
Abstract
In the past, scholars of academic dependency have tended to focus their discussions on social sciences while treating other fields as separate. They suggest that in order to escape dependency, alternative discourse and autonomy should be developed. In this paper, we examine the Public Health Liberation (PHL) movement in Taiwan and theorize on the marketization and medicalization of the healthcare system since the 1980s as a dependency syndrome. The PHL was initiated by a group of public health scholars—with the second author of this paper being one of its key protagonists—and frontline public health practitioners after the severe acute respiratory syndrome outbreak in 2003. Inspired by the mass mobilization model in public health in Asian and Latin American countries, particularly China, the Philippines, and Nicaragua, PHL trains grassroots public health educators, nurtures critical research, and has built a network of activists for radical public health reform in Taiwan. Based on participatory action research, this paper analyzes the emergence of this influential public health movement and situates it within the global context of neoliberal health reforms.
Introduction
The expansion of the current global health reform as marked by its distinctive neoliberal ideology, has created a global public health crisis since the 1980s (Waitzkin et al., 2007). Although the expansion of this specific global health reform is the result of a complicated process, the production and reproduction of academic knowledge plays a significant role in the establishment of this health reform that favors the privatization of the medical sector while downplaying the preventive sector of the health system. The 2020 COVID-19 pandemic crisis revealed the features of the current global health reform and demonstrates its consequence, namely the increasing global health inequality across societies. Giant pharmaceutical companies were afforded privileges and gained immense profits during the crisis, while poor countries could not afford to purchase vaccines and lacked the infrastructure needed to contain the pandemic. In this regard, the expansion of this specific health reform has created a dependency situation within the health and medical realm in which a society’s health status is dependent upon only a few centers.
The dependency of health and medical knowledge on certain centers is a different form of academic dependency. The healthcare and medical system in the peripheral societies often model their system based on the framework provided by the center and imitates the practice of the center. For example, peripheral countries typically build or reform their health systems based on the suggestions made by experts trained in the West (Waitzkin & Jasso-Aguilar, 2015). In this regard, the health and medical systems in peripheral societies bear similarities with the phenomenon of academic dependency (S.F. Alatas, 2006). In the past, scholars often examine the issue of academic dependency in social sciences, while treating the natural or applied sciences separately (Chen & Lee, 2021). However, as the literature on social health and medicine has demonstrated, the public health system, including preventive and medical sectors, is hardly immune from the influence of political economy and the social contexts from which the health and medical system is born (Waitzkin, 2015; Waitzkin et al., 2007). Therefore, we argue that the theory of academic dependency offers a fresh angle to examine the neoliberal capitalist regime’s effects on and expansion into global health reform. In addition, the expansion of the global capitalist regime has incurred widespread grassroots resistance in many societies. The resistance, from our understanding, bears similarities with academics seeking to resist the academic hegemony.
Our essay is inspired by the discussion of autonomous social science (S.H. Alatas, 2006). Autonomous social science is an ideal for peripheral academic communities and, at the same time, a way to escape the dependency trap. The chief traits of being autonomous are: Autonomy in the conceptualization and prioritization of problems; in the development of research agenda; in the building of original theory; and in the conduct of empirical research. Autonomy leads to a constructive critique of Western knowledge as well as a serious consideration of non-Western sources of knowledge. (S. F. Alatas, 2006, p. 114)
Building an autonomous academic community is highly regarded by scholars of dependency, but, in reality, it is unclear how to proceed. Furthermore, even though academic dependency scholars associate the phenomenon of academic dependency with other dependencies (e.g., economy), their solutions to academic dependency tend to only focus on actions within the academic field (e.g., being original in one’s research agenda). In this regard, the discussion of academic dependency could easily fall into a scheme within the ivory tower. In the case of health dependency, the production of knowledge within educational institutions (e.g., public health schools or medical schools) cannot be separated from the practices and policies in the health and medical fields. The case of resistance against the neoliberal health reform thus offers a valuable lens through which to discuss academic dependency beyond the ivory tower.
