
Abstract
In this paper, the authors develop a model of psychoanalytic clinical reasoning as the inferential process by which analytic therapists are able to arrive at an understanding of the clinical material. Starting from Bion’s theory of functions, the authors propose that a “function” can be thought of as a condition-action sequence that analytic therapists implicitly use to respond to certain configurations of elements in the material by executing conceptual or reflective operations. To investigate the main families of functions that are used by analytic therapists in everyday practice, the authors used an interpersonal process recall procedure based on supervision sessions from a theoretically heterogeneous group of participants. A consensual procedure was developed to identify operations, spell out the underlying functions, and group functions into families. Twelve families of functions were identified that appear to be used by analytic therapists regardless of their schools of thought. The authors call them the “operators” of psychoanalytic clinical reasoning. According to the operators model, the process of psychoanalytic clinical reasoning consists in the chaining together of operations using functions from different families. A specific collection of “clinical reasoning styles” seems to be interwoven in this process. Different avenues open up for research, clinical practice, and training.
Keywords
For present purposes, we are going to define clinical reasoning (CR) as the inferential process by which a therapist is able to pass from A to B, where A is the clinical material that is available about a case, and B is a relatively improved understanding of that material. By “clinical material,” we mean any information that is available about a case (as obtained, for instance, through a patient’s verbal communications or observable behavior), as well as any reaction of the therapist to that material, such as feelings or thoughts elicited by it. In turn, we assume that the understanding that is developed through CR can be used for two purposes: case conceptualization or reflective practice. Case conceptualization refers to the development of a hypothetical explanation of the factors causing and maintaining a patient’s difficulties. Reflective practice refers to the practical management or handling of the case, such as the planning and evaluation of intervention strategies. Although conceptually distinct, these two purposes of CR are seen as interrelated: consulting a conceptualization, in fact, can help a therapist to decide how best to intervene; just as reflecting on the effects of an intervention can help them redefine their conceptualization.
According to this working definition of CR, in order to pass from A to B, therapists will have to possess two kinds of skills: conceptual and reflective skills. Conceptual skills are needed to mentally manipulate the clinical material. They include, for example, the skills involved in selecting certain elements of the material, linking them together, or interpreting them in a new way. Reflective skills, on the other hand, are needed to adopt and maintain an optimal state of mind whilst carrying out the conceptual work. If conceptual skills are like “moves” that the therapist carries out on the clinical material (Schön 1983, p. 134), reflective skills are more like “positions” or “postures” that they maintain in order to monitor and regulate the CR process (Rober et al. 2008). If the process of passing from A to B can be compared to that of riding a bike, then conceptual skills are similar to the act of pedaling in order to advance, while reflective skills are more like the act of maintaining the balance as one is advancing.
Toward a Model of Psychoanalytic CR
In this study, in particular, we are concerned with the development of a model of psychoanalytic CR, as the process by which psychoanalytically oriented therapists are able to develop an understanding of the clinical material. The term “psychoanalytically oriented therapist” is used here in a purposefully generic way, to avoid associating our model to any specific school of thought. We acknowledge, in fact, that the task of CR will not be approached in the same way by a Freudian, an object relational, a Lacanian, or a Jungian therapist. Yet, as important as these differences may be, we do not wish to factor them in our model. Rather, we wish to remain at a previous level of generality, where the question is whether there are any common features to the way in which analytic therapists, regardless of their school of thought, are able to pass from A to B.
In particular, the aim of the study is to develop a descriptive model of the logic of psychoanalytic discovery. A “descriptive model” of CR is one that outlines what analytic therapists actually do in their everyday practice. This is in contrast to a prescriptive model, whose aim is to outline what they should do (e.g., Kligman 2010). On the other hand, the “logic of discovery” regards the steps that analytic therapists follow to arrive at an understanding of the clinical material. This is in contrast to the logic of justification, which regards the criteria by which such an understanding may be said to be valid (e.g., Isaacs 1939). 1
So, what are the inferential steps by which analytic therapists are able to arrive at an understanding of the clinical material in their everyday practice? On this point, the literature is surprisingly meager. Ramzy (1974) was one of the first to point out this gap: Unbelievable as it may sound, in the whole vast library of psychoanalysis—clinical, theoretical, technical or applied—there are hardly any references which outline the logical guidelines or the methodological rules which the analyst follows in order to understand his patient. (p. 36)
To address this gap, Ramzy (1974) resorted to a method which consists in the close examination of excerpts from analytical sessions. The idea is that, by studying in detail the “mental operations” by which an analytic therapist was able to arrive at certain conclusions on a particular case, we may reconstruct some of the underlying “rules of inference” (p. 550). In this way, for instance, Ramzy was able to document the implicit use made by analytic therapists of a principle of temporal contiguity, according to which elements of the clinical material that occupy a near point in time are assumed to be connected. A similar method was used by other authors to reconstruct the rules of inference that analytic therapists seem to rely on in their everyday CR (Ivey 2000; Meehl 1983; Peterfreund, 1975; Wolitzky 2007). However, such a method, grounded as it is on purposefully selected clinical vignettes and often on a single author’s reflection, is bound to remain anecdotal and unsystematic.
A search for more systematic methods was initiated by the European Psychoanalytic Federation (Canestri 2006, 2012). The comparative clinical methods working party, for instance, devised a method that involves group discussions with therapists from different analytic societies (Tuckett 2006). During these discussions, a clinical case is presented by an analytic therapist; then, the whole group works to reach consensus around a description of the analytic process by generating categories to classify the therapist’s interventions. The advantage of this method is that it reduces the influence of any single author’s perspective, as it is based on the integration of multiple points of view. However, the main limitation is that the analytic therapists who take part in such clinical case conferences tend to do so as analytic therapists, not as researchers. As already noted by Ramzy (1974), this poses a problem of “circular thinking” (p. 544), if the language that they use to describe the process of psychoanalytic CR is a psychoanalytic one. In fact, even if the participants are able to reach a consensus in this way, they are inclined to rely on their prior constructs and terminology thus recognizing in what they hear such phenomena as resistance, transference, defenses or the like. In other words, they go directly to conclusions rarely, if at all, spelling out the steps they have followed to reach them or noting the evidence or the reasons that led them to reach the particular understanding of what they have observed. (p. 544)
In the present study, we also used group discussions aimed at consensus building. However, to avoid the risk of circular thinking highlighted by Ramzy (1974), we made it a rule to avoid the use of any psychoanalytic jargon to describe the process of psychoanalytic CR.
Bion’s Theory of Functions
The theoretical starting point for our model of CR was Bion’s (1962) theory of functions. This theory was an attempt by Bion to formalize the process by which analytical therapists understand the clinical material. To do so, Bion built on Kant’s theory of knowledge, and specifically on the distinction between the content of knowledge (that is seen as coming from experience) and the forms of knowledge (that are seen as existing a priori). Just as human beings use certain a priori categories to organize the content of experience in general, so analytic therapists may be assumed to use certain a priori categories to organize the clinical material. Bion called these categories the functions.
Bion’s choice of the name function has to be understood as a mathematical metaphor. With this metaphor, Bion (1962) wanted to express how these a priori forms are like an unknown “variable” that is “devoid of meaning” in itself (p. 3). It is only when the variable is invested with a fixed “value” (p. 3)—which Bion calls a factor—that the function takes on meaning. But the purpose of the metaphor was also to underline how functions, in their “flexibility,” remain “constant,” while factors, being fixed, tend to be “replaced” (p. 38). In practical terms, this means that the clinical material at hand always changes: today it is a patient, tomorrow it is another; this session it is a certain story, the next it will be another. But as the content of CR changes, there must be something that does not—and these are the forms that are used to understand it. Still, such forms are meaningless in themselves, until they are applied to a concrete case. They are like Kant’s “empty thought,” which, in its abstractness, is empty until it is filled by the “qualities” of a particular experience (p. 91).
