
Abstract
Although socioeconomic status has been positively linked to health, little is known how socioeconomic disadvantage experienced in both childhood and adulthood influences cardiovascular illness in low- and middle-income countries. With particular emphasis on the elderly, this research uses Latin American data to test whether adult socioeconomic disadvantage, net of childhood socioeconomic disadvantage, is associated with being diagnosed with hypertension and experiencing a heart attack. This research also explores how location plays a role in the relationship between socioeconomic status and health by providing country-specific analyses. Findings indicate that while adult socioeconomic status is negatively associated with cardiovascular illness in the region overall, this relationship is positive in Argentina, Brazil, and Chile. Results suggest that, in the case of elderly Latin Americans, socioeconomic advantage did not uniformly translate into a definite health advantage.
Introduction
The rapid aging of the world’s population is now well-documented, with projections indicating that this trend will continue through 2050 (Kinsella et al., 2005). Demographically, this phenomenon is attributed to changes in the age structure and the decline in the risk of death at younger ages. Thus, late-life mortality is now a more crucial component of a country’s overall mortality than in the past (Grundy and Sloggett, 2003).
Among chronic illnesses, cardiovascular disease is the number one cause of mortality worldwide (World Health Organization, 2011). Although the death rate from coronary heart disease (CHD) is declining, the number of people who die from CHD is increasing (Mendis et al., 2011). To illustrate, there were 6.2 million global deaths from CHD in 1990 (Murray and Lopez, 1996), 7.3 million in 2001 (World Health Organization, 2002), and 17.3 million in 2008 (Mendis et al., 2011). Also, CHD deaths are concentrated at the older ages. Recent data suggest that individuals over the age of 60 are 4.4 times more likely to die from CHD than individuals aged 15–59 (Mendis et al., 2011). Moreover, while the rate at which people suffer from cardiovascular illness differs from region to region, its prevalence has increased in all countries (World Health Organization, 2011). Currently, more than 60% of the global burden of coronary heart disease occurs in low- and middle-income countries (Mendis et al., 2011). Thus, it is of increasing importance to better understand those factors that contribute to cardiovascular illness in order to propose effective preventative policy. Many behaviors associated with cardiovascular illness, such as smoking, drinking, and weight gain, are often acquired in childhood, yet they are seen as modifiable (Clark et al., 2009). Close to 90% of people dying from coronary heart disease possess at least one of these modifiable behaviors (Mendis et al., 2011). As a starting point for policy, many of the behaviors associated with cardiovascular illness also tend to be associated with poverty or low socioeconomic status.
Population dynamics, socioeconomic well-being, and health are issues that intersect in the context of Latin America. Demographically, this region, which includes South America, Central America, Mexico, and the Caribbean, is experiencing rapid population growth, especially among the elderly. Specifically, from 2003 to 2050, the population of Latin America is expected to increase by 42%, while the number of elderly adults will increase from 4% to 17% of the total population (Brea, 2003). Although this increase in the region’s elderly population is considered a public health success story, it presents many challenges. Like many low- and middle-income areas, Latin America is in the midst of an ‘epidemiologic transition’; rapid urbanization has given rise to diseases commonly associated with higher income, such as cardiovascular illness and diabetes (Schargrodsky et al., 2008). This disproportionate level of chronic disease could increase demand for health and social services, particularly for older individuals (Kalache and Keller, 2000). In addition, wealth accumulation and socioeconomic sustainability for the elderly must be maintained in order to keep up with the prolonged cost of health management for this highly fragile population (Kalache and Keller, 2000). Thus, socioeconomic well-being is a pressing factor that helps explain health among the elderly.
The purpose of this research is to identify how both childhood and adult socioeconomic characteristics are instrumental in understanding cardiovascular illness among the elderly. Data from a multinational survey on health and living conditions of people aged 60 and older in Latin America provide an opportunity to examine the associations of lifecourse socioeconomic well-being and cardiovascular illness in urbanized societies. Besides the increase in the elderly in Latin American countries, this region is also epidemiologically interesting, as medical advances and awareness, rather than social conditions, are the catalyst for population aging in the region. Thus, this research is poised to explore the influence of both material conditions (i.e., socioeconomic status) and health behaviors (e.g., alcohol use, healthy diet, or physical activity levels) on cardiovascular illness among Latin America’s elderly.
The Latin American context
When it comes to past studies of cardiovascular illness and socioeconomic status in Latin America, the literature is limited. A recent Google Scholar search indicates that as of 4 December 2013, approximately 3110 publications dealt with cardiovascular illness and socioeconomic status in Latin America (using ‘cardiovascular disease’, ‘socioeconomic status’, and ‘Latin America’ as search terms). By contrast, over 1.7 million publications appear when searching cardiovascular illness, over 1.7 million publications appear for Latin America, and nearly 1 million articles appear for socioeconomic status.
Thus, despite the surge of chronic diseases in Latin America, relatively few research articles examine the development of cardiovascular risk factors in this region. Furthermore, those studies that have looked specifically at cardiovascular risk factors in Latin American countries have yielded inconsistent results. For instance, it has long been argued that alcohol consumption does not offer protective cardiovascular benefits (Anderson et al., 1993). However, the opposite effect was found in Latin America where non-harmful levels of alcohol consumption were associated with lower levels of stress and lower risk of experiencing a cardiovascular event (Mendis et al., 2011). It may be argued that the difference in the cardiovascular risk factors within Latin America has led to variation in the prevalence of cardiovascular illness in the region. For example, some South American countries have experienced noticeable declines in the rate of cardiovascular illness while some Central American countries have seen rates increase (Reddy and Yusuf, 1998). The vast dissimilarities within extant studies, coupled with the increased chronic disease prevalence in Latin America, call for further investigation into the region’s cardiovascular risk factors and their relationship to socioeconomic status.
Socioeconomic status and health among the elderly
The literature on socioeconomic status and elderly health is mixed. Studies illustrate that elderly adults with high levels of socioeconomic status enjoy better health than those with low levels of SES (Feinstein, 1993). However, this effect tends to lessen over time (Adler and Newman, 2002), indicating that static measures of socioeconomic status (e.g., education) may be less consequential to elderly health than more dynamic measures (e.g., income).
The relationship between adult socioeconomic status and adult health seems to be formed at birth. From a systematic review of the biomedical literature, Pollitt et al. (2005) concluded that lower SES during childhood has a modest effect on adult cardiovascular outcomes that is direct and independent of adult SES. This ‘stickiness’ (Palloni, 2006) implies that socioeconomic conditions experienced during childhood have lasting effects on health beyond their initial impact on later-life status attainment. However, some research suggests that there is no significant association between childhood socioeconomic status and adult health once adult socioeconomic status is taken into account (Luo and Wen, 2002). The reverse has not been illustrated in the literature – that adult socioeconomic status effects on health can be attenuated by accounting for childhood SES.