In this essay, we examine the emergence of a grassroots public health movement. We should note here that the second author of this paper (Chen) is one of the key protagonists of this movement, and that the first author (Lee) was also involved in a Community University Movement (CUM) which served as the basis for this grassroots public health movement (this will be elaborated upon in the later sections). The movement emerged during the 2003 severe acute respiratory syndrome (SARS) crisis in Taiwan. Under the leadership of activist public health scholars (the second author being one of them), the movement coalesced into an organization, Public Health Liberation (PHL) in 2003. One of the founding goals of the PHL is to liberate public health knowledge from the dominance of knowledge favoring medicalization and the neoliberal health reform. In searching for the weapon, the movement leaders drew the public’s attention to alternative public health practices, such as the barefoot doctors, patriotic health movements, and collective medicine in China prior to China’s market reforms of the medical system. They also highlighted the grassroots health organization based on the mobilization and participation of ordinary people in Nicaragua after the Somoza dictatorship regime was overthrown in 1979, which was composed of Popular Health Work Days, Popular Health Councils, and the Health Brigadistas. They also featured the community health movement in the Philippines that was mobilized by liberation theology followers after the Marcos regime was overthrown in 1983.
Our paper proceeds as follows. First, we briefly describe the methodology of the research for this essay. Secondly, we theorize the withdrawal of the public from the health system in Taiwan as the syndrome of dependency. Thirdly we discuss the PHL’s emergence, its goals, and its activities. Fourthly, we analyze the knowledge produced by PHL leaders, students, and participants. In the final discussion section, we discuss the relationship between the PHL movement and China’s rise.
Methodology: Participatory Action Research
Since the mission of the PHL movement is to liberate public health knowledge and then to transform the public health system, the research methods used cannot be the traditional social science research of sampling, questionnaires, collecting data from sampled but unrelated and uninterested subjects, data analysis to identify variables that are “significant,” etc. On the contrary, the methodology employed in the PHL movement is participatory action research. In fact, it is large-scale participatory action research, where all the actors of the movement—including critical public scholars and activists, seed teachers, community university students, community members who enrolled in classes taught by seed teachers—all participated in the entire process of the movement. In the process of problem finding, defining, and solving, the relationship between theory and praxis is dialectic.
The PHL movement began with a critical analysis of the failures to control the SARS epidemic. The problems of commodification, marketization of the medical system, the medicalization of the public health system, and other issues leading to the failure of the public health system were first raised by critical public health scholars and activists. They were then discussed intensively and interactively among scholars, activists, and seed teachers during many seed teacher training sessions. The seed teachers then brought the knowledge they gained to their students at the community universities. They then discover more problems and then in turn they bring these problems and knowledge back to the training sessions and other gatherings. The whole process is a continuous and spiral feedback loop and is dialectic. The goal of transformative change is accomplished through the simultaneous process of taking action and doing research, with critical reflection as the guiding principle.
The Dependency Syndrome: The Withdrawl of the Government in Public Health
The development of a health care system in a given society results from a complex social process (Starr, 1984). Critical public health scholars have long reminded us that in a capitalist society, health provisions will resemble the dominant economic structure in which the pursuit of profit is prioritized (Waitzkin, 2015). In reality, not all capitalist societies develop the same health and medical systems. For example, the United States and the United Kingdom may be categorized as the same welfare state type (Esping-Andersen, 1990), but their health and medical systems are quite different. However, since the late 1970s, the rise of neoliberalism, which first appeared in Western societies, has created a strong isomorphic force to drive global health and medical systems to homogenize (Waitzkin & Hellander, 2016; Waitzkin et al., 2005). The best example of this transformation is perhaps from China. Its previous healthcare system, based on socialist units and public provisions, was transformed into a system based on the market logic by the end of the 1990s (Chen, 2001). In other words, the government withdrew from its role in health and medical provisions. In other societies, a similar phenomenon also takes place.
How do we explain this “great transformation?” A reasonable way is to look at how the neoliberal health reform is transmitted and implemented within the local society. In this regard, we argue that this great transformation, referring to the withdrawal of the government in health care provisions, is a dependency syndrome. Health and medical experts, scholars, and high government officials, are responsible for establishing institutions, setting goals, and implementing policies. In peripheral academic societies, scholars and high government officials are often educated in Western academic centers and therefore accept the mainstream ideology about the ideal health and medical system. This dependency on the ideas and concepts of the health and medical system further leads them to uncritically and unreflexively accept neoliberal health reform.
We briefly discuss three major syndromes in the health system in Taiwan. They are (1) over-medicalization of the system; (2) increasing commodification and marketization of the medical sector; and (3) the dominance of the ideology of market individualism in the system.
