analysis (N = 43). We also exclude 19 respondents who had missing data on any one of the independent variables. In total, the analysis of the transition to first premarital pregnancy utilizes data from 224 ever–sexually active female respondents, for a total of 6,323 person-months.
Event history analysis
The longitudinal nature of the RHC data allows us to use survival analysis techniques to estimate the probability of first premarital conception in each month as a function of individual characteristics and migration experience in the current or previous months. The month of first premarital conception is determined by information on pregnancy status, frequency of sexual intercourse, and marital status for each month of the calendar. For the analysis, the exposure period for the risk of premarital conception begins in the month of first reported sexual intercourse. We end the exposure period in the month of first premarital conception, 3 marriage, or the end of the calendar, whichever comes first. We censor respondents at marriage to ensure examination of the predictors of premarital pregnancy in particular.
We utilize Cox regression, a method that allows for precise ordering around the outcome of interest (ensuring in this case that residential transitions and other covariates of interest precede premarital conception) and for inclusion of time-varying covariates. It is also designed explicitly to deal with otherwise problematic right-censored cases—here, females who had not become pregnant before entry into marriage or by the end of the calendar period.
Independent variables
A particular benefit of the RHC instrument is that it captures a wide variety of young people’s residential changes over the periods of late childhood, adolescence, and early adulthood (the 10-year retrospective period began when respondents were ages 8 to 14 and ended when they were ages 18 to 24). These include all moves from a rural to an urban area for one month or longer, and vice versa, as well as rural-rural or urban-urban moves that cross district (within Nyanza Province), province (within Kenya), or country boundaries. 4 In this analysis, we focus on rural-to-urban moves because they are one of the most common type of moves experienced by the young women in our sample (Luke et al. 2012) and likely pose the most dramatic changes in context. In addition, the RHC data fully capture rural-to-urban migration as opposed to other types of moves, such as rural-to-rural moves within districts. 5
We are particularly interested in examining how the age at migration and the recency and number of residential moves are associated with the risk of premarital conception. Each of the three migration variables is time-varying. For each month of the RHC, we first group the number of rural-to-urban moves experienced since the beginning of the calendar into four categories: zero (no moves in the calendar), one, two, or three or more. For each month, we also designate the age at last rural-to-urban move with a trichotomous indicator of age 13 or younger, older than age 13, or no move in the calendar. We use this cutoff because it is a good marker for the starting point of sexual maturity and the transition to older adolescence (Dixon-Mueller 2008). Finally, for each month, we examine the recency of the last rural-to-urban move categorically as occurring in the last 1 to 6 months, 7 to 12 months, 13 or more months, or no move in the calendar.
We chose to measure the migration variables starting with the first month of the calendar (when respondents were between the ages of 8 and 14), rather than beginning at the age of sexual debut. Previous research using the RHC data has shown that a large proportion of young men and women had experienced residential changes prior to sexual debut and that these experiences were related to an elevated risk of initiating sexual intercourse (Luke et al. 2012). This implies that ignoring early migration experience may lead to biased estimates of the association between migration and premarital pregnancy.
With respect to control variables, we include sociodemographic characteristics investigated in previous studies of migration, of sexual activity, and of premarital pregnancy. All variables are time-varying monthly measures with the exception of location of birth. Age at sexual debut is measured in years and is used to adjust for the varying starting points of exposure across respondents. Other variables are coded dichotomously: born in an urban area, living in an urban area, attending school, currently employed, engaged to be married, and in a serious relationship. We control for place of birth to differentiate urban natives with migration experience from rural natives who moved to urban regions. School attendance is generally protective against risky sexual activity and premarital pregnancy (Garenne and Zwang 2006; Magadi and Agwanda 2009). Employment may decrease the need for sexual partners for economic support among young women (Luke 2003) and could therefore decrease the risk of premarital pregnancy. Being engaged or in a serious relationship may signal stronger commitment compared to less serious types of relationships, such as casual dating or one-night stands. As a result, sexual intercourse could be more regular, contraceptive use could be rare, and pregnancy could be intended (Baumgartner et al. 2009). 6
We also include time-varying measures of orphan status as controls. Given the ongoing HIV/AIDS epidemic in this region of Kenya, many young people are likely to have experienced a parental death during the calendar period, and previous research in Nyanza finds that orphans often move after the death of a parent (Nyambedha 2008). In addition, previous cross-sectional research in sub-Saharan Africa reports a positive association between orphan status and pregnancy in adolescent girls (Gregson et al. 2005). The RHC gathered information on the month and year of maternal and paternal death, if they occurred. We include separate measures for maternal and paternal death that occurred when the respondent was 18 or younger. These variables are measured dichotomously in each month (parental death prior to age 18 in the month, or not).