Although there is much literature that discusses how elderly health is linked to childhood and adult socioeconomic status, there has been little attention devoted to this topic in low- and middle-income countries (Kawachi, 1997), with the notable exception of exploring how macro-level processes such as economic development impact all-cause mortality (Preston, 2007). In an attempt to reduce this knowledge gap, the present study seeks to understand how micro-level processes (e.g., socioeconomic status, healthy behaviors) impact micro-level phenomena (i.e., cardiovascular illness) in Latin America.
SES and cardiovascular illness
The relationship between socioeconomic status and cardiovascular illness has been longstanding in the literature. Studies from the 1930s document a negative relationship between SES and heart disease in both Europe and the US (Cassel et al., 1971). This phenomenon has also been witnessed in high-income areas such as New Zealand, Australia, and Scandinavia (Bennett, 1995; Blakely et al., 2002; Møller et al., 1991). Scholars suggest that this relationship is mainly attributable to social class differences in health-related behaviors. Smoking, excessive alcohol consumption, lack of physical activity, and inadequate nutrition are linked to cardiovascular illnesses such as hypertension and coronary heart disease, but they are also behaviors that are more prevalent in low social classes (Kaplan and Keil, 1993).
Factors other than lifestyle behaviors also link socioeconomic status to general health. Childhood illness, particularly major bouts of infectious disease, has been associated with cardiovascular conditions experienced as an adult, even after controlling for socioeconomic status (Blackwell et al., 2001). Moreover, research has suggested a non-negligible selection effect of childhood health on adult SES. That is, healthy children tended to be more educated than children with a childhood illness (Van de Mheen et al., 1998b). As a ‘psychological risk factor’ of cardiovascular illness, depression is also linked to SES (Lynch et al., 1996). While poverty has been linked to high levels of depression (Lynch et al., 1996), sociological and social psychological research has argued that macro-social structures (such as the economy and the health care system) and meso-level entities (such as neighborhood quality) are dually associated with SES and with cardiovascular outcomes (Link et al., 1993; Schnittker and McLeod, 2005). This body of research suggests that the links between depression and health is apparent across all levels of SES, not just the extremes.
Certain demographic characteristics could also be considered moderators of the SES–cardiovascular illness relationship. A recent meta-analysis suggests that gender matters in the development of cardiovascular illness. While premenopausal women have a lower tendency to develop hypertension than age-matched men, the rate of hypertension is significantly higher at advanced ages for women than for men and this gender difference is higher at lower levels of SES (Regitz-Zagrosek et al., 2007, emphasis added). As a ‘social risk factor’, being in a relationship represents a level of social connectedness that has been found to be beneficial to heart health and socioeconomic status. Marriage has been shown to have positive impacts on health behaviors and cardiovascular-related outcomes, particularly at older ages, but these effects differ by gender, with men receiving a relatively larger marriage benefit than women (Lynch et al., 1996; Schone and Weinick, 1998). Marriage also has been argued to carry some economic benefits (i.e., ‘marriage premium’), although those benefits seem to be more advantageous for men than women (Waite and Lehrer, 2003).
Regardless, research on how factors associated with both socioeconomic status and cardiovascular illness relate to social inequalities in health among elderly populations has been less frequent (Knesebeck et al., 2003). Rarer yet are studies that examine how socioeconomic status in both childhood and adulthood relate to both health behaviors and cardiovascular illness in low- and middle-income countries, especially among the elderly (Fleischer et al., 2008). This research attempts to reduce both these gaps simultaneously through the analysis of a multinational dataset containing childhood and adult measures of socioeconomic status and elderly health. By using these data, we intend to show how socioeconomic status and lifestyle factors relate to cardiovascular illness within a vulnerable population (i.e., the elderly).
Theories on SES and health
The relationships between socioeconomic status and health are multifaceted, leading scholars across various disciplines to investigate their complex dynamics. These perspectives need to be comprehensively integrated. Central to this discussion is the theory of fundamental causes (Link and Phelan, 1995), which suggests that even as risk factors (e.g., non-communicable diseases and poor living conditions) decline (Omran, 1971), the effects of socioeconomic status on morbidities and mortality persist. The mechanisms affecting this relationship are financial, social, and cultural capital (Bourdieu, 1986) that protects health regardless of the risk factors associated with the specific disease. Because high SES fundamentally contributes to good health, any risk factor interventions may not be greatly effective for people who have the same level of capital (McDaniel, 2013).
The social gradient of health perspective suggests that health increases as SES increases, irrespective of the risk factor considered. For many of the validated measures of SES such as education, income, and occupational class (Adler et al., 1994; Marmot and Theorell, 1988), this monotonic effect is apparent. Yet in the case of heart disease, the well-known Whitehall study sought to understand disparities in health among different socioeconomic levels (Fuller et al., 1980) and found that risk factors associated with coronary heart disease (e.g., smoking, high blood pressure, cholesterol) only explain a small part of the gradient. This led to the conclusion that the unexplained variation in CHD must be endogenous to the SES gradient (McDaniel, 2013).
Perhaps the biopsychosocial pathway model offers a potential explanation for the unexplained variation and endogeneity within this particular health measure. It suggests that cardiovascular illness in old age is a result of a ‘complex chain of risk’ comprised of biological, psychological, and social links (Hagger-Johnson et al., 2012). This model is an improvement over prior work (Borrell-Carrió et al., 2004) that could not explain the gradient relationship observed between SES and cardiovascular illness in the Whitehall study. Additionally, prior work lacked a clear explanation as to why adult SES, rather than childhood SES, seemed to have a larger impact on cardiovascular illness. Thus, this model provides a long overdue explanation behind the association of risk and socioeconomic level as it posits that all cardiovascular risk factors originate in childhood and build up to adulthood, each playing upon one another to form a cumulative aggregate of risk.
The interplay between biology and environment has recently received attention in the social science literature on physical well-being (McDade et al., 2011). Stressors stemming from families, work, and participation in other social institutions may affect overall health through the mechanism of health risk factors. For instance, smokers often increase intake of cigarettes while under stress (Taylor and Repetti, 1997). These social influences combine with psychological risk factors and work in conjunction with a person’s biology to generate overall health. Low SES is often associated with risk factors such as smoking, over-eating, and high blood pressure, but the reasons why low socioeconomic status is linked to such factors can be traced back to their biopsychosocial origins (Hagger-Johnson et al., 2012; Kanjilal et al., 2006). This perspective many seem reminiscent of early 1950s thought on personal responsibility for health vis-a-vis structural functionalism (Parsons, 1951). However, the biopsychosocial pathway model suggests that an individual’s agency in protecting their health is shaped by external forces that are very much tied to the financial, social, and cultural resources to which one has access based on socioeconomic status.
