
Abstract
Considering the urgency of addressing grand challenges that affect human health and achieving the ambitious health targets set by the United Nations’ Sustainable Development Goals (SDGs), the role of business in improving health has become critical. Yet, our systematic review of the business–health literature reveals that business research focuses primarily on occupational health and safety, health care organizations, and health regulations. To embrace the health externalities generated by business activities, we propose that future research should investigate the conditions under which business (a) articulates and participates in health challenges, (b) engages in multilevel actions toward tackling health challenges, and (c) improves health outcomes and its impact on the health of external stakeholders, including customers and local communities. We also urge business scholars to engage with the public health research community to increase impact.
Keywords
Improving human health 1 is one of the grand challenges of our times. By grand challenges, we refer to “specific critical barrier(s) that, if removed, would help solve an important societal problem with a high likelihood of global impact through widespread implementation” (George et al., 2016, p. 1881). Health as a grand challenge is explicitly highlighted by the 2030 United Nations’ Sustainable Development Goals (SDGs), not only under SDG 3 on Good health and well-being (United Nations, 2015; Vakili & McGahan, 2016) but also in other SDGs such as SDG 2 on Zero hunger (Montiel et al., 2021). Current indicators of global health are worrisome. For instance, the United Nations reveals that more than 400 million people are still without primary health care globally (United Nations Development Programme, 2020). Also, nearly 690 million people suffer from hunger and more than 631 million people in Asia and Africa remain undernourished (United Nations, 2020), resulting in adverse consequences for health (Black et al., 2008; Olson, 1999; Swinburn et al., 2019). The most recent Lancet reports point to climate change as a critical factor leading to the health crisis (Watts et al., 2018, 2019, 2021) There has been a 54% increase in heat-related mortality among the 65 and older population since 2000, which resulted in 296,000 deaths worldwide in 2018 (Watts et al., 2021). We also cannot ignore the tremendous hit on global health that the COVID-19 pandemic has taken a toll on humans by the time we engaged in this review piece. In fact, COVID-19 is one of the main reasons that prompted us to study the connections between business and human health.
The health grand challenge needs to be addressed not only by governments and civil society organizations but also by businesses (Sachs et al., 2019). Business can play a critical role in society by considering the impact of its activities on the health of stakeholders either directly or indirectly (Leisinger, 2005, 2009; Pfeffer, 2010; Schrempf, 2014; Tempels et al., 2020; Zwetsloot & Pot, 2004), given that the impact of business on people’s health has become too substantial to ignore (McKee & Stuckler, 2018; Mialon et al., 2020; Millar, 2013). Cognizant that business can affect or be affected by health, business researchers have paid some attention to the bidirectional associations between business and health. From studies devoted to occupational health (Christian et al., 2009; Danna & Griffin, 1999; Ganster & Rosen, 2013; Grandey et al., 2020; Macik-Frey et al., 2007), to those dealing with health care administration (Atasoy et al., 2018; Blair & Boal, 1991; Brown et al., 2015; Fottler, 1987; Luke et al., 1989; Oddo, 2001; Paul et al., 2019; Russo, 2016; Vogus et al., 2010) and public health policy (Arnold & Reeves, 2006; Chaar & Lee, 2012; Jacobson, 1994; Nill et al., 2019; Oborn et al., 2013; Peterson, 1996; Tebbens & Thompson, 2009), the literature has mainly centered on the impact of business on the health of employees as an internal stakeholder, as well as on organizing dynamics in health care organizations (Blair & Boal, 1991; Brown et al., 2015; Fottler, 1987; Mayo et al., 2021) and the interaction between business and public health policy (Chaar & Lee, 2012; Flasher & Lamboy-Ruiz, 2019; Hegde & Sampat, 2015; Hemphill, 2019; Kramer & Greek, 2018).
However, the impact of business on the health of external stakeholders, such as consumers and surrounding communities, 2 has received much less scholarly attention. 3 This might be partially explained by the fact that firms are legally liable for the occupational health of their employees (i.e., private health costs) while there is rarely any legal liability for the health of external stakeholders (i.e., social health costs; Schrempf, 2014; Tempels et al., 2020), except in some particular cases such as product safety for consumers (Danley, 2005; Noggle & Palmer, 2005; Thirumalai & Sinha, 2011) or where pollution makes neighboring communities sick (Clifford, 1996; Simola, 2010). Despite the importance of understanding the relationship between business activities and external stakeholder health, to the best of our knowledge, no business academic literature review has yet looked at their intersection.
In an effort to answer why and how business addresses health as a grand challenge, we take stock of current research on business and health by applying the higher-order framework for addressing grand challenges developed by George and his colleagues (2016) to health. First, in our analysis, we focus on reviewing the literature on the impact of business on external stakeholder health to identify theories, themes, and research questions. Second, through mapping the surveyed articles within the higher-order framework, we identify future research avenues that embrace social health costs and the role of business in promoting health and well-being for external stakeholders in light of (a) the firm’s articulation of and participation in health challenges, (b) the movement from articulation into action, and (c) the transformation of action into health outcomes and impact. Third, we draw insights from three public health literature streams—social determinants of health, commercial determinants of health, and emerging infectious diseases—that will be useful in developing theoretical relationships connecting business to health. Fourth, we provide recommendations for an interdisciplinary approach to business scholars interested in health and the advancement of the 2030 Agenda and the SDGs on health and well-being for the next decade and beyond.
The rest of the article is structured as follows. In the first section, we delineate how business and health are closely connected. Using an extensive keyword search, we then identify articles at the intersection of business and health and further analyze them through descriptive, co-citation, and flexible pattern matching analyses. Building on the results of the analyses, we report the extent to which the current business–health literature matches with George and colleagues’ (2016) higher-order grand challenges framework. Finally, we outline research opportunities and interdisciplinary insights in the business–health literature along with some recommendations for an interdisciplinary approach to the literature.
The Interdependencies of Business and Health
The connections between business and human health have always existed. On one hand, health—or the lack thereof—has been at the center of many controversies, as many public health professionals argue that some firms contribute to making people sick through their products or services and engagement in the public health policymaking process; they also may profit from illness and those who are trying to stay healthy (Freudenberg, 2014; Moodie et al., 2013; Moynihan et al., 2002). For example, the pharmaceutical industry has been accused of consistently implementing high pricing strategies for the drugs that could have kept HIV/AIDS infection under control, keeping them beyond the reach of people who could not afford them (Flanagan & Whiteman, 2007; Leisinger, 2009). The food industry is often criticized for promoting high-fat and sugary products to consumers at risk of diet-related diseases (Beaver, 1999; Germano & Montiel, 2011; Schrempf, 2014; Tempels et al., 2020). The tobacco and alcohol industries have been considered as primary causes of the increasing burden of chronic diseases worldwide (Delpo, 1999; Stuckler et al., 2012). Moreover, public health scholars point to business engagement in the health-related policy formulation and implementation process as shaping public policy agendas in ways that potentially undermine health (Clapp & Scrinis, 2017; Freudenberg, 2014; Moodie et al., 2013).
On the other hand, business has the potential to reverse harmful impacts on the health of all its stakeholders, not only internally (i.e., employees), but also externally (e.g., consumers and neighboring communities; Lumpkin & Bacq, 2019; Pfeffer, 2010; Zwetsloot & Pot, 2004). For instance, corporate innovation capabilities place firms in a unique position to advance research and development in medicines, vaccines, and diagnostics (Le et al., 2020; Witty, 2011), contributing positively to health by enhancing access to medicine and health care products for all. The food industry can provide foods and beverages reinforced with micronutrients that are unavailable or lacking in local diets to respond to widespread malnutrition in developing countries (Bekefi, 2006; Yach et al., 2010). Thus, we argue that the health of external stakeholders—including consumers and communities—should be at the heart of a future research agenda for business scholars, and in particular, for business and society researchers, given that business, as a societal actor, may influence health challenges even if there is no single causal link between business activities and such health challenges (Schrempf, 2014; Tempels et al., 2020).
Review Method
We organize this section based on prior work by Tranfield and colleagues (2003) and proceed with the review of the existing business–health literature in three steps: (a) planning, (b) data collection, and (c) data analysis. In the planning stage, we determined the primary research focus and search strategies, including target journals and search keywords. In the data collection stage, we assessed the identified studies to extract data based on our specific inclusion and exclusion criteria. In the data analysis stage, we analyzed the data utilizing co-citation and flexible pattern matching analyses to synthesize and report the main findings.
Planning
We first defined our research goals, the list of journals, and the search time frame, and we identified keywords and a search database. Based on previous literature reviews on corporate social responsibility (CSR) and sustainability (Montiel, 2008; Montiel & Delgado-Ceballos, 2014), we searched 14 top academic management journals with tradition and traction, six leading business and society journals, and four practitioner management journals (see Table 1 for a detailed list of journals used for a keyword search). In terms of the time frame, we chose the period from 1986 to September 2020. In 1986, the World Health Organization published the Ottawa Charter for Health Promotion, which is considered a seminal document and template for health promotion geared toward improving health and reducing health inequalities (Thompson et al., 2018). This health manifesto emphasized that all societal actors, including business, are responsible for improving health, which should spur scholars’ interest in the role of business in addressing health.
Article Count by the Discipline Focus of Journals.
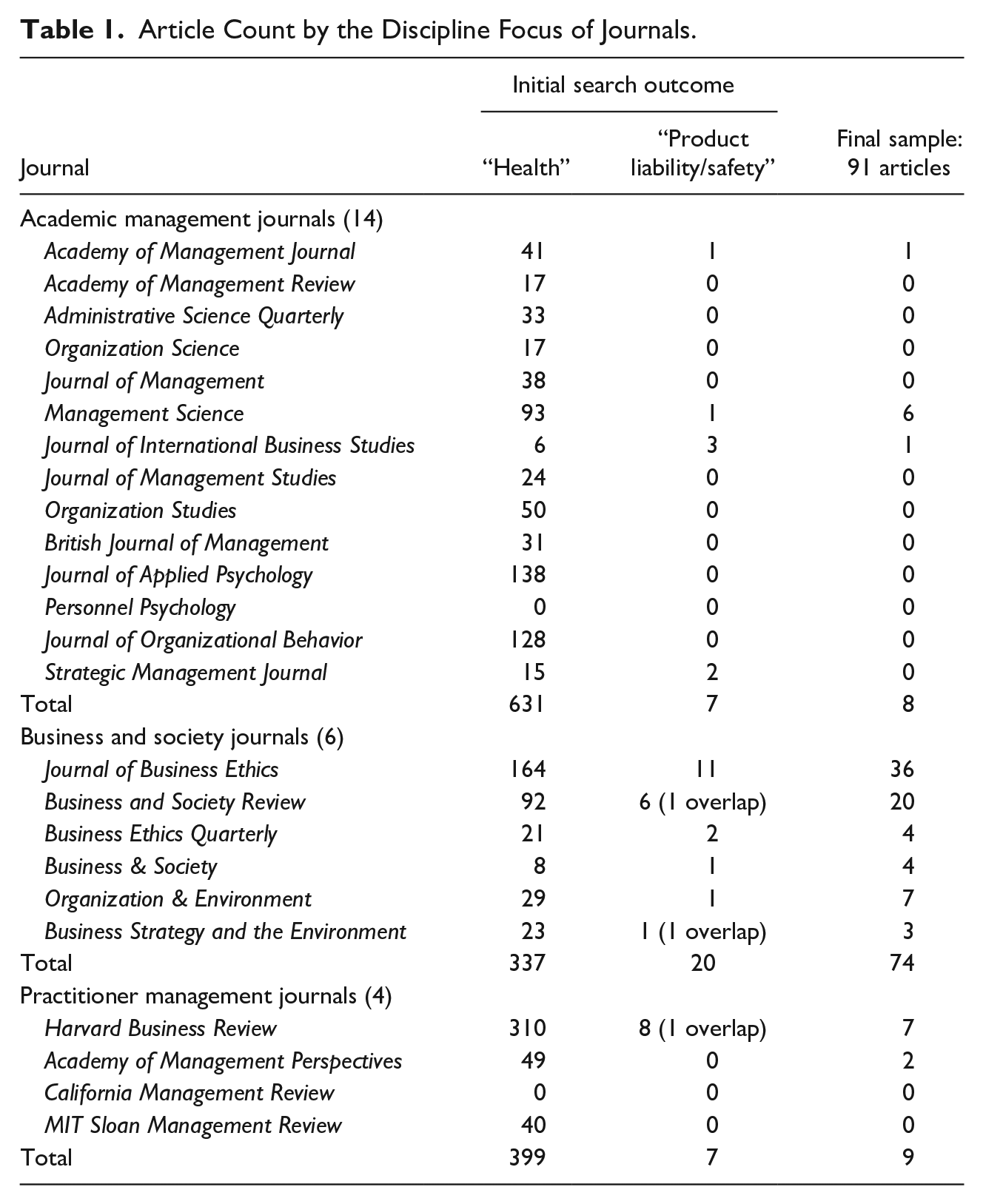
Once the list of journals and the time frame were determined, we proceeded with defining the keywords to be searched in the titles, abstracts, or keywords provided by the authors. We used the following keywords to cover a broad range of health challenges in the business literature: “health” OR “product liability” OR “product safety” OR “consumer safety.” We decided to include the product liability/safety-related keywords because some previous studies that examine the connection of business to consumer health from a product safety angle do not use the term health but adopt such keywords in titles, abstracts, or keywords provided by authors (Bapuji & Beamish, 2019; Schrempf, 2014). We used EBSCOhost’s Business Source Complete as it has been recently found to be the most suitable academic search system for a literature review due to its functionality for using Boolean operators, a large number of available records and search hits, and extended search strings (Gusenbauer & Haddaway, 2020). The database also covers the 24 journals used in the keyword search. These search criteria led to a total of 1,401 articles.