Results
Descriptive statistics
Table 1 presents descriptive statistics of the rural-to-urban migration experience for the analytical sample of ever–sexually active young women. Information was collected at the time of the interview (when respondents were ages 18 to 24) for the 10 years before the survey. In total, 59.8 percent of young women experienced a rural-to-urban residential move in the last 10 years. The mean number of moves is 1.2, with approximately 36 percent having experienced one, 11 percent two, and 13 percent three or more moves.
Rural-to-Urban Migration Experience in Last 10 Years of Ever–Sexually Active Young Women, Ages 18 to 24, Kisumu, Kenya

The remainder of Table 1 describes residential histories for migrants only. The mean number of moves is 2.1. Approximately 18 percent have experienced two moves and 22 percent three or more. With respect to the age and recency of the last move, it should be kept in mind that these figures refer to the last move that took place during the calendar period. Around 5 percent of female migrants experienced their last rural-to-urban move at age 13 or earlier. The last residential change occurred within the past 6 months for 23 percent of female migrants and in the past 7 to 12 months for 13 percent. Approximately 64 percent of last moves occurred more than one year prior to the interview. Overall, the statistics in Table 1 indicate that this population of young women in western Kenya is highly mobile, with a nontrivial percentage experiencing repeated rural-to-urban moves during the past 10 years.