But what makes Bion’s theory of functions particularly interesting as a starting point to develop a model of psychoanalytic CR is that, for him, even theories or concepts are but one of the factors that a function can entertain. Theories and concepts, for Bion (1962), are not the forms that analytic therapists use to understand the clinical material; rather, they are only one of the kinds of content that functions can be filled with, besides the elements of the clinical material (p. 2). Bion gives the example of an analytic therapist who is working on a clinical case: at a certain moment, a particular theory or concept may be “a major pre-occupation” of theirs; but “in subsequent weeks,” as the case evolves, another factor may take its place (p. 39). In this sense, the utility of a theory of functions remains “whatever the function and whatever the factors” (p. 39).
The fact that Bion saw his theory of functions as a theory of the process of analytic understanding—regardless of the content coming from the case at hand and of the theories or concepts that are entertained at any moment—explains why he did not think of his theory as one among others. According to him, his theory of functions did not “diminish or increase existing psycho-analytic theories” (Bion 1962, p. 89), for it was not a theory of any clinical phenomenon per se, but a theory of how analytic therapists think about clinical phenomena in general. That is also why, in developing his theory, Bion refrained from using well-established psychoanalytic concepts such as “counter-transference” or “defense mechanisms.” Rather, he resorted to a mathematical and philosophical language, precisely to maintain a distinction between specific theories or concepts, which are only some of the “thoughts” that can enter the process of thinking, and “thinking” itself. Yet at the same time, Bion (1962) claimed a right to redefine these terms in his own way: It may seem that I am mis-using words with an established meaning, as in my use of the terms function and factors. A critic has pointed out to me that the terms are used ambiguously and the sophisticated reader may be misled by the association of both words with mathematics and philosophy. I have deliberately used them because of the association, and I wish the ambiguity to remain. I want the reader to be reminded of mathematics, philosophy and common usage. . . . In psychoanalytic methodology, the criterion cannot be whether a particular usage is right or wrong, meaningful or verifiable, but whether it does, or does not, promote development. (pp. vi–vii)
A Revised Theory of Functions
Although a useful starting point, Bion’s theory leaves many questions unanswered. For instance, Bion did not specify how many functions there are, nor did he flesh out the steps by which analytic therapists use them to select elements from the clinical material, link them, or carry out other essential tasks. Furthermore, the way in which Bion uses the key terms in his theory remains ambiguous. As noted, part of this ambiguity was intended—Bion (1962) wanted to “retain” the “penumbra of associations” that his chosen terms evoked (p. vi). Yet part of it may have been due to a lack of systematicity on his part. In what follows, we propose a revision of Bion’s theory that aims for greater precision. In our revised version, we will retain some of the terms that Bion used: notably, function, but also operation. However, just like Bion, we claim a right to redefine these terms in our way, and ask that our usage be judged by the same criterion invoked above, namely, not so much whether it is “exact,” but whether it will be fruitful for other analytic therapists and researchers in the field.
We define an “operation” as any kind of mental act that an analytic therapist carries out in order to pass from A to B. In line with our definition of CR, we envision two kinds of operations: those that the therapist carries out for the purpose of mentally manipulating the clinical material (conceptual operations) and those that the therapist carries out for the purpose of adopting the right “position” or “posture” (reflective operations). We define a “function” as an operation, minus the content that comes from the particular case at hand. This definition is based on the same Kantian epistemology that Bion’s theory of functions was based on. We see a function as an “empty form” that has to be filled by an element of the clinical material in order to give rise to an operation.
To understand the relation between functions and operations, as we define these terms, let us take a mental act that Freud (1925) reported carrying out in his clinical practice. Freud gives two examples of this mental act. In the first example, the patient says, “I did not mean to insult you,” from which Freud infers, “I did mean to insult you.” In the second example, the patient says, “This person in the dream is not my mother,” from which Freud infers, “This person in the dream is my mother.” These two examples can be seen as conceptual operations, as they have to do with the mental manipulation of something that the patient said, rather than with the reflective positioning of the therapist. Now, these operations were carried out and reported by Freud in a specific theoretical context—namely, his theory of negation. However, let us abstract from this context and focus on the operations only from the point of view of the relation between content and form. If we do so, we may notice that, in the two cases, the content is different. In one case, it is about the patient insulting someone; in the other, it is about the identity of a person in a dream. Because the content is different, then so are the two operations. However, what is common to both is their form—that is, their underlying function. In this case, the function may be spelled out as the mental act of taking a negative proposition uttered by the patient (¬A) and reverting it into a positive one (A).
This example illustrates our approach to the study of functions as forms that can be abstracted from the theoretical context and from the content coming from the case at hand. However, this example should not give the impression that the process of CR, as we understand it, consists merely in the process of drawing logical inferences. Functions, in fact, may be said to work like “rules of inference” (Ramzy 1974, p. 550) or “if-then” rules. However, in the context of CR, these rules do not work as they do in classical logic. The function above, for instance, does not work as a rule establishing that conclusion q (“This person in the dream is my mother”) must follow from premise p (“This person in the dream is not my mother”) out of logical necessity. Rather, it works as a practical rule establishing that, whenever an analytic therapist is faced with a certain configuration of elements in the clinical material (e.g., the situation where a patient insists that something is not the case), then the execution of a certain mental action is recommended (e.g., the conceptual reversal of whatever the patient is saying). In other words, functions work as condition-action sequences by which analytic therapists are able to respond to certain configurations in the clinical material by executing certain conceptual or reflective operations.
Methodology
Our redefinition of functions as condition-action sequences tells us something important about the kind of knowledge that we wish to formalize in our model. It tells us that this knowledge is not one that analytic therapists are likely to possess in an explicit way, but rather in an implicit or tacit way. Condition-action sequences, in fact, are the main form that procedural knowledge takes, as opposed to declarative knowledge (cf. Binder 1999, p. 711). To go back to our initial analogy, analytic therapists may “know” how to pass from A to B in a similar way in which one is said to know how to ride a bike. The knowledge involved is not knowledge of any number of facts, nor one that can be easily verbalized. Rather, it is knowledge of a process: one that is difficult to explain in words and that is better demonstrated in action. 2
That is why, to formalize the implicit knowledge of analytical therapists, it may be useful to adopt some of the methods that have been described in the literature on professional knowledge. This field of studies deals precisely with the question of the “knowledge-in-action” that is mobilized by competent professionals in their everyday practice (e.g., musicians, athletes, chess players). In particular, in the present study, we decided to adopt a method proposed by Schön (1983), which consists in the analysis of transcripts from supervision sessions. Schön believed that, to study how the knowledge that defines competent practice in a profession is produced, structured, and transmitted, we need to observe practitioners (a) while they are at work on a concrete problem and (b) under conditions in which they are most likely to make their knowledge “public” (p. 74), that is, explicit. These, argued Schön, are conditions “in which a senior practitioner tries to help a junior one learn to do something” (p. viii).
In the present study, we adopted Schön’s method and studied transcripts of psychoanalytic supervision sessions. This method has several advantages. First, it helps solve the problem of defining what constitutes competent practice in psychoanalysis (cf. Tuckett 2005). While the working party of the European Psychoanalytic Federation, for instance, solved this problem by inviting to its groups only a selected few “well-respected and reputed analysts” (Tuckett 2006, p. 170), in our study we rather used status as supervisor as a proxy for competence in CR, invested as it is by a socially recognized educational role in the analytic community. Second, this method is in line with recommendations by other scholars who have attempted to formalize the implicit knowledge of analytical therapists. Canestri (1999), for instance, laid out some methodological proposals to study this knowledge in an empirical way. His first proposal, indeed, was to study supervision, which he saw as “an ambiance that comes as near as is possible to the private reality of the analytic situation” (p. 187).