Data Collection
In this stage, we manually read the titles and abstracts of the 1,401 articles identified to retain only those directly related to our research objective: taking stock of knowledge on the impact of business on the health of external stakeholders to identify theories, themes, and research questions and to propose an avenue for future research for business scholars interested in health. Specifically, two of the authors manually read the title and abstract of each of the 1,401 pieces to determine whether to retain them in the final sample. Of the 1,401 articles, 34 were retrieved via the terms product liability, product safety, or consumer safety and the two authors only included articles that contained a clear health implication for the external stakeholders of business. The two authors performed seven rounds of article reading and classification, around 100 articles for each round, followed by discussion among the authors to ensure that we were consistent in the application of the health of external stakeholders only. Then, the other two authors, who did not participate in the initial rounds of screening, adjudicated the inclusion or exclusion of the 245 doubtful articles in cases where an article has implications for the health of external stakeholders, but does not directly discuss the impact of business on such health challenges.
Figure 1 shows business–health themes of the 1,401 pieces initially identified. Of the total sample, 31% (438) were related to occupational health and 29% (403) to health care administration4,5 and/or public health policy, which we eliminated from our analysis. Our screening also revealed that 18% (259) did not apply to our review purpose because they address health issues without considering the impact of business on health or use health in different contexts, such as financial, economic, or organizational health. In addition, 15% (210) were not research articles but other types of documents (calls for papers, book reviews, editorial pieces, etc.). The application of the inclusion/exclusion criteria led us to reduce our sample to 91 relevant articles 6 that discuss the connection between business and the health of external stakeholders, including consumers and communities.

The conceptions of health in business research.
Data Analysis
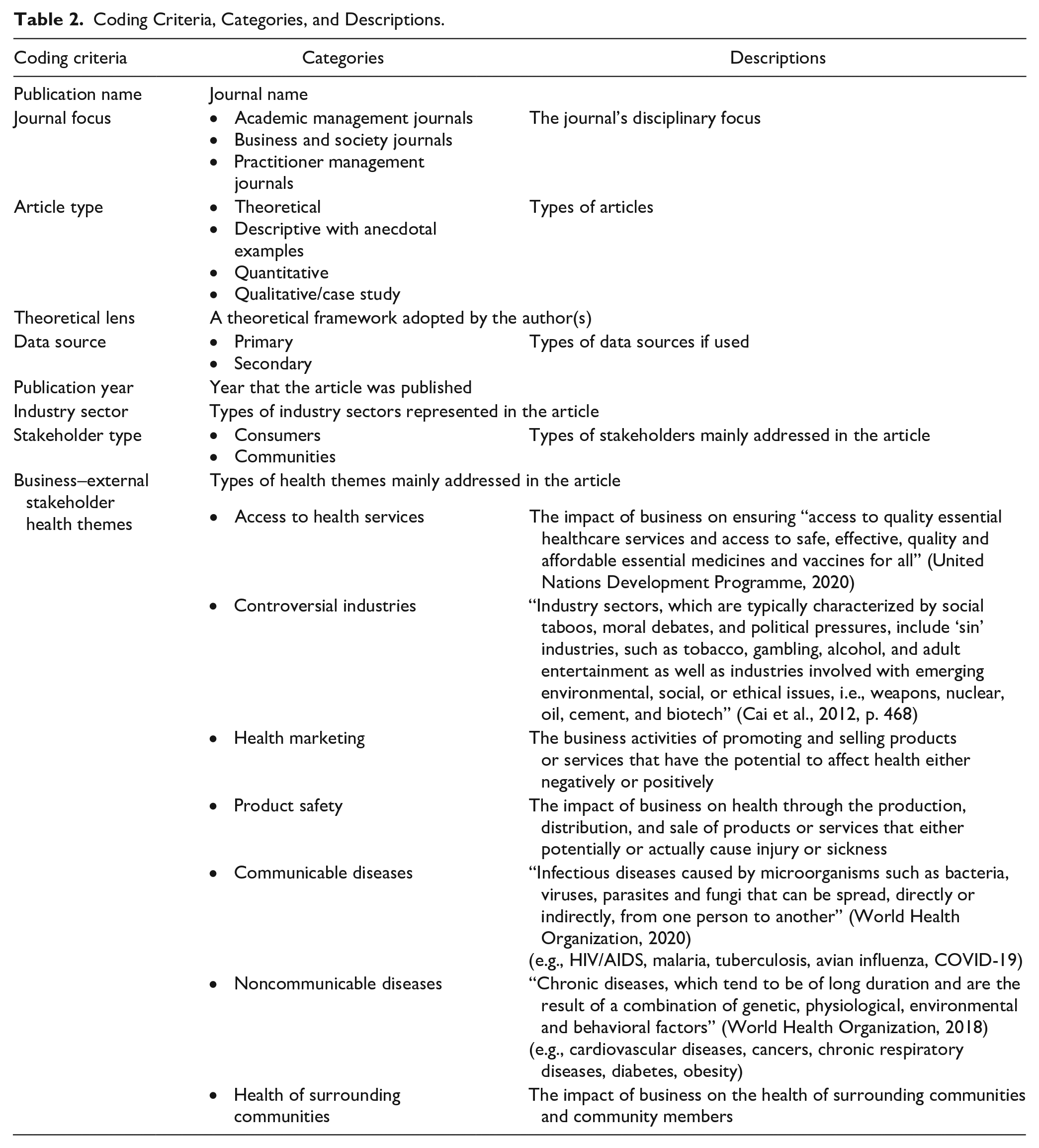
In this stage, we conducted co-citation and flexible pattern matching analyses to understand the characteristics of final sample articles and lay the foundation for a framework that may advance the business–health literature. First, we performed qualitative coding to content analyze the final sample of 91 articles. Two of the authors read each of the 91 articles and coded them in two ways. We began by coding the basic information of each article, such as the journal name and year of publication. Drawing on a widely accepted categorization adopted by other literature reviews (Dembek et al., 2020; Pisani et al., 2017), we also coded article type (theoretical, descriptive with anecdotal examples, quantitative/empirical, qualitative/case study), theory, data sources (primary, secondary), and industry sectors. In addition, to capture prior research on the relationship between business and external stakeholder health, we identified types of external stakeholders (consumers, communities) and the following seven business–health themes: (a) access to health services, (b) controversial industries, (c) health marketing, (d) product safety, (e) communicable diseases, (f) noncommunicable diseases, and (g) the health of surrounding communities. We drew on an inductive coding procedure adopted by Dembek and colleagues (2020), which generates themes for codification from the reviewed articles. The seven business–health themes emerged from their repeated appearance in the initial screening of the original 1,401 studies. Table 2 summarizes the coding criteria and categories coded along with a brief description of each one. Once we completed several rounds of codification and analysis for the articles, we calculated the Cohen’s kappa statistic (Cohen, 1960) between the final classification of each pair of two authors to analyze the interrater reliability. The Cohen’s kappa statistic of 0.87 revealed a high degree of agreement between the authors’ codifications. Values higher than 0.6 are considered as substantial agreement, whereas values higher than 0.8 are regarded as almost perfect agreement (Landis & Koch, 1977).
Coding Criteria, Categories, and Descriptions.
For co-citation analysis, we used VOSviewer—a bibliometric network software—to identify co-occurrences of two papers in the third paper’s citations to detect seminal studies in the realm of business–health research. Co-citation is defined “as the frequency with which two documents are cited together” (Small, 1973, p. 265), which helps identify the most cited documents that can be considered to have intellectual solid influence in a particular research domain (Culnan, 1986). Culnan (1986) highlights that “as the field matures, new theories are proposed and compete until paradigms emerge” (p. 156). Studies that are topically related to each other and repeatedly cited together in subsequent publications tend to belong to the same cluster as a result of co-citation analysis of cited references. We determined the more influential documents in the business–health space via co-citation analysis, given that researchers frequently cite documents that they consider crucial for their studies (Ramos-Rodríguez & Ruíz-Navarro, 2004). We carried out the reference co-citation analysis with the 68 articles available in Thomson Reuters’s Web of Science. The bibliographic information for 23 articles was not available on Web of Science. The omission of these articles does not threaten our co-citation analysis’s validity because 19 omitted articles were published without any cited references in either Harvard Business Review or Business and Society Review. We set the minimum number of citations of cited references as three.
In addition, we performed a flexible pattern matching analysis to determine the extent to which George and colleagues’ (2016) higher-order framework 7 for addressing grand challenges can organize the current literature and point to new avenues of research. Flexible pattern matching entails an iterative matching between theoretical patterns derived from the literature and empirical observations from the data (Bouncken et al., 2021). We drew on George and colleagues’ framework as a platform to encourage scholars to consider business–health challenges as a grand challenge, extend existing management theories and empirical questions, and guide future research in this realm. We delineate the details of the framework as we report the results of this review in a later section.
Based on the co-citation and flexible pattern matching analyses, we report our main findings in the next section.
Results
Descriptive Statistics
We begin by reporting the descriptive statistics of the 91 articles examined based on the qualitative coding and then delineating examples of studies by the two external stakeholder types (consumers and communities) and the seven business–health themes.