SES, health, and the lifecourse
While research has illustrated a tie between social factors, socioeconomic status, and health, it is important to explore the time component and SES in determining health outcomes. Knowing those times in a person’s life when socioeconomic status would have the highest impacts on their health could help in attenuating any poor health outcomes that might result. This type of inquiry is deeply rooted in the lifecourse perspective (Elder, 1975), which suggests that early and current life experiences dramatically affect physical health and well-being (Katz et al., 2012; Kuh and Ben-Shlomo, 2004). Within public health, the latency model is one important theoretical perspective that is complementary to the lifecourse perspective. It predicts that childhood SES is the main determinant of disease risk later in life, as opposed to adult SES (James et al., 2006). Barker’s (1992) early work argued that adverse socioeconomic experiences during childhood, even in utero, can create physiological changes to the body that enhance the risk of developing health conditions, such as cardiovascular disease, in adulthood. The latency model does not entirely disregard the influence of adult socioeconomic status, but insists that childhood is the principal origin of health behaviors (Conroy et al., 2010). This model reflects the essential ideas of the biopsychosocial pathway, but goes one step beyond to propose that childhood is where the chain of risk is initially forged. Also, it suggests that adulthood interventions cannot fully attenuate childhood experiences (Jeemon and Reddy, 2010).
While socioeconomic conditions experienced during childhood are potentially linked to adult and elderly health, it is impossible that these childhood socioeconomic effects are the sole determinants of later-life health. In fact, this argument seems to contradict many studies showing adult SES to be the chief predictor of cardiovascular illness (Pollitt et al., 2007; Strand and Kunst, 2007). The relationship between childhood socioeconomic status and health has, in fact, been found to be indirect through the socioeconomic achievement experienced in adulthood. Research on intragenerational mobility and stability suggests that childhood socioeconomic status is directly related to adult SES (Nolan and Erikson, 2007). Because of this tie, recent evidence has confirmed that mortality and other health outcomes experienced during adulthood are directly related to adulthood SES and only indirectly related to childhood SES (Hayward and Gorman, 2004).
Although childhood and adult SES are linked to later-life health, there is still much debate in the literature regarding which is the greater contributor to disease patterns and general health. The age-as-leveler hypothesis suggests that, across the lifecourse, health differences are wider during childhood but narrow at older ages. Thus, childhood SES is thought to be more important in predicting health than adult SES. House et al. (1990, 1994) provide some support for this hypothesis. They find that socioeconomic differences in health in later life reflect differences in exposure to education and income during childhood, but that these differences attenuate later in life. In addition, they find that the socioeconomic variation in risk factors associated with chronic diseases is large during middle age but small in old age. Combined, this research suggests that, due to mortality selection, socioeconomic differences in health appear to diminish later in life.
In contrast, the cumulative disadvantage hypothesis suggests that socioeconomic effects increase across the lifecourse. This hypothesis suggests that there is a tie between socioeconomic accumulation and health risk accrual. That is, higher SES translates to a lower number and severity of health risks. This relationship guides the health trajectory such that, at older ages, persons with lower SES are likely to be in worse health than individuals with higher SES. Because low SES accumulates from childhood to adulthood, it is likely that as time progresses, health precipitously declines. In this case, adulthood SES is more instrumental in shaping health later in life than childhood SES, since any socioeconomic differences in adulthood should account for differences in childhood SES. While cumulative disadvantage is applicable to many outcomes, including onset to criminal delinquency (Sampson and Laub, 1997) and educational attainment (Hannon, 2003), only a few studies support this claim in regard to health (Dupre, 2007). Because this theoretical debate still exists in the literature and because these western models have not been rigorously applied to the Latin American context, this project relies on the lifecourse perspective to assess the impact of childhood and adult SES on cardiovascular illness among the elderly population in several countries in the Latin American region.
Hypotheses
Based on the literature review and theoretical perspectives above, five hypotheses are examined:
H1: Better socioeconomic conditions experienced as a child will be negatively associated with the likelihood of developing hypertension and experiencing a heart attack.
H2: Better socioeconomic conditions experienced as an adult also will be negatively associated with the likelihood of developing hypertension and experiencing a heart attack.
H3: Controlling for socioeconomic disadvantage experienced in childhood is expected to explain away some of the effect that adult SES has on developing hypertension and experiencing a heart attack.
H4: Controlling for health behaviors will eliminate the effect that adult SES has on developing hypertension and experiencing a heart attack.
H5: We expect country-specific differences in the effects that SES measures will have on developing hypertension and experiencing a heart attack.
Data and methods
We rely on the Survey on Health Well-Being, and Aging in Latin America and the Caribbean (Project SABE). SABE provides a wealth of data regarding public health and aging in Latin America. The data were collected in seven Latin American and Caribbean cities (Pelaez et al., 2005). Data were collected between 1999 and 2000 in Buenos Aires, Argentina (N = 1039), São Paulo, Brazil (N = 2143), Santiago, Chile (N = 1301), and Montevideo, Uruguay (N = 1444) using face-to-face interviews in the respective official language of the cities. Because the questions were standardized, comparisons across countries are possible. Response rates varied from 60% (in Buenos Aries) to 85% (in São Paulo), with an average response rate of 74%.
The SABE study relied on a multistage, cluster sampling design. According to prior work using the data, ‘In each city, the primary sampling unit (PSU) was a cluster of independent households within predetermined geographic areas. The PSUs were grouped into either geographic or socioeconomic strata. The sample distribution by geographic or socioeconomic strata was determined by allocation proportional to the size of the elderly population in each city’ (Barceló et al., 2006: 226).
These data are ideal to study lifecourse socioeconomic disadvantage and health among the elderly. Individuals age 60 and older were interviewed for this study, and those individuals were asked both current and retrospective questions regarding their socioeconomic standing, as well as their current behavioral and lifestyle habits.
Dependent variable
Cardiovascular illness
We assess cardiovascular illness based on two self-reported variables. First, respondents were asked if they had ever been told by a medical professional that they had high blood pressure (or hypertension). Second, respondents were also asked if they had ever been told that they had a heart attack. Self-reported accounts of cardiovascular illness tend to be valid and reliable measures of actual cardiovascular illness in health surveillance data (Bowlin et al., 1996).