However, one problem remains: namely, that although the CR process becomes relatively explicit in supervision, much of it remains implicit, even there. This problem was pointed out already by Schön (1983), who noticed how, in a typical session, the supervisor seems to be guided by a system of implicit rules that they use, but do not describe to the supervisee: the supervisor “reflects-in-action,” but does not “reflect on his reflection-in-action” (p. 126). That is why, in the present study, we decided to complement the study of supervision sessions with an additional procedure known as interpersonal process recall. This procedure is widely used in psychotherapy research for the in-depth study of conceptual and reflective processes (Burgess, Rhodes, and Wilson 2013; Hill, Crowe, and Gonsalvez 2016; Rober et al. 2008). In our study, the procedure went as follows. First, pairs of supervisors and supervisees were asked to audio record a session in their naturalistic setting. Then, at the supervisor’s earliest convenience (usually 1 week after the supervision session), a 2-hour online interview was organized on Zoom. During this retrospective interview, the recording of the session was played back in its entirety, and the supervisor was asked to stop it whenever a significant conceptual or reflective process had taken place in them at that time in the session. The supervisor was then invited to explain that process in as much detail as possible.
Participants
The study was approved by the ethics committee of the Psychological Sciences Research Institute at the Université catholique de Louvain. To recruit participants, a brochure was circulated among psychoanalytic training institutions and associations in Europe, inviting pairs of supervisors and supervisees to take part in the study. Supervisors were required to be psychoanalytic psychotherapists with an official supervisory role in a training institute; supervisees were required to be undergoing or have completed a training program as psychoanalytic psychotherapists.
Twelve pairs of supervisors and supervisees participated in the study. Seven pairs were from Italy, four from Belgium, and one from the United Kingdom. The interviews were conducted by the first author in the supervisor’s preferred language (French, Italian, or English). Two supervisees were still undergoing their training program, while 10 had completed it. The supervisors were 9 psychologists, 2 psychiatrists, and 1 social worker. The supervisees were 10 psychologists, 1 social worker, and 1 counselor. More information about the participants can be found in Table 1. Each pair is identified with a number referring to the chronological order with which they contacted us.
Personal and Professional Characteristics of the Pairs of Participants
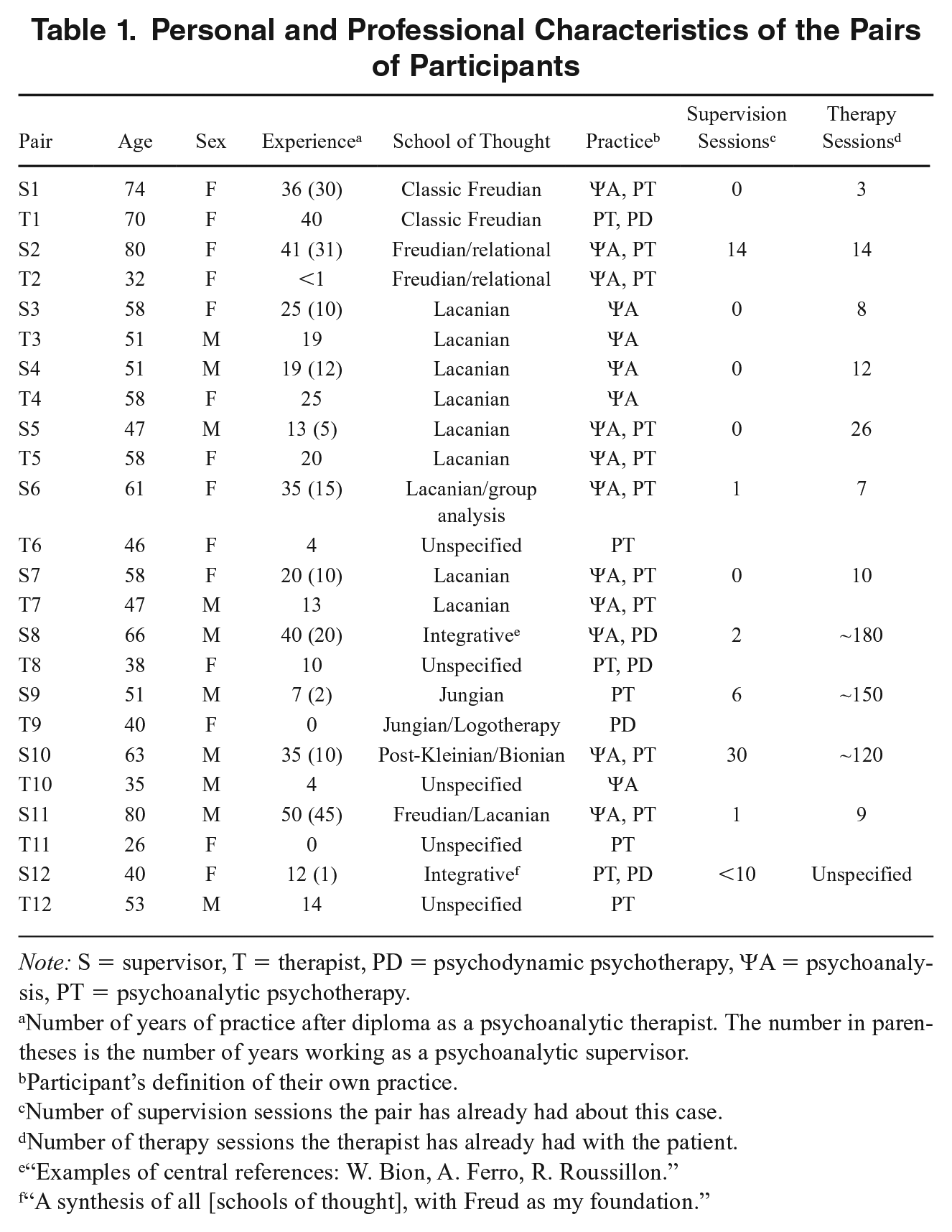
Note: S = supervisor, T = therapist, PD = psychodynamic psychotherapy, ΨA = psychoanalysis, PT = psychoanalytic psychotherapy.
Number of years of practice after diploma as a psychoanalytic therapist. The number in parentheses is the number of years working as a psychoanalytic supervisor.
Participant’s definition of their own practice.
Number of supervision sessions the pair has already had about this case.
Number of therapy sessions the therapist has already had with the patient.
“Examples of central references: W. Bion, A. Ferro, R. Roussillon.”
“A synthesis of all [schools of thought], with Freud as my foundation.”
Four couples formed spontaneously to take part in this study, while eight were preexisting. The pairs that formed spontaneously (Pairs 3, 4, 5 and 7) were constituted by a group of four Lacanian supervisors who are colleagues at a training institute. Instead of recording a session with one of their supervisees, these participants proposed to split into two pairs and record each two sessions: one in which an analyst brought a clinical case and the other acted as their supervisor, and a second session in which the roles were reversed.
Patients included six female and six male patients (one elder, seven adults, three young adults, and one adolescent). Cases covered a wide spectrum of clinical issues, from everyday difficulties to severe psychopathology. Clinical issues included posttraumatic stress, sexual abuse, occupational burnout, social withdrawal, domestic violence, obsessive-compulsive symptoms, and relational problems. In most cases, a formal diagnosis was not formulated, with the exception of one diagnosis of “hysteria” (Pair 3) and two of “ordinary psychosis” (Pairs 4 and 5).
Data Analysis
The aim of data analysis was to identify the main classes of functions that are implicitly used by analytic therapists. To do so, we developed a procedure for the classification of functions. This procedure resembles the one used in the “item generation” phase of measure development, where a certain domain is mapped through the identification of its constituent dimensions (Hinkin 1995). Similarly, our analysis was guided by the search for a minimum sufficient number of descriptors for the process of psychoanalytic CR.
