
Abstract
Objective:
The aim of this study was to estimate the finger-tapping rates and finger load capacities of eight fingers (excluding thumbs) for a healthy adult population and investigate the effects of various factors on tapping rate.
Background:
Finger-tapping rate, the total number of finger taps per unit of time, can be used as a design parameter of various products and also as a psychomotor test for evaluating patients with neurologic problems.
Method:
A 1-min tapping task was performed by 148 participants with maximum volitional tempo for each of eight fingers. For each of the tapping tasks, the participant with the corresponding finger tapped the associated key in the standard position on the home row of a conventional keyboard for touch typing.
Results:
The index and middle fingers were the fastest fingers for both hands, and little fingers the slowest. All dominant-hand fingers, except little finger, had higher tapping rates than the fastest finger of the nondominant hand. Tapping rate decreased with age and smokers tapped faster than nonsmokers. Tapping duration and exercise had also significant effect on tapping rate.
Conclusion:
Normative data of tapping rates and load capacities of eight fingers were estimated for the adult population. In designs of psychomotor tests that require the use of tapping rate or finger load capacity data, the effects of finger, age, smoking, and tapping duration need to be taken into account.
Application:
The findings can be used for ergonomic designs requiring finger-tapping capacity and also as a reference in psychomotor tests.
Introduction
Finger-tapping rate is the total number of finger taps in a specified period of time. Generally, it is measured as the number of taps of the index finger in 10 s (e.g., Schmidt, Oliveira, Krahe, & Filgueiras, 2000; Cousins, Corrow, Finn, & Salamone, 1998). Finger-tapping tests have been used for assessing the motor abilities for more than a century (Jobbagy, Harcos, Karoly, & Fazekas, 2005). It has been used to evaluate the integrity of the neuromuscular system and assess motor control and manual dexterity.
Researchers mainly used finger-tapping tests for quantification of neurologic problems, such as Parkinson’s disease, schizophrenia, Alzheimer’s disease, and so on. Ott, Ellias, and Lannon (1995) used this method for quantification of Alzheimer’s disease; Dodrill and Troupin (1975) for epilepsy; Wing, Keele, and Margolin (1984) for Parkinson’s disease; Notermans, van Dijk, van der Graaf, van Gijn, and Wokke (1994) for ataxia; and so on.
In the field of ergonomics, matching the task demands to the capabilities of the workers is the main principle of ergonomic work design. In this context, the design requiring tapping capacity should distribute the task loads to the fingers according to the finger capacities. In alignment with that goal, a number of researchers (e.g., Dvorak, Merrick, Dealey, & Ford, 1936; Eggers, Feillet, Kehl, Wagner, & Yannou, 2003; Yin & Su, 2011) used the tapping-rate capacity of fingers for the optimization of keyboard layout designs. These researchers attempted to distribute the total load (i.e., the total number of key presses) to the fingers based on the finger-tapping rate capacity. For instance, in their keyboard layout, Dvorak et al. (1936) proposed to assign 14% of typing load to the fastest finger (the right index finger) and 10% to the slowest finger (the left little finger). They assigned the finger loads based on the results of a study by Riemer (1929, as cited in Dvorak et al., 1936). Tapping-rate capacity of fingers may also potentially be used in the designs of some musical devices, tools, and machines that require high rates of finger tapping.
Finger-tapping rate is affected by a number of factors. There are studies that were designed to identify these effects, with some shortcomings. For instance, Cousins et al. (1998) studied the effects of age (two groups only: 17–22 years and 57–88 years) and found that, on average, older participants perform fewer total finger taps than younger participants.
Silver et al. (2002) studied the effects of smoking on index finger–tapping rate of schizophrenic patients and found that smoking is associated with faster central processing. Perkins et al. (1990) and Roth and Batting (1991) also found that nicotine administration can increase finger-tapping rate in normal smokers. West and Jarvis (1986) investigated the effect of nicotine intake in nonsmokers and again concluded that nicotine can substantially improve performance of nonsmokers on a simple motor task. However, the mechanism by which nicotine improves central processing is unknown (Silver et al., 2002).
Jackson (1953) studied the tapping rates of four fingers of the right hand of 10 males and 10 females for a duration of 10 s and found that tapping rates of index and middle fingers were not significantly different; however, tapping rates for the ring and little fingers were significantly lower than of those two.
Schmidt et al. (2000) investigated the effects of gender and hand preference on index finger–tapping rate and found that men perform faster and have a lower intertap variability than women. They explained this phenomenon with the effects of male hormones (testosterone) on muscles. They also concluded that hand preference does not have a significant effect on overall tapping rate. However, in the same study, they found that manual asymmetry (difference in tapping rate) between left and right hands is smaller in left-handed participants.
In their study, Aoki and Kinoshita (2001), using 11 right-hand-dominant male participants (18–32 years), recorded right-hand single finger (index and middle fingers only), double finger (index and middle fingers only), and hand tapping (using middle finger only) rate capacity with a tapping duration of 7 s. One of the results indicated that the index finger had a significantly faster tapping frequency than the middle finger.
In another study, Aoki, Francis, and Kinoshita (2003), with a sample of 12 healthy male subjects, investigated the dynamic motor ability of individual fingers under four different finger-tapping conditions (single-finger tapping, double-finger tapping, double-finger tapping in an unsupported condition, and submaximal constant-speed tapping with one finger in a passive manner). According to one of the results of the study, the index finger attained the fastest cadence and greatest movement velocity, followed by the middle, little, and ring fingers, respectively.
A review of the literature revealed that most of the studies were limited to the tapping rate of index finger of the right hand (Table 1). And only a few studies considered tapping rates of index and middle fingers of the dominant hand. The studies were based on relatively small samples that did not include all age groups. Overall, the following shortcomings were identified: (a) There were no studies on determining the tapping rates of all eight fingers, (2) the effects of tapping duration and regular exercise on tapping rate were not investigated, and (3) the effect of age on tapping rate was not investigated for all age groups.
Summary Data of Tapping-Rate Studies
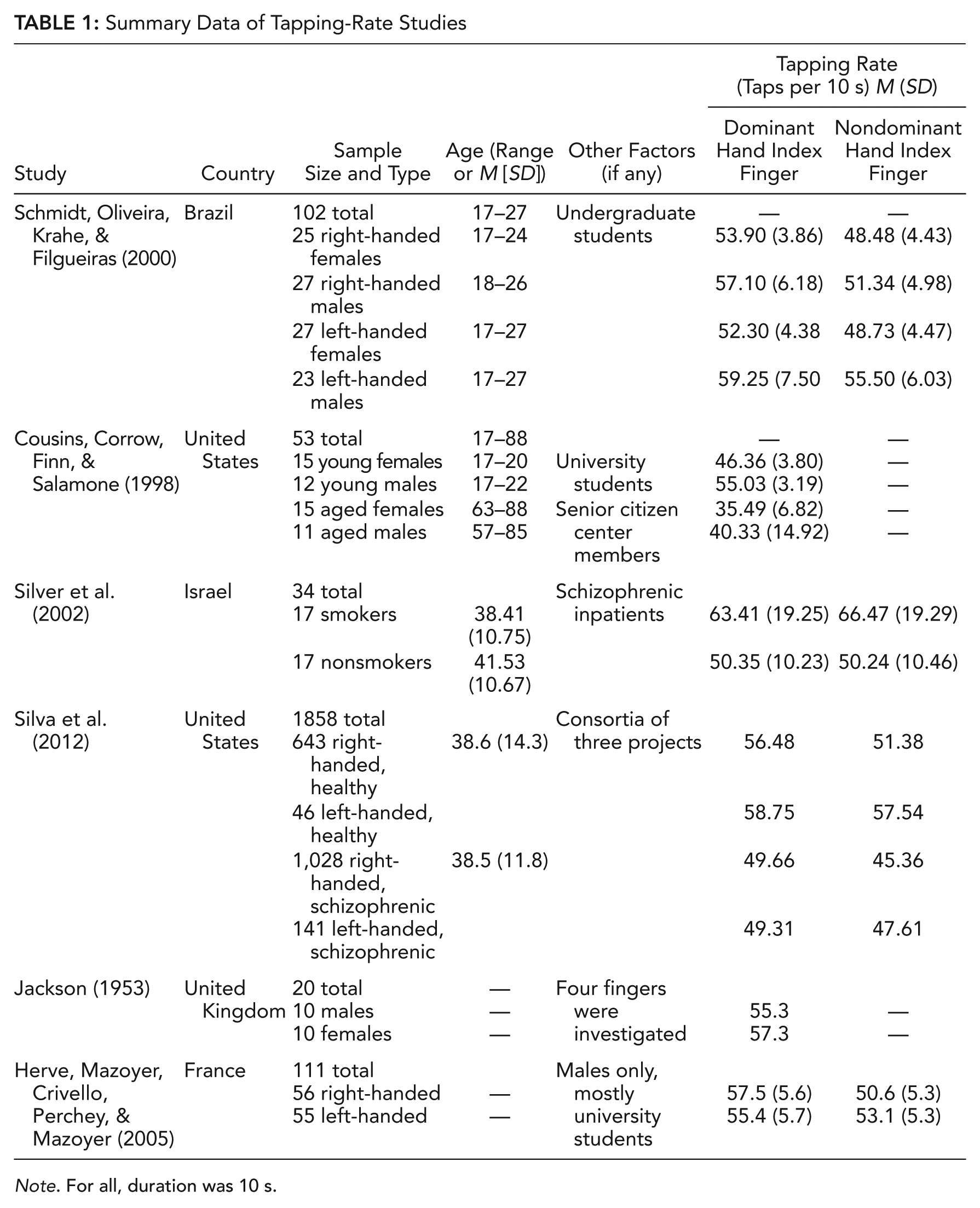
Note. For all, duration was 10 s.