Independent variables
Childhood socioeconomic status
We assess childhood SES using three distinct measures. First, respondents were asked, ‘During the first 15 years of your life how was the economic situation of your family?’ Valid responses for this question are ‘excellent’, ‘fair’, and ‘poor’. We altered this variable to indicate whether the respondents were poor or non-poor during childhood. Second, as a proxy for food insecurity, individuals were asked if they were ever hungry during the first 15 years of their lives. Third, respondents were asked if they lived in a rural area during the first 15 years of their lives. Rural poverty is an important indicator of socioeconomic status. As the International Fund for Agricultural Development suggests, ‘[Rurality] is associated with lack of access to and unequal distribution of productive land, and inadequate access to information and productive assets for smallholder farmers’ (International Fund for Agricultural Development, 2013).
Adult socioeconomic status
We assess adult SES with four measures. The number of years of education for each respondent are collapsed into four categories consistent with past research (Palloni et al., 2002): illiterate (no formal education), primary (1–6 years), secondary (7–12 years), and post-secondary (above 12 years). Respondents’ longest held job is recorded according to the International Standard Classification of Occupations (Ganzeboom and Treiman, 1996), and are sorted into the three categories of white-collar, blue-collar, and unskilled workers. This categorization is based on prior work using this dataset (Nguyen et al., 2008) and has been argued as reliably capturing external heterogeneity between classes (Ganzeboom et al., 1992).
Income sufficiency is measured by whether or not respondents believed they had enough money to survive. We note that income could not be used because of the excessive number of missing cases (86.4%), so income sufficiency instead serves as a proxy for income. Purchasing power is an index measure. Respondents were asked if they owned several items (i.e., refrigerator, automatic clothes washer, water heater, microwave, television, telephone, VCR, music player such as a radio or CD player, air conditioning unit or fan). The total number of goods owned is summed to create this index. Higher values indicate a greater purchasing power.
Health and demographic controls
These measures are a collection of risk factors associated with cardiovascular illness. Childhood health is self-reported. Respondents were asked, ‘During the first 15 years of your life, would you say that your health was excellent, good or poor?’ We altered this variable to reflect whether respondents indicated they had poor or non-poor health during childhood. Smoking status is a dummy variable that indicates if the respondent currently smokes. Respondents were asked to choose the days per week they consumed alcohol for the last three months. Alcohol consumption is broken into three categories: none, 1–6 times a week, and daily. Physical activity is a dummy variable that indicates if the respondent has exercised or done rigorous activity three or more times per week within the last 12 months. Nourishment is assessed by a survey question that asks if respondents are well-nourished, i.e., if they have had at least three meals per day. While nourishment is associated with SES, it is also a distinct pathway to cardiovascular illness as malnourished individuals (such as those who are anorexic) are less likely to have vital nutrients such as thiamine and potassium. Thus they would be at an enhanced risk of developing cardiovascular illness (D’Elia et al., 2011). For health care access, a dummy variable is used to indicate whether or not respondents are currently insured.
A depression measure is used as a health control for this study, mainly because prior research suggests that ‘elevated depressive symptoms appear to be a robust risk and prognostic marker of cardiovascular disease … and that depression treatment may alter the course of cardiovascular disease’ (Davidson et al., 2005: S6). SABE study organizers used the Geriatric Depression Scale (Sheikh and Yesavage, 1986), which contains 15 items to assess the presence of depressive symptoms. Positive responses were summed, with higher scores indicating higher levels of depression.
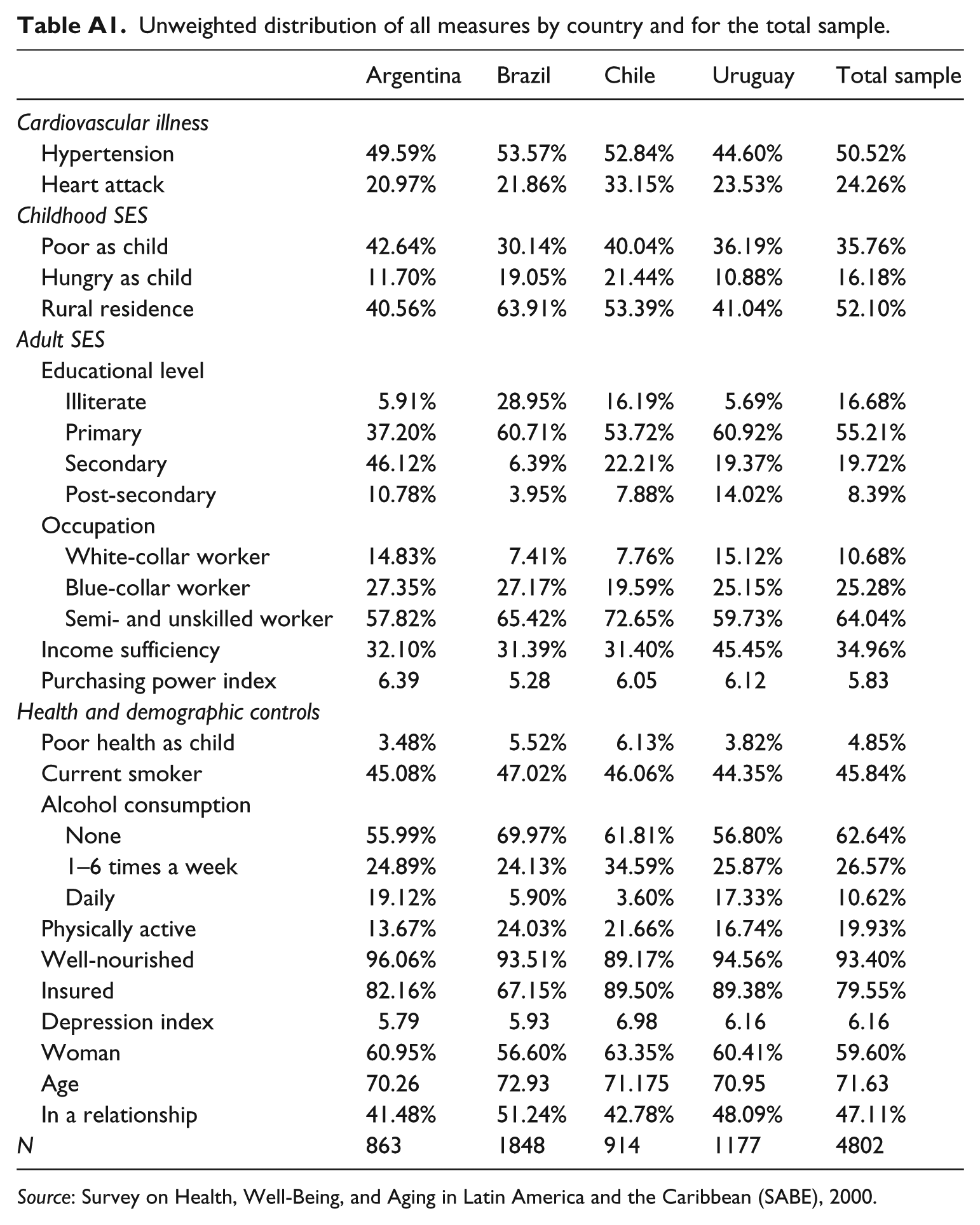
Gender, age, and marital status are all used as demographic controls. Age in the analyses is centered on the grand mean of the sample. A dummy variable is used indicating whether the respondent is in any kind of relationship (legal, civil, religious or free union). The Appendix provides the descriptive statistics and the unweighted distribution of all the measures used in the analyses for the total sample and by country. We note that ANOVAs were performed to test mean differences across all country types with all of the variables. Those ANOVA tests were significant at the .05 alpha level, suggesting that there are statistical differences across countries for all of the variables used in the analyses.