Over-medicalization
The term “medicalization” is commonly used in literature to indicate the phenomena in which an individual’s non-medical problems (e.g., alcoholism, suicide, and birth) are treated or handled as medical ones (Conrad, 1992; Zola, 1972). Most of the literature addresses the issue of medicalization at the individual level. However, the influence of the medicalization problem has gone beyond the individual level to that of the groups, institutions, and even the system. In this paper, we inquire into the impact of medicalization to the level of the system—the public health system in Taiwan. In 2003, Taiwan spent $18 billion USD in national total health expenditure for a population of 23 million individuals (Department of Health, 2005). However, out of this total expenditure, only 3.3% was used by the preventive sector. The data available from the Department of Health shows that this percentage has remained at this level since the 1990s: 3.0% in 1991, 1.8% in 1998, 2.4% in 1999, and 3.1% in 2000 (Chen, 2000; Department of Health, 1998, 1999, 2000). The situation has not improved in recent years. In 2018, the funding for the preventive sector accounted for only 4% of the national health expenditure in Taiwan.
Ironically, this development is in direct contrast to the past. One of the greatest achievements in the history of public health in Taiwan was the establishment of health stations during the 1950s in every district, in both urban and rural areas. The mission of these health stations was to provide: (1) health promotion and prevention programs such as maternal and child health, family planning, infectious disease control, chronic disease prevention, mental health, and general health education; (2) health administration and management for medical and pharmaceutical organizations and the monitoring of food manufacturing and delivery industries; and (3) the provision of primary medical care. From the 1950s to the 1970s, the primary function of the health stations were prevention oriented, focusing mainly on the first two aspects of the mission. For example, these health stations, with the support of local health departments, played an important role in the successful control of many infectious diseases, such as cholera, malaria, polio, smallpox, and tuberculosis, all of which were prevalent in Taiwan at that time. Public health workers in the health stations throughout Taiwan carried out disease control programs at the community level by, for example, making household visits, providing health education, and detecting and reporting possible cases of infectious disease. This was a period when the government set a much higher priority for the establishment and expansion of the preventive sector than for the medical sector. However, this policy was reversed during the 1980s because of the shift toward medical orientation in the government’s health policy (Chen, 2011, 2012).
Commodification and Marketization
Commodification of medical care is a precondition for the marketization of the medical sector. The commodification and marketization of medical care made the rapid expansion of the medical sector possible. Subsequently, medical entrepreneurs invested in the healthcare market to make profits. Since the investors had to ensure a certain profit rate so that their capital could accumulate and expand, they were more likely to invest only in those medical commodities with higher profit margins. Further, the medical market is different from other markets (e.g., shoes or computers) in that medical care is related to the individual’s own health—even their life and death. As a result, an individual who becomes ill has no choice but to seek medical care. Therefore, if manipulated by medical providers, consumers’ artificially created demands for medical care can be limitless. This condition provides medical capital with one of the most lucrative markets (McKinlay & Marceau, 2000). Consequently, the medical care market in Taiwan has attracted a great amount of capital. Through the continuous expansion and accumulation of capital, the medical sector has become much larger than the preventive sector in the past few decades, thus leading to the over-medicalization of the health system in Taiwan described above.
The government plays an important role in the degree of commodification and marketization in the medical sector. For example, public funding to the medical sector helps to lessen the extent of commodification and marketization. Conversely, public subsidization of the private medical sector can increase the medical sector’s levels of commodification and marketization. The Taiwanese government has been decreasing funding to public hospitals and increasing subsidies for private hospitals over the past few decades. As a result, private capital investments have clearly exceeded public funding in the medical sector in Taiwan. From the 1950s to present, increases in the number of private hospitals, clinics, medical providers, hospital beds, and nursing homes have been much greater than in public ones. As an example, Figure 1 demonstrates that the rate of increase for private hospital beds has exceeded that of public hospital beds since the 1980s.