Research Objectives
For an answer to the aforementioned shortcomings, this study had three primary objectives: (a) estimating the finger-tapping rates across finger, gender, hand preference, and age factors; (b) determining the effects of the independent factors (finger, gender, tapping duration, hand preference, age, smoking, and exercise) on the response variable (finger tapping rate); and (c) determining the finger load capacities of all eight fingers (excluding thumbs) based on the tapping rates to be used in ergonomic designs and as a reference for psychomotor tests. This objective includes the estimation of the load capacities separately for the right-handed, left-handed, and whole population.
The secondary objectives of the study were (d) to investigate the strength of linear association between tapping rate and several characteristics of the participants (age, hand length, hand breadth, and middle finger length) and (e) to assess the subjective ratings of the perceived exertion for all the eight fingers after 1 min of tapping task.
Method
Participants
The sample of participants included a total of 148 healthy voluntary adults (71 male and 77 female) with a wide range of age spectrum (18 to 85 years). A self-reported survey tool was administered to determine the health status of the participants. All the participants were in good health both physically and mentally and had no records of upper-extremity, neck, or shoulder disorders or pain. The participants signed an informed consent form after a full explanation about the study procedures prior to the experiments. This study was approved by the Institutional Review Board for Research With Human Subjects at Boğaziçi University.
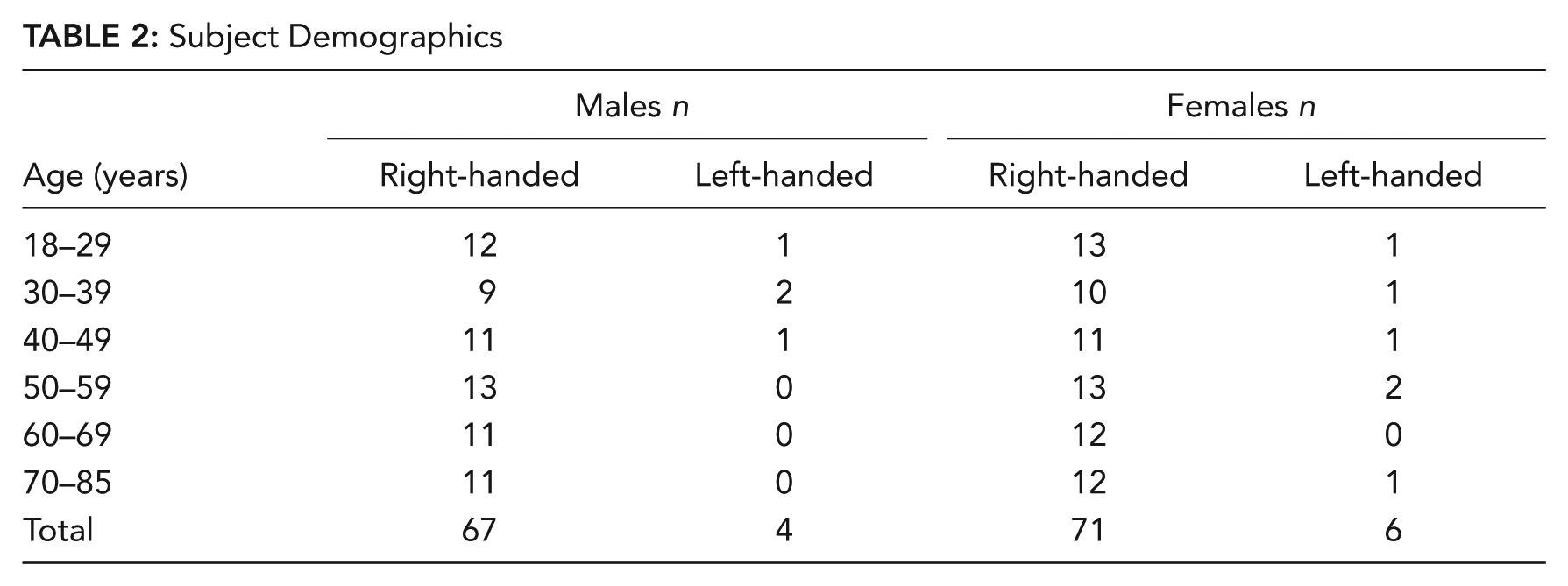
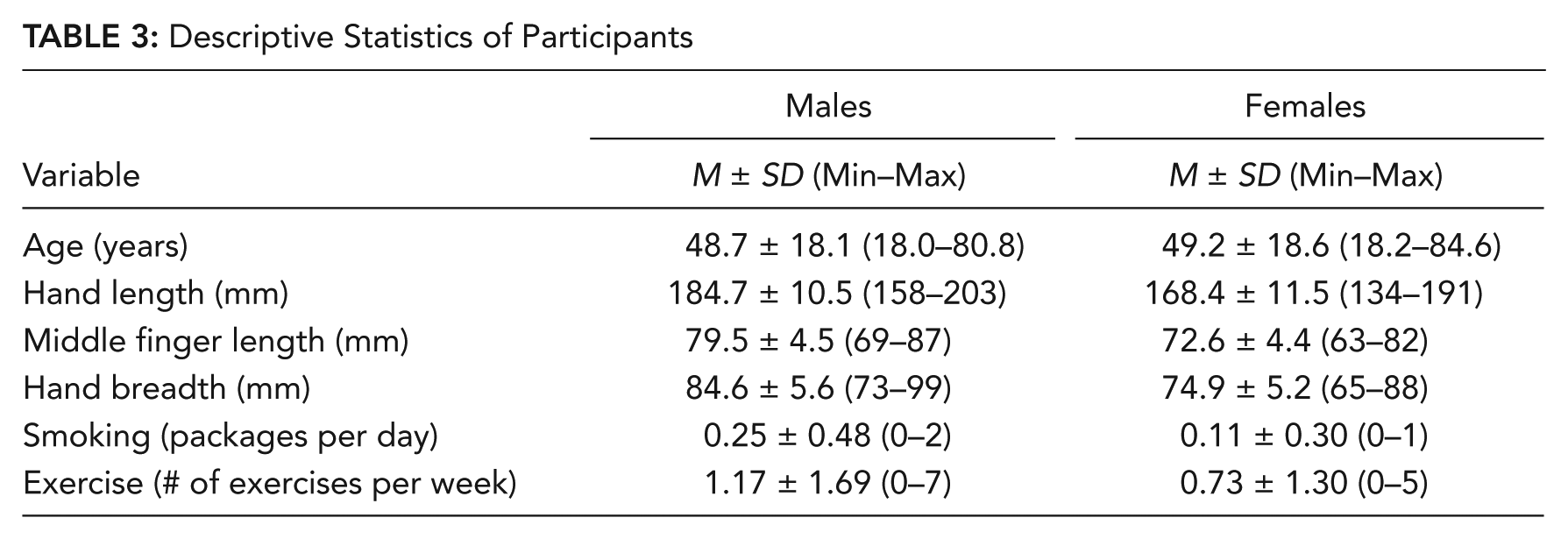
A stratified random sampling approach was used in order to include the participants within the considered age groups and both genders. Age range of the participants was divided by 10-year intervals, and a uniform distribution was attempted as much as possible for both gender and all age groups. The proportion of the left-handed participants in the sample was not more than the actual proportion in the population, which is about 7% to 10% (Table 2). The data of some characteristics of the participants were also collected (Table 3).
Subject Demographics
Descriptive Statistics of Participants
Study Protocol
Prior to the experiments, the data of the characteristics of the participants such as date of birth, gender, dominant hand, daily cigarette usage, weekly exercise rate, and occupation were recorded, and several hand anthropometric measures (hand length and breadth, middle finger length) were taken. A short explanation regarding the task and experimental procedure was given to each participant. Then, each participant practiced the tapping task until he or she felt comfortable to perform the actual tests.
The experimental task consisted of 1-min maximum volitional tapping with each of eight fingers (excluding thumbs). For each of the tapping tasks, the participant, using the corresponding finger, tapped the key in the standard position on the home row of a conventional keyboard for touch typing (Figure 1). For instance, for left little finger, the participant typed on key A (on standard QWERTY layout) repetitively with his or her maximum voluntary tempo for 1 min. Immediately after 1 min tapping for every finger, the participant was asked for his or her subjective rating about the fatigue in the associated finger according to Borg’s 10-point scale of ratings of perceived exertion (Borg, 1998). The participant was seated in neutral sitting posture with keyboard at about elbow height while the thumb and bottom part of palm were supported and forearm unsupported.