There are two main approaches to item generation. A deductive approach (or “classification from above”) works by applying to the data categories that have been derived from a review of the literature or from theory; an inductive approach (or “classification from below”), on the other hand, works by generating new constructs from the data (Hinkin 1995, p. 969). In this study, we used the latter approach. Our procedure, in fact, was informed by our revision of Bion’s function theory; yet, this theory did not provide any insight into the content of functions, nor into the number or kind of classes of functions. The categories were thus not preexisting, but generated through data analysis.
To prepare the data for analysis, the recordings of the supervisor session and of the interview were transcribed ad verbatim. Identifying details were removed and data were pseudonymized using P for patient, T for therapist, and S for supervisor, followed by the number identifying each pair. The transcripts of the supervision session and of the interview were merged into one document. Both transcripts (session and interview) were analyzed as data for each pair. The data were analyzed in three steps: (a) identifying operations, (b) spelling out the underlying functions, and (c) grouping functions into families.
Identifying Operations
Data analysis was conducted on instances of CR. Because the process of psychoanalytic CR occurs in a dialogue between two persons, an “instance of CR” was defined liberally as (a) any CR process that the supervisor verbalizes during the session; (b) any CR process that occurs at the time of the session, which the supervisor does not verbalize to the supervisee, but which they verbalize during the interview; and (c) any CR process that the supervisee verbalizes during the session, with which the supervisor agrees. Within instances of CR, the task was to identify operations. As noted, operations were defined as any kind of mental act that an analytic therapist carries out in order to pass from A to B, whether for the purpose of case conceptualization or reflective practice. It was assumed that an instance of CR could contain more than one operation (e.g., in the case of a long supervisory intervention).
Spelling Out Underlying Functions
Once an operation was identified, the task was to spell out the underlying function. This was done by removing from the operation the content that came from the case at hand. To illustrate, let us take an operation that was carried out by S6. During the session, T6 was telling S6 how P6 had always been a “model-child.” During the interview, S6 explained that, as she listened to this element of the clinical material, she thought that T6 might have been talking about herself, as she also happened to have always been a “model-child.” This mental act can be seen as a conceptual operation, as it consists in the mental manipulation of something that the supervisee said. If we abstract from the content that comes from the case at hand, then the function underlying this operation may be spelled out as the mental act of taking something that A says about B, and inferring that A may be talking about themselves.
In spelling out the function underlying an operation, researchers can rely on (a) the context in which the operation appears, as well as (b) any explanation that the supervisor might have left about the CR process behind that operation. Importantly, (b) is not always available. This is typically the case of operations that are contained in an intervention that the supervisor made during the session, but for which they left no comment during the interview (e.g., because they did not decide to stop the recording of the session at that particular point). In such cases, researchers have to spell out the function using context alone, an activity that is obviously going to involve some degree of inference on their part. But even when the supervisor’s explanation of the CR process behind a certain operation is available, the activity of spelling out the underlying function remains necessarily inferential. Supervisors, in fact, do not think explicitly in terms of functions; rather, functions have to be extracted from what they say. This is why researchers have to spell out functions as descriptively as possible, to limit the introduction of extraneous elements with their own inferences.
Grouping Functions Into Family
The next step is to group functions into classes or, as we rather call them in our model, into families of functions. In mathematics, a “family of functions” is a set of functions whose equations have a similar form. In the context of CR, a family of functions may be defined as a set of functions that respond to the same core idea. To illustrate, let us take an operation that was carried out by S8. T8 was telling S8 how P8 and his mother “almost formed a couple.” During the interview, S8 explained that, as he listened to that element of the clinical material, he thought that T8 might have been talking about P8 and herself, who also “almost formed a couple.” If we remove the content that comes from the case at hand, then the function underlying this conceptual operation may be spelled out as the mental act of taking something that A says about B and C, and inferring that they may be talking about B and themselves. Now, if we compare this function with the previous one from Pair 6, we can see that they are not identical. However, the “form” of the two functions may be said to be similar. In both cases, in fact, it is about taking something that a person said and reflecting it back to themselves, as in a mirror. The final step is thus to find a name for the family that best expresses the core idea to which its functions seem to respond. In this case, for instance, to express the core idea of a mirrorlike reflection, the family that grouped the two functions in question was eventually called “Self-reflective” (see Table 2).
The 12 Operators of Psychoanalytic CR
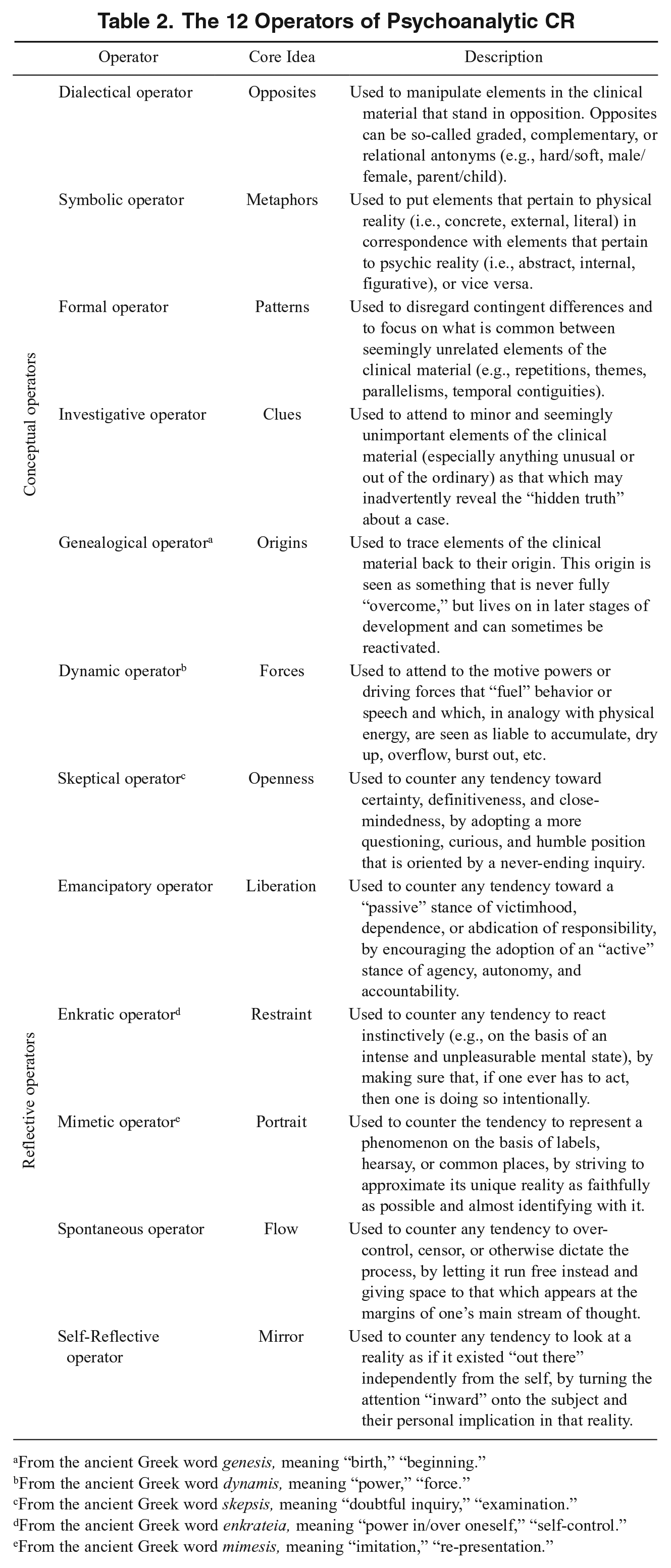
From the ancient Greek word genesis, meaning “birth,” “beginning.”
From the ancient Greek word dynamis, meaning “power,” “force.”
From the ancient Greek word skepsis, meaning “doubtful inquiry,” “examination.”
From the ancient Greek word enkrateia, meaning “power in/over oneself,” “self-control.”
From the ancient Greek word mimesis, meaning “imitation,” “re-presentation.”
