
Abstract
Objective:
The aim of this study was to evaluate the efficacy of the new Variable Lifting Index (VLI) method, theoretically based on the Revised National Institute for Occupational Safety and Health [NIOSH] Lifting Equation (RNLE), in predicting the risk of acute low-back pain (LBP) in the past 12 months.
Background:
A new risk variable termed the VLI for assessing variable manual lifting has been developed, but there has been no epidemiological study that evaluates the relationship between the VLI and LBP.
Method:
A sample of 3,402 study participants from 16 companies in different industrial sectors was analyzed. Of the participants, 2,374 were in the risk exposure group involving manual materials handling (MMH), and 1,028 were in the control group without MMH. The VLI was calculated for each participant in the exposure group using a systematic approach. LBP information was collected by occupational physicians at the study sites. The risk of acute LBP was estimated by calculating the odds ratio (OR) between levels of the risk exposure and the control group using a logistic regression analysis. Both crude and adjusted ORs for body mass index, gender, and age were analyzed.
Results:
Both crude and adjusted ORs showed a dose-response relationship. As the levels of VLI increased, the risk of LBP increased. This risk relationship existed when VLI was greater than 1.
Conclusion:
The VLI method can be used to assess the risk of acute LBP, although further studies are needed to confirm the outcome and to define better VLI categories.
Introduction
Despite high automation levels in today’s factories, manual lifting is still to be considered a widespread risk factor. According to Eurofound’s fifth survey (Eurofound, 2012), gender, employment status (e.g., manual or high-skilled clerical workers), and age have been shown to be associated with low-back pain (LBP; Biering-Sørenson, Thomsen, & Hilden, 1989; Guo et al., 1995; Hidalgo et al., 1995; Karwowski, 1983; Liberty Mutual Research Institute for Safety, 2009).
The World Health Organization announced in 2009 that “37% of back pain is attributable to occupational risk factors” and it is the “main cause of absence from work, generating economic losses” (Driscoll et al., 2014).
The National Institute for Occupational Safety and Health (NIOSH) has recognized work-related back injuries as an actual problem. In 1981, it published the Work Practices Guide for Manual Lifting (Department of Health and Human Services, 1981), where the NIOSH Lifting Equation (NLE) was first introduced. In 1993, in order to extend the applicability of the method and make it suitable for a greater number of work situations, the NIOSH equation was revised (Waters, Putz-Anderson, Garg, & Fine, 1993). It has since been widely used all over the world and adopted for the publication of Standard ISO 11228 Part I (International Organization for Standardization [ISO], 2003).
According to the NIOSH method, the estimate of the level of physical stress is defined as the ratio of the weight of the load lifted divided by the recommended weight limit (RWL) for the task.
This ratio is termed the lifting index (LI). The LI is applicable to a single manual lifting task, defined as a job in which the task variables do not significantly vary from lift to lift, or only one lift is of interest (e.g., task with the worst value of LI). For assessing a multitask lifting job, a composite LI (CLI) may be used, which is defined as a job in which there are significant differences in concurrent lifting tasks, such as a palletizing job, where the vertical height can vary from lift to lift. Both the LI and the CLI have been validated by many previous studies (Waters et al., 1999; Waters, Lu, Piacitelli, Werren, & Deddens, 2011) that showed that the odds of LBP increased as the LI increased from 1.0 to 3.0.
The mathematical equation for computing the CLI is not efficient for a large number of variable lifting tasks. The Variable LI (VLI) method used in this study was designed to handle a large number of variable lifting tasks, where conditions vary significantly between exertions (Waters, Occhipinti, Colombini, Alvarez-Casado, & Fox, 2016).
To further extend the applicability of the NIOSH method, the VLI was presented in 2009 at the annual International Ergonomics Association conference in Beijing (Colombini, Occhipinti, Alvarez, Hernandez, & Waters, 2009). A guide for its application was published in 2012 (Colombini, Occhipinti, Alvarez-Casado, & Waters, 2012). The proposed VLI approach was developed in order to assess manual lifting jobs with highly variable tasks—work situations becoming more and more common.
In addition to the limitation of handling a large number of variable lifting tasks, both LI and CLI are also limited to several other factors, such as one person lifting and two-handed lifting activity only. Two-person or one-handed lifting is an important reality in the workplace and has been examined for its risk for LBP in many previous studies (Allread, Marras, & Parianpour, 1996; Arjmand, Plamondon, Shirazi-Adl, Parnianpour, & Larivière, 2012; Karwowski & Mital, 1986; Karwowski & Pongpatanasuegsa, 1988; Marras & Davis, 1998; Marras, Davis, Kirking, & Granata, 1999), and ISO Standard 11228 takes it partly into account: In Section A8, “Individual Considerations,” it is stated that “an approximate guide, the capability of a two-person team is two-thirds the sum of their individual capabilities and, for a three-person team, the capability is half the sum of their individual capabilities” (ISO, 2003). To machine designers, the standard EN 1005-2 (European Committee for Standardization, 2003) identifies a method for calculating the LI for one-handed lifts; according to the NIOSH method, an additional factor has to be added to calculate the RWL.
Furthermore, the NIOSH method calculates a single LI for both males and females, although the level of protection for males reaches 90% versus 75% for women, and for both young and old people (Waters et al., 1993).
These aspects go against the European legislation for safety and health in the workplace, which has been underlining, since 20 years ago, the need to take into account gender and age differences when assessing risk.
From a conceptual point of view, the VLI comes from the LI and CLI and is aimed at assessing the overall physical demand of a lifting job. To date, no studies have yet been carried out to evaluate the relationship between risk index and LBP.
This article presents a cross-sectional study carried out in several Italian companies in 2013 to 2014. The study investigates the relationship between the VLI and acute LBP. European criteria that differentiate risk assessment according to gender and age have been applied in the VLI calculation.
Method
The eligibility criteria for the study took into account the previous validation studies of the NIOSH method and were discussed by an expert committee formed for the occasion.
Selection criteria for exposed subjects were the following:
Having performed daily lifting activities for at least 167 days in the past year, regardless of the number of objects lifted per day;
Having spent more than 12 months on the current job being exposed to the risk;
Pulling, pushing, and carrying activities had to be residual tasks of the whole work shift;
No exposure to whole-body vibration;
No exposure to handling activities for more than 8 hr in a work shift.