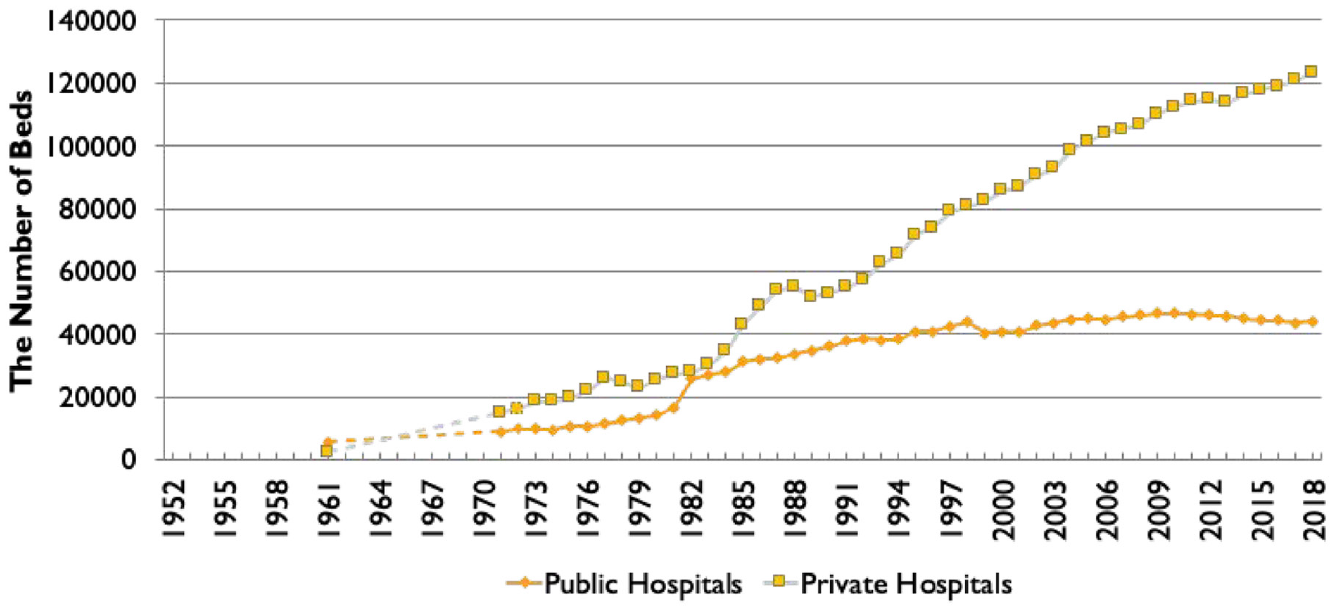
The increase of private versus public hospital beds, 1952 to 2018.
While the medical sector has been increasingly dominated by private capital, government funding for public hospitals has been decreasing. This can be seen in the significant decline since the early 1990s of the amount of public funds and the percentage of the total national health expenditure, which accounts for the governmental funding for public hospitals (see Figure 2). This situation has forced the public hospitals to compete with private hospitals in the medical care markets and subsequently to join the bandwagon for commodification and marketization. In fact, the management of many of these public hospitals has been contracted out to private capital firms.
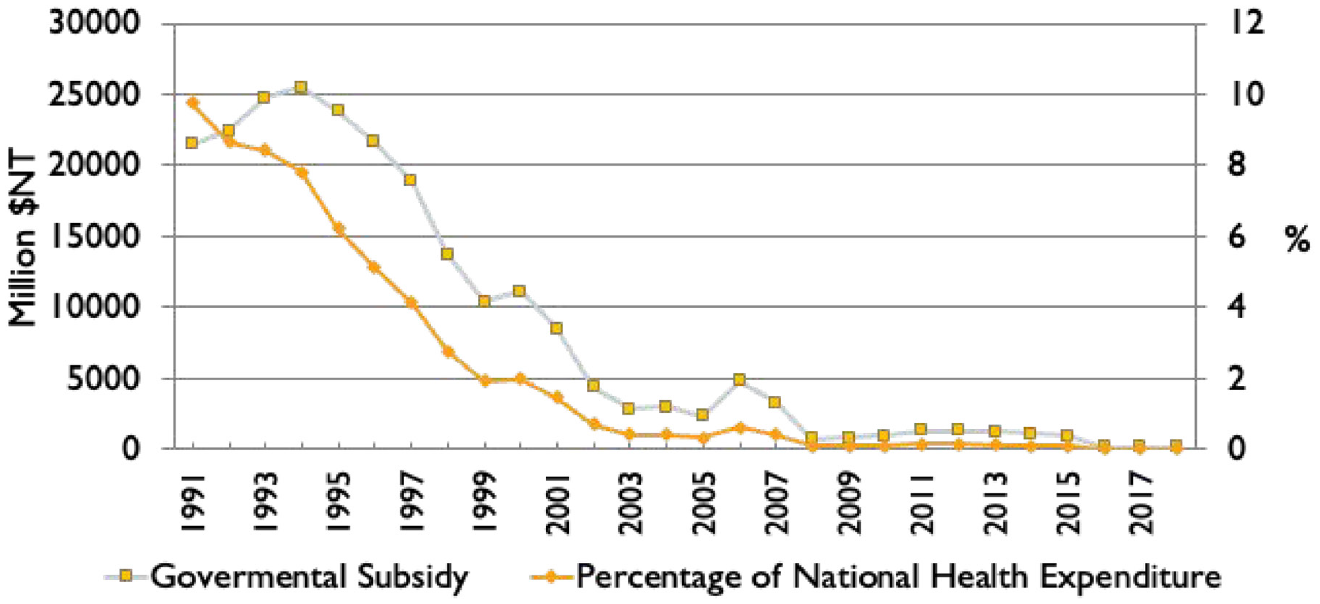
The change in the amount (left ordinate) and percentages (right ordinate) of governmental funding for public medical institutions in national health expenditure, 1991 to 2016.