Table 2 presents descriptive statistics for first premarital pregnancy as well as other characteristics of ever–sexually active respondents at the time of the interview. We find that 38 percent of young women ever experienced a premarital pregnancy, and among those who conceived before marriage, the median age is 20 years. By age 16, 9 percent have had a premarital pregnancy, and 22 percent have done so by age 18.
Descriptive Statistics at Time of Interview of Ever–Sexually Active Young Women, Ages 18 to 24, Kisumu, Kenya
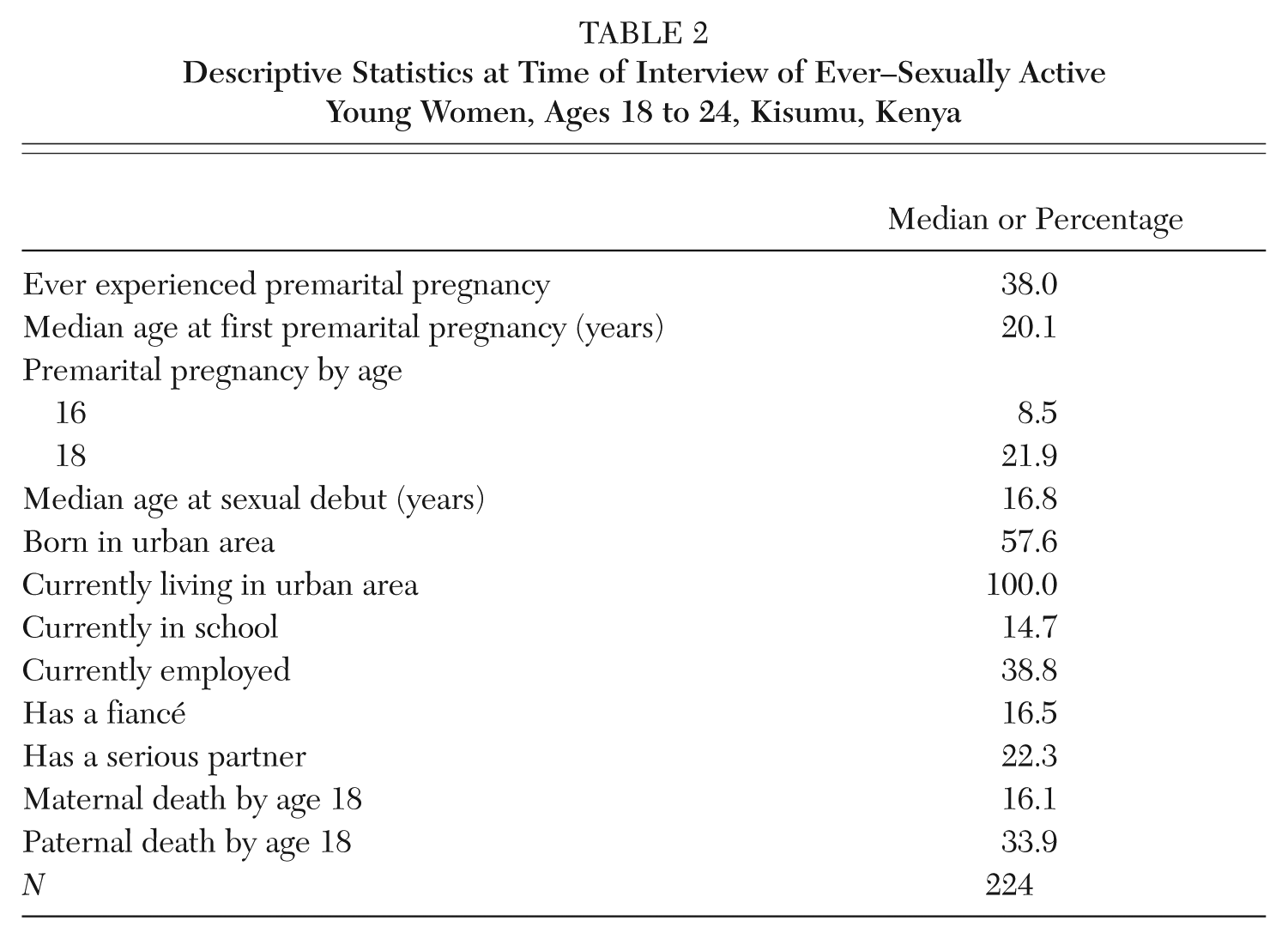
With respect to background characteristics, the median age at sexual debut is 17 years. In the sample, 58 percent of respondents were born in an urban area, and by survey design, 100 percent were living in an urban area (Kisumu) at the time of the interview. Approximately 15 percent are currently in school, 39 percent are employed, and 17 percent and 22 percent have a fiancé or serious partner, respectively. We also see that many respondents have been orphaned; 16 percent of the sample had experienced the death of a mother and 34 percent the death of a father before reaching age 18.
Cox regression results
Table 3 presents results from Cox regression models that examine the correlates of the timing of first premarital conception for young women. The hazard ratios represent the relative hazard of reporting premarital pregnancy during the month for one group, compared with that for the reference group. All three regressions contain control variables and one migration experience variable: the number of previous moves (model 1), the age at last move (model 2), or the recency of last move (model 3). To avoid problems of collinearity, we do not include more than one migration variable in a given regression model.