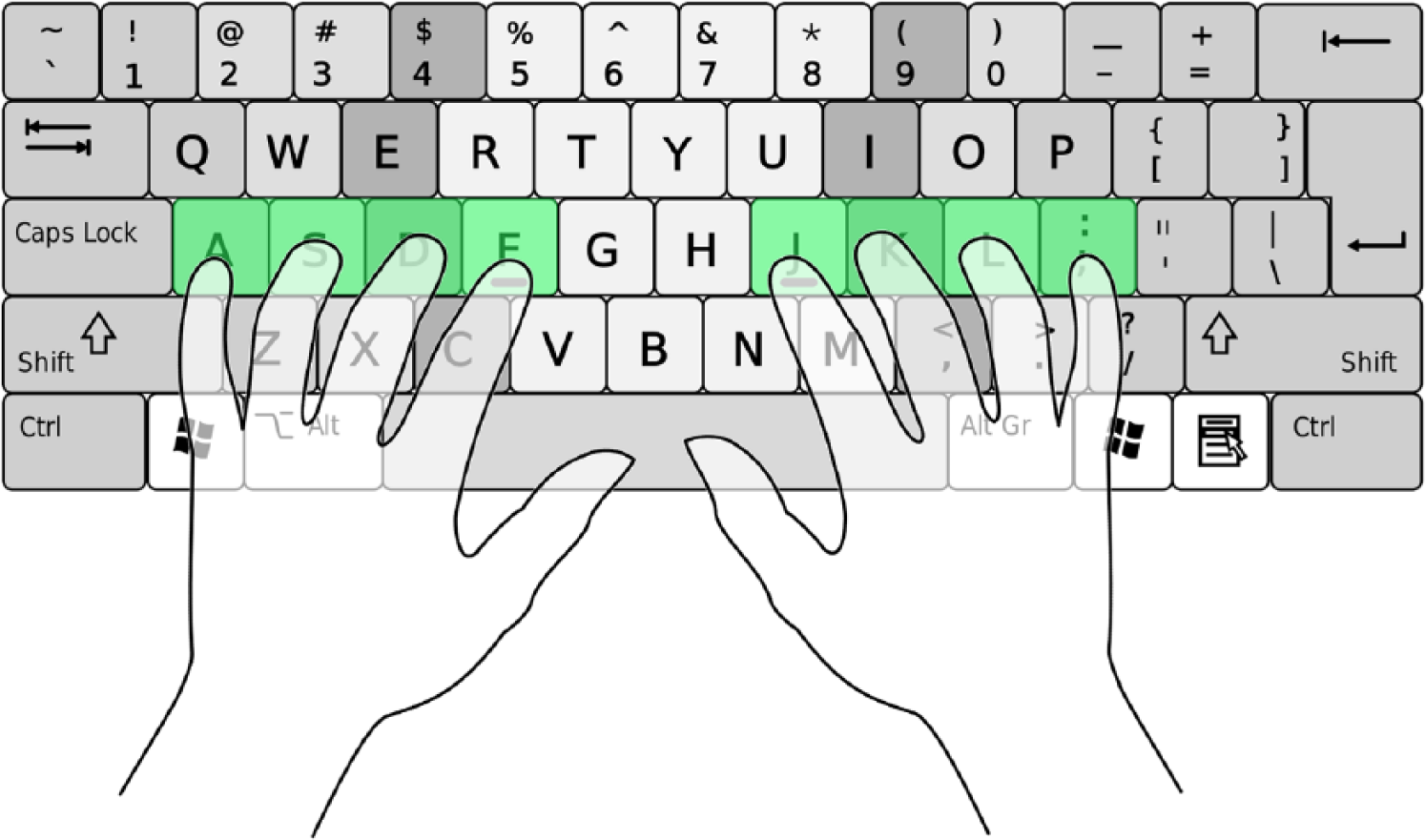
Standard positions of the fingers on a conventional QWERTY keyboard for touch typing.
The tapping duration of 1 min per finger was determined based on the results of the pilot study performed prior to the actual study. The pilot study indicated that the tapping rate does not change significantly after 30-s duration for a 2-min tapping task.
Experiments were carried out with all eight fingers except thumbs. The order of the eight fingers was randomized for each participant to reduce experimental error. Between the two consecutive test sessions, there was a 30-s rest period for recovering from the fatigue. Moreover, the same-hand fingers were not tested consecutively; instead, the finger of one hand followed the finger of the other hand to further minimize the fatigue effect. That is, a rest period of at least 2 min was provided between the testing of the fingers of the same hand.
A notebook computer was used as the test device, and the same notebook was used for all the participants. A computer program written in MatLab 7.11 (R2010b) is used to count and record the number of taps every 5 s of 1 min. There was no feedback to the participants about their performance during the tests, but they were instructed and encouraged to perform tapping as fast as possible and with the same effort each time.
One week after the completion of the actual experiment, a repeatability study was performed with randomly selected 20 subjects among the participants who performed the actual tests. The randomization was done in a stratified manner: 10 male and 10 female participants were selected randomly with one participant from each age group. The results did not seem to differ significantly (p > .1).
Statistical Method
The study investigated the finger-tapping rates of eight fingers and the effects of a number of independent variables on the tapping rate (the dependent variable). The tapping rate was defined as the number of keystrokes in every 5-s period of 60 s. That is, each of 1 min experiments was divided into 5-s periods (a total of 12 periods in 60 s) to investigate the variation in the response from the first period to the last. The independent variables were age group (6 levels), gender, finger (8 levels), period (12 levels), hand preference, smoking (smoker or nonsmoker), and exercise (regular exercise or not).
To accomplish the first objective, descriptive statistics (mean, standard deviation, and box plots) of the finger-tapping rate were performed.
To accomplish the second objective, an analysis of variance (ANOVA) was used after verifying the underlying assumptions (normality, equal variance, and independency). In this analysis, the fingers were categorized as dominant- and nondominant-hand fingers rather than left- and right-hand fingers. When the ANOVA indicated significant effect for an independent variable, comparisons across the multiple variable levels were tested using a post hoc Tukey’s test.
To accomplish the third objective of the study, the obtained tapping-rate data were transformed into a more useful form by normalization, which were called finger load capacities (FLCs). The FLCs are nothing but the relative values of the tapping rates. The normalization was performed because most of the time, designers consider the relative values of capacity instead of the absolute values when designing for humans. The normalization was performed as follows: FLC of the finger = (Main effect of the finger / Sum of the main effects of all the eight fingers) * 100. The main effect values were obtained from the ANOVA that was performed for the purpose. In this ANOVA model, the participants were set as block factor (since other independent factors of the previous ANOVA—such as age, gender, smoking, exercise, and hand preference—were characteristics of the subjects, they were embedded in this block factor) and period and finger as factors. This new model was used since it had a higher Radj2 value as a result of the blocking of the participants factor and enabled us to estimate the load capacities of fingers more precisely. Response variable was the same as before: the tapping rate in 5 s. In this model, to estimate the FLC values separately for the right-handed, left-handed, and whole population, unlike the previous statistical analysis, finger factor was taken as right-hand and left-hand fingers, considering that the design for finger tapping may involve the use of both left and right hands. In estimation of these parameters, three analyses were made: the first for the whole sample (7% left-handed and 93% right-handed), the second solely for the right-handed participants, and the third solely for the left-handed participants.
To accomplish the first of the secondary objectives of the study, a correlation analysis (Pearson product-moment correlations) was performed to determine the strength of linear association between the tapping rate and the several characteristics of the participants (age, using the continuous values; hand length; hand breadth; and middle finger length).
To accomplish the second of the secondary objectives of the study, means and standard deviations of the subjective ratings of the perceived exertion based on Borg’s 10-point scale after 1 min of the tapping task were calculated for all the eight fingers.
For all the inferential statistical analyses, a p value <.05 was used to indicate significance. Minitab 16 software was used for all the analyses.