During the first meeting of the expert committee, the inclusion requirement had been set at 180 worked days in the past year. However, one of the companies had to rely on “defensive” job security agreements due to financial issues, which caused a reduction of the workdays in the past year. Setting the cutoff parameter at 167 worked days in the past year, we have been able to include most of the company’s exposed workers (most of whom, however, worked for more than 170 days).
For what concerns point (c), the Italian legislation requires employers to fill out a risk assessment form that considers all possible risks. This form serves as a basis for the drafting of a work plan, complete with the relative work times, with the aim of improving health and safety in the workplace. Such drafts allowed us to determine the type and duration of residual tasks.
Unexposed subjects were selected according to the following criteria:
Be employed in the same company as the exposed subjects;
Perform mainly clerical jobs or use a visual display unit;
Make autonomous decisions for what concerns breaks and have the possibility to switch between sitting and standing position.
All the involved companies were formally invited, and their participation in the research project was voluntary.
Risk Assessment
The risk assessment was carried out by experts in the field (especially for what concerns the RNLE and the VLI) using the “systematic organizational analysis approach” (Waters et al., 2016). Collected data (number and weight of handled objects, lifting times, handling geometry, etc.) were entered into software, available online for free at www.epmresearch.org, thus ensuring homogeneity in the calculation of VLI values for the whole sample of exposed subjects. All investigators involved in risk assessment were blinded to whether workers reported LBP. Every single risk assessment was carried out or checked by the authors of this paper.
Based on the indications from European standards, risk indexes for gender and age were calculated for all exposure ranges. In this case, calculation of the RWL has been based on different load constants (maximum weight lifted in ideal conditions), following instructions from ISO-TR 12295 (ISO, 2014).
Weight that can be lifted in ideal conditions is as follows:
Men ages 18 to 45 = 25 kg
Women ages 18 to 45 and men ages <18 and >45 = 20 kg
Women ages <18 and >45 = 15 kg
To identify the VLI in the tables according to ISO-TR 12295, the code VLI_EU was used. The NIOSH load constant (23 kg) was also used to calculate the VLI; in this case, the code VLI_NIOSH was used.
In cases where direct observation of the work showed that weights were lifted with one hand, another multiplication factor of 0.6 was added in the calculation of RWL, as suggested by EN 1005-2.
When particularly heavy objects were lifted simultaneously by two operators, the following formula was used:
where W is the weight lifted.
From the information concerning the calculation of the VLI, it is possible to retrieve the value of the cumulative mass, meant as the sum of all weights lifted in one shift.
In order to make sure that the right method was used, involved companies attended a meeting where the research methodology was presented. Data on risk assessment were collected and recorded on a form prepared for the occasion, where risk assessors needed to indicate all handled objects, their weight, number of lifts, and handling geometries. These data were confirmed through an onsite inspection, at least two for each company.
Our analysis also includes jobs where either the horizontal or the vertical multiplier factor exceeded the limits established by the NIOSH method; when one of the factors in the RWL calculation is zero, the LI approaches infinity. For the purpose of this study, in the VLI calculation, the worst multiplier (closest to zero) was used for both horizontal factor and vertical location factor. For what concerns the horizontal factor, Waters et al. (2011) states that such procedure may cause an upward or a downward bias in the risk level. If the height at origin or destination is more than 175 cm, with regard to the subject’s anthropometric measurements, an extension of the lumbar spine is possible, which, according to biomechanical studies, may cause damage to the front part of the annulus (National Academy of Sciences & National Research Council, 2001). As a consequence, the VLI may be downward biased.
A total of 298 lifting jobs were assessed, 37 of which exceeded NIOSH limits for horizontal distance and 22 those for vertical location.
Companies that participated in the project belong to different sectors: manufacturing, pharmaceutical, and food. At the beginning (2013), 19 companies joined, to which eight more were added later (2014), for a total of 27 companies. By the end of the research, the number had decreased to 16, mainly due to corporate restructuring in which handling activity was performed on a nondaily basis.
Damage Assessment (Low-Back Health Assessment)
The damage assessment in this study considered episodes of acute LBP that occurred in the past 12 months (Chaffin & Park, 1973; Colombini et al., 1999). Clemmer, Mohr, and Mercer (1991) use the term back injury, differentiating it from LBP, when counting the episodes that tend to be more acute.
The “damage variable” used in this study was the acute LBP episodes that had occurred in the previous 12 months. Such events were defined as “presence of lumbar pain with or without irradiation obliging the patient to remain immobile for at least 2 days, or 1 day if a medication was taken.” This kind of episode shall also require a sick leave, to better differentiate chronic LBP from acute LBP. This choice was due to the well-known association between lumbar biomechanical overload and stimulation of LBP (Marras, 2008, p. 16; Radwin, Marras, & Lavender, 2001; Yassi et al., 1995).
Before starting the actual research, occupational physicians from the participating companies attended a meeting during which the procedure for collection of clinical data was described. In addition to personal and anthropometric data, the questionnaire included information on possible confounding factors (Gyntelbers, 1974; Heneweer, Vanhees, Susan, & Picavet, 2009; Knox, Orchowski, & Owens, 2012; Ono et al, 2012; Shiri, Karpiinen, Leino-Arjas, Solovieva & Viikari-Juntura, 2010). Such protocol was preliminarily applied by every physician, in an experimental way, to at least 10 workers. Results were then controlled. Physicians who had joined the survey in a satisfactory way (complete information and conformity of answers) were given the possibility to enter their data in a specific online database. Every 2 months, such data were checked in order to monitor the collection process and highlight possible mistakes in the application of the protocol.
By the end of the research period, 3,357 subjects exposed to manual material handling and 1,409 unexposed had been entered in the database (4,766 total). After applying the eligibility criteria, the sample was reduced to 2,385 exposed subjects and 1,028 unexposed. Exclusions were mainly due to nondaily handling activity and the fact that, in some companies, collection of clinical data did not match a similar collection of data on risk exposure.