Hazard Ratios from Cox Proportional Hazard Models of the Timing of Premarital Pregnancy among Ever–Sexually Active Young Women, Kisumu, Kenya
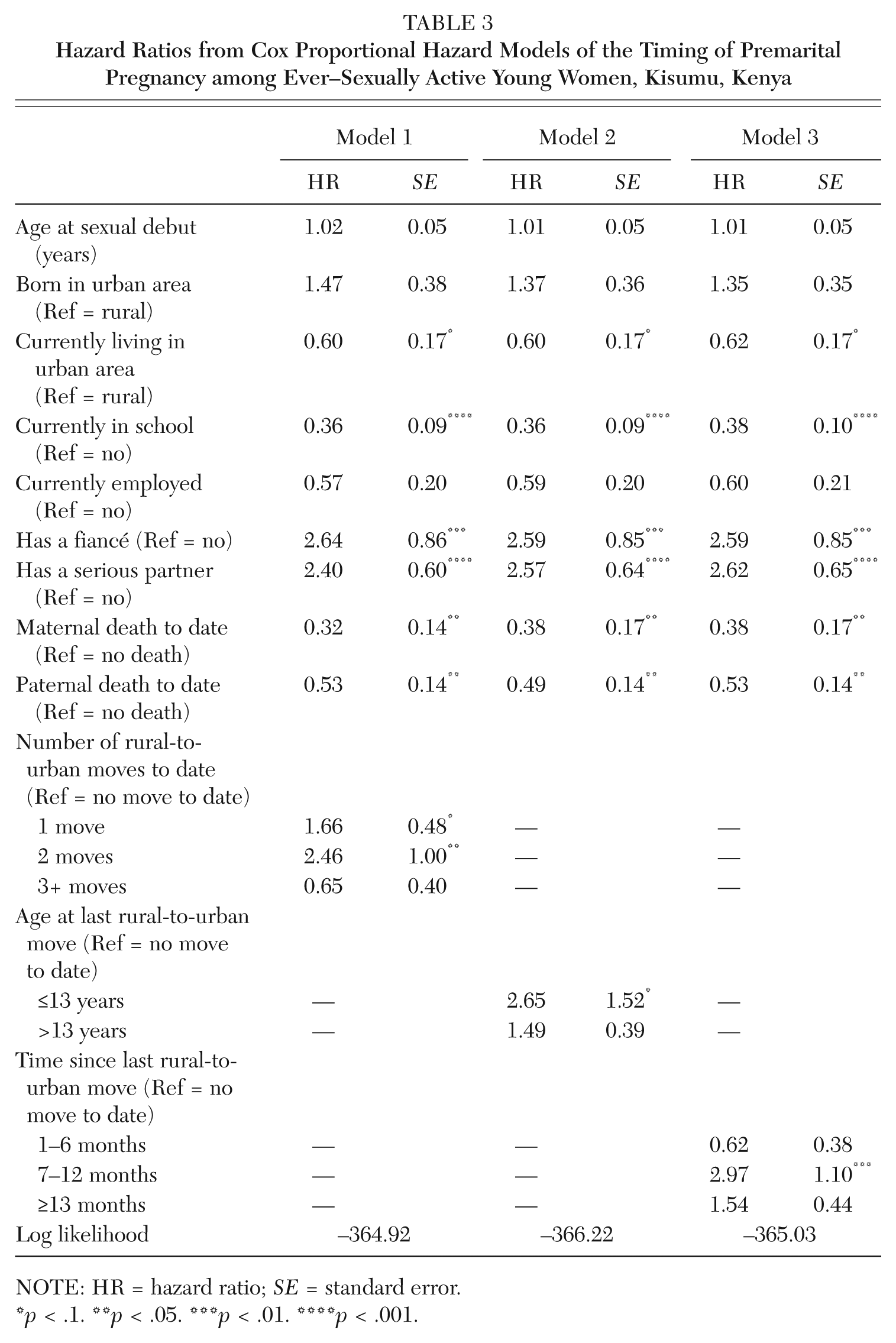
NOTE: HR = hazard ratio; SE = standard error.
p < .1. **p < .05. ***p < .01. ****p < .001.
Each of the three migration variables has a significant or marginally significant relationship with premarital conception. Premarital pregnancy is 1.7 times and 2.5 times as likely for young women who experienced one and two moves, respectively, compared to nonmovers. There is no significant difference between those who moved three or more times compared to nonmovers. Those whose last move occurred at an early age (age 13 or younger) are 2.7 times as likely to have a premarital pregnancy compared to nonmovers. We also find a significant association between recency of last move and the timing of premarital pregnancy. Girls whose last move occurred in the previous 7 to 12 months are three times as likely to experience a premarital conception compared to those who never moved. There is no significant difference for last moves that occurred in the previous one to six months compared to nonmovers, or for those whose last move took place more than one year in the past.
Turning to the control variables, we find that living in an urban area decreases the risk of premarital pregnancy, which is an unexpected result. It could be that rural-to-urban moves—and the disruptions and assimilation processes accompanying them—have the most detrimental impacts on the risk of premarital pregnancy and that it is not living in an urban area per se. Current school enrollment also decreases the risk of premarital pregnancy, as expected. Having a fiancé or serious partner increases the risk of premarital pregnancy, as expected. The hazard ratio for urban residence is marginally significant, while it is significant for schooling and having a fiancé and serious partner across all models. Interestingly, both maternal and paternal orphanhood by age 18 lower the risk of premarital pregnancy, which is significant across all models. One possible explanation is that the surviving parent or other caregivers compensate for the loss of a mother’s or father’s supervision.