In this section, we examine the type of journals, type of article, theoretical frameworks used, type of data, and industry setting of the data. First, in terms of the disciplinary focus of journals, Table 1 illustrates that 81% of the reviewed articles were published in business and society journals, and 10% and 9% were published in practitioner management journals and academic management journals, respectively. It is worth noting that we identified six empirical articles published in Management Science while not seeing similar types of studies published in the other academic management journals. Research themes of these six articles include product recalls in the medical device industry (Thirumalai & Sinha, 2011); business incentives for voluntary product safety certifications (Iyer & Singh, 2018); the impact of copay coupons on patients, insurance companies, and drug manufacturers (King et al., 2019); adulteration in farming supply chains (Levi et al., 2020); the relationship of food safety inspector schedules to inspection quality (Ibanez & Toffel, 2020); and the influence of firm lobbying on the timing of safety alert announcements leading to drug-related side effects (Diestre et al., 2020). Management Science may be more likely to embrace these types of articles than other management outlets, given that the journal has historically encouraged multidisciplinary research at the intersection of public health and management and functional areas of business in light of “measuring and improving population health” (Management Science, 2021).
Second, regarding article type, 39% of the reviewed articles are predominately descriptive with anecdotal examples, followed by quantitative (22%), theoretical (20%), and qualitative/case studies (19%). Third, in terms of theory, our analysis reveals that there is no coherent theoretical framework used across the business–health literature, but some articles in the sample build on theoretical grounds widely used in management or development studies, including the dependency theory of development (Jorgenson, 2009; Shandra et al., 2011), social network theory (Schrempf, 2014), and stakeholder theory (Lumpkin & Bacq, 2019). Fourth, regarding data sources, 12% and 25% of the reviewed articles used primary and secondary data, respectively. Among the reviewed articles, interview and survey methods stand out as the most frequent sources for primary data, and company annual reports and trade publications were the most common secondary data sources. Finally, for the type of industry, studies focus on the pharmaceutical (16%), food and beverage (11%), tobacco (10%), agriculture (5%), health care products and services (4%), consumer goods (4%), biotechnology (4%), tourism (3%), alcohol (2%), and toy (2%) industries, all of which have implications for the health of external stakeholders, especially consumers.
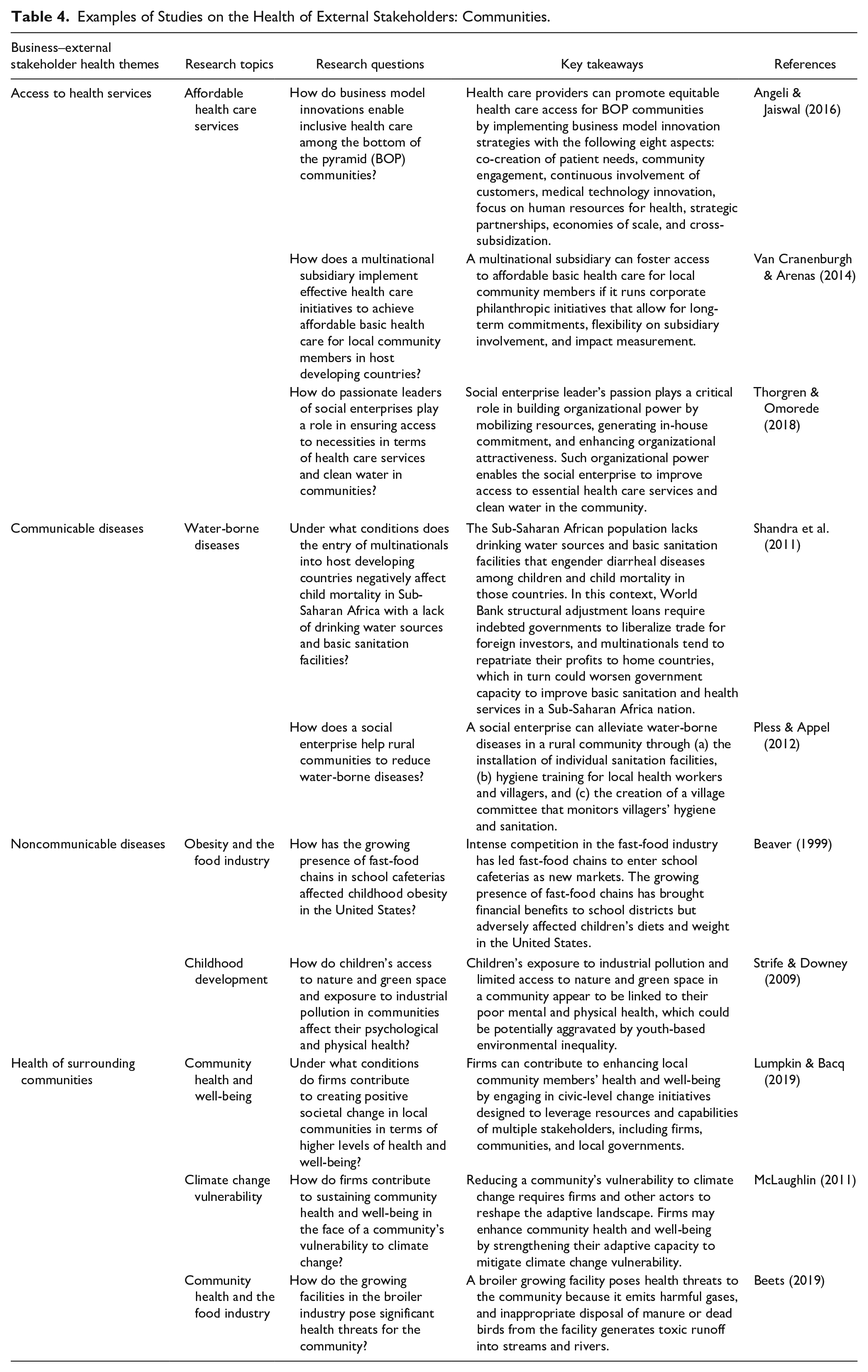
To further our understanding of the extent to which business research attends to external stakeholder types and business–health themes, we assessed which of the two types of external stakeholders and the seven business–health themes are the main focus of each article. Our results show that 57% of the reviewed articles address consumers’ health, 28% deal with communities, and 15% discuss the health of consumers and communities at the same time. For the business–health themes, product safety, health marketing, and controversial industries remained highly dominant from 1986 to 2020. This may be attributed to the fact that these three health themes are associated with the direct impact of business on consumer health. Our analysis illustrates that business scholars seem to have started to shift their attention to the health of surrounding communities and communicable and noncommunicable diseases from 1990 to 2020. Tables 3 and 4 describe typical studies at the intersection of business and the health of consumers and communities, respectively.
Examples of Studies on the Health of External Stakeholders: Consumers.
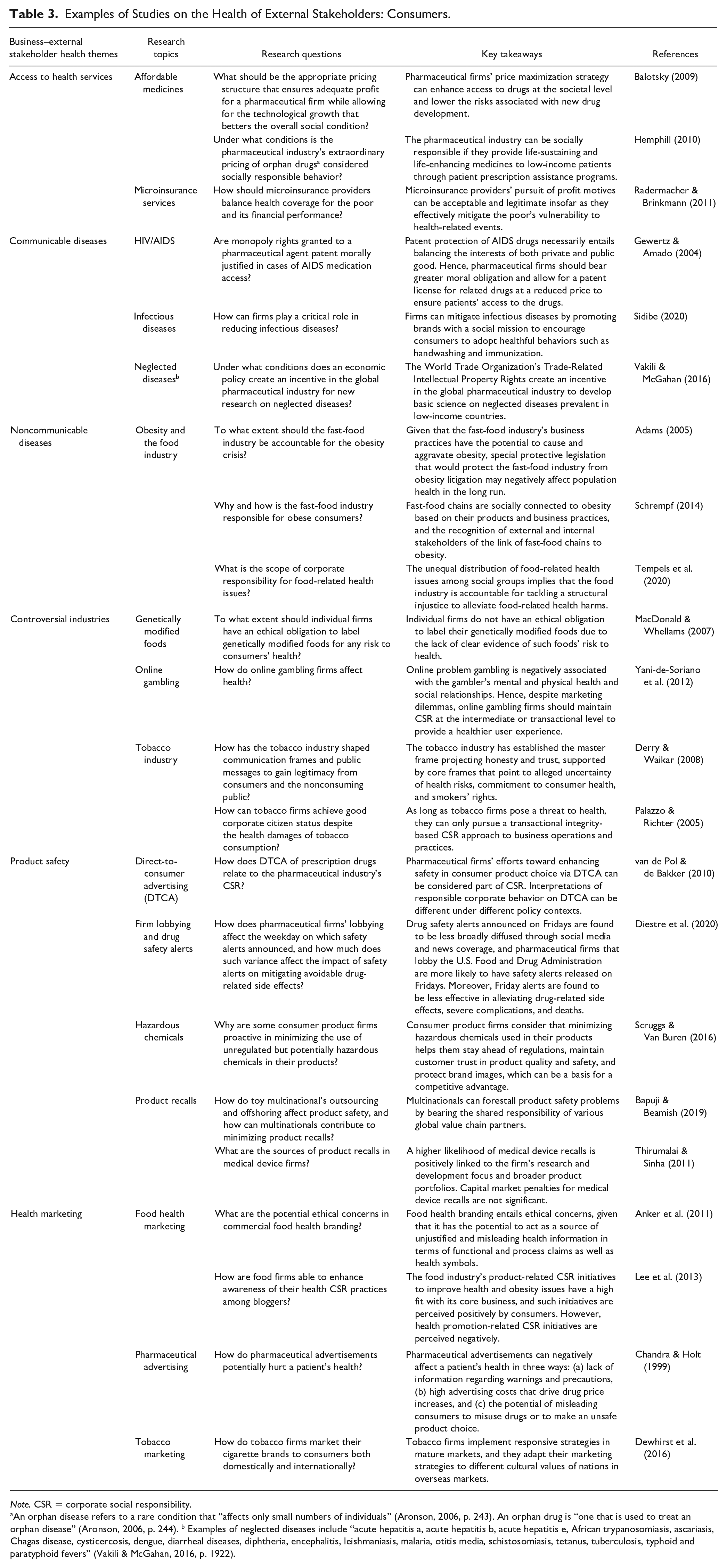
Note. CSR = corporate social responsibility.
An orphan disease refers to a rare condition that “affects only small numbers of individuals” (Aronson, 2006, p. 243). An orphan drug is “one that is used to treat an orphan disease” (Aronson, 2006, p. 244). b Examples of neglected diseases include “acute hepatitis a, acute hepatitis b, acute hepatitis e, African trypanosomiasis, ascariasis, Chagas disease, cysticercosis, dengue, diarrheal diseases, diphtheria, encephalitis, leishmaniasis, malaria, otitis media, schistosomiasis, tetanus, tuberculosis, typhoid and paratyphoid fevers” (Vakili & McGahan, 2016, p. 1922).
Examples of Studies on the Health of External Stakeholders: Communities.
Co-Citation Analysis
We conducted a co-citation analysis to identify the most co-cited references among the 68 articles in the final sample with bibliographic information available on the Web of Science. The top three most co-cited references among the 68 articles are Carroll (1991, 1999) and Mitchell and colleagues (1997), but the number of co-citations for the three articles does not exceed five. The low number of co-citations for even the most co-cited references confirms that the business–health literature is highly fragmented, so that there are no coherent conceptual frameworks and theories applied consistently across studies. It is also worth noting that of the most co-cited articles, only one article was published in a nonbusiness journal, American Journal of Public Health (Glantz, 1996), indicating that business scholars have yet to take an interdisciplinary approach to an inherently interdisciplinary subject.
Specifically, our analysis yields two clusters that group according to their intellectual underpinnings. The first cluster consists of Carroll (1991) and Carroll (1999), and both studies address the types and features of CSR. The key studies in the second cluster are DiMaggio and Powell (1983), Mitchell and colleagues (1997), Palazzo and Richter (2005), and Suchman (1995), all of which deal with organizational legitimacy under either institutional theory or stakeholder theory. These two clusters demonstrate that the intellectual underpinning for research regarding the impact of business on the health of external stakeholders lies in CSR in the first cluster, and institutional and stakeholder theories in the second cluster.