Marketization further distorts the direction and content of medical education and hospital management. For example, during the SARS epidemic, most hospitals were dangerously lacking infection control specialists. It was later revealed that two factors partly contributed to this problem. First, infection control specialists earn a much lower income than those in other specialties. Therefore, fewer medical students choose infection control as their specialty. Second, the department of infection control at any given hospital rarely generates a profit, so most hospitals are reluctant to invest in its expansion or the training of its personnel (Chen, 2012).
Market Individualism
The final syndrome is the reluctance of public health professionals to challenge the worsening situation. This is mainly because of market individualism, a feature of neoliberalism, which has been dominant in the field of public health education and research, making it difficult for public health professionals to remain critical of the situation (Chen, 2003). Similar to what occurs in the West (Burris, 1997), this ideology manifests itself in Taiwan’s system in three dimensions: first, health and disease are primarily considered to be an individual’s responsibility; second, health issues that do not necessarily require medical treatment tend to be medicalized; third, medical services are considered commodities to be provided in a medical care market, and it is assumed that the individual will purchase these medical care commodities rationally (Chen, 2003, 2011). Market individualism was strengthened in the 1980s when neoliberal welfare reform was initiated in the Western world.
While a detailed description of market individualism informed by neoliberal thinking is beyond the scope of this essay, we would like to emphasize that the lack of an autonomous local community has led to the uncritical acceptance of this specific health and medical model. In the past few decades, market individualism has dominated the discourse in the field of public health. According to this ideology, an individual’s health maintenance and promotion is considered their own responsibility. Thus, in the United States, the United Kingdom, and many other parts of the West, the mainstream interpretation of causation for cancer, heart disease, hypertension, etc., is the individual’s unhealthy lifestyle (e.g., Crawford, 1977). This ideology has a profound impact on public health policymakers and health workers in Taiwan.
For example, health institutions blame the 10 leading causes of death in Taiwan mainly on people’s unhealthy lifestyles, and most health programs are designed around this mainstream ideology. Secondly, under this framework, the issue of personal health is medicalized. Access to medical care is often considered the major determinant of health (Burris, 1997). Many programs initiated by health organizations in Taiwan often reflect their tendency to medicalize health problems. One example is when top-ranked health officials promoted the erectile dysfunction drug Viagra by appearing at press conferences organized as a part of the drug manufacturer Pfizer’s publicity campaign. However, the Department of Health did not engage in a similar publicity campaign to promote public health education regarding the multitude of social, environmental, psychological, and other underlying factors that lead to male sexual dysfunction, or for the prevention of these health problems (Chen, 2003). Thirdly, market individualism further strengthens the commodification of medical care and the marketization of the provision of that medical care. From this perspective, the government’s role is merely to facilitate rational decision-making by ensuring the provision of adequate medical services as commodities.
Searching for Autonomy and Alternative Discourses: the PHL Movement
In the previous section, we outlined the “great transformation” of the health system in Taiwan from a collective and preventive style to a marketized and medicalized style. We also briefly mention the role played by researchers and policymakers in this process. The dependency on Western academic centers for ideas and concepts has helped to legitimize the marketized health system. Under these conditions, scholars of academic dependency theory may argue for the creation of an alternative discourse and the building of a local autonomous academic community. However, this is not as easy and straightforward a process as one may think. Alternative discourses may not have the opportunity to be voiced from the mainstream academic platforms because these outlets are generally under the control of biased gatekeepers. For example, one of the authors had an experience where his study, written about a Shanghai-based cancer patient organization with more than 20,000 members, was implicitly forced by a major China studies journal to identify this organization by the party propaganda machine during a review process. The paper was rejected because the authors refused to comply with the requests. The case demonstrates that alternative academic discourses are often stigmatized based on the dominant categorizing framework in which market individualism is treated as orthodox, while everything else (e.g., a collective patient group focusing on healthy lifestyles) is treated as heterodox.