Discussion
For sub-Saharan African youths, migration experience may open the door to new educational and job opportunities. At the same time, the life disruptions engendered by major residential change could lead to adverse outcomes that in the longer term undermine successful transitions to adulthood. Taking advantage of the detailed life history calendar data collected from youths in urban Kisumu, Kenya, this study investigates the associations between various dimensions of rural-to-urban migration and premarital pregnancy among young women. Studies to date on the connection between migration and sexual and reproductive behavior have been limited by cross-sectional data. The longitudinal nature of the RHC data allows us to capture 10-year migration histories for our respondents, including precise measurement of the number and timing of residential moves by month. Furthermore, we can account for the ordering of events, ensuring that residential moves take place before premarital conception, which helps to rule out reverse causality.
The descriptive statistics indicate that young women in Kenya are highly mobile, as more than half of the study sample experienced at least one move from a rural to an urban area in the 10-year calendar period. These young women are also at extremely high risk for premarital pregnancy, with more than one-fifth of ever–sexually active young women having experienced a premarital pregnancy by age 18 and almost 40 percent having done so by the time of interview, when respondents were ages 18 to 24.
How is rural-to-urban migration associated with the progression to premarital pregnancy? There has been little research to date on this topic. Our study is the first to adopt a life course approach to investigate how multiple dimensions of the rural-to-urban migration experience act to hasten or delay the event of premarital pregnancy. Our event history analysis reveals significant effects for all three migration variables, including two interesting nonlinearities.
With respect to the number of moves, compared to nonmovers, we find that those who experience one or two rural-to-urban moves are at an increased risk for premarital pregnancy, while those who have moved three or more times are not significantly different. This finding is consistent with the view that one or two residential changes could create a sense of transiency or increase psychological stress, leading young women to engage in risky sexual activities. A possible explanation for the finding of no significant effect for those who moved three or more times is that this group of very frequent movers (less than 6 percent of our sample) has become resilient to the disruptions that accompany residential change. Due to repeated moves, these young women could also have had less time to assimilate into the sexual networks and less restrictive social norms of urban destinations.
Regarding the association between age at last move and premarital pregnancy, we find an elevated risk for premarital pregnancy for those young women whose last rural-to-urban move occurred at age 13 or younger compared to nonmovers. This finding suggests that the circumstances surrounding residential changes in late childhood and early adolescence may be particularly consequential for unsafe sexual behavior later in adolescence and young adulthood. It should be noted that our variable for early age at last move singled out those young women who experienced a rural-to-urban move at an early age and did not experience another such move again in the calendar period. We also investigated if any rural-to-urban move at an early age (age 13 or younger) is associated with premarital pregnancy, regardless of whether there was also a later move, and we find this association is not significant (not shown). Taken together, these results suggest that young women who move to urban destinations in early adolescence with no subsequent move are most vulnerable; they may have experienced a combination of residential disruption at a young age and a longer period to assimilate to more permissive social norms and peer networks that encourage risky behavior in the urban destination (Luke et al. 2012).
Finally, with respect to the recency of the last rural-to-urban move, we find a nonlinearity in its relationship to premarital pregnancy. Compared to nonmovers, those whose last move occurred in the past 7 to 12 months experience an increased risk of premarital pregnancy, while there is no differential risk for those who moved more recently (in the past 1 to 6 months) or longer ago (more than one year in the past). One possible explanation for this inverted U-shaped relationship is that, although a major move might lead to engaging in high-risk sexual behavior, it could take time both to establish the social networks needed to meet new sexual partners and to conceive a child after engaging in unprotected sex. Furthermore, young women could receive greater adult supervision immediately following a move, and this attention could wane after several months’ time (Luke et al. 2012). At the same time, young women’s knowledge of contraceptive methods and safer sexual practices likely increases with time in an urban area, making moves dating back to more than one year ago unrelated to the risk for premarital pregnancy.