Analytic strategy
Logistic regression is used to explore how various SES, health, and demographic measures are related to cardiovascular illness. Model 1 tests the first hypothesis, as it includes childhood SES as predictor of cardiovascular illness. Model 2 tests the second hypothesis because it includes adult SES in the model. Subsequent models are cumulative. That is, Model 3 combines childhood and adult SES measures (testing the third hypothesis). To test the fourth hypothesis, Model 4 adds health and demographic information to the SES measures presented in the previous model. Because we expect country-level differences in how these measures model cardiovascular illness, we stratify the sample based on country and run the final model (i.e., Model 4) separately for respondents in Argentina, Brazil, Chile, and Uruguay. These models test our fifth hypothesis. In order to test for multicollinearity between the measures used, we calculated the variance inflation factors (VIFs). With a mean VIF of 1.18 and a range of 1.02–1.67, we find no collinearity issues with these measures since the VIFs are well below the value of 10 (DeMaris, 2004: 228). Stata 12.1 is used to analyze the data (StataCorp, 2011).
Results
Socioeconomic status and cardiovascular illness
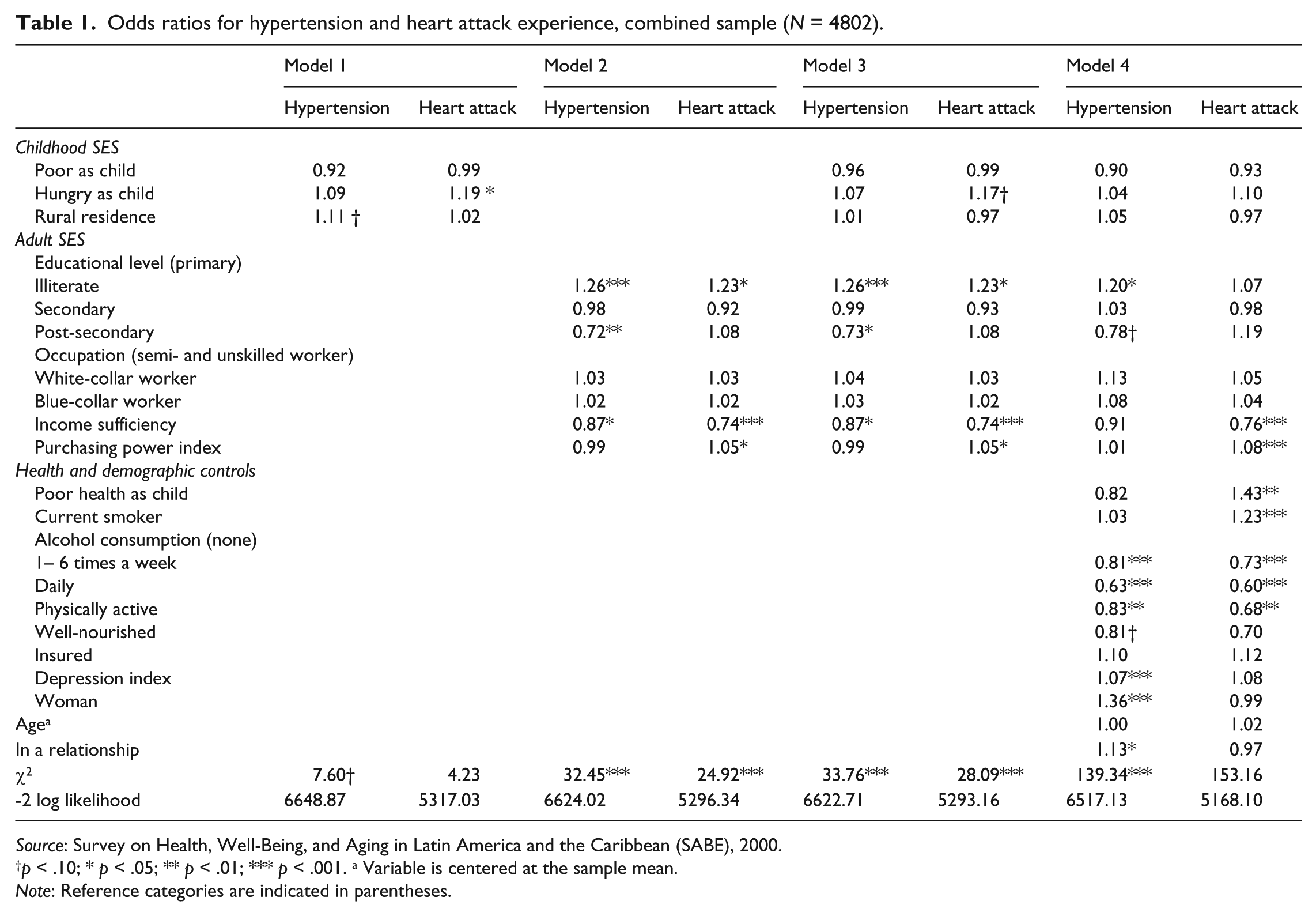
The results of the logistic analyses are presented in Table 1. For each model, the odds of being diagnosed with hypertension and having experienced a heart attack are presented separately. Model 1, which tests the first hypothesis, includes the retrospective childhood socioeconomic variables. In this model, adults who grew up in a rural area have 11% greater odds of being hypertensive than adults who did not grow up in a rural area. Also, adults who indicate they were hungry as children have 19% higher odds of experiencing a heart attack than those who grew up in food-secure households.
Odds ratios for hypertension and heart attack experience, combined sample (N = 4802).
Source: Survey on Health, Well-Being, and Aging in Latin America and the Caribbean (SABE), 2000.
p < .10; * p < .05; ** p < .01; *** p < .001. a Variable is centered at the sample mean.
Note: Reference categories are indicated in parentheses.
Model 2, which tests the second hypothesis, includes current adult socioeconomic variables. For both cardiovascular outcomes, educational level is significantly associated with cardiovascular illness. Compared to having a primary level of education, illiterate individuals have 26% greater odds of being hypertensive and 23% great odds of experiencing a heart attack. Conversely, respondents with post-secondary educations have 28% lower odds of being hypertensive compared to those with a primary education.