Flexible Pattern Matching
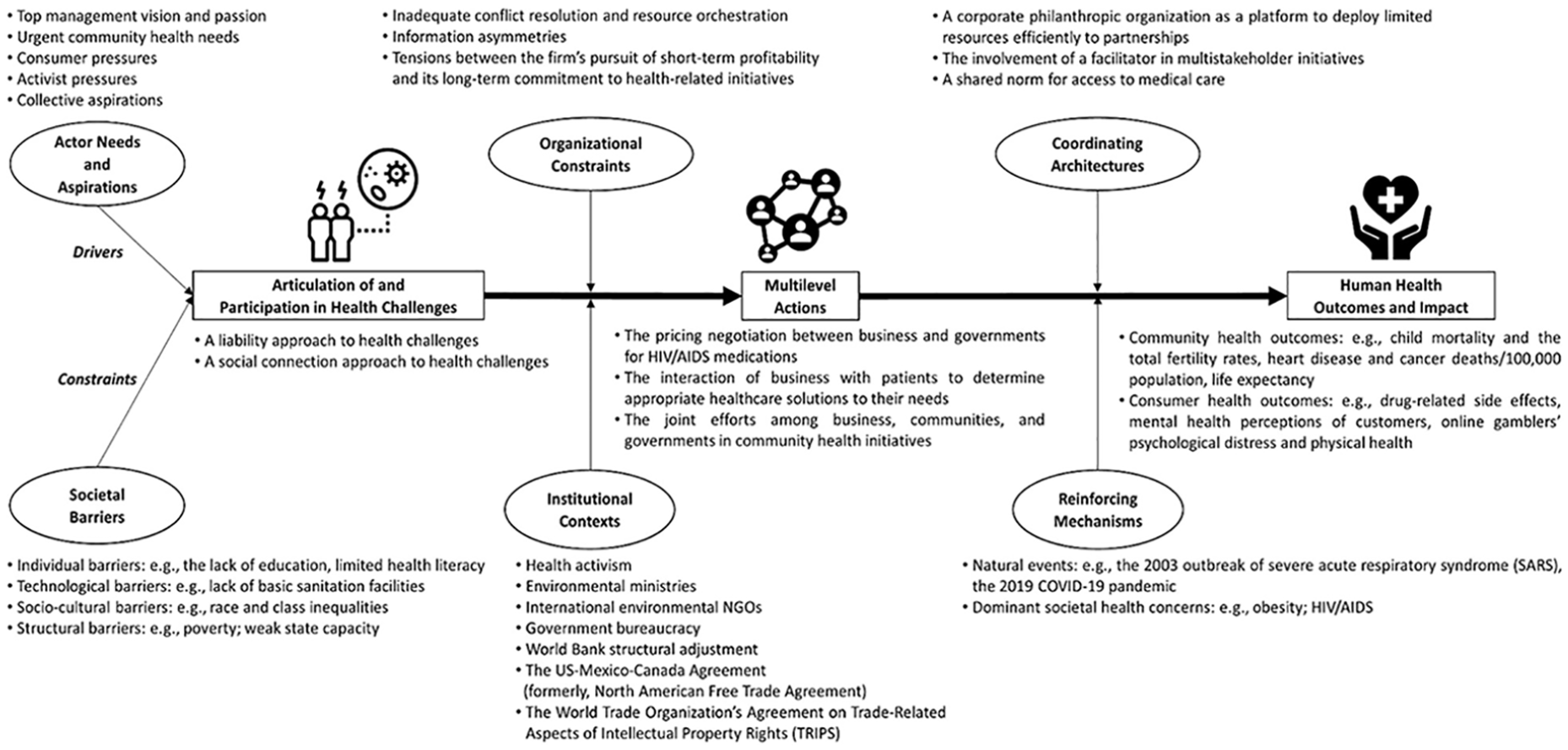
Our next step was to dig deeper into the content of the articles included in this study to organize the literature on business and health of external stakeholders and the conceptualization of health as a grand challenge. Utilizing the method of flexible pattern matching, we report the extent to which the current literature at the intersection of business and health fits George and colleagues’ (2016) higher-order grand challenges framework, consisting of three core and six ancillary components (see Figure 2). A key proposition of George and colleagues’ model is that addressing grand challenges requires multilevel actions. Their framework consists of three core components: (a) articulating and participating in grand challenges, (b) multilevel actions toward grand challenges, and (c) consequences of multilevel actions. Health challenges faced by business’s external stakeholders are complex because oftentimes no clear root causes are recognized and they include interwoven sociocultural and technological elements. Hence, the health of external business stakeholders represents a grand challenge, which requires collective action to help solve them moving forward.
Mapping the Business–Health Literature.
Based on our findings from the analysis of 91 articles in the final sample, we use the framework to layout potential variables of interest to business scholars. Because most of the reviewed studies do not deal with grand challenges, we identify variables potentially well suited to a framework for addressing health challenges from the business perspective. Hence, our analysis and modified framework are designed to determine what we know and do not know about the role of business in addressing health challenges within the disjointed business–health literature. Precisely, we assess the causes and outcomes of multilevel actions on health challenges along with the moderators at play. Then, we offer new research lines by building bridges between business research and health challenges faced by external business stakeholders.
Articulation of and participation in health challenges
Our review of the business literature shows that current business practices have yet to identify external stakeholder health as a grand challenge. A set of reviewed articles suggests that firms become interested in coping with health if their investments in developing a new lineup of healthier products and services help them increase sales and enhance corporate image and customer loyalty (Han et al., 2020; Han & Hyun, 2019; Zwetsloot & Pot, 2004). Also, firms tend to identify and address external stakeholder health only if there is clear evidence that the firm’s action is a direct cause of health-related harm based on a legalistic approach (Schrempf, 2014; Tempels et al., 2020). For example, Bapuji and Beamish (2019) illustrate how toy multinationals shirk responsibility by finding scapegoats rather than admit their inadequacies and improve product safety and thus consumer health. Similarly, some reviewed articles deal with business’s legal and moral responsibility underpinning product liability issues. For instance, Noggle and Palmer (2005) delineate how Ford tried to divert stakeholders’ attention from the safety problems with its vehicle by questioning the safety issue of tires manufactured by Firestone—Ford’s tire supplier—thereby avoiding taking responsibility for accidents and deaths caused by tire blowouts leading to its vehicle rollovers. In the medical device industry context, Thirumalai and Sinha (2011) confirm that a firm’s prior recall experience is negatively associated with the likelihood of future recalls.
It appears that a new research stream is emerging, such that a handful of studies at the business–health crossroads have focused on altering the dominant theoretical paradigms of responsibility that business adopts. For instance, Schrempf (2014) points to the need to shift business attention in relation to the food industry and obesity issues from a liability paradigm to a focus on responsibility based on social connection. Given that a legal approach to external stakeholder health challenges assumes corporate responsibility can only flow from clear causal relationships, this view of responsibility fails to address systemic harms to which many firms contribute, but from which none can draw a unique linear or perceptible causal relationship (Schrempf, 2014; Tempels et al., 2020). Hence, these scholars indicate that business should instead adopt a broader model of health responsibility that considers all relevant stakeholders. Using this broader approach to responsibility, some scholars discuss the extent to which pharmaceutical firms are responsible for ensuring access to adequate medicines for the poor, even if the firms are not directly accountable for their health (Leisinger, 2005, 2009).
Next, we examine two groups of factors that drive or curb the firm’s articulation of and participation in the resolution of health challenges: (a) actor needs and aspirations and (b) societal barriers.
By unifying actor needs and aspirations, collaborative efforts may help trigger articulation of and participation in health challenges. Our review reveals that the current business literature primarily focuses on how internal and external stakeholders motivate business firms to be concerned with health. Regarding internal stakeholders, the organizational leaders’ vision can help firms attend to health challenges (Johnson, 2015; Sethi et al., 2011). For example, Sethi and colleagues (2011) show that the vision and decisive nature of the CEO at Freeport-McMoRan Inc., an American mining multinational, push the firm to make its strong commitments to the expansion of public health programs available to the local Papuan communities where the firm operates. For external stakeholders, urgent health needs among community members can stimulate business to participate in tackling health challenges. Boehm (2009) finds that business gives a high priority to making financial contributions toward improving community health conditions—such as hospitals, clinics, and health care services—during wartime. Other examples of external stakeholders include consumer pressures (Rosenberg, 1987; Scruggs & Van Buren, 2016) and activist pressures (Derry & Waikar, 2008; MacDonald & Whellams, 2007). Regarding consumer pressures, Scruggs and Van Buren (2016) argue that firms are motivated to become proactive in minimizing the use of unregulated but potentially hazardous chemicals in their products to gain competitive advantage and legitimacy through preempting pressures from their external stakeholders, including consumers, government agencies, and the media. In a similar vein, Derry and Waikar (2008) examine how the tobacco industry has sought to gain legitimacy from consumers and the nonconsuming public in the presence of strong public health activism.
Based on our review, we find that actor needs can be articulated under three conditions. First, health challenges can be identified via a collective aspiration for positive societal change among key stakeholders, including business, communities, and governments (Lumpkin & Bacq, 2019; Pless & Appel, 2012). For example, Lumpkin and Bacq (2019) suggest that societal change initiatives for community health challenges—such as lack of access to health care and water-borne diseases—likely take place if business, communities, and governments shape a collective aspiration aimed at creating positive societal change. Second, health challenges can be addressed if there is a co-creation process through which health needs are identified by business and patients or community members together (Angeli & Jaiswal, 2016; Pless & Appel, 2012; Van Cranenburgh & Arenas, 2014). For instance, Pless and Appel (2012) delineate how a social enterprise set up participatory decision-making processes ensuring the equal representation and participation of the entire community to identify its pressing needs such as improved community health, water sanitation, and childhood education. In a similar fashion, Van Cranenburgh and Arenas (2014) illustrate how a community’s specific health needs shape a multinational’s philanthropic activities and strategies in developing countries. Third, health challenges can be articulated through the engagement of business leaders in social movement processes that raise community members’ awareness of community health challenges and the firm’s health initiatives (Thorgren & Omorede, 2018). Thorgren and Omorede (2018) describe how the leaders of social enterprises lay the foundation to make a positive impact enhancing community health conditions by informing community members of urgent health issues through personal communication with individuals and the larger community, public relations, or the media.
Societal barriers can prevent actors from tackling health challenges because they are seen as being beyond the scope of the interventions of individual actors. Four groups of societal barriers are particularly relevant to the context of business–health: individual, technological, sociocultural, and structural barriers (George et al., 2016). Our review of the literature helps identify (a) individual barriers, such as a lack of education (Tansey & Hyman, 1995) and limited health literacy (Angeli & Jaiswal, 2016); (b) technological barriers, such as access to clean water and basic sanitation (Pless & Appel, 2012; Shandra et al., 2011) and access to health services (Angeli & Jaiswal, 2016; Radermacher & Brinkmann, 2011; Thorgren & Omorede, 2018; Van Cranenburgh & Arenas, 2014); (c) sociocultural barriers, including class- and race-based inequalities (Gautier & Bricher, 1991; Strife & Downey, 2009; Tempels et al., 2020); and (d) structural barriers, including poverty (Beets, 2019; French, 2010) and weak state capacity (Jorgenson, 2009; Leisinger, 2009; Shandra et al., 2011; Van Cranenburgh & Arenas, 2014). It is worth noting that several studies treat poverty as a manifest structural barrier that hampers the access of the poor to essential health care services or medications (Angeli & Jaiswal, 2016; Gewertz & Amado, 2004; Leisinger, 2005, 2009; Radermacher & Brinkmann, 2011; Thorgren & Omorede, 2018; Vakili & McGahan, 2016; Werhane & Gorman, 2005).