Results
Descriptive Statistics
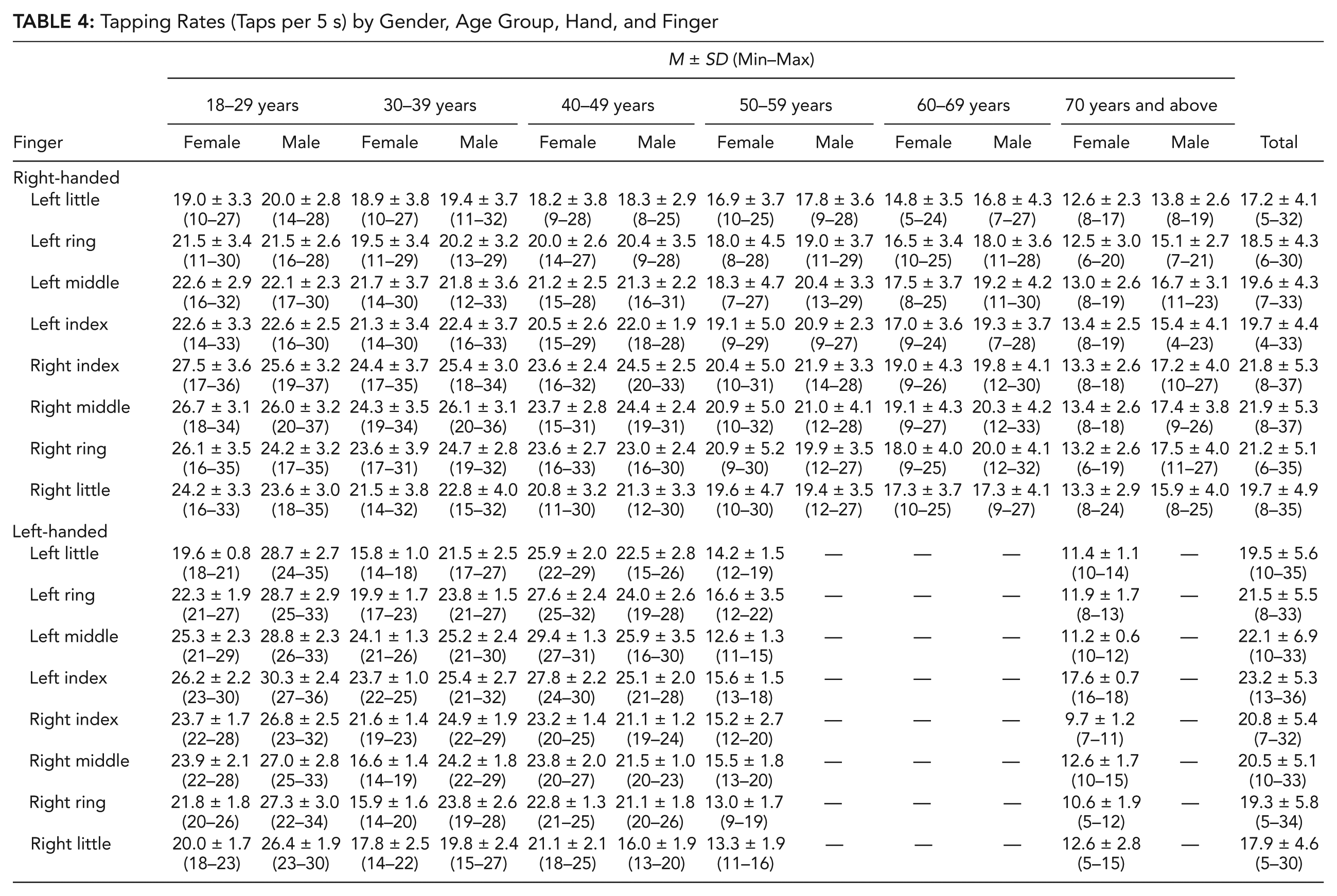
For the first objective of the study, a descriptive statistical analysis of the collected tapping-rate data was performed, and the finger-tapping rates of all the eight fingers were estimated across finger, gender, hand preference, and age factors. The results were summarized by a table (Table 4) and box plots (Figures 2 and 3). The box plots depict the mean (circles), median, first and third quartiles, and range values and spread of the data.
Tapping Rates (Taps per 5 s) by Gender, Age Group, Hand, and Finger
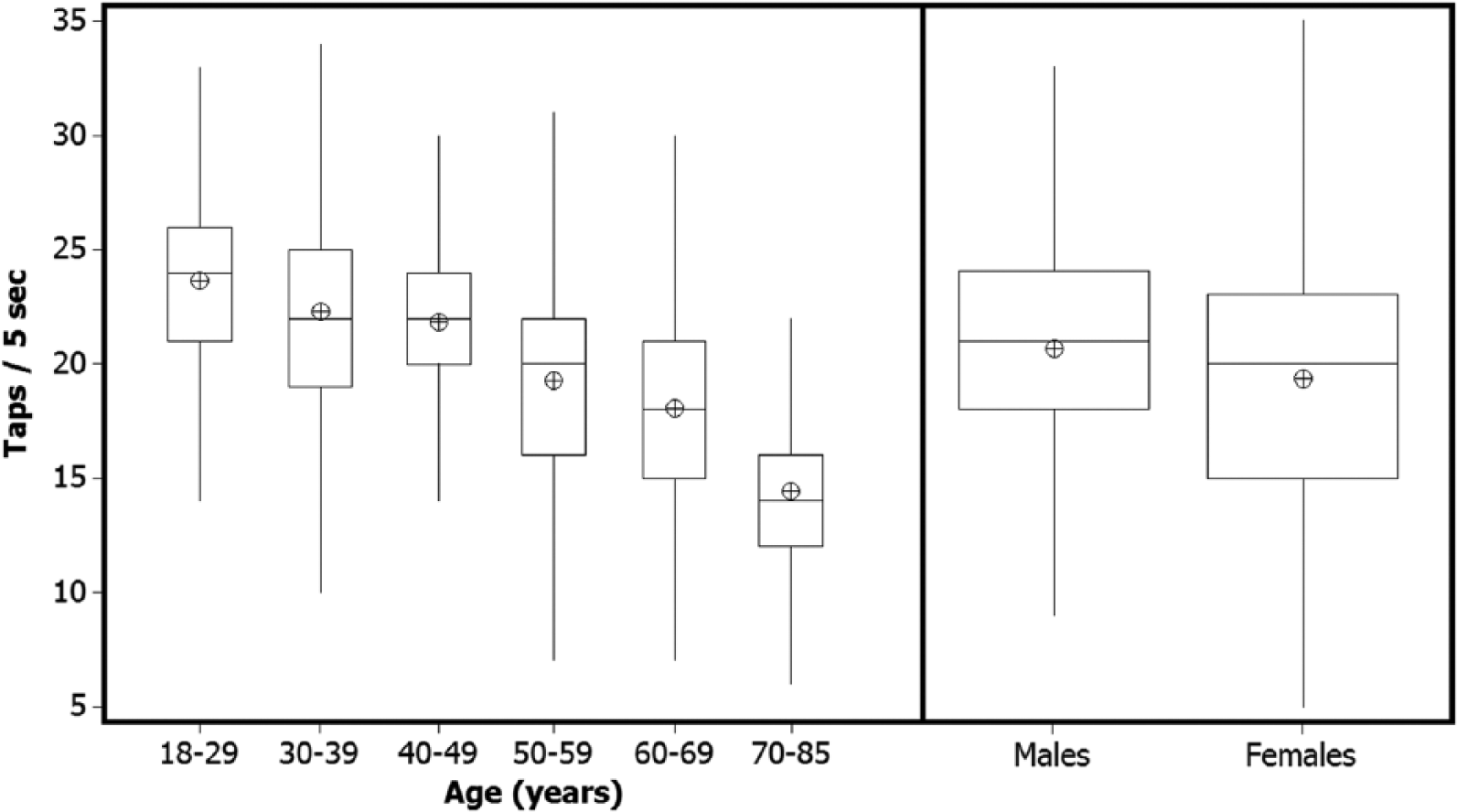
Box plots of finger-tapping rate for (a) age and (b) gender.
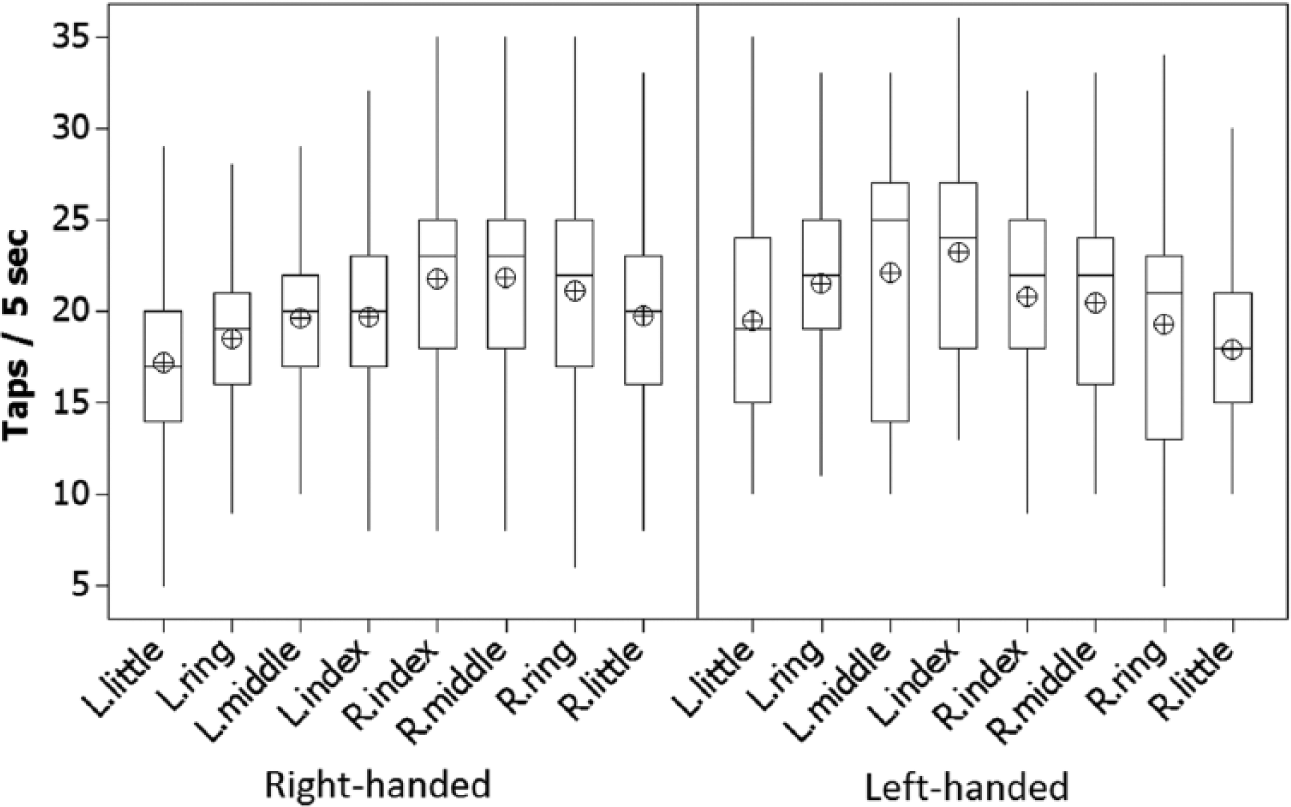
Box plots of finger-tapping rate by each finger.