Though our study utilized detailed data on the temporal sequencing of migration and premarital pregnancy and offered a first step to documenting the link between migration and premarital pregnancy, there are, nonetheless, several limitations. Although our analyses controlled for the timing of orphanhood and other individual characteristics, we were unable to examine changes over time in individual stress levels, connectedness to and supervision by parents and other caregivers, and the content and influence of peer or sexual networks as the mechanisms that could account for the observed associations between migration and premarital pregnancy. We also did not evaluate the association between migration and the proximate sexual or reproductive activities that lead to premarital pregnancy, including the timing and frequency of sexual intercourse and contraceptive and condom use. These are important areas for future work. Furthermore, our dataset includes little information on the specific circumstances of each residential move, such as household structure and socioeconomic status in each new location, or other unobservable characteristics that could be correlated with both migration and premarital pregnancy. 7 Finally, the RHC instrument did not collect information on the reasons for each residential change. Given that many women in sub-Saharan Africa migrate for marriage, it could be the case that much of the premarital sex and pregnancy that we observe among young women in Kisumu occurs immediately before or as part of the marriage process and is not related to the life disruptions or assimilation processes that accompany rural-to-urban migration. In the analyses, we were able to control for having a fiancé or serious partner, and the effects of the migration variables remained statistically significant. This finding gives us some confidence that the observed relationships between migration and premarital pregnancy do not merely reflect a concurrent process of entry into marriage.
Future work should further explore how knowledge and use of contraception changes with migration experience. While rural-to-urban migration increases the likelihood of premarital sexual activity (Luke et al. 2012), it might also increase young women’s access to modern methods of contraception. Nevertheless, it appears that young urban migrant women do not fully utilize available contraception in Kisumu, and many face premarital pregnancies that are likely unintended. It could be challenging for new migrants—particularly those hailing from rural areas—to learn about and feel comfortable accessing reproductive health services in the city.
Overall, the findings from our study suggest that researchers and policy-makers should pay greater attention to settings with large migrant populations, such as urban Kenya, where residential change is becoming a common feature of adolescence. In such settings, migration experiences will be increasingly intertwined with key life course transitions, such as premarital pregnancies and their associated social and economic consequences. To ensure successful transitions to adulthood, it is essential to provide young migrants with the support they need as they adjust to their new urban environments, including psychosocial support and sexual and reproductive health education and services.
Footnotes
NOTE:
The data used in this analysis come from the Urban Life among Youth in Kisumu Project, directed by Nancy Luke, Brown University; Shelley Clark, McGill University; and Eliya Zulu, African Institute for Development Policy. The research was funded by a grant from the Eunice Kennedy Shriver National Institute for Child Health and Human Development (#R21-HD 053587) and supported by the African Population and Health Research Center. The data are available through the Life Histories, Health, and HIV/AIDS Data Laboratory at McGill University (![]() ). The authors thank participants at the IUSSP International Seminar on Youth Migration and Transitions to Adulthood in Developing Countries for helpful comments on an earlier draft.
). The authors thank participants at the IUSSP International Seminar on Youth Migration and Transitions to Adulthood in Developing Countries for helpful comments on an earlier draft.
Notes
Hongwei Xu is a faculty research fellow at the Survey Research Center, University of Michigan. He has published on issues of population health and spatial methods. He is currently a research team member on the Chinese Family Panel Studies, one of the largest longitudinal data collection projects in contemporary China.
Blessing U. Mberu is a research scientist at African Population and Health Research Center (APHRC) in Nairobi, Kenya. There, he works in the Urbanization and Wellbeing Research Program. His research interests include migration and urbanization, youth reproductive behavior, and poverty in sub-Saharan Africa. His work has been published in international peer-reviewed texts and journals.
Rachel E. Goldberg is a postdoctoral research associate at the Office of Population Research and the Center for Research and Child Wellbeing at Princeton University. She has published on issues of youth well-being, family disruption and instability, and health and sexual behavior in the United States and numerous developing countries.
Nancy Luke is an associate professor of sociology and affiliate of the Population Studies and Training Center at Brown University. Her research focuses on gender, family, migration, and health. Her current projects examine youth life course transitions and sexual behavior in Kenya and community contexts and health in India.