In sum, the literature does provide an important foundation to understand why and when firms will identify and participate in solving a specific health challenge. The needs of actors, catalyzed by collective aspirations, co-creation processes, and business engagement in social movements, and societal barriers (individual, technological, sociocultural, and structural barriers) are factors that will either foster or inhibit the decision of a firm to articulate and participate in a given challenge. The outlines of potential research essentially exist, but clearly the studies examining how and why firms engage with specific issues are lacking. Having decided to engage with health challenges, the firm needs to define specific actions to address them.
Multilevel actions
Turning from the factors that influence the firm’s articulation of and participation in grand challenges, we move to the effects of this articulation and participation—multilevel actions, which are the interventions that an organization can make to address health challenges. Understanding the relationship between business and other societal actors at multiple levels is crucial to predict subsequent health outcomes, as well as to achieve health-related goals. The current business literature focuses on the health impacts of firm-level actions, including, but not limited to, marketing practices (Chandra & Holt, 1999; Dewhirst et al., 2016; Lee et al., 2013; Sidibe, 2020), CSR practices (Maloni & Brown, 2006; Palazzo & Richter, 2005; Yani-de-Soriano et al., 2012), corporate political lobbying (Diestre et al., 2020), governance practices (Karagiannis et al., 2019), pricing practices in the pharmaceutical industry (Balotsky, 2009; Hemphill, 2010), and voluntary measures to minimize the use of potentially hazardous chemicals in products (Scruggs & Van Buren, 2016). The literature reviewed highlights a few studies on multilevel actions related to the interactions between business and patients to determine appropriate health care solutions to patients’ health needs (Angeli & Jaiswal, 2016), the pricing negotiation between business and governments for HIV/AIDS medications (Flanagan & Whiteman, 2007), and the engagement of business, communities, and governments in initiatives for community health challenges (Lumpkin & Bacq, 2019; Pless & Appel, 2012; Van Cranenburgh & Arenas, 2014), among others. Organizational constraints and institutional contexts affect a firm’s ability or willingness to address health challenges.
Organizational constraints include coordination costs, goal and incentive conflicts, and information asymmetries between business and other actors, all of which hinder the mobilization of coordinated resources for collective goals and actions to meet health challenges. Some of the organizational constraints that impede the pursuit of collaborative efforts toward addressing health challenges include inadequate conflict resolution and resource orchestration among business and its stakeholders (Lumpkin & Bacq, 2019); information asymmetries between the firm and its stakeholders, such as consumers and government agencies (Scruggs & Van Buren, 2016), and between farms and food manufacturers (Levi et al., 2020); and constant tensions between the firm’s pursuit of short-term profitability and its long-term commitment to health-related initiatives or schemes (Gewertz & Amado, 2004; Radermacher & Brinkmann, 2011; Van Cranenburgh & Arenas, 2014). In each case, these constraints hinder the ability of firms to engage in multilevel health initiatives.
Institutional contexts provide the rules of the game that underpin how multiple actors engage in health challenges. Examples of institutional contexts include political institutions such as policymaking processes, regulatory environments, and sociocultural institutions. Our analysis reveals that institutional contexts can expedite actions to meet health challenges, including the World Trade Organization’s Agreement on Trade-Related Aspects of Intellectual Property Rights (Vakili & McGahan, 2016) and health activism (Derry & Waikar, 2008). Also, the existence of environmental ministries and international environmental nongovernmental organizations (NGOs) can serve as an institutional context that promotes health (e.g., industrial water pollution that leads to adverse health consequences can be mitigated by such organizations; Jorgenson, 2009). However, institutional contexts can also obstruct efforts toward improving health. For instance, multilateral agreements like the U.S.–Mexico–Canada Agreement (formerly, North American Free Trade Agreement) may undermine sovereign nation-states’ capacity to set and enforce their own environmental and health regulations (Oliver, 2005). Other similar examples include government bureaucracy (Pless & Appel, 2012) and World Bank structural adjustment mechanisms such as trade liberalization, privatization, and deficit reduction (Shandra et al., 2011). Unfortunately, bureaucracy can slow down the implementation of multilevel initiatives, whereas structural adjustment concentrates government attention on economic issues rather than health goals.
Health outcomes and impact
Finally, actions lead to outcomes and impact. Our review of the business–health nexus confirms considerable variation in measuring health outcomes (Beets, 2019; Diestre et al., 2020; Han et al., 2020; Han & Hyun, 2019; Jorgenson, 2009; Shandra et al., 2011; Vakili & McGahan, 2016; Yani-de-Soriano et al., 2012). First, a few reviewed studies focus on the link between business activities and community health outcomes. Examples of such outcomes include child mortality and total fertility rates (Jorgenson, 2009; Shandra et al., 2011), infant deaths/1,000 live births, heart disease and cancer deaths/100,000 population, and life expectancy (Beets, 2019). Beets (2019) compares several indicators of health outcomes and quality of life between those who live in states that have many broiler growing facilities and those who live in states that have no or few broiler growing facilities. The author confirms that states with large concentrated animal feeding operation (CAFO) broilers show worse population health measures than states with small or no CAFO broilers in terms of the higher rate of infant deaths/1,000 live births, the greater incidence of heart disease and cancer deaths/100,000 population, the lower life expectancy, and the lower quality of life indices drawn from the Human Development Index and the Organization for Economic Cooperation and Development Quality of Life Index.
Second, some reviewed studies deal with the relationship of business activities to consumer health outcomes, such as drug-related side effects (Diestre et al., 2020), mental health perceptions of customers (Han et al., 2020; Han & Hyun, 2019), and online gamblers’ psychological distress and physical health (Yani-de-Soriano et al., 2012). For instance, Yani-de-Soriano and colleagues (2012) examine how online gambling companies negatively affect the gambler’s mental and physical health and the authors measure psychological distress and physical health with muscle ache, wrist pain, backache, sleeplessness, and indigestion. The authors find that among three categories of gamblers—no problem, at risk, and probable pathological—probable pathological gamblers report the highest degree of psychological distress and physical health problems. In the context of the tourism sector, both Han and colleagues (2020) and Han and Hyun (2019) investigate the effect of nature-based solutions—such as green indoor and outdoor environment and green atmospherics—on customer mental health and they collect survey data to measure mental health perceptions of customers. Han and Hyun (2019) demonstrate that green indoor and outdoor surroundings in a hotel are positively associated with customers’ perception of mental health and emotional well-being. Han and colleagues (2020) confirm that specifically designed green spaces in international airports positively affect visitors’ mental health.
The ability of multilevel actions to generate these health impacts is moderated by two factors: coordinating architectures and reinforcing mechanisms. A coordinating architecture refers to a coherent set of norms, an organizational structure, or a platform that allows actors to bring together various resources and capabilities to achieve collective goals (George et al., 2016), which in the present case is health. Within the set of studies examined, we identify three types of coordinating architectures. First, business may use a corporate philanthropic organization as a platform to deploy limited resources efficiently between its subsidiary, local NGOs, and governments (Van Cranenburgh & Arenas, 2014). Second, a multistakeholder initiative may consider involving a facilitator to advance their actions on health challenges. Lumpkin and Bacq (2019) illustrate that a facilitator, like a consultant, can play a role in helping multiple stakeholders—business, communities, and governments—communicate effectively, as well as identify and combine complementary resources and capabilities needed to achieve a civic-level health initiative in a sustainable manner. Third, a shared norm among multiple stakeholders can help them make ongoing commitments and systems to achieve health initiatives. For instance, Leisinger (2005, 2009) suggests that the universal norm for access to medical care for all can help multiple actors—including the pharmaceutical industry, governments, NGOs, and multilateral and bilateral donors—sustain the shared responsibility, thereby facilitating a multistakeholder approach to bringing together different types of resources and capabilities. In each case, these factors enable the scaling of impact by using resources more efficiently, coordinating stakeholder efforts more effectively, or reducing political opposition to potentially controversial health access policies.
To sustain motivation, reinforcing mechanisms enable business and other actors to commit to and continue to engage in efforts to resolve specific health challenges. In the absence of these mechanisms, the health impacts of these interventions are reduced simply because such efforts cannot be sustained over time. As we observed in relation to the COVID-19 pandemic, one health crisis pandemic may serve as a reinforcing mechanism that shifts the attention of actors toward other existing health challenges such as inequalities in access to health care services and medicines and populations with underlying health conditions like noncommunicable diseases. Our review includes a couple of articles from “Preparing for a Pandemic,” a special report published by Harvard Business Review in 2006. In this report, Cooper (2006) briefly describes how the 2003 outbreak of severe acute respiratory syndrome (SARS) drew societal actors’ attention to a city’s ineffective health care system that caused delays in testing and essential treatments. Staples (2006) suggests that the H5N1 strain of avian flu represents a nontraditional global threat and the flu presents an opportunity for business to attend to its pandemic preparedness and continuity planning. In a similar vein, dominant health concerns, including obesity (Schrempf, 2014; Tempels et al., 2020) and HIV/AIDS (Flanagan & Whiteman, 2007; Van Cranenburgh & Arenas, 2014), may direct actors’ attention toward larger health challenges.
An Overdue Business–Health Research Agenda
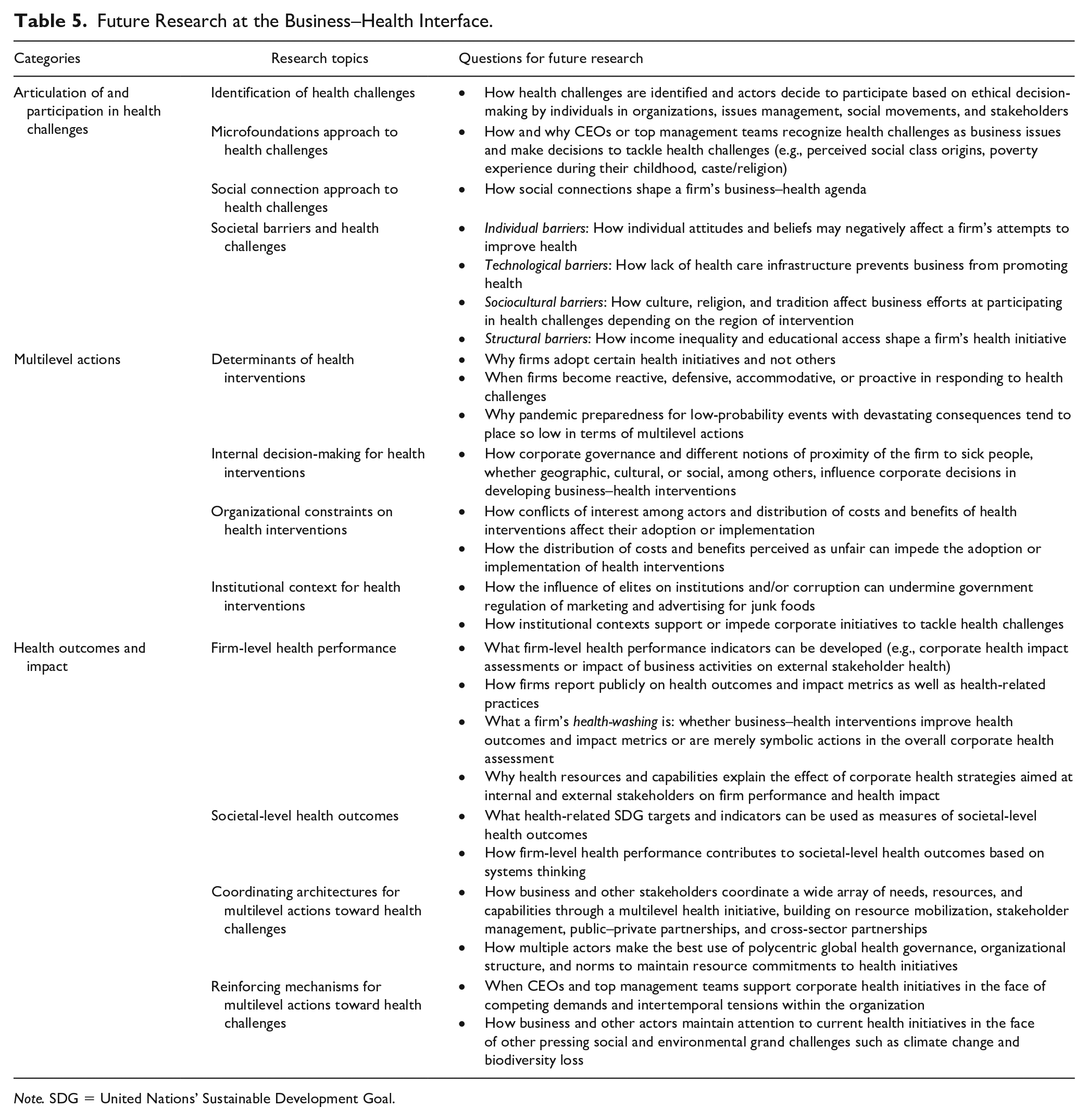
We began this review by asking the question, “What do the current business and management literatures say with respect to the social health costs that business imposes on its external stakeholders and society?” In short, the answer appears to be—not much. After surveying literature related to business and health from 1986 to September 2020, only 91 articles satisfied our search criteria, which focused on external stakeholders: consumers and communities. We found that this literature is highly fragmented, sharing only a few citations, and largely inward-looking, rarely stepping outside the business literatures to engage with the large body of work in public health and medicine. Generally speaking, the current literature only establishes a link between business and health when liability is direct (e.g., occupational health). Only rarely does it look at the role of business as part of a larger system, where its activities may indirectly improve or undermine health. For example, we did not find empirical studies analyzing the health impacts of business on external stakeholders such as supply chain partners, employees’ families, and the surrounding communities. Similarly, the prevention of health challenges did not appear in our review, although business has the potential to not only act when health challenges are present but also prevent them from happening. Although the 91 studies found in this review do not represent a vast body of scholarship, the current management literature provides a wealth of resources to begin research into health challenges. We now return to the final mapping within the higher-order framework to organize potential management and organizational theories and research questions to spur future work at the business–health crossroads. Table 5 summarizes questions for future business–health research that we discuss below.