The study of the association between exposure and damage was carried out using the method of logistic regression analysis (Kleinbaum, Kupper, & Morgenstern, 1982), considering a binary response variable for each subject: the presence of “damage” (at least one episode of acute LBP in the past year) and the absence of “damage” (no episodes). For each exposure index level, the odds ratio of prevalence (POR or simply OR) was calculated, using subjects employed in the same companies as a reference.
The use of OR (hence the logistic regression) is appropriate in this case. Because the frequencies of acute LBP are below 10%, the OR could be interpreted as an estimate of relative risk (i.e., ratio of proportions). Analyses were first conducted with raw data; multivariate analyses were then adjusted for potential confounding factors (sex, age, body mass index [BMI]). The program PROC GENMOD in SAS (SAS Institute, Cary, NC) was used for statistical analyses.
Results
Table 1 shows the main data about the analyzed sample. For a total of 3,402 subjects, 1,028 were unexposed and 2,374 were exposed (11 exposed subjects have been removed as they had spent less than 1 year on the job).
Description of the Sample for Categories of VLI_EU a

Note. M = male; F = female; BMI = body mass index.
Recommended weight limit based on different weight constants (maximum weight lifted in ideal conditions) as specified in ISO-TR 12295.
As shown in Table 1, study participants were fairly evenly distributed across four exposure levels of the VLI. There was no statistically significant difference in age, BMI, sector, and job seniority between the exposure levels. Among exposed subjects, gender ratio increases remarkably as exposure levels increase; this finding is particularly evident in the highest exposure category.
Table 2 shows that when the NIOSH load constant (VLI_NIOSH) is applied, subjects’ distribution on the basis of VLI levels turns out to be partially different: As the levels of VLI become higher, the number of subjects decreases. The other descriptive characteristics appear to be the same as those from the previous sample (VLI_EU) except the percentages of male workers in the increased VLI categories above 2.
Description of the Sample for Categories of VLI_NIOSH a
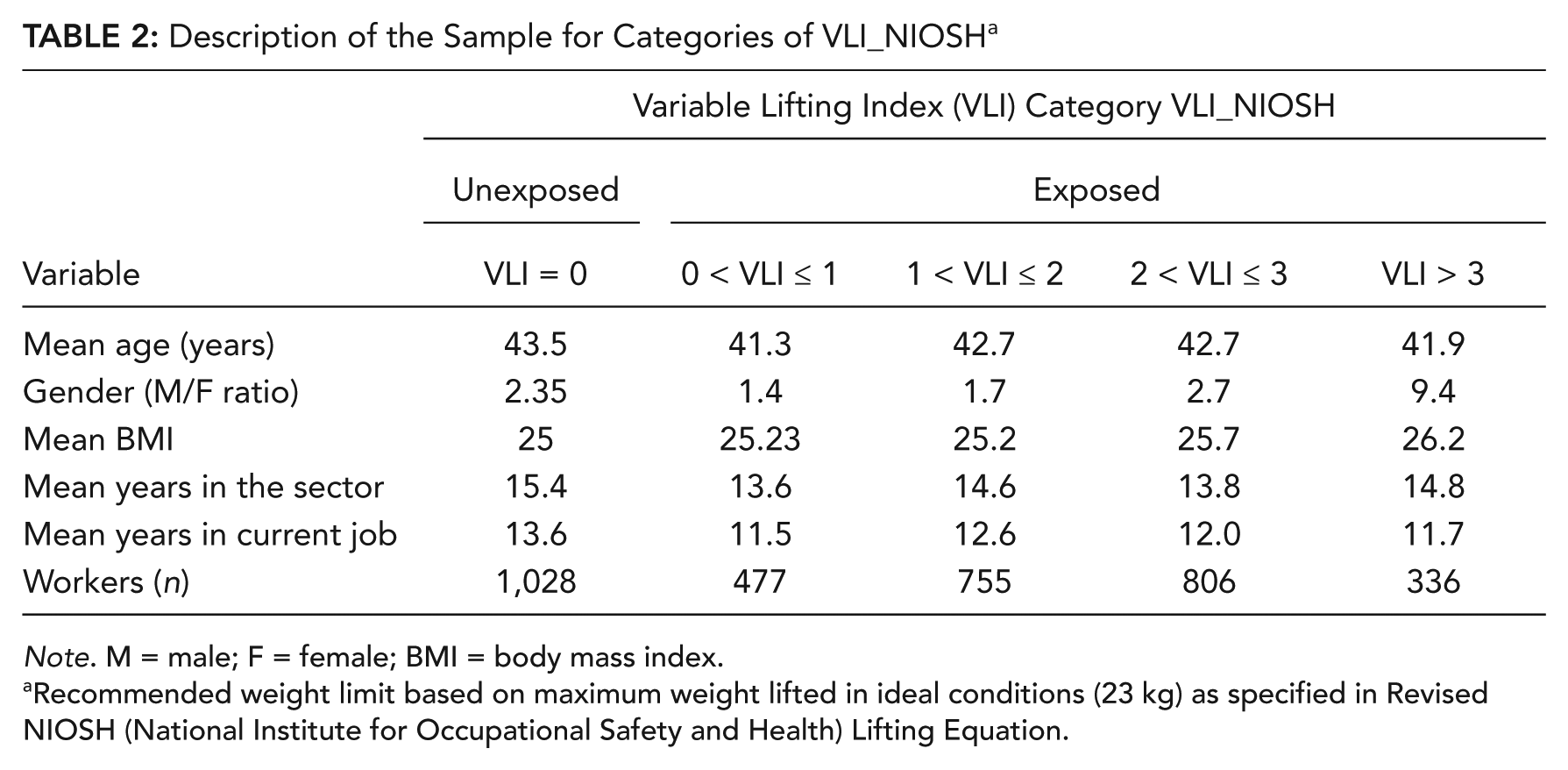
Note. M = male; F = female; BMI = body mass index.
Recommended weight limit based on maximum weight lifted in ideal conditions (23 kg) as specified in Revised NIOSH (National Institute for Occupational Safety and Health) Lifting Equation.
Table 3 shows the crude OR of the analysis of the relationship between VLI_EU levels and acute LBP episodes in the past year. In the range from VLI_EU = 1 to 3, as the level of the VLI_EU increases, the OR of acute LBP increases. Nonetheless, the linear trend for OR indicates the presence of linear growth as the level of exposure increases.