Data were analyzed by the three authors. After independent coding of the transcripts from each pair, a consensus session was held. During these sessions, we discussed what functions had been identified and how best to group them into families. When there was disagreement on the function underlying an operation or on the core idea that could be used to define a certain family, we went back to the data and tried to ground both in passages from the transcripts. As we moved from a within-case to a cross-case analysis, the grouping of functions into families underwent some adjustments. These adjustments were guided by the striving to ensure that (a) the core idea defining a family was the “best fit” for the functions that it grouped (homogeneity); (b) the families had a minimal conceptual overlap between them (independence); and (b) each family could be documented to be used in most or all of the pairs (generality). The last criterion was added under the assumption that the use of functions in a certain pair might have been due to idiosyncratic characteristics of the participants (e.g., their schools of thought) or of the case (e.g., the type of patient difficulties).
The Operators Model Of Psychoanalytic CR
We identified 12 families of functions that were used in most or all pairs, regardless of the participants’ school of thought or the particular case at hand. We call them the operators of psychoanalytic CR. Operator is another term that we take from Bion (1963, p. 19), but that we use with a different meaning. We have chosen this term because it evokes the idea that operators, as families of functions, are a “potential” that allows individual operations to be carried out. Table 2 provides a brief description of each operator and the core idea behind it. Below, a clinical example is given for each operator. These examples—each taken from a different pair—serve to give the reader a better idea of how our procedure led us to our results. They illustrate the steps that we took in our own inferential process as we developed the operators model.
By looking at the examples, a distinction seems possible between two kinds of operators: conceptual and reflective ones. Conceptual operators seem to be used by analytic therapists prevalently (albeit not exclusively) for the purpose of carrying out conceptual operations, such as filtering, linking, or transforming elements of the clinical material. Reflective operators, on the other hand, seem to be used prevalently (albeit not exclusively) for the purpose of carrying out reflective operations, such as (re)positioning, that is, discerning the risk of leaning toward an undesirable stance, and adjusting accordingly. 3 While the functions from conceptual operators are mostly applied to the clinical material, those from reflective operators are mostly applied by analytic therapists to themselves (as in the case when a supervisor strives to listen to the clinical material in a certain way) or to their interlocutor (as in the case when a supervisor invites their supervisee to adopt a certain stance with their patient).
The Dialectical Operator
T8 says that sessions with P8 (male adolescent patient) are “boring.” P8 only talks about his videogames and nothing of significance ever happens. However, during the supervision session, S8 notices some “transformations” in T8’s telling of the case, whereby the painted scene of boredom gives way to episodes that reveal, on the contrary, the presence of strong emotions playing out between T8 and P8. S8 underlines the contrasts between these two elements (boredom vs. strong emotions) and starts developing a hypothesis that he does not share with T8, but will make explicit during the interview. S8’s hypothesis is that the opposite of what T8 says might be true. That is, not only the therapy sessions might not be boring, but they might actually be exciting, because of an unrecognized erotic transference that is developing between P8 and T8. In this instance of CR, S8 is carrying out two operations, underlying which are different functions. The first operation consists in noticing the conversion of the scene of boredom into episodes of an opposite nature. The function underlying this operation may be spelled out as the mental act of noticing the conversion of an element of the clinical material (A) into its opposite (¬A). The second operation consists in taking T8’s claim that “sessions with P8 are boring” and inferring that sessions with P8 might be exciting instead. The function underling this operation may be spelled out as the act of taking a proposition (A) and considering that the opposite (¬A) might be the case. Both are examples of the kind of functions that we grouped in the Dialectical operator. Other functions in this family include posing that A and ¬A might be paradoxically true at the same time, negating both A and ¬A to affirm third option B, and so on.
The Symbolic Operator
P2 often puts on too much perfume, but she does not realize it, until people start pointing it out to her. During the supervision session, T2 suggests that P2’s perfume might represent her need to affirm herself in relationships, a need that sometimes can be overwhelming. S2 agrees. In the interview, S2 comments, “There is a considerable symbolic dimension, here: ‘I, [P2], do not realize my own desire, carried on in a dysfunctional way, to be seen. To be seen in a positive light, as perfumed.’” Later in the supervision session, T2 reports another element of the clinical material. P2 received as a gift a plant that “incredibly is still alive.” “It is an indoor plant,” explains P2, “but I put it in the sun at first, and it was dying, because it is a plant that should stay in the shade.” T2 interprets this element by suggesting that the plant might represent P2’s denial of her “desire to be warmed by the other.” S2 agrees. In these two instances of CR (the one about the perfume and the one about the plant), T2 and S2 carried out two conceptual operations that are underlaid by the same function. This function may be spelled out as the mental act of taking a concrete or external element of the clinical material (e.g., the perfume, the plant) and interpreting it as the representation of an abstract or internal one (e.g., P2’s need to be perceived, desire to be warmed). Alternatively, the function may be spelled out as the act of taking something that the patient meant literally, and interpreting it figuratively. In both cases, this is an example of the kind of functions that we grouped in the Symbolic operator. Other functions in this family include attending to the metaphors that are used by one’s interlocutor, interpreting a particular element as the representative “par excellence” of a general idea, and so on.
The Formal Operator
P5 grew up in a family characterized by a grandmother who was always intruding into P5’s mother’s life. Upon turning 18, P5 decided to leave his hometown and move to a bigger city. At some point, P5’s mother, exasperated by her own mother, decided to also leave the hometown and move in with P5. A few months later, P5 started a relationship with a girl living “next door.” S5 suggests that there might be a link between these two events, namely, the beginning of the cohabitation with the mother and the start of the relationship with the girl. S5 sees a pattern of “transitivisms” in these “relations of invasion”: just as P5’s mother sought refuge from her looming mother by moving in with P5, so P5 sought refuge from his own looming mother by starting a relationship with the girl. S5 is supported in his belief that these two events might be linked by the fact that they have something else in common, namely, their point in time. The relationship with the girl, in fact, started just a few months after P5’s mother moves in with him. In this instance of CR, S5 was able to link two seemingly unrelated elements of the clinical material by means of two conceptual operations. The function underlying the first operation may be spelled out as the act of extracting the smallest common denominator X (in this case, their being an “invasion”) from events A and B. The function underlying the second operation may be spelled out as the act of noticing that events A and B are temporally contiguous, and inferring that they might be meaningfully linked. Both are examples of the kind of functions that we grouped in the Formal operator. Other functions in this family include extracting pattern of behavior X from actions A, B, and C; extracting theme X from communications A, B, and C; attending to the recurrence of expression X in someone’s speech; and so on.
The Investigative Operator
Five minutes into the supervisory session, T3 accidentally refers to P3 (a young woman) as “he,” instead of “she.” S3 immediately notices it: “But you said ‘he’!” At this stage, S3 only points out the lapsus. But at the end of the interview she will be able to propose that: the whole supervision session served to signify that lapsus. When I say, “this ‘he’, in my opinion, says something important with respect to the position, the subjective structure of this patient,” it is because I make the hypothesis that it is a hysteric subject. And in hysteria, there is a strong side of identification with the masculine.
S3’s hypothesis was formulated in a particular theoretical context, namely, the Lacanian system of structural diagnosis. However, let us abstract from this context and focus only on the operations that were carried out. The first operation is the one by which S3 selected an element of the clinical material as revealing (i.e., T3 making a mistake in their speech). The function underlying this operation may be spelled out as the mental act of attending to an element that breaks out of the ordinary as something that might reveal a “hidden truth.” The second operation is the one by which S3 declared T3’s lapsus as the key to the whole supervision session. The function underlying this operation may be spelled out as the act of taking a minor and seemingly accidental element and interpreting it as the key to the whole case. Both are examples of the kind of functions that we grouped in the Investigative operator. Other functions in this family include attending to elements that are unusual by excess or deficiency; attending to inconsistencies in someone’s speech; taking something that a person insists is the case, and inferring that it might be otherwise; and so on.