Future Research at the Business–Health Interface.
Note. SDG = United Nations’ Sustainable Development Goal.
We organize avenues for future research direction for the business–health literature in terms of (a) articulation of and participation in health challenges, (b) moving from articulation to action, and (c) transforming action into health outcomes and impact.
Articulation of and Participation in Health Challenges
In this section, we examine how actor needs and aspirations as well as societal barriers enable or hinder the articulation of and participation in grand challenges by firms. First, articulation and participation of the firm in addressing health challenges are connected with existing literature discussing the identification of moral and social issues regarding business activities. Whether using models of ethical decision-making by individuals in organizations (Jones, 1991), issues management (Dutton & Duncan, 1987), social movements theory (McCarthy & Zald, 1977), or stakeholder theory (Freeman, 1984), current literature in the field of business and society deals with the identification and activation of actor needs and aspirations in response to an incipient issue. These theories can be applied to processes of articulating and participating in health challenges whether at the individual, firm, or systems level of analysis.
At the individual level, scholars may apply microfoundations approaches (Barney & Felin, 2013; Felin et al., 2015) to investigate how the individual cognition of CEOs or top management teams is organized as collective needs and aspirations at the firm level. Future studies can also explore how characteristics of CEOs, top management teams, and board members influence the recognition of health challenges as business issues. In this vein, one interesting path lies in how CEOs’ social backgrounds—such as perceived social class origins (Kish-Gephart & Campbell, 2015), CEOs’ poverty experience during their childhood (Xu & Ma, 2021), and CEOs’ caste/religion preference (Damaraju & Makhija, 2018)—determine their approach to and decision-making in addressing health challenges and CSR.
At the firm level, it is worth reflecting on the different approaches that business adopts toward health challenges. We see a new research stream where both business and researchers identify health as a grand challenge and take a social connection approach to health challenges (Schrempf, 2014; Tempels et al., 2020) rather than a legal approach that considers health as a liability issue rather than a basic human right to be fulfilled. The social connection approach is also useful to study health from a systems perspective because health challenges are indeed systemic. The causes and consequences of individual actions are difficult to pinpoint. Thus, solutions require coordinated and collaborative actions at multiple levels and by multiple actors. Future research can also examine how diverse actors’ health needs and aspirations—whether employees, neighboring communities, or marginalized and forgotten populations—shape business–health agendas.
Second, understanding the roots and consequences of societal barriers is critical in the business–health space, given that such barriers may hinder business efforts at recognizing and addressing health challenges. Regarding individual barriers, behavioral and cognitive theories in the organizational context can help explain such barriers, including, but not limited to, individual attitudes and beliefs toward certain diseases or vaccination (Blume, 2006) that may negatively affect firms’ attempts to improve health. For technological barriers—combined with institutional voids in emerging economies’ premises (Mair et al., 2012)—scholars may explore how health care service deficiencies prevent business from promoting health. These deficiencies may range from the lack of infrastructure to deliver health services in rural areas to the lack of health care infrastructure even within hospitals (e.g., the absence of simple refrigeration systems to preserve vaccines). Similar to individual barriers, sociocultural barriers can also deter business efforts to promote health. Future studies should investigate how cross-cultural differences (e.g., considering cultural dimensions such as Hofstede’s), religion, and customs affect business efforts at participating in health challenges depending on the region of intervention. For instance, just as HIV/AIDS has been stigmatized in urban religious congregations (Bluthenthal et al., 2012), certain diseases have been stigmatized in some cultures, presenting hurdles for any actor, including business, to promote health. Finally, understanding more structural barriers—such as income inequality and access to education—that can affect any business–health initiatives is critical.
Another structural barrier of extreme relevance to the business and health interface is income inequality, which is considered a grand challenge that has the potential to adversely affect health and well-being (Bapuji, 2015; Elmes, 2018; Jiang & Probst, 2017; Pickett & Wilkinson, 2015). We suspect that business-induced income inequality may function as a crucial grand challenge leading to adverse health outcomes. One basic feature of human life is that we compare ourselves with one another in an effort to gauge how well we are doing. These comparisons generate a stratification of people according to status (Festinger, 1954), which can be defined as “the prestige accorded to individuals because of the abstract positions they occupy” (Gould, 2002, p. 1147). It is not surprising that income is an important basis for comparison with others (Hagerty, 2000). Thus, relative differences in income create differences in status, which then generate competition for status (Wilkinson, 2006). Individuals experience a range of health effects as a result of chronic stress created by anxiety over status. Stress refers to “a cognitive perception of uncontrollability and/or unpredictability that is expressed in a physiological and behavioural response” (Koolhaas et al., 2011, p. 1292). That chronic stress then creates harmful physiological consequences for the individual (Wilkinson, 2006). Research has uncovered that people tend to compare themselves with their neighbors; in fact, people with wealthier neighbors experience chronic stress, which then leads to adverse health impacts (Pham-Kanter, 2009). Chronic stress, characterized by its frequency and duration, increases cardiovascular reactivity, which refers to the responsiveness of the cardiovascular system, such as heart rate and blood pressure, to stress (Berntson et al., 1998; Dimsdale, 2008). Specifically, stressors, such as anxiety from status competition, stimulate excessive catecholaminergic release and adrenalin, which can increase cardiovascular activity and depression (Kvetnansky et al., 2009). We know little about how grand challenges such as income inequality and education interact with other grand challenges including the one that we review in this article—human health. We urge researchers to pay close attention to all these societal barriers—especially structural barriers such as income inequality and lack of education—to inform business on how to best articulate and participate in addressing health challenges.
Moving From Articulation to Action
We offer research opportunities for the relationship of articulation to multilevel actions and two moderators of this relationship—organizational constraints and institutional contexts. Having articulated a problem at the business–health interface and decided to participate in its solution, business must turn to action at multiple levels. So why do organizations adopt certain business–health initiatives and not others? Much of organizational theory, including institutional theory (DiMaggio & Powell, 1983), resource dependency (Pfeffer & Salancik, 1978), organizational economics (Williamson, 1985), and population ecology (Hannan & Freeman, 1977), has been concerned with the adoption of specific practices and structures by organizations. The business and society field adds to this work a focus on the responsiveness of organizations and their practices and structures to social and environmental issues, as specified in the reactive, defensive, accommodative, and proactive scale developed by Carroll (1979). This work on the responsiveness of the firm to the environment provides the business and society field with the tools to examine questions such as why some firms were quick to respond to the H1N1 swine flu pandemic by liberalizing sick leave policies and creating backup systems to cover sick employees while others were reluctant. The Harvard School of Public Health (2010) performed a survey of employees regarding company preparedness for the 2009 H1N1 pandemic. Most believed that the H1N1 pandemic would help prepare their firms for future pandemics. Apparently, it did not and most of the business world was caught unprepared for the COVID-19 pandemic. Why has pandemic preparedness placed so low in terms of multilevel actions? Clearly, there is an opportunity to extend the literature on learning from catastrophes based on low-probability events with devastating consequences (Kunreuther & Useem, 2009).
In addition to the adoption of specific multilevel health interventions, we know little about internal decision-making and innovation processes that lead to the development of such actions by firms to reduce health threats and continue operations. The role of corporate governance in these decisions is also unknown. Comparing HIV/AIDS and H1N1, how did boards of directors influence decisions about health strategies? How do different notions of proximity of the firm to victims, whether geographic, cultural, or social, among others, influence corporate decisions?
Yet, not all medical interventions are harmless. For example, disease mongering—identifying new “diseases” that broaden the idea of illness and then selling supposed treatments (Moynihan et al., 2008)—the medicalization of conditions of everyday life by the pharmaceutical industry has received attention in the medical and popular press (Walsh, 2018). Yet, the problem continues largely unabated, with governments reluctant to intervene. How will actor needs coalesce around the problem so that Big Pharma will acknowledge the problem and begin to respond?
This review has revealed that the existing scholarship on organizational constraints on multilevel actions has barely scratched the surface. The many conflicts of interest and distribution of costs and benefits related to health interventions can affect the adoption or proactive implementation of health interventions. In addition, research on the perception of the fairness of the distribution of costs and benefits perceived as unfair can often impede the adoption or implementation of organizational practices related to stakeholder relations (Husted, 1998), including health interventions. Just as the perception of unfairness influences the degree to which employees accept human resource practices (Folger & Cropanzano, 1998), the alignment or misalignment of fairness perceptions could affect the ability of all sorts of transactions, including health interventions, to take place or could increase the costs associated with these interventions (Husted & Folger, 2004).
Institutional contexts significantly influence the ability of organizations to act. A clearly articulated vision to participate in improving health can be hindered by institutions that enforce regulations unevenly and create an uneven playing field for companies. Institutional contexts can vary according to the incompleteness of institutions as well as the influence of elite interests on institutions (Dorobantu et al., 2017). Clearly, work needs to be undertaken that explores how different institutional contexts facilitate or hinder the effective implementation of health interventions. How has government regulation of marketing and advertising practices related to “junk” foods, or the lack thereof, influenced the severity of childhood obesity around the world? How has the influence of elites on institutions or corruption undermined efforts at such regulation? How does the variation in institutional contexts in nations and communities support or impede corporate initiatives to tackle health challenges?