Unadjusted Association Between Variable Lifting Index (VLI_EU a ) and Occurrence of Acute Low-Back Pain in the Previous Year
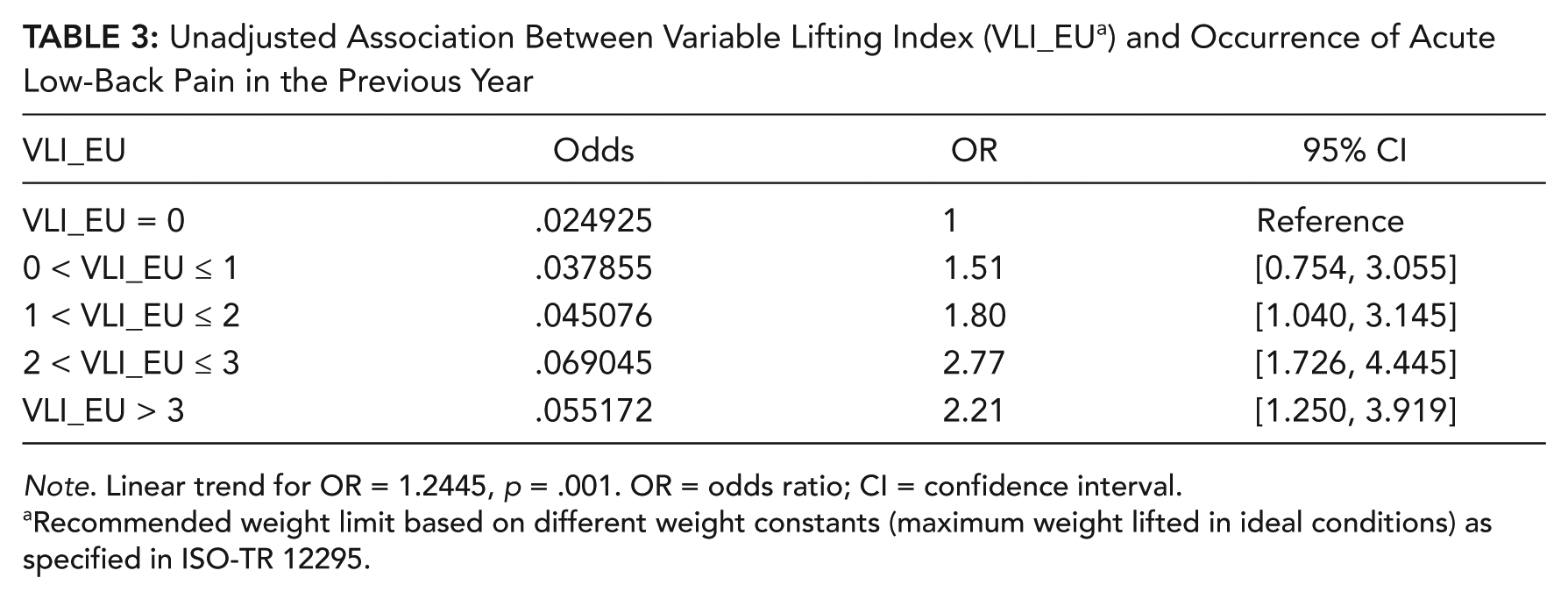
Note. Linear trend for OR = 1.2445, p = .001. OR = odds ratio; CI = confidence interval.
Recommended weight limit based on different weight constants (maximum weight lifted in ideal conditions) as specified in ISO-TR 12295.
As shown in Table 4, the result is not remarkably modified by adding the chosen confounders (BMI, gender, and age); the linear growth is still positive. It is worth underlining that the only confounder that seems to play an important role is BMI, especially for underweight subjects. As the VLI_EU calculation is differentiated according to gender and age, data confirm that, as expected, such factors are irrelevant.
Association Between Variable Lifting Index (VLI_EU a ) and Occurrence of Acute Low-Back Pain in the Previous Year, Adjusted by Body Mass Index, Gender, and Age
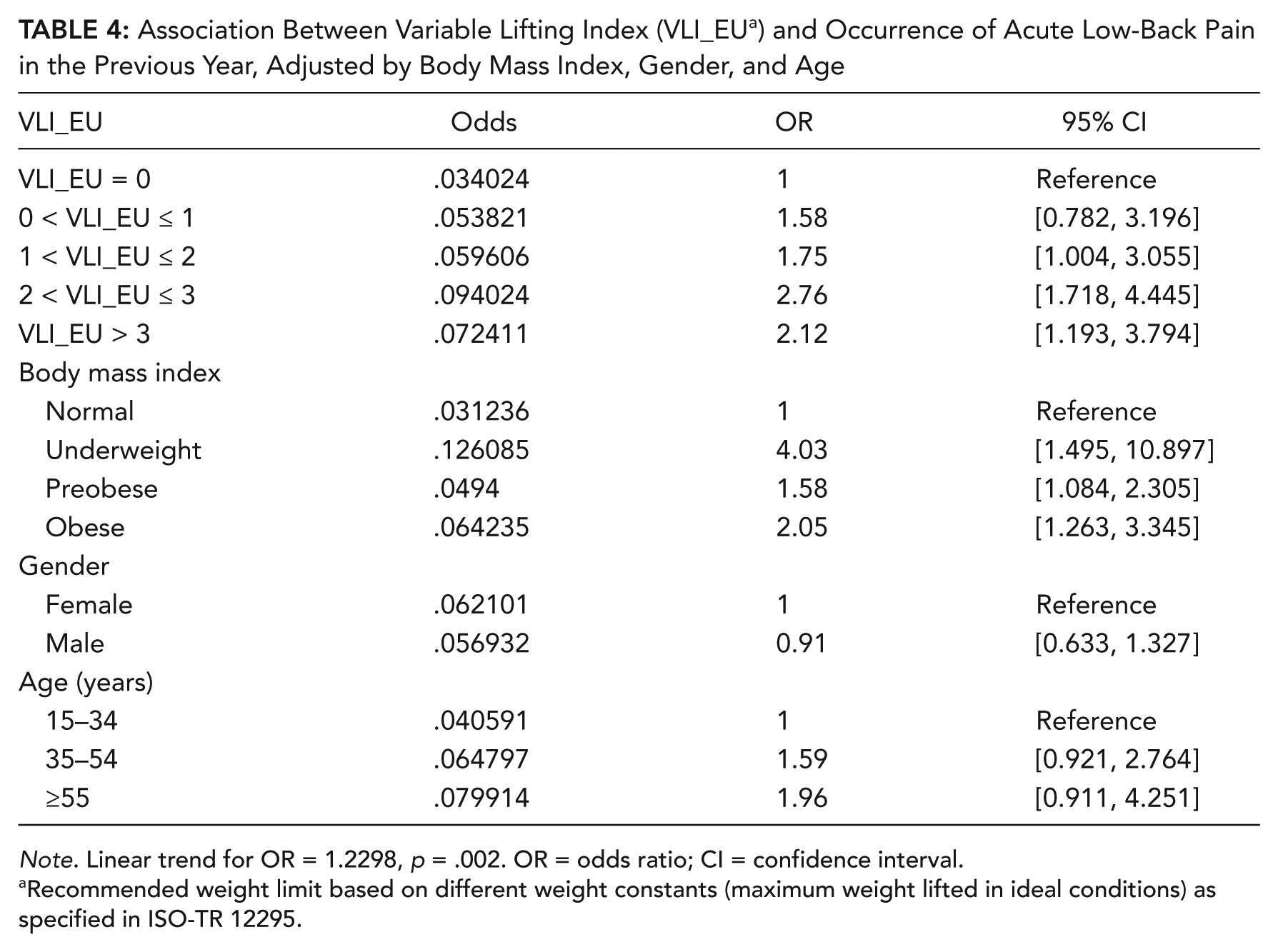
Note. Linear trend for OR = 1.2298, p = .002. OR = odds ratio; CI = confidence interval.
Recommended weight limit based on different weight constants (maximum weight lifted in ideal conditions) as specified in ISO-TR 12295.
For VLI_EU values higher than 1, in both analyses, adjusted and unadjusted, ORs are statistically significant at confidence level of 95%.