The Genealogical Operator
P11 is an avid reader of erotic stories involving vampires. When T11 shares this element of the clinical material with her supervisor, S11 invites her to look for the “roots” of this interest. In particular, S11 suggests that these roots might be found in P11’s infantile past. “Where does this interest come from? What do those stories remind P11 of her childhood?” In the interview, S11 further explains: My hypothesis was—but I have not shared it with T11 in supervision—it’s cannibalism. It’s sucking the mother’s blood. . . . I think that, hypothetically, it may have to do with archaic erotic cannibalism. Sucking the mother’s breast, devouring her breast. That is the hypothesis that led me to try to see with T11 what the roots of this interest in vampires are.
S11’s hypothesis was formulated in a particular theoretical context, namely, one that makes implicit use of the notion of “oral-sadistic stage.” However, we can abstract from this context and focus only on the operation that was carried out. The operation consisted in taking P11’s interest in erotic stories and looking for the first version that this interest might have taken in her personal history. The function underlying this operation may be spelled out as the act of taking an element of the material and tracing it back to its earliest version. This is an example of the kind of functions that we grouped in the Genealogical operator. Other functions in this family include hypothesizing that element X developed through stages A, B, and C; interpreting a current event as the “reactivation” of a past one; hypothesizing that the beginning of a process already contained the rest of it in embryonic form; and so on.
The Dynamic Operator
T10 has trouble being sufficiently assertive with P10. According to S10, T10 is too “elegant” and not “incisive” enough with his interpretations. Later in the supervision session, T10 tells S10 that he always ends the therapy sessions with P10 by telling him, quite abruptly, “we’re done.” He feels there is something “sadistic” in his use of this formula. S10 intervenes: Because my recommendation to you, T10, is “try to use your aggressiveness more during the session.” But perhaps, such is your need not to be too incisive and to find an elegant way to interpret the patient’s aggressiveness, that this implies for you an exercise of self-control. And then the aggressiveness accumulates at the end of the session.
In this instance of CR, S10 carried out two operations. The first is the one by which he interpreted T10’s end-of-session “sadism” in a new way, i.e., as an expression of his aggressiveness. The function underlying this operation may be spelled out as the mental act of taking a behavior and hypothesizing it to be underlaid by a driving force of which the person is not aware. The second operation is the one by which S10 linked T10’s end-of-session “sadism” with his in-session “elegance.” The function underlying this operation may be spelled out as the act of taking two behaviors and hypothesizing them to be underlaid by the same driving force which, finding no outlet through behavior 1, would build up and then express itself in an intensified way through behavior 2. Both are examples of the kind of functions that we grouped in the Dynamic operator. Other functions in this family include attending to a person’s general level of animation (vs. lifelessness), attending to emotionally charged portions of speech, attending to where a person’s interest or investment lies, and so on.
The Skeptical Operator
T4 brings to supervision the case of a patient who was referred by the police for episodes of domestic violence. In the interview, S4 stops the recording at the very beginning to make a preamble: A first point that I feel is important to make clear is that for me there was always a return of the kind that—having an already extensive experience working with subjects who have problems with justice—somehow, this for me was a point where—I was saying to myself, “how shall I manage to sustain my continued ignorance and inquiry in this?”
When the interviewer asked for clarification, “You mean, even though you had an extensive experience with this class of patients?” S4 replied, “Well, precisely because of this extensive experience, how can I get rid of it, to focus on the case that is at play in that moment.” In this instance of CR, S4 carried out a reflective operation. The operation consisted in discerning a risk that his prior knowledge about forensic patients would thwart his understanding by making him too sure of himself. To counter this risk, S4 adjusted himself into an attitude of “continued ignorance and inquiry.” Abstracting from the case at hand, the function underlying this operation may be spelled out as the mental act of discerning the risk of “closing” one’s view on a case, and “reopening” it. This is an example of the kind of functions that we grouped in the Skeptical operator. Other functions in this family include discerning a tendency to formulate a hypothesis too affirmatively, and reformulating it in a more tentative way; discerning a tendency to focus only on one hypothesis, and considering alternative ones; discerning a tendency to take something for granted, and calling it into question; and so on.
The Emancipatory Operator
P7 complains about her role in the relationship with her husband (for whom she works as a secretary) and with her family of origin (for which she manages some properties). She says that she always feels like the “poor little one.” Yet T7 notes that it is P7 who accepts being put in this position by others. S7 agrees. In the interview, S7 explains The aim [of psychoanalytic therapy], what one tends towards, is always something that touches on the question of subjective responsibility. That is to say, the idea, as T7 rightly says, of trying to have the subject realize that, beyond the denunciation that she makes of the position in which the other puts her, there is something that makes P7, in any case, put herself—and remain, above all—in that position, of which she then complains . . . [and] therein lies also her personal advantage . . . what you do gain from staying there?
In this instance, T7 and S7 carried out a reflective operation. The operation consisted in discerning a tendency in P7 to put herself in the position of the poor little one whom the family would take advantage of, and promoting a position in which P7 realizes that it is her choice to accept these “shackles.” The function underlying this operation may be spelled out as the mental act of discerning a tendency to present oneself as a victim, and promoting accountability. This is an example of the kind of functions that we grouped in the Emancipatory operator. Other functions in this family include discerning a tendency to let an authority decide for oneself, and promoting autonomy; discerning a tendency to imitate others, and promoting the search for one’s “style”; discerning a tendency to “play it safe,” and promoting taking risks; and so on.
The Enkratic Operator
P6 is severely depressed and has shown no progress for months. T6 is worried and considers having P6 hospitalized. During the supervision session, S6 suggests that hospitalizing P6 risks to be a way for T6 to get rid of her own anxiety. Instead, T6 should try to “just be there” with her patient during this difficult phase. In the interview, S6 further explains: I feel that T6 risks getting caught up in her anxiety . . . and anxiety quickly leads to acting out . . . [when a patient comes to us and says] “but I’m falling! I’m in the abyss! Am I going to fall any further?” rather than having the reflex of saying, “I’ve got to get you out of there!” how on the contrary can we be in this posture, in this position, where we accompany the fall . . . how, through a work of speech, we can postpone the urgency . . . since that is our job, it is about opening up a space for speech, precisely to try not to resort to action straight away.
In this instance, S6 carried out a reflective operation. The operation consisted in discerning in T6 a tendency to rush to act in favor of P6 as a way to relieve herself of the anxiety caused by the situation. S6 advised to resist giving in to this “reflex,” and to make the difficult situation rather into an object of reflection (“work of speech”). The function underlying this operation may be spelled out as the mental act of discerning a tendency to act on the basis of an intense and distressing mental state, and trying to think/talk it through. This is an example of the kind of functions that we grouped in the Enkratic operator. Other functions in this family include discerning an urge to fill an uncomfortable silence, and trying to bear it; discerning an urge to “fix” a problem, and just trying to understand it; and so on.
The Mimetic Operator
T1 is telling about P1, but for S1 things remain “vague.” T1 says, for instance, that P1 suffers from “attacks.” “Anxiety attacks? Anger attacks?” inquires S1. “Not just ‘attacks.’” Later in the session, S1 suggests that, “to get a better feel of P1’s experience,” T1 may ask P1 to describe to her one of her typical days. In the interview, she further explains: There I wanted to draw T1’s attention—to really have her try to specify things, so that we can get a little closer to this woman. . . . It is precisely to try to approach more the—really, the day-to-day experience of this woman . . . to be as close as possible to this woman’s lived experience. Not to be satisfied with vague things.