Tapping rate seemed to decrease with age, especially after age group of 40 to 49 (Figure 2a). The rate of decrease seemed to be even faster after age group of 60 to 69. The participants within the age group 60 to 69 had a 0.58-taps-per-second higher rate than the participants within the 70-to-85 age group.
The males seemed to have slightly higher tapping rate and lower variation than females (Figure 2b). Trends of tapping rate with respect to both hands and the fingers of both hands (both right- and left-handed) are also tabulated and shown graphically (Table 4 and Figure 3).
Factor Effects
For the second objective of the study, an ANOVA was performed to determine the effects of the independent factors on the response variable. In the ANOVA, the interaction effects were found insignificant, thus they were omitted. Therefore, when calculating the sum of squares, we took only significant main effects into consideration.
According to ANOVA results, all factors (age, gender, finger, period, smoking, and exercise), except hand preference, were found significant on the response variable. That is, hand preference had no significant effect on the finger-tapping rate when the fingers were categorized as dominant-hand and nondominant-hand fingers. Due to this finding, an ANOVA without hand preference factor was rerun. The results of the ANOVA as taken from Minitab 16 statistical software package is shown in Table 5, and the main effects plots are shown in Figure 4.
ANOVA Results
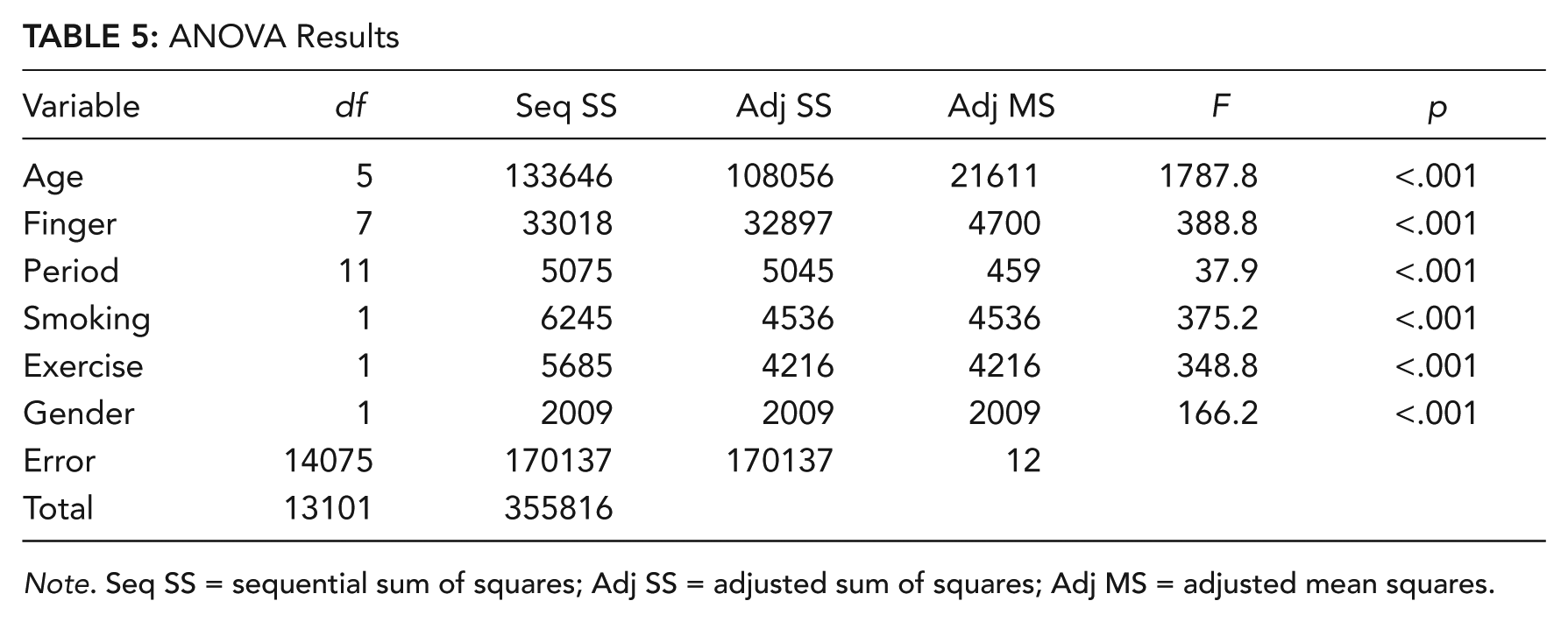
Note. Seq SS = sequential sum of squares; Adj SS = adjusted sum of squares; Adj MS = adjusted mean squares.
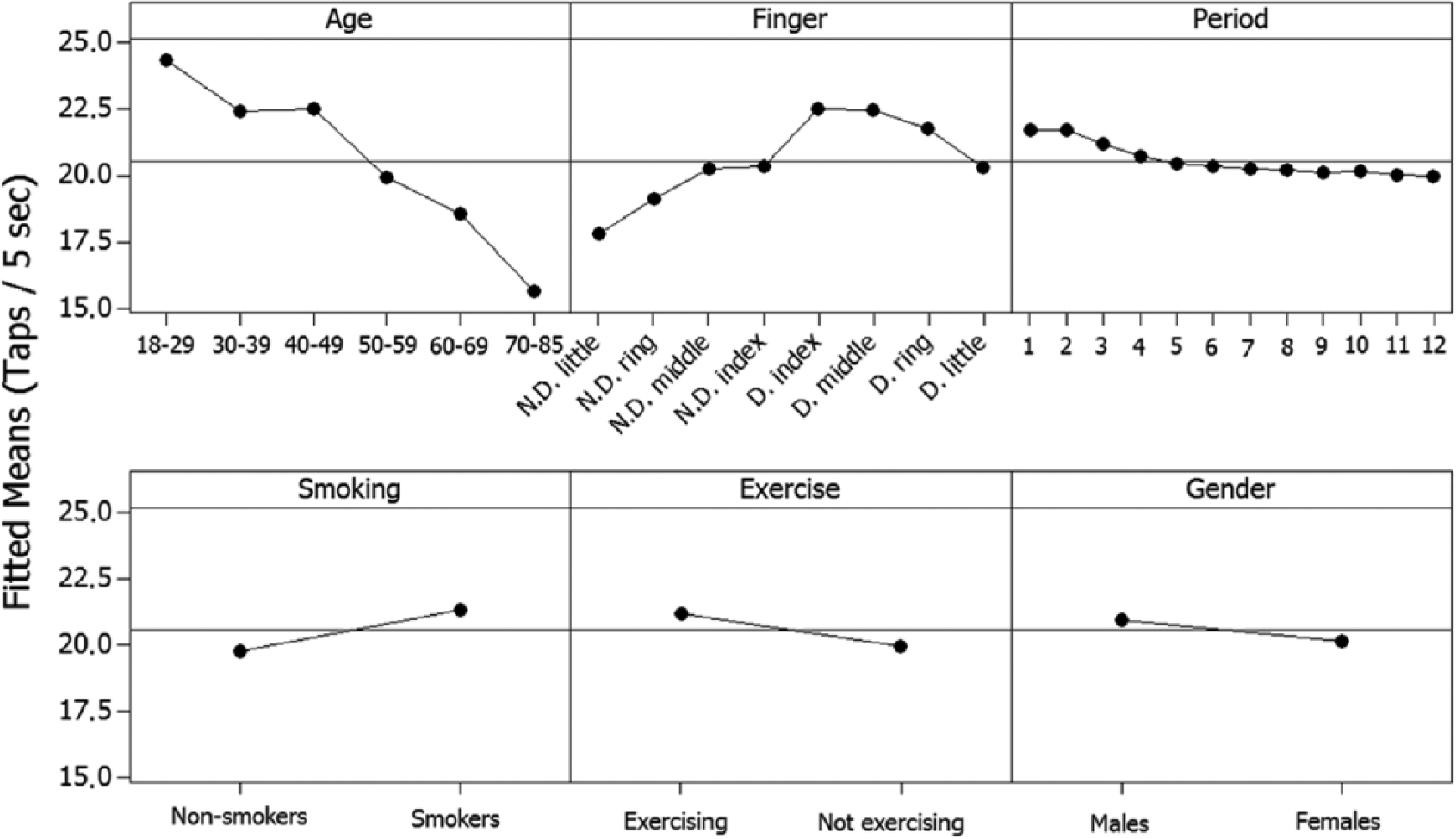
Main effect plots of finger-tapping rates.