A similar statistical analysis was carried out for VLI_NIOSH. Tables 5 and 6 show unadjusted results first and then adjusted results for the same confounding factors. Results appear to be similar to those highlighted in the VLI_EU analysis. Namely, the OR linear trend is positive, and BMI is the only significant confounder. For VLI_NIOSH values higher than 1, in both analyses, adjusted and unadjusted, ORs are statistically significant at confidence level of 95%. Given the type of analysis, age and gender were expected to be important confounding factors, as the VLI_NIOSH calculation method does not take into account age and gender differences; this result is similar to Waters et al.’s (1999, 2011).
Unadjusted Association Between Variable Lifting Index (VLI_NIOSH a ) and Occurrence of Acute Low-Back Pain in the Previous Year

Note. Linear trend for OR = 1.258474, p = .0009. OR = odds ratio; CI = confidence interval.
Recommended weight limit based on maximum weight lifted in ideal conditions (23 kg) as specified in Revised NIOSH (National Institute for Occupational Safety and Health) Lifting Equation.
Association Between Variable Lifting Index (VLI_NIOSH a ) and Occurrence of Acute Low-Back Pain in the Previous Year, Adjusted for Body Mass Index, Gender, and Age
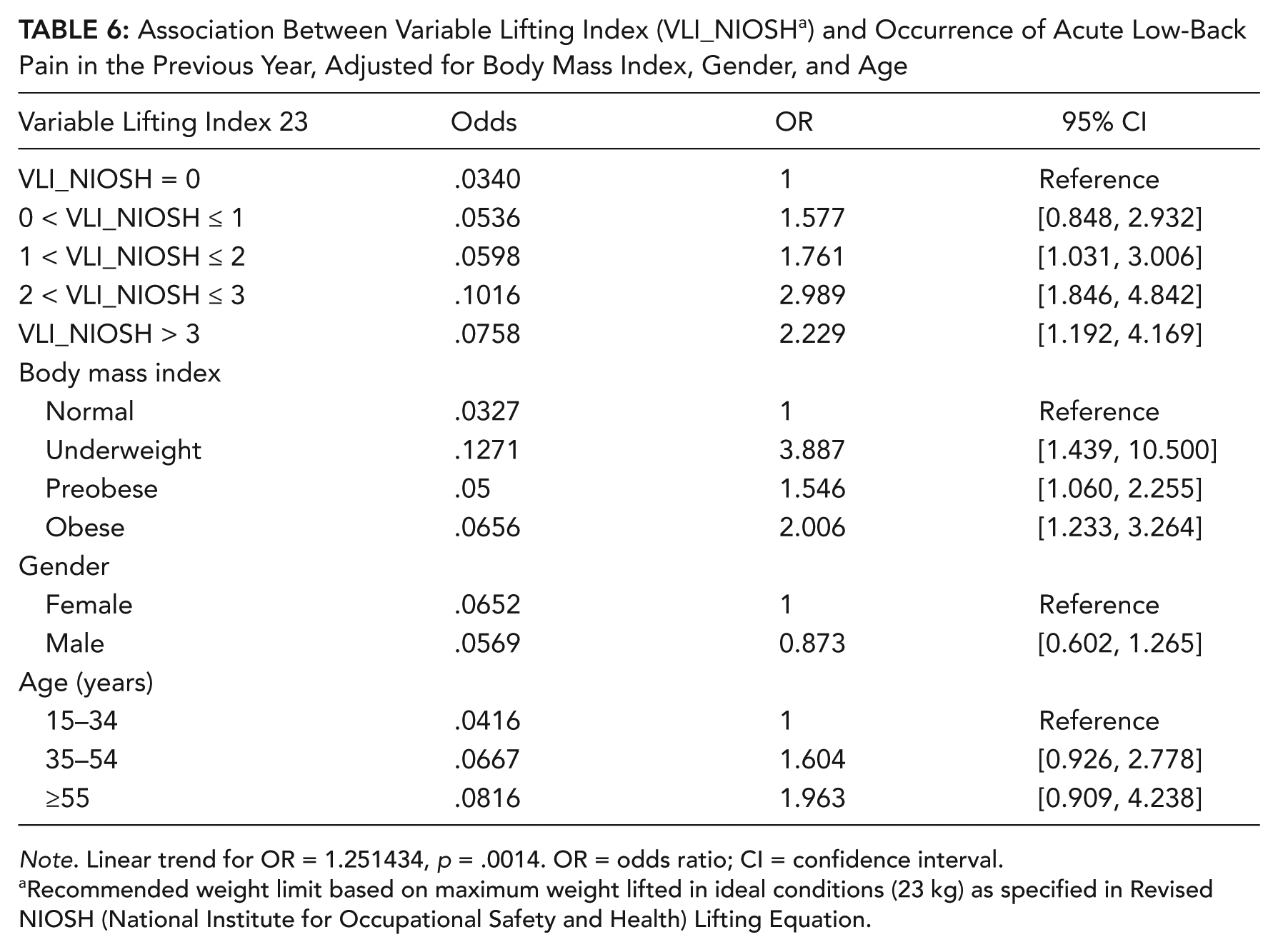
Note. Linear trend for OR = 1.251434, p = .0014. OR = odds ratio; CI = confidence interval.