Transforming Action Into Health Outcomes and Impact
In this section, we discuss the direction of future research on the impact of multilevel actions on health outcomes along with two moderators: coordinating architectures and reinforcing mechanisms. Our analysis reveals that business research has yet to actively undertake empirical studies addressing the outcomes of business–health initiatives. Companies have key firm-level performance indicators to evaluate not only their financial performance but also environmental, social, and governance (ESG) performance. However, firm-level health performance evaluations, such as corporate health impact assessments (Anaf et al., 2017; Baum et al., 2016) or the evaluation of the impacts of business activities on external stakeholder health, have rarely been implemented. The impact of business on external stakeholder health spans from workers’ health conditions to health-related consumer behavior, such as food consumption and health care–seeking behavior, to community-level health indicators, such as air and water quality and exposure to pollutants (Baum et al., 2016). Similar to a natural-resource-based view, future studies could theorize a health-resource-based view of the firm to explain the link between corporate health strategies aimed at internal and external stakeholders, on one hand, and firm competitive advantage and health impact, on the other hand. Such a new theoretical perspective on the relationship of business to health factors has the potential to help scholars shift attention toward health outcomes attributable to business (Pfeffer, 2010).
Although still incipient, current literature has encouraged moving the management literature to carefully examine the social impacts of CSR initiatives (Barnett et al., 2020; Rawhouser et al., 2019). We acknowledge that some aspects of health are easily attributable to business and often are covered by extensive legislation, including health and safety at work or consumer health. It is less easy to see why such obligations should be extended to issues related to indirect stakeholders, such as child mortality and fertility rates. Nevertheless, a social connection approach to health challenges offers business scholars and practitioners the ability to embrace both the direct and indirect impacts of business on health, including issues such as the influence of advertising on the consumption of soft drinks, which can lead to obesity.
Regarding an example of business–health outcome and impact metrics, BSR (formerly known as Business for Social Responsibility), a global nonprofit organization of sustainable business experts, launched the Healthy Business Coalition initiative via collaborative efforts with the Robert Wood Johnson Foundation and leading firms. The initiative aims to provide guidance on corporate health impact assessments (i.e., how business can invest in health programs along its value chains; BSR, 2016) and measure outcome and impact metrics of its health-related program (BSR, 2018). Building on the BSR initiative’s five business–health categories from access to care, disease burdens, economic and social determinants of health, healthy behaviors, and physical environment, the initiative suggests outcome metrics—such as greenhouse gases and pollutants and water discharge as part of environmental responsibility and universal coverage—and impact metrics—including affordability of health care, chronic respiratory illness mortality, healthy eating choices, infant mortality rates, and obesity rates (BSR, 2018). Similarly, the recently released recommendations to business from the Office of the U.S. Surgeon General to contribute more broadly to community and economic prosperity provide a solid outline of the business case for greater investment in community health, including the steps for developing a business strategy that would eventually result in more data on the linkages between corporate action and community health (Office of the U.S. Surgeon General, 2021). Future studies can consider the use of these business–health outcome and impact metrics to investigate the influence of business activities on external stakeholder health.
In addition, the BSR’s Healthy Business Coalition initiative points to the potential contribution of business efforts to advocating for health equity and shared health ambitions outlined in the SDGs (BSR, 2018). Since its launch in 2015, the 2030 SDG Agenda has provided business scholars and practitioners with a coherent guideline for health measures, given that the SDGs have been broadly adopted, not only by governments but also by academia and business in both developing and developed countries. The SDGs consist of 17 goals with 169 related targets to be achieved by 2030 and are considered the most effective cross-country plan of action to address pressing grand challenges (Cuervo-Cazurra et al., in press; Montiel et al., 2021). Future research should consider the use of health-related SDG targets and indicators as measures of health goals according to the type of health challenges and the types of actors involved in solving or aggravating those challenges. The health-related SDG targets include Target 3.1, Reduce the global maternal mortality ratio to less than 70 per 100,000 live births; Target 3.3, End the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases; Target 3.5, Strengthen the prevention and treatment of substance abuse, including narcotic drug abuse and harmful use of alcohol; Target 3.8, Achieve universal health coverage, including financial risk protection, access to quality essential health care services and access to safe, effective, quality and affordable essential medicines and vaccines for all; and Target 3.9, Substantially reduce the number of deaths and illnesses from hazardous chemicals and air, water, and soil pollution and contamination (United Nations Development Programme, 2020). Each of these offers abundant opportunities for future work. Building on systems thinking, scholars could delve into how firm-level health performance contributes to societal-level health outcomes.
Another important avenue of inquiry can explore how firms report publicly on health outcome and impact metrics as well as health-related practices. Similar to greenwashing (Delmas & Burbano, 2011; Lyon & Montgomery, 2015; Ramus & Montiel, 2005), firms might end up engaging in health-washing (i.e., the discrepancy between a firm’s claims and actions toward making its operations, products, and services appear healthier). For example, firms can diversify their portfolio toward healthier products and services by acquiring other healthier companies (e.g., Philip Morris’s takeover bid to purchase Vectura, a British asthma inhaler maker; Ziady, 2021). Also, firms may pursue partnerships with nonprofit organizations addressing health challenges to be perceived as if they are genuinely concerned about health challenges (e.g., McDonald’s partnership with the U.S. Academy of Nutrition and Dietetics; Stan, 2017). To determine whether these strategic moves fall under health-washing, it is important that business scholars assess whether these strategic moves improve the actual health outcomes and impact metrics or are a merely symbolic action resulting in no substantive changes in the overall corporate health assessment. Next, we turn our attention to the factors that facilitate or hinder the transformation of actions into outcomes and impact (a) coordinating architectures and (b) reinforcing mechanisms.
Our review shows that there are still many opportunities for business scholars to examine the coordinating architectures through which the interdependence between business and other actors—including community members, consumers, patients, school children, health activists, regulators, and medical community—shapes health consequences. In many cases, standalone business actions may not be able to tackle health challenges effectively, given their inherent complexity. For example, Kraiselburd and Yadav (2013) provide insights into the detrimental impact of poorly designed global health supply chains. The authors contend that the coordination of multiple supply chain stakeholders’ divergent interests is key to tackling health challenges because such coordination significantly affects the purchase and distribution of medicines, vaccines, and health technologies that are essential to all aspects of health. Current literatures on CSR and multistakeholder collaboration (Boiral & Heras-Saizarbitoria, 2017; Elia et al., 2020) may be harnessed to examine how business and other stakeholders coordinate a wide array of needs, resources, and capabilities through multilevel health initiatives. Studies on resource mobilization (Jenkins, 1983), stakeholder management (Freeman, 1984), public–private partnerships (Roehrich et al., 2014), and cross-sector partnerships (Johnston & Finegood, 2015) may also provide insights into not only how the nature of a health challenge takes different forms of coordinating architectures among actors but also how the actors make the best use of such architectures to attain health goals. Examples include polycentric global health governance that has the potential to embrace multiple voices and perspectives to influence the health agenda of countries and multilateral institutions (Held et al., 2019; Tosun, 2017), and organizational structure and norms designed to maintain continuous resource commitments to health initiatives among business and other stakeholders.
For reinforcing mechanisms, our review shows that scholars have not examined the conditions under which such outcomes can sustain and reinforce actors’ attention and actions to address health challenges. Similar to other business sustainability agendas that oftentimes yield competing demands (Hahn et al., 2010; Wright & Nyberg, 2017) and/or intertemporal tensions (Slawinski & Bansal, 2012), it is likely that business is faced with such trade-offs and tensions between the pursuit of short-term profitability and the long-term vision of health initiatives. Hence, scholars should continue to research the circumstances under which CEOs and top management teams can uphold health initiatives that the firm pursues in the face of competing demands and intertemporal tensions within the organization. Moreover, building on the attention-based view (Ocasio, 1997), future studies can investigate how business and other actors maintain attention on current health initiatives in the face of other pressing grand challenges such as poverty, inequality, and climate change (Montiel, 2020). For instance, COVID-19 diverted much-needed attention and financial and human resources to tackle the pandemic while probably neglecting other diseases. Hence, scholars should continue to research the circumstances under which the consequences of social and structural issues and natural events reinforce or attenuate the ongoing efforts of business and its stakeholders toward achieving health goals. One important theme to be addressed as part of a reinforcing mechanism is the link between business, climate change, and health. Climate change has created extreme weather patterns and posed a threat to human health (Watts et al., 2021). However, it is surprising that business has paid little attention to the climate change–health connection, while it is more focused on financial climate risks such as disrupted supply chains and increased insurance costs (Deloitte, 2021). It is thus crucial that business scholars analyze the climate change–health connection. After all, climate change is affecting human health and business is also responsible for climate change.
The management literature thus provides an excellent foundation for studying many of the elements in Figure 2. We have reviewed how actor needs and societal barriers enable or hinder the firm’s articulation of and participation in health challenges. We examined how organizational constraints and institutional contexts moderate the transformation of the decision to participate into concrete actions at multiple levels. Where the management literature provides the weakest foundation is in the human health outcomes and impacts of these actions.
Bringing Public Health Insights Into the Business–Health Literature
As demonstrated in the previous section, the management literature falls short in providing a platform for research into the relationship between multilevel actions and health outcomes. It is in this relationship represented by the second thick arrow in Figure 2 where current theory is insufficient. Here, business scholars may need to turn to colleagues in the fields of public health to begin to develop new models relating business to health. To illustrate the possibilities, we point to three emerging literatures that will be helpful in elaborating these theoretical relationships, namely, (a) social determinants of health, (b) commercial determinants of health and noncommunicable diseases, and (c) emerging infectious diseases, which we encapsulate in Table 6.
Public Health Insights for a Business–Health Research Agenda.