Income sufficiency, or having enough money to live, is associated with a 13% reduction in the odds of being hypertensive and a 26% reduction in the odds of experiencing a heart attack. Lastly, purchasing power is significantly related to experiencing a heart attack but not for being hypertensive. The greater number of goods a person owns corresponds to a 5% increase in the odds of experiencing a heart attack.
Model 3, which tests the third hypothesis, builds on Model 2 by adding both childhood and adult socioeconomic status variables into the same model. Results indicate that adult SES effects seen in Model 2 maintain their statistical significance. However, one childhood SES measure loses its significance with the addition of adult SES measures. Namely, rural residence ceases to be predictive of being hypertensive after controlling for adult SES. Supplemental mediation analyses (i.e., Sobel tests) indicate that the addition of education helps explain this change in statistical significance across models. Specifically, when education is added to the model, the effect of rural residence disappears.
Model 4, the full model, includes the socioeconomic measures from the previous model as well as the health and demographic control variables. These control variables attenuate the socioeconomic effects seen in the previous model such that none of the childhood SES measures are significant for either dependent variable and the only significant adult SES predictors are income sufficiency and the power purchasing index, and these only for experiencing a heart attack.
Model 4 also indicates that many control variables are significant predictors of hypertension or experiencing a heart attack. Having poor health as a child is associated with 43% higher odds of experiencing a heart attack when compared to having good or excellent health. Current smokers have 23% greater odds of experiencing a heart attack compared to individuals not currently smoking. Compared to not drinking alcohol, drinking alcohol between 1 and 6 days a week is associated with 19% lower risk of being hypertensive and a 27% lower risk of experiencing a heart attack. Likewise, drinking alcohol daily corresponds to 37% lower odds of being hypertensive and 40% lower odds of experiencing a heart attack. Physical activity is associated with decreased odds of both being hypertensive (17%) and experiencing a heart attack (32%). Being well-nourished is associated with a 19% reduction in the odds of being hypertensive and a 30% reduction in the odds of experiencing a heart attack. The depression scale is also statistically related to both cardiovascular outcomes. A one point increase on the depression scale (i.e., being more depressed) corresponds to a 7% increase in the odds of being hypertensive and an 8% increase in the odds of experiencing a heart attack. Women are 36% more likely than men to have been diagnosed with hypertension. Each additional year of age is associated with a 2% increase in having a heart attack starting at 70. Lastly, individuals in a relationship are 13% more likely to be diagnosed with hypertension compared to those not in any kind of union.
Auxiliary analyses for mediation using Sobel tests indicate that the addition of age and having poor health as a child explain the reduction in significance levels for SES measures from Models 3 to 4. Thus, although many of the control variables discussed above were significant predictors, they could also be mediating the relationship between the earlier introduced SES measures and the outcomes of hypertension and heart attack. Consequently, SES remains important since it affects the health behaviors that were introduced in Model 4.
Country-specific analyses of socioeconomic status and cardiovascular illness
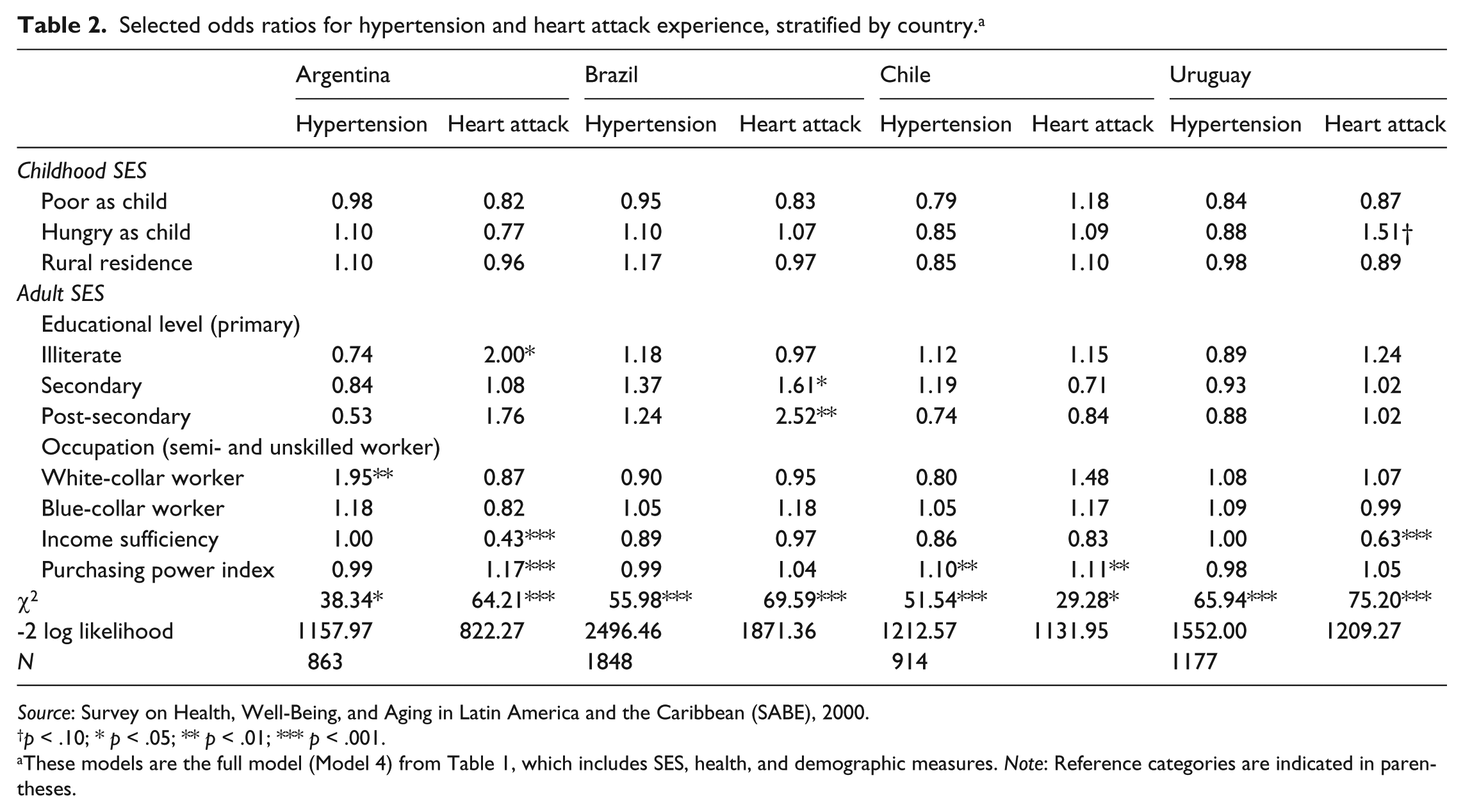
Table 2 tests the final hypothesis by exploring country-specific differences in socioeconomic effects on hypertension and experiencing a heart attack. This table presents the odds ratios for socioeconomic status measures for each dependent measure separately for all four Latin America nations. It is important to note that a model which includes dummy variables for the four sites was run, and there was statistical significance at the .05 alpha level, indicating that net of other covariates there are specific differences in the effect of country on cardiovascular illness. Auxiliary analyses also examined interaction terms between SES measures and country. These analyses and a global chi-square test indicate that there were significant differences in the effect that SES has on cardiovascular illness depending on the country in which respondents live (p < .05). Based on this information, we performed stratified analyses to see which socioeconomic effects correspond to each particular site. In this stratified analysis, each country has a full model (corresponding to Model 4 from Table 1). However, only the SES measures are displayed for ease of interpretation.