Recommended weight limit based on maximum weight lifted in ideal conditions (23 kg) as specified in Revised NIOSH (National Institute for Occupational Safety and Health) Lifting Equation.
A problem with subject inclusion criteria is low-rate manual lifting. In Waters’s previous studies (Waters et al., 1999, 2011), one of the inclusion criteria was the following: “job in which manual lifting is performed with at least 25 lifts per day.” Such criterion derives from the definition of frequent job (Liles & Deivanayagam, 1984) used to calculate the Job Severity Index (JSI). In this study, the definition of frequent job is a job that requires at least 25 lifts per day, not less than 4.53 kg, and requires an exposure of at least 2 hr per day. In the RNLE (Waters, Putz-Anderson, & Garg, 1994), the value of the frequency factor is related to manual lifting duration. For infrequent lifting (i.e., frequency < 0.1 lift per minute), it will usually be sufficient to use the 1-hr-duration category; the frequency factor can be set equal to 1. In this case, the VLI value will be equal to the lifting task with a higher LI; therefore, the contribution of the other lifting tasks will be null.
In order to verify whether the VLI method for manual-lifting risk assessment can be applied to low-rate lifting, an analysis of the sample was carried out after excluding those subjects whose job had a lifting rate < 0.1 lift per minute, thus reducing the sample size from 2,374 exposed subjects to 1,803. A 24% reduction among exposed subjects occurred almost equally in the different VLI categories.
Tables 7 and 8 show the data obtained from such analysis for both VLI_EU and VLI_NIOSH. Compared to the previous analysis, no particular variations are visible. However, a less significant OR positive trend is to be highlighted together with a minor difference between the categories VLI < 1 and VLI < 2.
Association Between Variable Lifting Index (VLI_EU a ) and Occurrence of Acute Low-Back Pain in the Previous Year, Adjusted by Body Mass Index, Gender, and Age
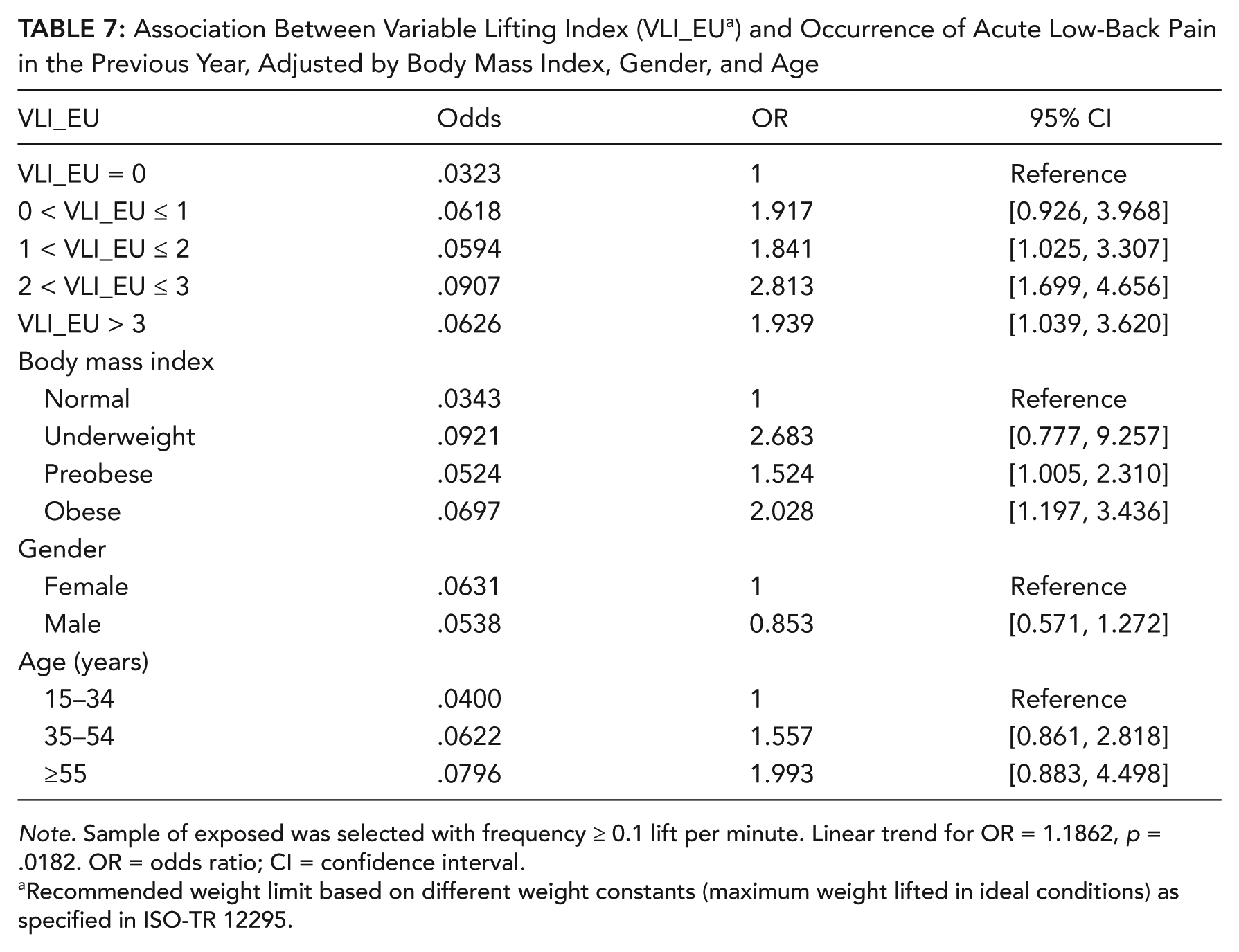
Note. Sample of exposed was selected with frequency ≥ 0.1 lift per minute. Linear trend for OR = 1.1862, p = .0182. OR = odds ratio; CI = confidence interval.