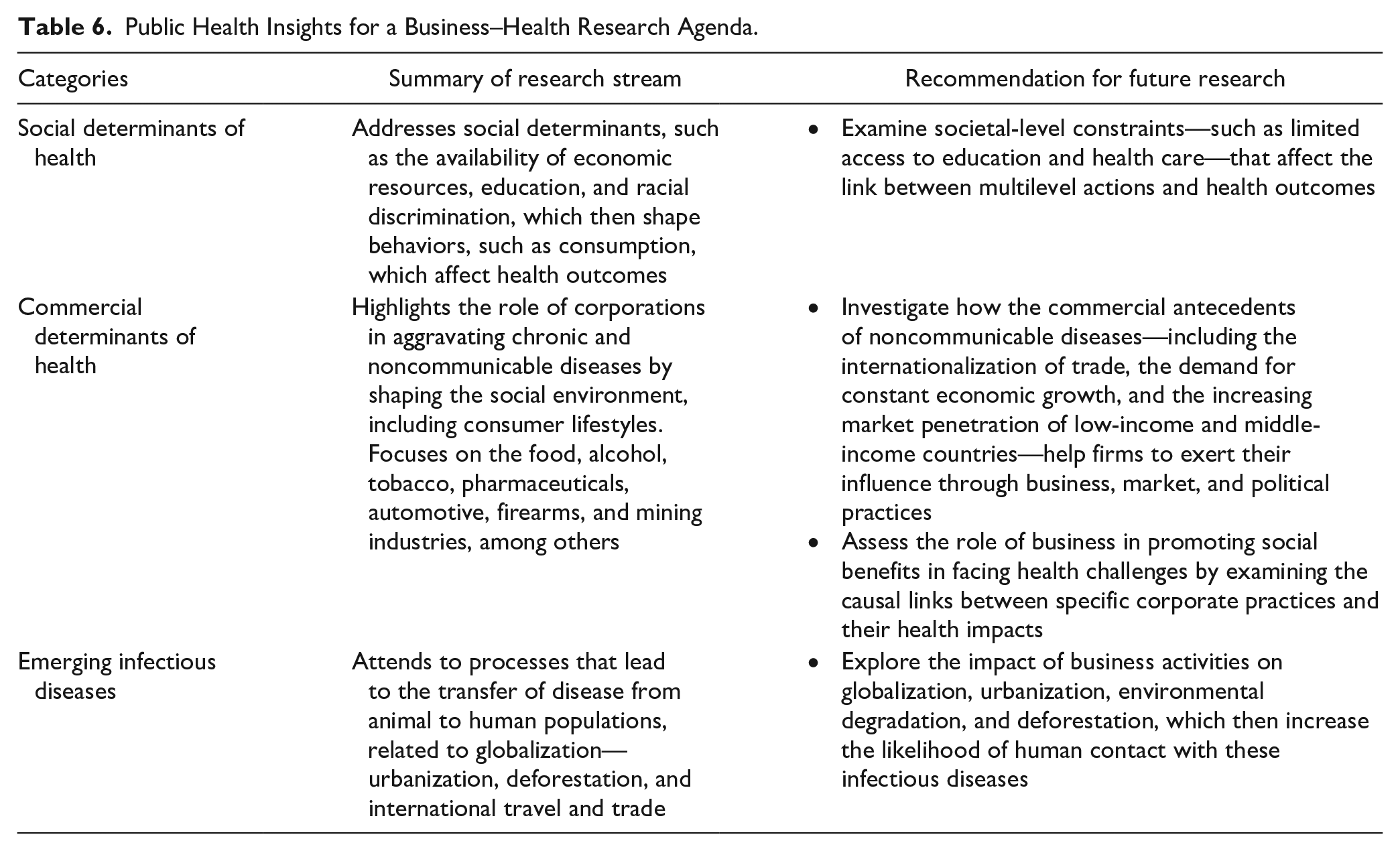
Social Determinants of Health
Social determinants include the availability of economic resources, education, and racial discrimination, which then shape behaviors, such as consumption, which affect health outcomes (Braveman et al., 2011; Braveman & Gottlieb, 2014). This literature ties into development studies via a common interest in the work of Nobel Laureate Amartya Sen (1999a, 1999b) and his capabilities approach. What is more important for health and development is not the level of economic development of a country as measured by gross domestic product (GDP) per capita, but the opportunities that people have for access to education and health care. This literature formed the basis of the commercial determinants of health literature that has developed over the last decade.
Commercial Determinants of Health
The literature on the “commercial determinants of health” or “corporate determinants of health” explores how
health outcomes are determined by the influence of corporate activities on the social environment in which people live and work: namely the availability, cultural desirability, and prices of unhealthy products. The environment shapes the so-called lifeworlds, lifestyles, and choices of individual consumers—ultimately determining health outcomes. (Kickbusch et al., 2016, pp. e895–e896)
The commercial determinants of health have highlighted the role of corporations in chronic and noncommunicable diseases, such as obesity, diabetes, heart disease, and cancer (de Lacy-Vawdon & Livingstone, 2020; Kickbusch et al., 2016; McKee & Stuckler, 2018; Mialon et al., 2020). There is also a strong industry focus, including the food, alcohol, tobacco, pharmaceuticals, automotive, firearms, and mining industries, among others.
Public health scholars have identified several frameworks that examine the link between business and chronic and noncommunicable diseases. At the institutional level, Millar (2013) uses a market failure framework to justify government intervention to regulate the sale of sugar, fat, and salt. At the firm and industry level, McKee and Stuckler (2018) find four ways in which business affects chronic/noncommunicable disease: helping set the dominant narrative, setting social rules, commodifying knowledge, and undermining human rights. The commercial antecedents of noncommunicable diseases include the internationalization of trade, the demand for constant economic growth, and the increasing market penetration of low-income and middle-income countries (Labonté et al., 2011). These drivers help firms to exert their influence through business, market, and political practices. Business practices—such as supply chain management, labor relations, tax avoidance, and profit shifting—can affect the health of both employees along the value chain and other people (Kickbusch et al., 2016; Mialon et al., 2020). Market practices related to health, which include research and development, pricing, advertising, and distribution, influence consumers to make poor choices (Mialon et al., 2020). Political practices such as lobbying, political contributions, and even CSR can be used to influence public policy to benefit corporate interests (McKee & Stuckler, 2018).
Emerging Infectious Diseases
Researchers have found that emerging infectious diseases occur as a result of increasing contact between human and animal populations (Daszak et al., 2000; Frenk et al., 2011). The processes that lead to zoonosis, or the transfer of disease from animal to human populations, are closely related to global economic development: urbanization, deforestation, and international travel and trade. In processes that mirror those of humans, deforestation, for example, upsets delicate habitats for animal populations, which generates stress. Just like stressed humans, stressed animals suffer weaker immune systems and become more susceptible to viruses. Urbanization and the trafficking of wild animals can then become a vehicle for zoonosis as humans and animals come into closer contact. With globalization, such animal–human crossovers of viruses are then carried around the world.
In summary, there exist three public health literatures—the social determinants of health, the commercial determinants of health, and emerging infectious diseases—that provide relevant insights into the impacts of multilevel actions on health outcomes and impacts. Although the commercial determinants of health address the role of the business firm directly, the social determinants of health and emerging infectious diseases need to bring the firm in more prominently. These literatures speak more broadly of general social processes like globalization, in which the firm plays a central role. Nevertheless, the firm’s role in globalization as it relates to human health as generally been mentioned, rather than addressed directly. The opportunities for partnerships between business and health scholars to explore this role are almost limitless.
Recommendations for an Interdisciplinary Approach to the Business–Health Literature
Public health studies have the potential to provide business scholars with complementary insights into the impact of business on the health of external stakeholders. Yet, a significant weakness of the public health literature is the lack of empirical research in the area. For instance, the commercial determinants of health literature remain largely conceptual and descriptive (de Lacy-Vawdon & Livingstone, 2020). Another observation is that public health studies lack nuance with respect to the business firm, treating it as a black box. Business scholars could provide much-needed detail here. In the case of both the literatures on the commercial determinants of health and emerging infectious diseases, business seems to be primarily seen as the culprit as it participates in a relentless pursuit of profit.
Nevertheless, the case of HIV/AIDS does reveal ways in which business can contribute to both the development of supportive policies for employees, including educational and training programs (Kohl et al., 1990) as well as participation in transnational policy networks (Dahan et al., 2006), and the research and development of new vaccines and treatments. Certainly, the role of business should be scrutinized, but its potential for positive social benefit in facing health challenges should not be overlooked. Not all business influence on health is negative. When do firms exert a positive influence on health outcomes? Many of these themes are familiar to business and society scholars, but references to the corporation as a “vector of disease” are alarming (Gilmore et al., 2011, p. 2). Most of this literature is very recent, having appeared in the last 10 years or so. Although there are some published commentaries and perspectives, business and society scholars can make sound contributions to the commercial determinants of health literature by examining the causal links between specific corporate practices and specific health impacts.
The literature stream of emerging infectious diseases is another avenue that business scholars could investigate further. Firms usually participate in processes such as urbanization, deforestation, and globalization, which then increase the likelihood of human contact with these emerging infectious diseases. The COVID-19 pandemic has alerted us to the importance of emerging infectious diseases, but other diseases such as HIV/AIDS and dengue fever suggest that the role of business in the spread of infectious diseases deserves much greater attention. In the case of emerging infectious diseases, the causal chains between business and health involve many more links than in the case of noncommunicable diseases. Nevertheless, research focused on environmental degradation has raised the issue of emerging infectious diseases and the increased risk for pandemics (Castro et al., 2019; Young et al., 2006). Yet, only rarely have emerging infectious diseases been studied by business scholars; HIV/AIDS, which also involved zoonosis, did make it onto the radar screen of businesses and researchers, while other diseases did not.
Clearly, the relationship between business and health is an unusually complex one. The time lags involved between a specific business practice and a health outcome are long and the causal links are many. In addition, analyzing the impact of business on health challenges requires systems approaches that are not always easy to implement in our more traditional firm-level research approaches. It is unlikely that a single study can cover everything from a particular business practice to a health outcome. However, through collaborating with colleagues in other disciplines, knowledge may advance incrementally by focusing on particular links in the causal chain. It is probably wise to explore additional interdisciplinary collaboration that not only embraces the public health research community but also establishes bridges between different business academic disciplines from strategy and economics to social psychology, marketing, and consumer research. Management scholars, together with scholars of marketing, social marketing, consumer behavior, and responsible consumption as well as sociologists, and psychologists, would be especially well equipped to focus on the relationship between business practices and their impact on human behaviors, whether consumers, employees, or others. Then, colleagues in public health could take the next step of linking specific behaviors to health outcomes. Such collaboration is essential when designing specific interventions in business practices to influence human behavior and then health outcomes. Such interventions would require an intimate knowledge of business and its inner workings as well as the psychology of human actors and the health sciences, necessitating such collaboration.
Study Limitations
No study comes without limitations. First, our review focuses on a set of business management academic journals while intentionally omitting potentially relevant articles from neighboring disciplines such as public and environmental health, international development, marketing, and consumer research. Our brief detour into the public health literature has been suggestive but not conclusive. In addition, our focus on academic journals also excludes other research documents produced by consultancies like BSR, government agencies like the Office of the U.S. Surgeon General, and international agencies like the World Economic Forum or the World Health Organization. We encourage researchers to continue exploring this work as it can also inform us about business–health interdependencies.
Second, we discuss the grand challenge of human health by examining the conditions under which business generates social health costs and negative externalities for human health, rather than how business may support the development of good health and well-being. Future studies should delve not only into how business responds to health challenges but also into how it contributes to improving overall health and well-being in a proactive manner.
Concluding Remarks
As the COVID-19 pandemic unmasked immense deficiencies in health care systems worldwide during the first months of the 2020s, both humanity and business began to reconsider their relationship with health and their responsibility in protecting the health of all their stakeholders. In this article, we take stock of how business scholars have integrated the social health costs generated by business for external stakeholders into their research agendas only to find a set of fragmented studies that just scratch the surface of the complex interconnections between business and health. We hope that this study will inspire business scholars to shift scholarly attention from a more limited view of health as a private cost regarding internal stakeholders to a broader approach that (a) recognizes the many interdependencies between business and health, (b) integrates the social health costs of external stakeholders into their research questions, (c) treats health as a grand challenge that needs to be addressed, and (d) explores potential business contributions to achieving the health targets established by the SDGs. Once scholarly attention switches from healthy business to healthy communities, we are likely to see the beginning of a flourishing research agenda that enables business to improve health in collaboration with governments, researchers, communities, and civil society.
Supplemental Material
sj-docx-1-bas-10.1177_00076503211073519 – Supplemental material for The Grand Challenge of Human Health: A Review and an Urgent Call for Business–Health Research
Supplemental material, sj-docx-1-bas-10.1177_00076503211073519 for The Grand Challenge of Human Health: A Review and an Urgent Call for Business–Health Research by Junghoon Park, Ivan Montiel, Bryan W. Husted and Remy Balarezo in Business & Society
Footnotes
Acknowledgements
We thank Hari Bapuji, Jill Brown, and three anonymous reviewers for their constructive criticisms and helpful suggestions, which helped us improve our article. We also thank Michael Barnett, Matthew Caulfield, Carolina Mendes de Barros, Andres Velez-Calle, the Business & Society Co-Editors, and all attendees at the virtual presentation session for Business & Society’s 60th Anniversary Special Issue on October 23 of 2020, for their useful suggestions to improve the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: For financial support, I.M. and J.P. thank the Lawrence N. Field Center for Entrepreneurship at Baruch College, the City University of New York, and R.B. thanks the Department of Business Policy at Universidad de Piura (UDEP)—Campus Piura.
Supplemental Material
Supplemental material is available in the online version of the article.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.