In this situation, a sustainable alternative discourse cannot be just some dialog, conversations, or negotiations within the ivory tower. A truly autonomous academic community needs to generate alternative discourse while also bringing about change to the local society. The alternative discourse will remain alternative if it does not alter the base assumptions and daily practices derived from the academic centers. In the case of public health in Taiwan, generating a critical understanding of the global expansion of the neoliberal health reform is followed by the grassroots public health movement. In what follows, we will first discuss the PHL movement. Then, we discuss how the PHL facilitates the production of alternative knowledge on public health and medicine.
The PHL Movement
The PHL originated from the government’s failures in responding to the 2003 SARS epidemic. The movement can be roughly divided into two periods. The first period is between 2003 and 2008; in the first period, the PHL movement actively collaborated with another new social movement, the CUM. The CUM was initiated by a group of activist scholars, NGO workers, and grassroots intellectuals in the late 1990s. Its goal was to liberate knowledge and reform society (Lee, 2017). We note here that the first author of this paper (Lee) was involved in this movement. The overlapping of the instigators and the similarities in the movements’ goals created a natural affinity between the PHL and CUM. In the second period, post 2008, the PHL established its own organization, the Association for Promoting Public Health, and gradually ended its reliance on CUM as its primary partner.
After the SARS outbreak, the public recognized both the importance of the public health system and its weaknesses, and began calling for reform. With society more open to reform than ever before, a large group of about 200 committed public health scholars, students, and professionals, in collaboration with public intellectuals actively involved in the CUM, seized this opportunity and successfully developed a critical pedagogy program of public health for community universities. Among these 200 people, about 30—including public health scholars, community university activists, graduate students in public health and nursing programs, and a few seed teachers—participated in the initial planning, organization, implementation, and continued promotion of the program.
The program was designed in this manner: first, the program will use the community university system as the platform through which critical public health knowledge, concepts, and analyses will be liberated to people in the community. Second, the program will recruit public health and medical professionals and social scientists with strong interests in, passion for, and commitment to the transformation of the public health system. They will serve as “seed teachers” to offer critical public health courses at community universities. Through interacting and dialoguing with community members who enroll in these courses, the seed teachers will facilitate the community to critically analyze and deconstruct their interpretations of the public health system, and finally, will collectively transform the system (the latter, of course, is the long-term goal of this program). Third, every semester, seed teachers will attend an intensive educational program co-designed by the promotion team and other seed teachers. This program is composed of courses for critical public health knowledge and analysis provided by public health scholars. Fourth, to the extent the budget and human resources will allow, the program should be conducted at a large scale—recruiting at least 150 seed teachers and providing courses in 30 to 40 community universities across Taiwan every semester.
The promotion team is the engine of the program. The team members (which include the second author of this paper) are highly committed, passionate, and critical of the public health system and society as a whole. The team is responsible for the overall planning, integration of concepts, theory, and strategies, mobilization of program participants, close interaction and coordination with seed teachers and community university activists, as well as the publicization the program. Its work includes the following:
• Recruit seed teachers
• Design critical public health courses for seed teachers
• Organize and coordinate critical scholars to teach these courses through which they pose problems, provide critical analyses, and encourage seed teachers to question and to have dialog with these scholars
• Match public health seed teachers with community universities geographically near them
• Facilitate seed teachers by providing the critical public health courses where they learn from critical scholars, and to enroll students (members of the community) in their classes
• Facilitate the process for seed teachers to form regional support groups for their continuous critical pedagogy at their community universities
• Organize and hold conferences to broadcast the program to the public and collaborate with other non-government organizations
• Hold press conferences to publicize the program through media and other channels.