Selected odds ratios for hypertension and heart attack experience, stratified by country. a
Source: Survey on Health, Well-Being, and Aging in Latin America and the Caribbean (SABE), 2000.
p < .10; * p < .05; ** p < .01; *** p < .001.
These models are the full model (Model 4) from Table 1, which includes SES, health, and demographic measures. Note: Reference categories are indicated in parentheses.
Although childhood SES was not statistically significant in predicting cardiovascular illness in the full sample, one measure was marginally significant in the case of Uruguay. That is, being hungry as a child is associated with 51% higher odds of experiencing a heart attack compared to those not food-insecure during childhood.
Education is statistically significant in both Argentina and Brazil. In Argentina, being illiterate is associated with 100% higher odds of experiencing a heart attack, compared to having a primary level of education. In Brazil, higher levels of education are associated with a higher risk of experiencing a heart attack. Specifically, individuals in Brazil with a secondary education have 61% higher odds of having a heart attack and individuals with post-secondary education have 152% higher odds of experiencing a heart attack.
While occupation SES was not statistically significant in predicting cardiovascular illness in the full sample, it is significant in the Argentinian sample. White-collar workers are associated with 95% greater odds of being hypertensive compared to semi- or unskilled workers. Income sufficiency is statistically associated with experiencing a heart attack in Argentina and Uruguay. Specifically, having enough money to survive is associated with 57% lower odds of having a heart attack for respondents from Argentina and 37% lower odds among the Uruguay sample. Lastly, purchasing power is positively related to cardiovascular illness in the Argentina and Chile samples. In Argentina, each additional material purchase is associated with 17% higher odds of experiencing a heart attack. In Chile, each item purchased in the home is associated with 10% higher odds of being hypertensive and 11% higher odds of experiencing a heart attack.
Discussion
This research employed innovative data from Latin America to assess how childhood and adult socioeconomic status affected two self-reported cardiovascular outcomes: hypertension diagnosis and heart attack experience. This topic is important because social, economic, and health progress is still relatively stagnant in the region (Hall and Patrinos, 2005). Three main hypotheses were tested in this research. First, this research tested the relationship between socioeconomic disadvantage and cardiovascular illness. Regression results indicated that both childhood and adult socioeconomic status independently played major roles in understanding cardiovascular illness. For example, food insecurity during childhood (i.e., being hungry as a child) was found to be a significant predictor of a heart attack, while living in a rural area as a child was a significant predictor of being hypertensive. These results are consistent with earlier studies (e.g.,Vozoris and Tarasuk, 2003) that also found a relationship between food insecurity and heart disease, and that rural locations are often associated with poor health infrastructure, geographical isolation, risk-taking behaviors, and lack of extensive social support (Dixon and Welch, 2001).
Moreover, education and measures of income (i.e., income sufficiency and purchasing power) in adulthood were found to be associated with cardiovascular illness. Education and income have long been established as important predictors of general health as well as heart health (Smith, 2004). Interestingly, purchasing power was found to enhance cardiovascular illness. Research indicates that the quest for material possessions could be a risk factor for heart disease because it normally entails working long hours, little work–life balance, safety compromises, and exposure to intense stress (Iwasaki et al., 2006).
Adult SES measures, most notably education, were found to offset most of the effects that childhood SES had on cardiovascular health. In low-, middle-, and high-income countries, post-secondary education is a mechanism for escaping poverty. This is particularly true for Latin America, since the region has the unique challenge of investing in quality education for children while simultaneously dealing with widespread poverty (Hall and Patrinos, 2005). It is also important to consider that selectivity could be occurring, as those children who are healthy and non-poor are much more likely to be able to attain post-secondary education (Van de Mheen et al., 1998a) than their less fortunate peers.
We also hypothesized that SES effects could be explained by health and demographic measures, which was partially the case. Childhood SES effects were completely explained with age and childhood health, suggesting a more complicated trajectory where various health measures mediate the relationship between SES and hypertension and heart attacks.
The health controls, which are risk factors for cardiovascular illness, were also significantly related to cardiovascular illness. Consistent with medical literature, most of the unhealthy behaviors were risk factors for cardiovascular illness. However, alcohol consumption results were somewhat counterintuitive as more alcohol consumption lowered the risk of a cardiac event. While some evidence exists that limited alcoholic consumption is beneficial to heart health (Marmot and Brunner, 1991) and moderate alcohol consumption is beneficial as one advances in age (Thun et al., 1997), it is unclear how daily alcohol consumption is protective against cardiovascular health. Recent medical research suggests that flavonoids in red wine are related to cholesterol and blood clotting reductions (Mudry, 2010). However, we do not know if daily alcohol consumption includes red wine. More research should be done to explore this finding in these and other societies to see if this relationship holds. To this point, our results provide support for many of the theories earlier reviewed, but especially the theory of fundamental causes, the social gradient of health, and the lifecourse perspective.
The fifth hypothesis assessed the country-specific effects of socioeconomic status on cardiovascular illness. Results revealed distinct patterns as some socioeconomic indicators were predictive of hypertension and experiencing a heart attack in some sites but not others. In Argentina, no education and insufficient income were risk factors for cardiovascular illness, but ironically, so was white-collar worker status and high purchasing power. Within the past two decades, white-collar workers in Argentina were hit with shrinking wages and increased productivity, particularly men (Arias, 2001). These kinds of changes brought about by economic restructuring may lead to stressful situations that could affect cardiovascular risk. Likewise, having various material items in the home could be a function of this productivity increase, which could be the type of job-related stress that increases the risk of high blood pressure and heart attacks.