Since the ANOVA indicated significant effects for independent variables, comparisons across the multiple variable levels were tested using post hoc Tukey’s tests with 95% confidence. The results with the model coefficients are provided in Table 6.
ANOVA Model Coefficients and Post Hoc Analysis
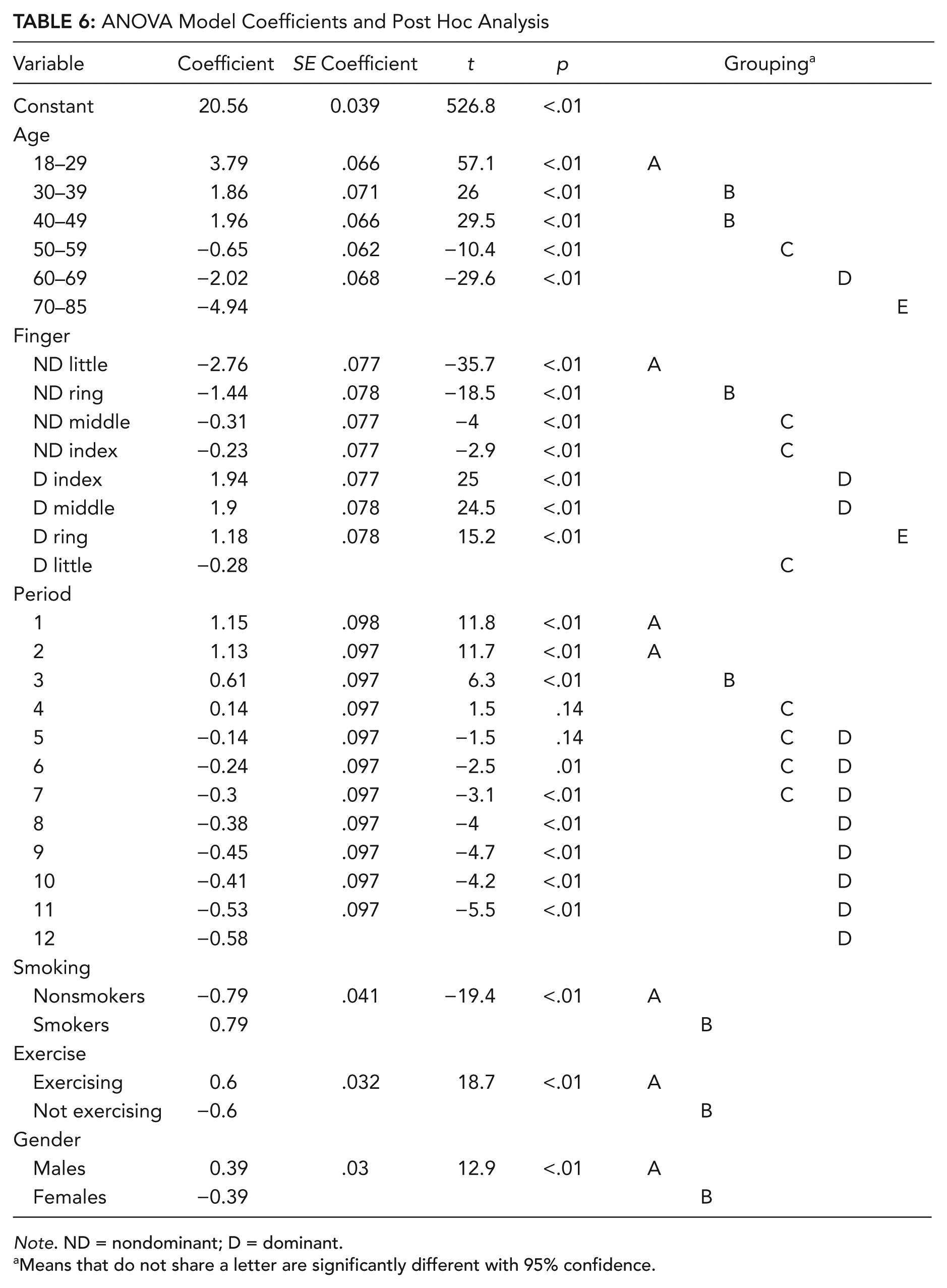
Note. ND = nondominant; D = dominant.
Means that do not share a letter are significantly different with 95% confidence.
Age effect
According to Tukey’s test results, all groups, except 30-to-39 and 40-to-49 age groups, were significantly different from each other (Table 6). The highest tapping rate was obtained at age group of 18 to 29 and the lowest at age group of 70 to 85.
Gender effect
Males had significantly higher tapping rates than females (Table 6). However, the average difference was only 0.16 taps per second.
Finger effect
Finger was found to be another important factor significantly affecting tapping rate (Table 6). Index and middle fingers were the fastest fingers for both hands, and the little fingers, the slowest. There was no significant difference between index and middle fingers, and this finding was true for both hands. All dominant-hand fingers, except little finger, had higher tapping rates than the fingers of the nondominant hand. The slowest finger of the dominant hand, the little finger, had the same tapping rate of the fastest fingers of the nondominant hand, index and middle fingers.
Period (duration) effect
There was no significant difference between Period 1 and Period 2 (i.e., in the first 10 s; Table 6). Then, significant decrease occurred for the 3rd and 4th periods. Then again, there were no significant differences among the 4th through 7th periods. The last eight periods (5th through 12th) were also statistically insignificant.
Smoking effect
Smoking was found to be another factor significantly affecting tapping rate (Table 6). The finger-tapping rates increased with smoking. There was, on average, a difference of 0.32 taps per second (1.58 taps per 5 s) between the smokers and nonsmokers.
Exercise effect
Weekly exercise rate was also found to be statistically significant (Table 6). The finger-tapping rate increased with the weekly regular exercise. There was, on average, a difference of 0.24 taps per second (1.2 taps per 5 s) between the exercising and nonexercising participants.
FLCs
For the third objective of the study, three ANOVA models were formed with participants taken as the block factor to determine the FLCs of all the eight fingers (excluding thumbs) based on the tapping rates. The first ANOVA was for the whole sample (composed of 7% left-handed and 93% right-handed participants), the second ANOVA was solely for the right-handed, and the third ANOVA was solely for the left-handed participants (for details, refer to the Method section).
For all three models, all the factors significantly affected the response. For the sake of brevity, the ANOVA results table for the whole-sample model only is provided (Table 7).
ANOVA Results for the Whole-Sample Model
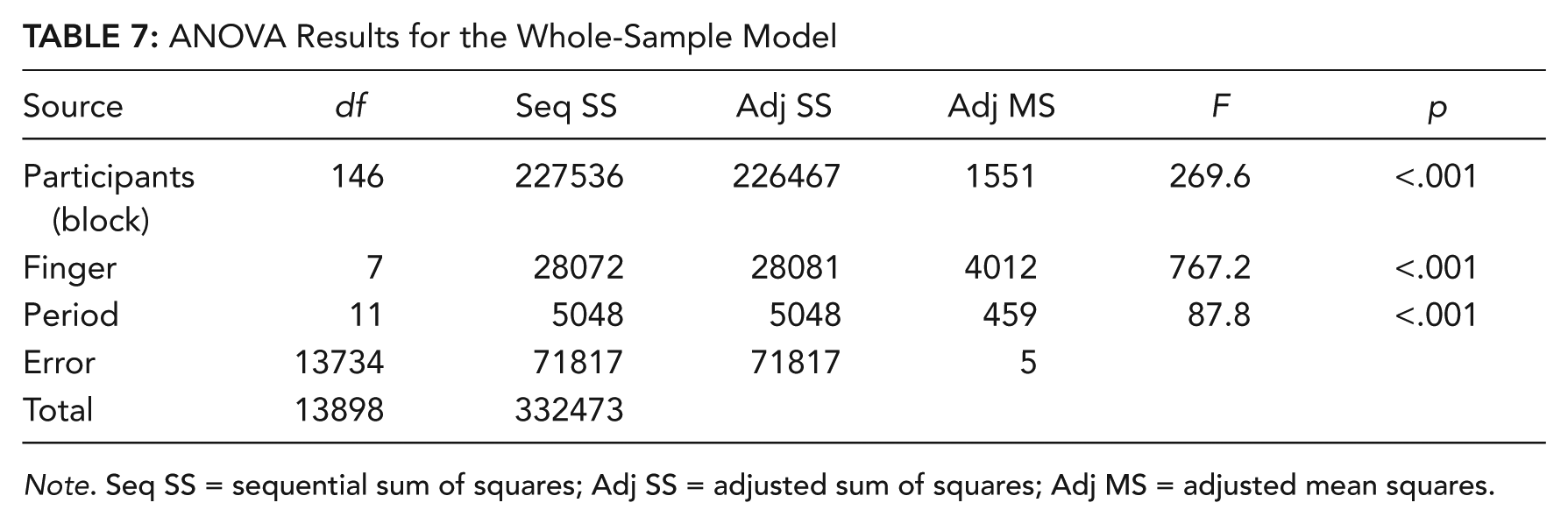
Note. Seq SS = sequential sum of squares; Adj SS = adjusted sum of squares; Adj MS = adjusted mean squares.