Seed teachers play a unique role in the PHL’s collaborative program with the CUM. Inspired by Paulo Freire’s critical pedagogy, seed teachers serve as students and educators in this critical pedagogical program (Freire, 1996). In general, most of the seed teachers obtained their academic degrees from traditional universities. However, the dependency means that traditional universities merely provide professional training (e.g., management skills) but lack critical perspectives that require students to think beyond the status quo. Therefore, the education for seed teachers combines two types of courses: (1) critical public health perspectives and analytical skills; and (2) Freirean pedagogical methods. After this education, the seed teachers will then provide critical public health courses at the community universities that are adapted with layperson language and based on Freirean methods. Seed teachers thus occupy a dual role in the PHL movement. When they themselves participated in the educational program, they were the students. They receive critical public health education and Freirean pedagogy from critical scholars organized by the promotion team of this program. However, during the semester, they become educators themselves, providing critical public health courses at their assigned community universities to the public. Hopefully, this will attract more people to become seed teachers in the future and broaden the influence of the PHL. Furthermore, while seed teachers are liberating public health knowledge at the community universities, they are on the frontlines of the PHL movement. It is hoped that they will take on promotional and leadership roles in the future movement to transform the public health system.
In addition, the promotion team developed several organizational strategies to facilitate the collective enrichment and personal growth of seed teachers and movement participants. First, regional associations of seed teachers have been organized. The functions of these informal associations include, for example, providing support and resources for teaching and student enrollment, organizing study groups, planning and organizing conferences, and coordinating with the promotion team and participating in the planning of program activities. Second, every semester, the promotion team organizes a seminar for all seed teachers to share their experiences at their community universities. Third, the promotion team and the regional association of seed teachers together hold conferences with critical regional public health issues as the central theme. The key speakers at the conference include public health scholars and NGO representatives active in regional public health activities. The purpose of the conference is not only to enrich the seed teachers, but also to establish collaborative relationships with regional NGOs and public health scholars. Fourth, the promotion team publishes a monthly electronic newsletter which includes articles discussing and analyzing conceptual and theoretical issues in public health, reporting the activities related to the program, reporting seed teachers’ teaching experiences, and announcing new activities. Fifth, an email discussion group—named “phlib,” representing PHL—has been formed so that seed teachers from all over Taiwan can communicate and discuss in cyberspace without any time or space barriers. This email listserv includes not only seed teachers but the promotion team, scholars involved in training seed teachers, and other community university activists. Sharing experiences and discussions about important public health issues are the most common occurrences in the email listing. Finally, a website, www.phlib.org.tw, has been established to provide announcements about activities, posts on relevant articles and teaching materials, and to hold group discussions. The website also serves as the official website for the Association for Promoting Public Health.
Alternative Knowledge
The PHL movement creates alternative discourse against the dominant ideology of global health reform through three major routes—building a collective teaching and learning community, an autonomous research agenda, and nurturing critical scholarship. For example, the subjects of the courses offered in the CUM were determined collectively through multiple channels: (1) discussions among seed teachers, community university activists, the promotion team, and students enrolled in the courses; (2) discussions among scholars engaged in offering critical public health courses to seed teachers; and (3) the availability of a critical scholar who is capable of providing a rich and profound critical analysis of the subject. The scope of the courses includes infectious diseases, chronic diseases, work-related stress, health protection and promotion, the public health system, and media. The substantive critical issues discussed include medicalization, commodification, marketization, and privatization in the public health system, market individualism and its impact on the public health system, the stigmatization of disease and illness, gender, class, the role of the state, international monopoly on capital, a political economic analysis of the public health system and occupational health and safety, power and patient-provider relationships, and the corporatization of the medical sector. These issues were chosen through ongoing discussions and reflections between the actors mentioned above and based on the theoretical framework and the participatory action research of the PHL movement.
The PHL’s promotion team continues to search for critical scholars working in health and medicine. They primarily look for individuals with autonomous research agendas and those who can reveal deep problems, provide critical analyses, and suggest possible transformative actions. In this regard, the criteria for the critical scholar’s selection is similar to the definition of academic autonomy advocated by S.H. Alatas (2006). It includes the following: (1) they have established rigorous and critical scholarship; (2) they have a strong passion for and commitment to transforming the public health system and subsequently society as a whole; and (3) they identify with the cause and mission of the program’s initiatives and the community universities. Critical scholars’ course content is often the results of their rigorous actionable research. For example, one of these critical scholars—the second author of this paper—taught a class titled “a historical and political economy of the rise and decline of the health stations in Taiwan,” for both regular college courses and a CUM course. To her surprise, she was informed that this kind of class had never been taught in public health and medical schools in Taiwan before. The content of this course was the result of her action research and in-depth interviews with seed teachers, many of whom were health station workers and directors, and a historical analysis of the development of health stations in Taiwan. In short, her autonomous research agenda helped the public to understand the importance of health stations, the value of which has been forgotten in the mainstream discourse.