Recommended weight limit based on different weight constants (maximum weight lifted in ideal conditions) as specified in ISO-TR 12295.
Association Between Variable Lifting Index (VLI_NIOSH a ) and Occurrence of Acute Low-Back Pain in the Previous Year, Adjusted by Body Mass Index, Gender, and Age

Note. Sample of exposed was selected with frequency ≥ 0.1 lift per minute. Linear trend for OR = 1.1831, p = .0315. OR = odds ratio; CI = confidence interval.
Recommended weight limit based on maximum weight lifted in ideal conditions (23 kg) as specified in Revised NIOSH (National Institute for Occupational Safety and Health) Lifting Equation.
Discussion and Conclusion
It is undeniable, despite some limitations reported later, that this study highlights the existence of a “dose-response” relationship between VLI and acute LBP in the past 12 months.
When the definition of acute LBP causes absence from work or a strong limitation of motion of the lumbar spine, the prevalence on an annual basis is around 2% to 3%, males usually being more affected without a clear trend in relation to age (Abenhaim & Suissa, 1987; American National Standards Institute, 1993; Clemmer et al., 1991). In this study, the prevalence of acute LBP in the past year in subjects not exposed to manual handling of loads is about 3%.
The analysis shows that the risk of developing acute LBP increases linearly as the VLI levels go from 1.0 to 3.0, both for VLI_EU and VLI_NIOSH. The finding is based on a large sample with balanced risk exposure varying from VLI = 0 to VLI above 3.0.
Selection criteria may be among the main biases of this study. At the beginning of the study, workers’ representatives were asked to make a list of exposed subjects to make sure that at least 90% were entered into the database. Some participants were then removed from the sample due to a number of reasons. One company provided only clinical data, leaving out data on risk assessment, which caused 101 participants to be removed. Another 1.8% of the exposed subjects (equaling 61 participants) from the other companies were removed because they did not undergo any health checks. Subjects who had injured themselves during the past year, regardless of the modality, were also removed. The removal of exposed subjects was due to onsite inspections revealing that a great number of exposed subjects did not perform daily lifts, whereas, on the contrary, many nonexposed subjects did perform occasional pushing, pulling, or handling activities (from once to three to four times a week). Nonexposed subjects were also removed if they did not have the possibility to switch autonomously between sitting and standing position; Waters et al. (1999, 2011) highlighted how the sustained use of a seated posture can be a possible selection bias. Womersley and May (2006), too, underlined that LBP rates may be higher than in a truly unexposed population.
Because the VLI is methodologically derived from the RNLE (Waters et al., 1994), it should have the same limits of applicability. Some restrictions have been considered in this study, such as lifting/lowering for more than 8 hr per shift, while seated or kneeling, in a restricted workspace, or with unstable objects and whether the pulling, pushing, and carrying activity could be considered residual compared to lifting. Other restrictions were not considered, some of which are difficult to assess in current practice, such as the speed of movement or the coefficient of friction between the soles and the floor, and for this reason, they were not controlled in this study.
The main causes of inapplicability of the method are the following: objects lifted with one hand or simultaneously by two operators, exceeding the maximum horizontal distance (H), and handling an object above the height of 175 cm. The first two violations (one-handed lifts and two operators lifting together) are also mentioned both in ISO 11228 Part I and in the European Standard EN 1005 Part II. Regardless of the ISO and European standards, with respect to one-handed lifts, biomechanical studies agree that the relative load on the spine can be greater when lifting with one hand (instead of two). Also, the pattern of biomechanical overload on the lumbar spine changes, as compression forces are approximately equal to those observed when lifting with two hands, and anterior-posterior shear decreases and lateral shear increases (Marras, 2008; Marras & Davis, 1998; Mital, Nicholson, & Ayoub, 1997).
As for team lifting (two people), indications from European Standard EN 1005-2 were followed (RWL multiplied by 0.85 and lifted weight divided by 2). The literature review revealed partly contradictory studies on the subject (Karwowski & Mital, 1986; Marras, 2008; Marras et al., 1999; Rice, Sharp, Nindl, & Bills, 1995; Sharp, Rice, Nindl, & Mello, 1995), and only one study (Dennis & Barret, 2002) demonstrated a significant reduction in L4/L5 torque and compression force by about 20% during team lifting compared to individual lifting. Many factors should be considered in the assessment of team lifts, yet coordination of the movements appears to be the most important (Marras, 2008). It is possible, therefore, that the correction applied in this study in order to calculate the VLI does not correspond to the actual biomechanical strain of the lumbar spine.
For what concerns violations of the horizontal factor and vertical location factor, the results presented in this study seem to refute even this limit applicability. Such considerations indicate that caution is required when rejecting the applicability of the NIOSH method, at least the VLI, in those work conditions where the LI may over- or underestimate the extent of physical stress.
Although the category 1 < VLI < 2 shows a statistical difference compared to that of unexposed subjects, its comparison with the category 0 < VLI < 1 shows no remarkable differences, especially when jobs with a handling frequency below 0.1 lift per minute are excluded from the analysis. This result may be due to the damage variable used; jobs with a low lift rate may, in fact, cause a lumbar spine overload that could possibly lead to acute LBP. Such effect is not completely explained by the damage variable used in this study, as Waters’s study showed a difference between these two LI or CLI categories similar to that highlighted in this study, despite damage variables being different.