In this instance of CR, S1 carried out two reflective operations. The first one was to notice T1’s use of words like “attacks” that left things rather “vague.” The function underlying this operation may be spelled out as the mental act of discerning a tendency to use generic descriptors, and asking for more specific ones. The second operation was to discern in T1 a tendency to paint the case in a way that did not allow S1 to build a concrete picture of P1 in her mind. S1 thus invited T1 to ask for a typical day, as a way to get immersed in her patient’s life and almost think and feel like P1. The function underlying this operation may be spelled out as the act of discerning a tendency to paint a superficial picture of a case, and asking for a more immersive one. Both are examples of the kind of functions that we grouped in the Mimetic operator. Other functions in this family include discerning a tendency to use labels and asking for what personal meanings lie behind them; discerning a tendency to apply general theories, and trying to look at the situation in its uniqueness; and so on.
The Spontaneous Operator
While T12 is talking about the case, the word deprivation comes to S12’s mind. S12 intervenes by asking T12, “Would you say that P12 is emotionally deprived? Because I was thinking of ‘deprivation,’ somewhere, but I don’t remember why.” In the interview, S12 explains: While T12 was talking earlier on, I would have some associations, some pictures in my mind, some sensations. Now I am sharing these ideas with T12 to see whether he connects with any of these, whether he takes them somewhere. It is hard to explain how do you do that, where that comes from. . . . What is your response to the material you are listening to? What are the first things that come to your mind? It is important just to empty your mind . . . that creates different associations, and you just share them.
In this instance of CR, S12 carried out both a reflective and a conceptual operation. The reflective operation consisted in putting herself in a position from which, while listening to T12, she could attend to the contents that the material would evoke. The function underlying this operation may be spelled as the act of attending to the side contents that spontaneously come to mind while one is occupied with a main task. The second operation consisted in taking one of these contents (the word “deprivation”) and trying to link it with the rest of the material. The underlying function may be spelled as the act of inferring that, if A makes one think of B, then A and B might be meaningfully linked. Both are examples of the kind of functions that we grouped in the Spontaneous operator. Other functions in this family include discerning a tendency to put a thought aside, and bringing it back into the process; discerning a tendency to think on the basis of a predefined script, and trying to think “on the spot”; and so on.
The Self-Reflective Operator
P9 has been talking about his mistrust and suspiciousness toward women. Even in the relationship with his girlfriend, he always feels “vigilant.” S9 intervenes by asking, “And with you, how does this shine through? After all, what P9 is saying regards his relationship with his girlfriend. But then he brings it to you, he tells it to you.” In the interview, S9 further explains: When a patient tells me something, at the same time I always ask myself the question: “But what is s/he telling me? In relation to what is happening between us?” I keep this question inside. We may be working on something, on a content; but at the same time, it is a question I always ask myself. I find myself thinking it in the sense that I find myself doing this overturning.
In this instance, S9 carried out a reflective operation. The operation consisted in discerning in T9 a tendency to listen to what P9 was bringing to her (about his suspiciousness and mistrust toward women) as if it had nothing to do with her. To counter this tendency, S9 invited T9 to consider instead that what P9 was discussing sub specie aeternitatis might have been brought to bear on what was happening hic et nunc, in the relationship between P9 and herself. The function underlying this operation may be spelled out as the mental act of discerning a tendency to describe a phenomenon as if it only regarded others, and trying to consider how it might regard also oneself. This is an example of the kind of functions that we grouped in the Self-Reflective operator. Other functions in this family include discerning a tendency to talk about third parties, and refocusing the discourse on oneself; discerning a tendency to “beat around the bush,” and refocusing on the “heart of the matter”; and so on.
Discussion
Our results confirm some of the ideas that emerge from the literature on psychoanalytic CR. For instance, previous authors have suggested that analytic therapists would routinely look in the clinical material for elements that tend to repeat, such as patterns of behavior or recurring themes in a patient’s communications (Arnold 2006, p. 759; Meehl 1983; Peterfreund 1975, p. 89), or that they would scan that material for “clues,” that is, seemingly accidental or unimportant elements that step out of the ordinary (Arnold 2006, p. 757; Ginzburg 1980; Peterfreund 1975, p. 84). These mental activities find their place in our model with the Formal and Investigative operators, respectively.
However, the operators model provides for the first time a unified description of the variety of mental activities carried out by analytic therapists. Besides formal or investigative reasoning, in fact, analytic therapists have been described as engaging also in that “particular way of thinking” which Jung (1906) described as “thinking in symbols” (p. 289), or in that way of thinking that Freud (1896) compared to an archeological excavation into the past. These mental activities, too, find their place in our model: with the Symbolic and the Genealogical operators, respectively. Overall, while previous authors tended to emphasis now this and now that facet of the process of psychoanalytic CR, the operators model brings its various facets together in a comprehensive account.
According to our model, in fact, there is no single defining feature to the process of psychoanalytic CR, other than the specific collection of “CR styles” that it seems to consist of. The brief examples that we offered may give the false impression that each operator is used in isolation from all others. But a fuller account would reveal how all 12 operators were interwoven within each case discussion. The central proposition of the operators model is that, although the process of CR may feel “one” to analytic therapists, passing from A to B actually consists in chaining together operations using functions from different families. And in this sense, the capacity to “think psychoanalytically” may be regarded as a higher order or emerging function, that is, as a function of functions.
In developing the operators model, we made it a rule to avoid any analytic jargon. Instead, we decided to follow Bion (1962) and describe the process of psychoanalytic CR using a mathematical (e.g., “function,” “operator”) or philosophical language (e.g., “Dialectical,” “Skeptical”). However, now that this “new” language has been formulated, it could easily be translated back into the “old” language of theory. The reader, in fact, will have realized how the operators subsume, without mentioning them, several classic analytic concepts, such as ambivalence, conflict (Dialectical); drives, sublimation (Dynamic); defensiveness, latent content (Investigative); repetition compulsion (Formal); abstinence, acting out (Enkratic); (counter)-transference (Self-Reflective); secondary gain (Emancipatory); free associations, evenly suspended attention (Spontaneous)—and many others. In this sense, the operators model invents nothing new. Just as Bion’s theory, it does not “diminish or increase existing psycho-analytic theories” (p. 89), but simply provides a formal language to describe the process of psychoanalytic CR.
However, there is an advantage to using this formal language to describe the process of psychoanalytic CR, over the content-based language of theory. To illustrate, let us return to the example from Freud (1925) about the concept of “negation.” Applying our procedure, we showed how the clinical use of that concept may be translated into the implicit use of a function, which we have spelled out as taking a negative proposition uttered by one’s interlocutor (¬A) and reverting it into its opposite (A). In light of our model, we may now classify this function as belonging to the Dialectical operator, as it revolves around the core idea of opposites. 4 But let us take now another Freudian concept, for instance, that of “reaction formation.” The clinical use of this concept, too, may be translated into the implicit use of a function belonging to the Dialectical operator, insofar as it entails the mental act of taking an element of the clinical material A (e.g., a conscious behavior) and considering its opposite ¬A (i.e., the diametrically opposed impulse that the behavior is defending the person against). 5
Now let us go beyond Freudian theory and consider a Jungian concept, such that of “enantiodromia.” The clinical use of this concept, too, may be translated into the implicit use of a function belonging to the Dialectical operator, insofar as it entails the mental act of noticing the conversion of an element (e.g., a conscious attitude) into its opposite (e.g., the unconscious compensation that arises to correct the conscious attitude). But this same function we have already encountered with S8, for instance, who used it in noticing the shift from boredom (A) to excitation (¬A). S8, who is neither a Freudian nor a Jungian, explained the CR process behind his operation invoking yet another concept, namely, that of “transformation,” as theorized by Christopher Bollas. We see then how the clinical use of different concepts (negation, reaction formation, enantiodromia, transformation) may translate, from an operational point of view, into the use of one and the same operator—a fact that would be easily overlooked if we were relying on the content-based language of theory alone.