In the past two decades, in addition to publications by several key activist scholars (e.g., Chen, 2011), the PHL has nurtured a group of young researchers in regular academic institutions. The second author of this essay has advised 16 master’s level theses in the department of public health at a major medical school in Taiwan. These theses substantively differ from the typical theses at other public health schools. Several of these theses are dedicated to demystifying and destigmatizing the popular perceptions of the indigenous population. For example, Chen (2007) and Kao (2010)‘s theses remind us of the importance of the worsening social economic status of indigenous people in understanding their health status, as well as the political and economic causes of this problem (e.g., tuberculosis and alcoholism). Another cluster is dedicated to understanding the effects of marketization and medicalization on the public health sector. For example, Chang (2009)‘s study finds that the disengagement of the earlier public health stations with the local community is the result of the marketization and over-medicalization of the public health sector. Over-medicalization disproportionately increases doctors’ social status, but at the same time weakens other health professions’ status (Chang, 2003). Ironically, Chen (2022) argues that physicians are now proletarianized because most are now hired by giant medical corporations. Interestingly, after graduating from graduate school, some of these students became dedicated activists working in the PHL movement and social sectors.
Conclusion: PHL, Challenges for Alternative Health Models, and China
In this essay, we critically reflect on the idea of alternative discourses and autonomous academia and apply it to the case of the grassroots public health movement in Taiwan. We argue that the issue of over-medicalization in the public health system and the commodification and marketization of the medical system should be viewed as a syndrome of dependency because most of the public health policies are designed and implemented by high ranking officials, mostly scholars trained in Western academic centers. Without understanding the linkage between academic knowledge production and policymaking, efforts to change the existing system will fail. Our discussion, therefore, shows a critical insufficiency in the existing discussion on academic dependency and academic autonomy. The dialog is mostly centered on the academic ivory tower, and at first glance it would appear that scholars should be able to overcome the issues of academic dependency on their own. However, our study on the PHL movement shows that ideas (e.g., medicalization and the market-based healthcare system) are generated within the university system. Once they are established, they begin to take on lives of their own. In return, the institutions founded on these ideas further shape the thinking and operations of academia. The dependency of academia and intellectuals on certain centers cannot be separated from the dependency of these peripheral areas on other areas (e.g., economy, culture, and defense). Lee and Chen (2022)’s study shows that even as they top the global university rankings, social science departments in East Asian universities still heavily rely on Western academic centers. Under this dependency, the knowledge produced by the universities in these peripheral societies is deemed to fit within the global division of social science knowledge. As a result, periphery produces raw materials to be consumed and refined by the center.
In this dependent situation, as mentioned above, the critical public health scholars and activists of the PHL movement in Taiwan, in their enormous efforts searching for and developing their own autonomy in health and medicine, were inspired by the alternative health models in countries such as China, Nicaragua, and the Philippines. Have these models been able to change this dependent situation in the past decades? The results are mixed. At the end of this short essay, we would like to briefly discuss the challenges faced by peripheral countries struggling to fight against global neoliberal expansion and the implications of the rise of China within this neoliberal capitalist reform. For the past few decades, the trend of US corporatization has overshadowed the global neoliberal turn. Private health capital, with the dominance of US firms, many of which are multinational, is rapidly spreading internationally. This trend undoubtedly will monopolistically influence national and international health policies. The peripheral countries, like Nicaragua and the Philippines, although their peoples have struggled heroically for independence in health and medicine, have been historically under the tight control of the US empire. Moreover, countries like Nicaragua and the Philippines in the past two to three decades have been under regime changes, and thus prone to unstable political conditions. As a result, it is unclear whether the efforts toward alternative health models will be sustainable in the long term.
China’s prospects for alternative health models may be more positive. Although as we have mentioned, China’s economic reforms since the 1980s have fundamentally changed its early collective-style medical and public health tradition into a system similar to the market-based medical system. This great reversal has brought about serious social issues, such as deteriorating doctor–patient relationships. However, since 2009, the Chinese government has changed its stance on its previous marketization policies. The perspective that medicine and healthcare belong to the public realm is further strengthened in several recent government statutes. In the ongoing COVID-19 pandemic crisis, China is the only non-Western country that has the capacity to research and manufacture vaccines on a large scale. It also donates the largest amount of vaccines to developing and underdeveloped countries. Viewed from this angle, China’s rise, at least, may serve as a balancing power to the ever expanding neoliberal health reforms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.