The main effects of finger factor obtained from the ANOVA were normalized to obtain the FLCs as described in the Statistical Method section. The estimated FLCs for the right-hand-dominant and left-hand-dominant participants and for the whole sample are provided in Table 8. Table 8 also lists the FLC values used by Dvorak et al. (1936). The FLC values from the two studies indicate that the order of the finger capacity is the same, and there are small differences in the values of the two studies. The FLC values of the present study are slightly higher for the little and ring fingers, whereas the FLC values used by Dvorak et al. are a little higher for index and middle fingers. In addition, the difference between the FLCs of left and right hands of the present study are higher than the difference between the FLCs of left and right hands used by Dvorak et al.
Normalized Tapping-Rate Capacities of Fingers (FLCs) for Right-Hand-Dominant and Left-Hand-Dominant Participants and Whole Sample and the Data From the Study by Dvorak, Merrick, Dealey, and Ford (1936) (in percentages)
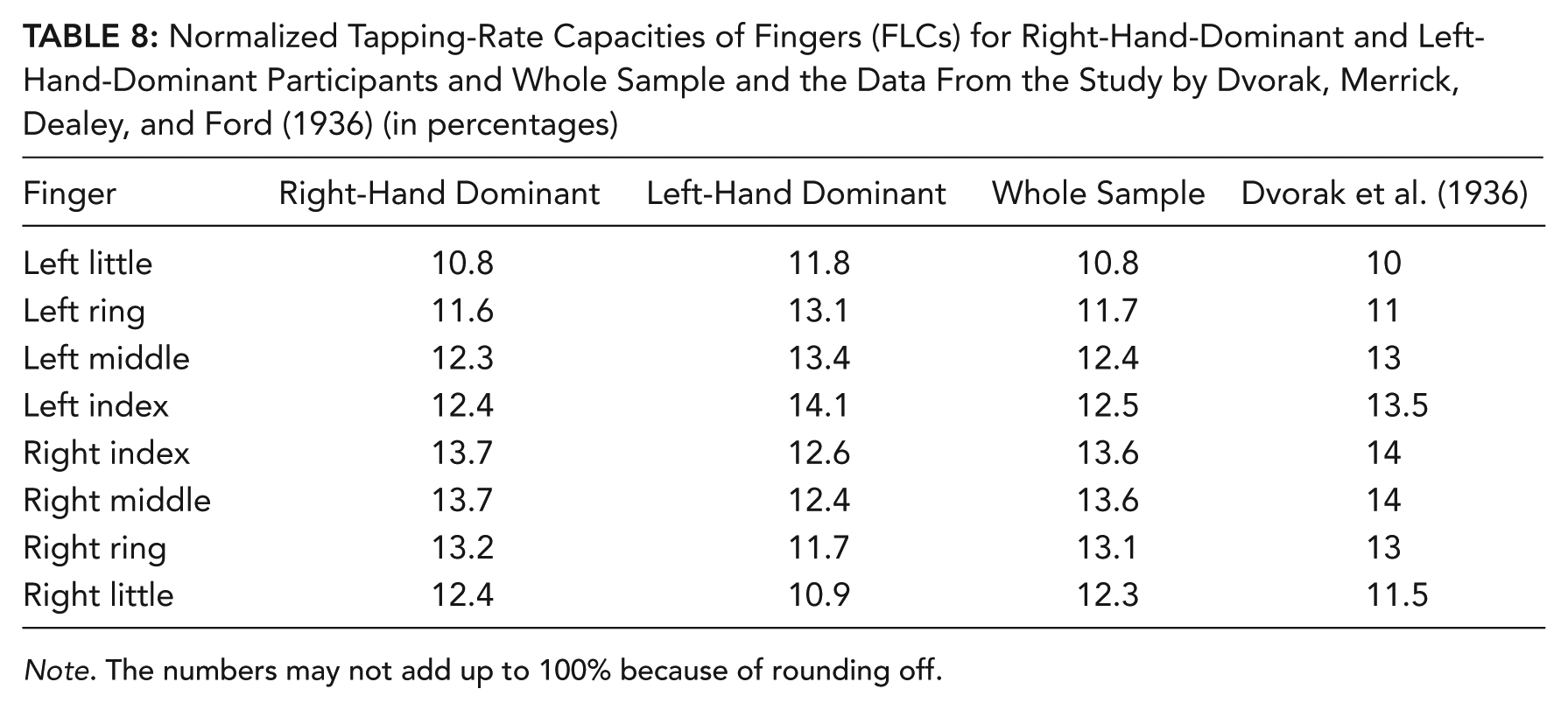
Note. The numbers may not add up to 100% because of rounding off.
Correlation Analysis
For the first secondary objective of the study, a correlation analysis (Pearson product-moment correlations) was performed to determine the strength of linear association between tapping rate and the participants’ characteristics (age, for the continuous values; hand length; hand breadth; and middle finger length).
All the variables, except middle finger length for the females, were significantly correlated with tapping rate for both genders (Table 9). Age and hand breadth were negatively and hand and middle finger lengths were positively correlated with tapping rate for both genders (except middle finger length for females). Age factor had the strongest correlation with the tapping rate.
Pearson Correlations Between Tapping Rate and the Subject Characteristics With p Values for Both Males and Females
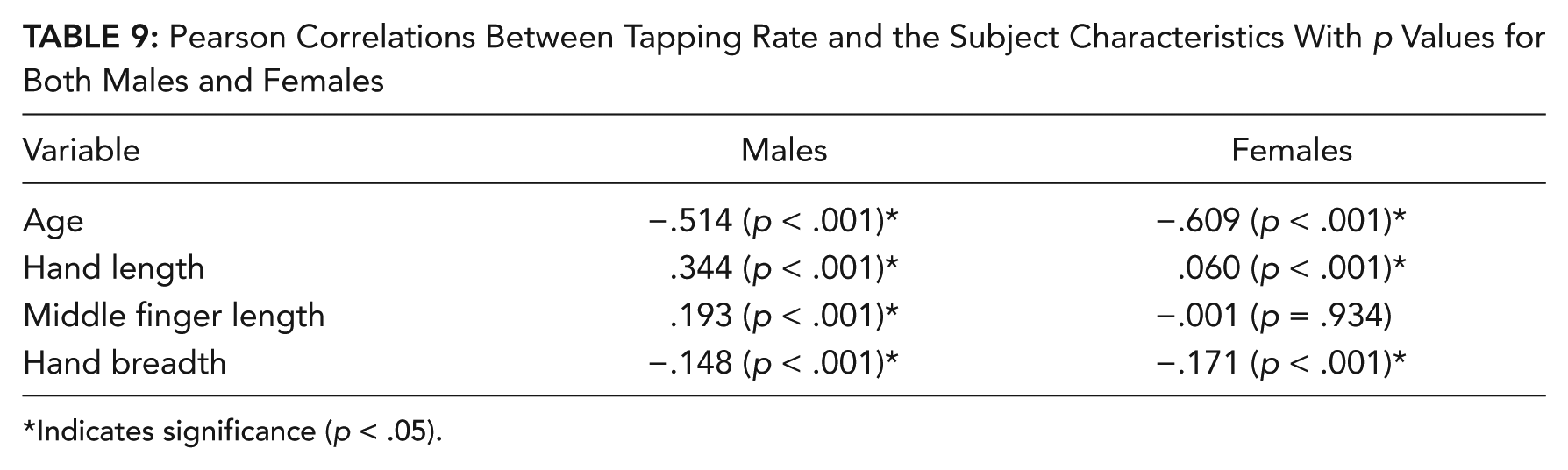
Indicates significance (p < .05).
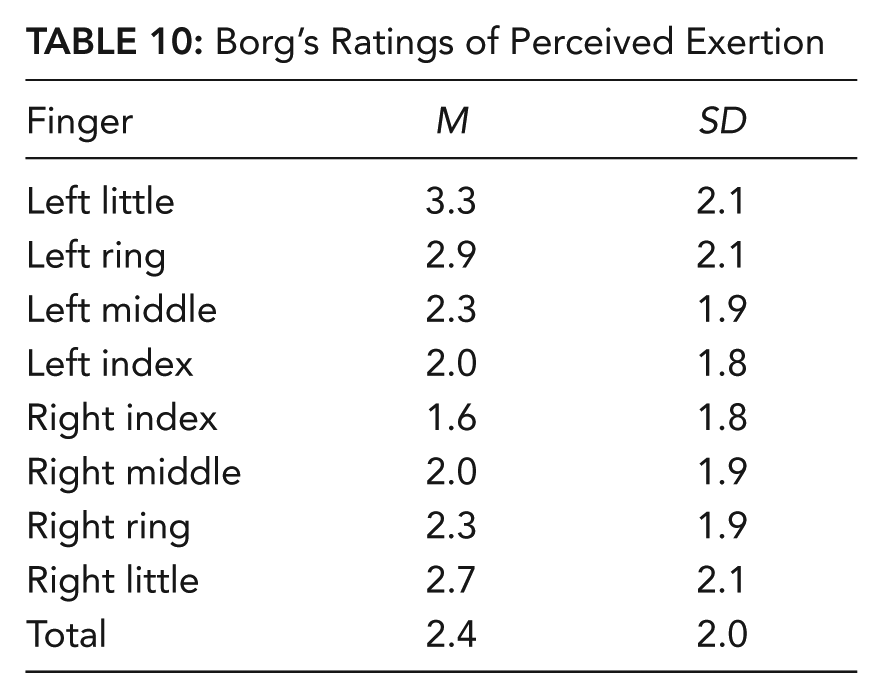
Subjective Ratings of Perceived Exertion
For the second of the secondary objectives of the study, the ratings of perceived exertion according to Borg’s 10-point scale were estimated based on the collected ratings data. The ratings were varied among the participants and decreased from little finger to index finger (Table 10). The fingers with higher tapping rates had lower ratings than the others. In addition, the ratings of right-hand fingers were lower than left-hand fingers. However, it should be noted again that 93% of the subjects were right-handed. The highest mean rating value of 3.3 was obtained for left little finger, which corresponded to “moderate” fatigue level.