By focusing on form rather than content, the operators model runs counter the “increasing babelization of the conceptual language” in contemporary psychoanalysis (Canestri 2006, p. 25). Not being associated to any specific school of thought, but being able to capture commonalities that exist at a more fundamental or transversal level than theory, the operators model may foster the dialogue between analytic therapists, by providing them with a sort of lingua franca. But there is also another form of “babelization of languages” that this formal language may be serve to counteract, that is, the one between treatment modalities. The reflective positioning that the Mimetic operator invites the therapist into, for instance, may come close to what person-centered therapists describe as “empathy,” although it might be better known to analytic therapists as “trial identification” (Ivey 2000, p. 33). Or the reflective positioning that the Skeptical operator invites the therapist into may come close to what family therapists describe as “not knowing,” although it might be better known to analytic therapists by many other names (Larner 2000).
Limitations of the Study
The operators model was grounded on data from a small and culturally connotated sample, which makes its generalizability unclear. It is difficult to say how the model would have been different had we had, say, fewer Lacanians and more Kohutians in our sample, or had the participants come not from Europe but from a different environment, such as America or a non-Western culture. One of the most significant factors that limited the possibility of collecting more data was the resistance that we encountered during the recruitment process. Despite wide efforts to reach out to analytic therapists, only 12 pairs agreed to participate in our study. We believe that the nature of the study, which uses empirical methods to explore everyday practice, put some therapists “on the defensive.” In this regard, we hope that the present study might facilitate the future involvement of clinicians in this kind of research, by showing how it can be consonant with their tradition and respectful of their craft. Our study sought to describe what analytic therapists already do, not to “evaluate” their practice.
As noted, we decided to include in our model only those operators that could be documented to be used in most or all of the 12 pairs that participated. This is also a limitation of this study, as it is conceivable that, depending on the composition of the sample, other operators might have appeared in the model. During data analysis, for instance, we hesitated on a couple of occasions to include further operators. To illustrate, one of these occasions regarded a family of functions that seemed to be centered on the core idea of context. Examples of functions in this family included taking an element of the clinical material (e.g., a seemingly solipsistic behavior) and “zooming out” to consider its relation to the environment (e.g., its function vis-à-vis a relational “addressee”). Adding such a “Systemic operator” would have been consistent, for instance, with Isaacs’s (1948, p. 75) idea of the importance of context in psychoanalytic thinking. However, because the use of this operator was documented to be used only in a few pairs, we decided not to include it. The aim of this study, from the beginning, was to develop a general model of psychoanalytic CR. Future research may empirically investigate these less used operators, perhaps with the hypothesis that they may account for some of the specific differences that exist between analytic schools of thought.
Finally, in this study, we put in place a number of procedures to limit the influence of our backgrounds on our results. These procedures included (a) working on clinical data obtained from an independent source, (b) avoiding the use of any analytic jargon, and (c) building consensus as a theoretically heterogeneous group (the first author being a trainee in Jungian analysis, and the other two authors being qualified analytic therapists: Lacanian and integrative, respectively). However, despite these procedures, we acknowledge that our results are bound to have been influenced by our stance toward inquiry. Our Bionian starting point already came with a series of epistemological assumptions, such as the distinction between form and content. Furthermore, the philosophical and mathematical language that we used is not theoretically “neutral,” but refers to ideas that are historically connotated. It is also unrealistic that, while analyzing the data, we were able to set entirely aside any prior knowledge about the process of psychoanalytic CR. In coming across certain operations, it was impossible not to think about well-established analytic concepts such as “projection,” “transference,” or others. Yet at the same time, refraining from using these concepts might have helped us to look at data with relatively “fresh eyes,” and possibly discover something new, instead of confirming what we already knew. We take as evidence of having at least in part succeeded in doing so the fact that, throughout data analysis, we struggled to find the words to name the functions and their families, as if attempting to lay a map on a territory that felt, to a large extent, unknown.
Implications of the Study
We envision three possible applications of the operators model.
Research
This was an exploratory study at an early phase of method development. As a result, we did not apply here rigorous procedures such as the collection of frequencies or the calculation of interrater reliability indices. However, going forward, it would be necessary to test whether the procedure that we have developed can be used by other researchers to reliably code new sets of transcripts. If shown to be reliable, this coding method might be used in psychotherapy research to address important questions, such as whether the frequency or variety of use of the operators is associated to a better therapeutic process or outcome, or what kind of factorial structure underpins the operators. This would also be an opportunity to test whether our model, which has been developed on the basis of supervision sessions, actually generalizes to therapy sessions. While there is reason to believe that the conceptual and reflective skills that are mobilized by an analytic therapist during supervision are comparable with the ones that are mobilized during therapy (Yerushalmi 2012), this assumption needs to be substantiated by further research. Furthermore, it would be important to consider whether a recall taking place immediately after the session would help obtain more reliable accounts of the CR process (Caspar 1997).
Clinical Practice
The main clinical application of Bion’s (1962) theory of functions was the development of a tool intended to help analytic therapists think through clinical problems in their everyday practice. Bion (1963) called it “the Grid.” Similarly, the main clinical application that we envision for the operators model is as a tool for the self-supervision of analytic therapists. Further research would be needed to develop such an “operators grid” and to empirically test its clinical utility. Importantly, this tool would not be intended for use during the session, lest it interfere with the spontaneous process of CR. Rather, just like Bion’s Grid, it would be intended for use after the session, especially in cases of clinical impasse where the therapist wants to deliberately think through a clinical problem from different points of view.
Training
Traditionally, the didactic component of the training to become an analytic therapist focuses on the teaching of theories and concepts. However, trainee analytic therapists may benefit from learning not only about this content-based aspect of clinical thinking, but also about its formal aspect. In this context, the operators model may play a role as a didactic tool to introduce future clinicians to what competent analytic therapists implicitly do.
Conclusions
Bion (1962) described his theory of functions as an “attempt to understand our understanding” (p. v). We see our model as a continuation of that project: to shed light on what goes on in the mind of an analytic therapist while they are working on a case. In particular, the aim of this study was to take this attempt at self-understanding one step further. To use a metaphor that was dear to Bion (1962), if thinking (or understanding) can be compared to digesting, then we wanted to explore what are some of the main classes of “digestive enzymes” that allow analytic therapists to process the raw food of the clinical material (A) into absorbable nutrients (B).
Yet at the same time, we see the operators model as a first, tentative step in a certain direction, not as a conclusive theory. Many important questions, in fact, remain unanswered at this stage. For instance, how do these enzymes (i.e., the operators) get called upon or “activated” in response to certain elements of the clinical material? Are there specific “chains” of operators that are frequently used? Is there a hierarchy among operators, such that some are more fundamental than others? These and similar questions, which are raised by our model for future research, illuminate all the work that still lies ahead of us in trying to understand a profession as complex as that of the analytic therapist.
Footnotes
Niccolò Fiorentino Polipo, clinical psychologist and PhD student, Psychological Sciences Research Institute, Université Catholique de Louvain. Jochem Willemsen, assistant professor of clinical psychology, Université Catholique de Louvain; coordinator, Louvain Psychotherapy Research Group; and psychoanalytic therapist. Delphine Kallai, clinical psychologist, teaching assistant, and PhD student, Psychological Sciences Research Institute, Université Catholique de Louvain.
The authors wish to thank all the analytic therapists who decided to participate in this study. It was an enrichening experience to cast a glance into the complexity of their daily work. Submitted November 21, 2022; revised March 7, 2023; accepted June 13, 2023.
1
2
3
The distinction between conceptual and reflective operators is only indicative and should not be taken rigidly, as some operators seem to contain both conceptual and reflective functions.
4
This operation may be seen as relying also on the Investigative operator, insofar as it consists in taking something that a person insists is the case, and inferring that it might be otherwise.
5
This operation may be seen as relying also on the Dynamic operator, insofar as it consists in hypothesizing a behavior to be underlaid by a driving force of which the person is not aware.