In Brazil, only education was predictive of cardiovascular illness, specifically experiencing a heart attack. However, more education was associated with an increased risk. Only a few studies have corroborated this counterintuitive finding in the Brazilian context (Barreto et al., 2001; Duncan et al., 1993). Brazil’s relatively recent transformation to an industrialized nation-state has led to high levels of inequality (Wilkinson and Pickett, 2009). While risk factors for major non-communicable diseases are highly concentrated among the poor, job-related stress, brought upon by highly-credentialed occupations, is still one major risk factor for cardiovascular illness that could help explain this finding in Brazil.
In Chile, the only socioeconomic indicator that significantly captured cardiovascular illness was purchasing power. According to recent research, living standards in Chile have significantly increased across the country over the past century, with more far-reaching gains occurring since the 1950s (Astorga et al., 2005). However, similar to the cases of Argentina and Brazil, this kind of development has led to mass and conspicuous consumption among the socioeconomic elite. As a result, the stresses of demonstrating socioeconomic and cultural capital may help explain this increased cardiovascular illness.
In Uruguay, both the childhood SES indicator of food insecurity and the adult SES indicator of income sufficiency were associated with cardiovascular illness. These two results are intuitive. Food insecurity is a proxy for childhood poverty, which other research has linked with cardiovascular illness. Likewise, not having enough funds to survive is a proxy for adult poverty, which is also associated with heightened cardiovascular illness. These country-specific findings highlight the diversity in effects that SES plays in determining hypertension and heart attack experience. This research suggests that policies that attempts to curve poverty in ways that deal with elevating health in these nations are well-grounded and necessary. However, also needed are health literacy programs and other ways to limit the adoption of a high-calorie, low-activity lifestyle. Such policies could benefit both the poor and affluent. The contrasting results from the various locations reviewed provide support for the notion of a biopsychosocial pathway model and its suggestion that cardiovascular illness is a result of a ‘complex chain of risk’ comprised of biological, psychological, and social links which typically will vary from place to place.
This study is not without its limitations. Socioeconomic indicators were asked retrospectively. It would have been useful to have longitudinal, prospective information on socioeconomic circumstances during childhood, since retrospective data may be biased. With cross-sectional data, it is nearly impossible to disentangle the causal ordering of events. This research presented associations between certain processes (e.g., SES) and health. A longitudinal study would illuminate how direct associations (or the causal ordering of events) impact health. Because this study is cross-sectional, it is possible that the inferences drawn about SES and health are contingent on the cohort analyzed. While the occupation measure used in this research captures external heterogeneity between classes, it is also likely that it does not capture internal heterogeneity among classes. That is, classifying occupations as white-collar, blue-collar or unskilled fails to capture variability between occupations within the classification. This point is critical since the life chances of different occupations within the same class could be dissimilar.
In addition, the dependent measures are self-reported and not based on medical examination records. Individuals must have an option to see a medical professional in order to be told if they have any cardiovascular illnesses. Thus, there could be some endogeneity between the health measures and the SES measures used, as access to medical care, particularly for this region, is strongly tied to a person’s level of access to financial and social resources.
Limitations aside, this research possesses many strengths. The unique data examined helped extend our current understanding of SES and cardiovascular health in the Latin American region, an understudied area in terms of these increasingly important concepts. Moreover, the statistical power of this research allowed us to conduct cross-country comparisons of SES and cardiovascular health to showcase how SES matters differently in distinct contexts. Future studies should expand upon this research to compare and contrast findings from Latin America to other global regions to better understand how contexts matter in determining the ways in which SES influences different health outcomes.
Footnotes
Appendix
Unweighted distribution of all measures by country and for the total sample.
| Argentina | Brazil | Chile | Uruguay | Total sample | |
|---|---|---|---|---|---|
| Cardiovascular illness | |||||
| Hypertension | 49.59% | 53.57% | 52.84% | 44.60% | 50.52% |
| Heart attack | 20.97% | 21.86% | 33.15% | 23.53% | 24.26% |
| Childhood SES | |||||
| Poor as child | 42.64% | 30.14% | 40.04% | 36.19% | 35.76% |
| Hungry as child | 11.70% | 19.05% | 21.44% | 10.88% | 16.18% |
| Rural residence | 40.56% | 63.91% | 53.39% | 41.04% | 52.10% |
| Adult SES | |||||
| Educational level | |||||
| Illiterate | 5.91% | 28.95% | 16.19% | 5.69% | 16.68% |
| Primary | 37.20% | 60.71% | 53.72% | 60.92% | 55.21% |
| Secondary | 46.12% | 6.39% | 22.21% | 19.37% | 19.72% |
| Post-secondary | 10.78% | 3.95% | 7.88% | 14.02% | 8.39% |
| Occupation | |||||
| White-collar worker | 14.83% | 7.41% | 7.76% | 15.12% | 10.68% |
| Blue-collar worker | 27.35% | 27.17% | 19.59% | 25.15% | 25.28% |
| Semi- and unskilled worker | 57.82% | 65.42% | 72.65% | 59.73% | 64.04% |
| Income sufficiency | 32.10% | 31.39% | 31.40% | 45.45% | 34.96% |
| Purchasing power index | 6.39 | 5.28 | 6.05 | 6.12 | 5.83 |
| Health and demographic controls | |||||
| Poor health as child | 3.48% | 5.52% | 6.13% | 3.82% | 4.85% |
| Current smoker | 45.08% | 47.02% | 46.06% | 44.35% | 45.84% |
| Alcohol consumption | |||||
| None | 55.99% | 69.97% | 61.81% | 56.80% | 62.64% |
| 1–6 times a week | 24.89% | 24.13% | 34.59% | 25.87% | 26.57% |
| Daily | 19.12% | 5.90% | 3.60% | 17.33% | 10.62% |
| Physically active | 13.67% | 24.03% | 21.66% | 16.74% | 19.93% |
| Well-nourished | 96.06% | 93.51% | 89.17% | 94.56% | 93.40% |
| Insured | 82.16% | 67.15% | 89.50% | 89.38% | 79.55% |
| Depression index | 5.79 | 5.93 | 6.98 | 6.16 | 6.16 |
| Woman | 60.95% | 56.60% | 63.35% | 60.41% | 59.60% |
| Age | 70.26 | 72.93 | 71.175 | 70.95 | 71.63 |
| In a relationship | 41.48% | 51.24% | 42.78% | 48.09% | 47.11% |
| N | 863 | 1848 | 914 | 1177 | 4802 |
Source: Survey on Health, Well-Being, and Aging in Latin America and the Caribbean (SABE), 2000.
Acknowledgements
A previous version of this article was presented at the 2009 International Union for the Scientific Study of Population (IUSSP) meeting in Marrakesh, Morocco. The authors would like to thank Margarita Alegría, Benjamin Cook, Ivy Ken, and four anonymous reviewers for helpful comments.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.