For what concerns the category 2 < VLI < 3, a higher OR is clearly noticeable in all analyses, whereas the category VLI < 3 does not show a further increase. This aspect, which is probably due to the “healthy worker effect” (Checkoway, Pearce, & Crawford-Brown, 1989), can be seen in many epidemiologic studies. To explain this trend, Waters et al. (2011) hypothesized a “survivor” effect because the mean years spent on the job increased as the risk index did. However, in this set of data, all exposure categories reported virtually no differences in mean years on the current job. Another possible explanation may derive from the fact that during the research, one of the companies had to rely on “defensive” job security agreements due to financial issues, which caused a reduction of workdays in the past year: About 10% of the exposed subject belonging to the category VLI > 3 worked around 170 days.
Despite these considerations, the positive value of the observed linear trend is unquestionable.
Data referring to the cumulative mass need in-depth examination, as their range appears to be quite wide in the different VLI categories (both VLI_EU and VLI_NIOSH). This finding may mean that the episodes of acute LBP are to be ascribed more to lifting heavy loads at low frequency, handling geometry, and work organization than to the total weight lifted in a shift. Despite requiring further examination, this aspect underlines the theoretical effectiveness of LI, CLI, and VLI. There does exist, however, an ever-increasing interest in the identification of tools able to evaluate a cumulative low-back load that could be used to estimate the risk of occurrence of LBP (Coenen et al., 2013). It would be interesting, in future studies, to investigate a possible link between the RNLE, adjusted for cumulative mass, and LBP.
It needs to be underlined, however, that back in 1962 the International Labour Office suggested, for occasional weight lifting, differentiated weight limits depending on age and gender. Several authors emphasize the necessity to take such individual variables into account preventively (Adams, McNally, & Dolan, 1996; Garg, 1991; Jäger & Luttmann, 1999; Jäger, Luttmann, & Laurig, 1999; Marras, 2008; Mital et al., 1997).
With regard to such aspects, the approach defined by the ISO (2014; ISO-TR 12295) appears to be better intended to protect, at least in terms of prevention, although the results reported in this study do not allow to define clearly which load constant is to be used in the calculation of the risk index in relation to age and gender differences.
Considering the multivariate analysis, neither VLI_EU nor VLI_NIOSH reported effect modification due to gender and age. As for VLI_EU, it might be a question of overfitting. Nonetheless, it is still surprising how the calculation of VLI_EU—with load constants adjusted for age and gender—and that of VLI_NIOSH—with an unvaried load constant—give equal results.
In previous validation studies on LI (Lu, Waters, Krieg, & Werren, 2014; Waters et al., 1999, 2011), psychosocial factors were also considered as confounders. In particular, job satisfaction was the only confounder found to be statistically significant. However, although the literature highlights the importance of psychosocial factors in determining LBP (Hoogendoorn, Van Poppel, Bongers, Koe, & Bouter, 2000; National Academy of Sciences & National Research Council, 2001; Sterud & Tynes, 2013; Widanarko, Legg, Devereux, & Stevenson, 2015; Yu, Lu, Gu, He, & Wang, 2012), few studies consider both aspects at the same time: biomechanical overload and psychosocial factors. This aspect is one of the limitations of this study, though psychosocial factors would be important when levels of exposure to manual material handling are low (Marras, 2008).
While carrying out the research, it became evident how easy it is to simulate preventive actions with the purpose of reducing the risk, also thanks to free online software. This software is an essential tool for those who need to have their cost-benefit analysis evaluated by the management.
The findings of this study show that the VLI method can be used to assess the risk of acute LBP, although further studies are needed to confirm the outcome and to define better VLI categories.
Key Points
On the basis of either the EU or National Institute for Occupational Safety and Health recommended weight limit, as the Variable Lifting Index (VLI) increased from 1.0 to 3.0, the risk of acute low-back pain (LBP) increased.
The exposure of VLI above 3.0 needs further research for validating its effect on the development of LBP.
Among personal risk factors, body mass index was significantly associated with acute LBP.
Footnotes
Acknowledgements
This study was partially supported by Azienda Unità Sanitaria Locale Imola (Italian National Health Service) and by Associazione Ricerca, Prevenzione ed Ergonomia–ARPE (a nonprofit organization), Imola, Italy. The authors would like to thank Aschieri Antonio, Arfini Giuseppe, Bruno Ricci, Cerbai Roberto, Cermesoni Maurizio, Fontana Luciana, Galli Paolo, Missere Maurilio, Nicoletti Sergio, Pezzuto Enzo, Pompei Iliana, Quadrini Giacomo, Tisato Silvia, Venturi Silvia, Bulgarelli Fabio, Porati Sara, Baldiserri Giulia, Rinaldini Italo, Ponzio Ennia, Vidari Fabio, Franco Modeo, Giuseppe Cappelli Catalano Giulia, Rigovacca Luigi, Monopoli Leonardantonio, Malengo Marco, Piero Patane, Diano Claudio, Palmieri Matteo, for their assistance in collecting data. The authors are grateful to Enrico Occhipinti, Enrique Alvarez Casado, Olga Menoni, Marco Cerbai, Marco Placci, Giulia Stucchi, and Elisa Stucchi for their suggestions.
Natale Battevi graduated in medicine and surgery, and specialized in occupational medicine (University of Milan, Italy) and medical statistics (University of Pavia, Italy). He works at the Department of Occupational and Environmental Preventive Medicine, Fondazione Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy. His main field of research includes the study of simplified methods for assessment of risk of biomechanical overload and, for several years, searching for ergonomic solutions for the prevention of musculoskeletal disorders.
Monica Pandolfi graduated in science of occupational safety and health protection and environment (University of Ancona, Italy) and specialized in science of health professions for preventive care (University of Milan, Italy). As a PhD student at University of Milan, she focused on occupational ergonomics and industrial hygiene.
Ivan Cortinovis graduated in statistics. He has worked since 1979 at Laboratory GA Maccacaro of the Department of Clinical Sciences and Community Health (University of Milan). As medical statistician, he has worked with several research groups on perinatal preventive medicine, on children growth, and on the studies for early detection of diseases.