Borg’s Ratings of Perceived Exertion
Discussion
The main aims of this research were to quantify the tapping rates of the fingers and determine the effects of various factors on the finger-tapping rate. This study provided one of the most comprehensive tapping data and showed the effects of the various factors on tapping rate.
The tapping rate decreased significantly with age. It is not surprising that as people get older, their physiology slows down and causes the response initiation and duration deficit. That is, muscle contractions and neural conductions take more time. In addition, there may be motivational differences and perhaps orthopedic or medication-related difficulties in aged subjects (Cousins et al., 1998).
Average male tapping rate was significantly higher than female. However, the average difference was small to be considered significant in practical sense. The studies by Bornstein (1985), Cousins et al. (1998), and Schmidt et al. (2000) also reported significantly higher tapping rates for males. In contrary, the tapping study for the right-hand fingers by Jackson (1953) reported higher tapping rates for females. However, the faster rates of the women were mostly due to women typists, since the rates of nontypists differed little from those of the men. One may speculate that although males are faster in many sports activities, such as swimming and running, due to bodybuilding and testosterone effects, it seems that for the tasks that require minimal force exertion, such as tapping, these factors do not play a significant role.
Fingers varied in their tapping rates. Index and middle fingers were the fastest fingers for both hands, and the little fingers, the slowest. Although the absolute tapping rates of right-hand fingers obtained through the present study were somewhat different from the rates reported by Riemer (1929) and the right-hand finger-tapping rates reported by Jackson (1953), the speed order of fingers was similar between the two studies. The tapping-rate differences among the fingers can perhaps be attributed to differences among the biomechanical advantage of the finger muscles and a practice effect.
Hand preference had no significant effect on the finger-tapping rate when the fingers were categorized as dominant-hand and nondominant-hand fingers. Previous research supports this result. For example, Schmidt et al. (2000) used a larger number of left-handed participants and concluded that hand preference had no significant effect on overall finger-tapping rate.
For the period effect, roughly speaking, tapping data showed a decreasing trend, especially between second and fourth periods. After the fourth period, the decrease was marginal. It seems that in the last 30-s period of the 1-min tapping task, there was a nearly steady rate of tapping. The effect of time on the tapping rate needs to be tested for longer durations, for example, until fatigue, to have a better idea about the variation of tapping rate as a function of time. Since none of the tapping studies in the literature used a tapping duration as long as 1 min, a comparison with previous studies was not possible for the effect of time on tapping rate.
Smokers tapped faster than nonsmokers. This result is in agreement with the results of previous studies on the effect of smoking and nicotine on finger-tapping rates (e.g., Perkins et al., 1990; Roth & Batting, 1991; Silver et al., 2002; West & Jarvis, 1986). This finding is explained by the increase in central processing speed by smoking (Silver et al., 2002). Exercising participants also tapped, on average, faster than the nonexercising participants. This finding may be attributed to the improvement in the physical conditioning of the body due to exercise.
With the model coefficients in Table 6, tapping rates can be estimated as a function of the investigated factors. For instance, in order to estimate the tapping rate of a right-handed 64-year-old woman’s right index finger in the first 5 s (assuming she smokes and does not exercise regularly), one can use the coefficients in Table 6 in this way: (20.56 − 2.02 + 1.94 + 1.15 + 0.79 − 0.60 − 0.39 = 21.43 taps per 5 s). However, as explained earlier, these coefficients are for estimating the tapping rates in periods of 5 s. For estimating the tapping rate as taps per second, the result should be divided by 5. To find the prediction interval in which 95% of this type of observations will fall, one should add and subtract
The ratings of perceived exertion varied among the participants for fatigue after the 1-min tapping task. Fatigue rates decreased from little finger to index finger for both hands. In addition, left-hand fingers were more prone to fatigue. It seemed that the fingers with higher rates of tapping had also less fatigue than the others. The highest mean fatigue rate value of 3.3 for left little finger corresponded to “moderate” fatigue. This rating meant that most of the participants could carry on tapping more than 1 min.
Conclusions
The main aims of this research were to determine the tapping rates of fingers and to investigate the effects of gender, age, finger, tapping period, hand preference, smoking, and exercise on the finger-tapping rate. Based on the estimated tapping rates, the FLCs were also estimated.
Generally speaking, the results showed that the tapping rate varies with respect to the finger: Index and middle fingers are the fastest and the little fingers are the slowest for both hands. In addition, dominant-hand fingers were found to be faster than the nondominant-hand fingers. Based on these results, right-hand index and middle FLCs were estimated as the highest, and the left-hand little FLC was estimated as the lowest. Age was another important factor affecting the tapping rate. Roughly speaking, the tapping rate decreases with age and shows a sharp decline after age group of 60 to 69. For the case of gender effect, the difference between male and female tapping rates was found to be marginal and may be considered indifferent for practical applications. The effects of tapping period, smoking, and exercising were found as other factors significantly affecting the tapping rate. Tapping rate, roughly speaking, decreased from the 1st to the 12th period. However, the decreases were not statistically significant for the first two periods or from 4th to 7th and from 5th to 12th period. On average, the smokers performed faster than the nonsmokers, and regular-exercising participants performed faster than nonexercising participants.
This study is one of the most comprehensive studies, if not the only one so far, performed with relatively large samples including all adult age groups for both genders. Another important contribution of the study is that it provides tapping capacity of all eight fingers. Exercise effect and tapping duration effect on tapping rate were studied for the first time. Based on the study results, the normative data of finger tapping rates were obtained for adult population ages 18 to 85 years. By normalizing the tapping rates, FLCs were estimated. These data can serve as a valuable reference for ergonomic product and work designs and evaluations that require finger tapping, FLC, manual dexterity, and motor control. The data may also serve as a standard for clinicians to perform psychomotor tests to evaluate the integrity of the neuromuscular system and to examine motor control in order to assess motor abilities and neurological problems.
It should be noted that the tapping data in this study were collected by the use of a standard notebook computer keyboard. Tapping capacity may be affected by the keyswitch design, especially the key travel distance and the key resistance force. Thus, the absolute values of tapping rates may be limited to the standard notebook computer keyboard. However, the authors also think that the normalized values of the tapping rates of fingers (FLCs) will not be affected significantly by the keyswitch design, and these normalized values are more important than the absolute values in ergonomic designs.
Key Points
Normative data of tapping rates for eight fingers (excluding thumbs) were estimated for a healthy adult population consisting of both genders ages 18 to 85.
Age, finger, smoking, period, and exercise factors significantly affected the tapping rate.
Index and middle fingers were the fastest fingers for both hands, and little fingers were the slowest. Dominant-hand fingers were faster than nondominant-hand fingers.
Tapping rate decreased with increasing age and increased with smoking and regular exercise.
Finger load capacities were calculated using the tapping-rate data for the convenience of the ergonomic designs.
Footnotes
Acknowledgements
This research was supported by the Scientific and Technological Research Council of Turkey (TÜBİTAK) Grant 111M530 awarded to Mahmut Ekşioğlu.
Mahmut Ekşioğlu is an associate professor and founding director of the Ergonomics Laboratory in the Department of Industrial Engineering, Boğaziçi University. He received his PhD in industrial engineering in 1996 from Wichita State University. He earned a BS in mechanical engineering from Yıldız Technical University (Istanbul) and an MS in aerospace engineering (1990) and an MS in industrial engineering (1992) both from Wichita State University. Before joining academia, he served as an ergonomics consultant and a National Institute for Occupational Safety and Health researcher in the United States. His teaching and research interests are in the area of ergonomics and human factors engineering, safety engineering and management, and applied statistics.
Ali İşeri is an assistant professor in the Department of Industrial Engineering at Fatih University (Istanbul). He received his PhD in industrial engineering in 2014 from Boğaziçi University, Istanbul, Turkey. He earned a BS (2006) and an MS (2008) in industrial engineering both from Fatih University. His teaching and research interests are in the area of ergonomics, applied optimization, and statistics.