
Abstract
Objective
The aim was to review the biomechanical origins of occupational shoulder damage, while considering the complexity of shoulder mechanics and musculoskeletal consequences of diverse task demands.
Background
Accessible measures of physical exposures are the primary focus of occupational shoulder assessments and analyses. This approach has led to guidelines and intervention strategies that are often inadequate for mitigating shoulder disorders amongst the complexity of modern workplace demands. Integration of complex shoulder mechanics into occupational assessments, analyses, and interventions is critical for reducing occupational shoulder injury risk.
Method
This narrative review describes shoulder biomechanics in the context of common injury mechanisms and consequent injuries, with a particular focus on subacromial impingement syndrome. Several modulators of shoulder injury risk are reviewed, including fatigue, overhead work, office ergonomics considerations, and pushing and pulling task configurations.
Results
Relationships between work requirements, muscular demands, fatigue, and biomechanical tissue loads exist. This review highlights that consideration of specific workplace factors should be integrated with our knowledge of the intricate arrangement and interpersonal variability of the shoulder complex to proactively evaluate occupational shoulder demands and exposures.
Conclusion
A standard method for evaluating shoulder muscle exposures during workplace tasks does not exist. An integrated approach is critical for improved work design and prevention of shoulder tissue damage and accompanying disability.
Application
This review is particularly relevant for researchers and practitioners, providing guidance for work design and evaluation for shoulder injury prevention by understanding the importance of the unique and complex mechanics of the shoulder.
Although many occupational shoulder assessments and analyses pragmatically focus on accessible external measures of physical exposures and their interpretation, the effects of these exposures on vulnerable tissues and their specific mechanical responses are typically either not estimated or neglected altogether. This has led to generic guidelines and interventions that are both sparsely supported and frequently inadequate to respond to the challenges and nuanced musculoskeletal risks of modern work. Indeed, the complexity of shoulder mechanics combined with intricacies of pathophysiology prevents simplified interpretation of the localized tissue demands based on broadly defined task requirements. However, a sufficient evidence base exists to identify the biomechanical origins of occupational shoulder damage.
A Brief Review of Shoulder Biomechanics
The shoulder complex has four articulations, which include three synovial joints (sternoclavicular, acromioclavicular, and glenohumeral) and a unique gliding scapulothoracic interface. A fundamental understanding of shoulder mechanics is predicated on recognizing a trade-off between kinematic flexibility and joint stabilization, particularly of the glenohumeral joint. This dichotomy is explored extensively in a topical review (Veeger & van der Helm, 2007).
The extraordinary mobility and postural flexibility of the shoulder is enabled by relatively low intrinsic restriction, including a shallow joint fossa on the scapula, known as the glenoid. This anisotropic fossa allows substantial joint articulation, particularly anteriorly, enabling countless manual and bimanual activities that are essential for human life and work. Indeed, modern humans derive much of their diverse arm functionality from the construction of the shoulder complex (Larson, 2007), including the ability to throw objects rapidly (Roach & Lieberman, 2014). Orthopedic directional stability of the glenohumeral joint has been reported (Lippitt et al., 1993) and incorporated into biomechanical shoulder models to reflect this unique aspect (Dickerson et al., 2007). The relatively scant and posture-sensitive contributions (Matsen et al., 1994) of the ligamentous components of this joint also enable mobility, but concurrently combine to demand stabilization from other contributors, most notably muscular action. Other mechanisms include adhesion in the glenohumeral joint, intra-articular pressure, labral deformation and associated compression-concavity, proprioception, and articular version. Matsen et al. (2004) provide an extended review of these complementary stabilizing mechanisms.
Recognizing the importance of shoulder musculature in maintaining stability, it is crucial to consider how muscle capacity and actions vary. The spatial arrangement of the shoulder musculature assists the identification of its various functions and potentially dysfunctional behaviors, particularly those that insert on the proximal humerus (such as the rotator cuff and deltoid). Shoulder region muscular moment contributions are highly posture dependent, due to a combination of short moment arms caused by insertions close to rotational axes and the highly mobile shoulder complex. Most reported geometric data focus on elevation capability. In a resting posture, both the supraspinatus and middle deltoid have abduction moment arms; the supraspinatus is more active in initial abduction, while the middle deltoid contributes progressively more as elevation increases and its abduction moment arm grows (Ackland et al., 2008; Howell et al., 1986; Inman et al., 1944; Otis et al., 1994). Experimentally measured values confirm this concept (Ackland et al., 2008; Liu et al., 1997); the maximum moment arm of the supraspinatus occurs during early flexion and abduction (<5°), while the anterior and middle deltoid demonstrate increasing moment arms with higher degrees of elevation (Ackland et al., 2008). Additionally, the infraspinatus moment arm increases rapidly with abduction before plateauing near 15° of elevation, while the subscapularis moment arm decreases to 0 mm by 60° of elevation. The dynamic abilities of muscles during elevation relate to injury mechanisms, as capability shifts, modifying both overall and specific muscular actions. In addition to elevation, muscle moment arms are differentially sensitive to humeral axial rotation (Liu et al., 1997), with a reduction in abduction moment arms for both the supraspinatus and middle deltoid with deviation from neutral rotation. This postural sensitivity is also revealed by muscle activity responses to multiplane elevation. The upper trapezius, middle and posterior deltoid, and supraspinatus are more highly activated during initial ranges of abduction compared to flexion (Sigholm et al., 1983), following which higher activity is elicited in either plane of movement with increased elevation (Tse et al., 2016; van der Helm, 1994a). The anterior deltoid is more active in flexion than abduction, and infraspinatus is equally active in both planes. Overall, increased elevation yields higher muscle activity, likely accelerating fatigue responses (as in Section “Overhead Work”). In summary, confirmation of the intrinsic functions of shoulder muscles over the range of multiplane elevation is critical for understanding potential mechanisms of injury and the impact of work characteristics on muscular responses and capacity. The take-home message is that it is dangerous to assume consistent function for any muscle that crosses the glenohumeral joint, which subsequently complicates occupational exposure interpretation.
Characteristics of Shoulder Injury Mechanisms
Applying injury mechanism concepts from other body regions, particularly the low back (e.g., compression and shear tolerance limits) and distal upper extremity (with fewer degrees of freedom), is ineffective when assessing shoulder demands due to persistent differences in the nature of observed pathologies. Initial attempts to prevent occupational shoulder overexposure were either based on strength comparisons at a simplified shoulder joint (Chaffin, 1997; Kumar et al., 1988; Stobbe, 1983), setting psychophysically acceptable limits (Mital et al., 1997; Snook, 1978; Snook & Ciriello, 1991), or through postural assessments that incorporate rough estimates of force requirements (McAtamney et al., 1993). This was borne perhaps from an historical focus on the prevention of lower back disorders, particularly of the vertebral endplates and annulus related to traumatic or high-exertion overexposure events. The directionality and susceptibility to failure of the critical “weakest links” in each body region, however, defy simple transfer of concepts. Many shoulder injuries are to soft tissue (van der Windt et al., 1996) and are likely chronic in nature, compelling a cumulative exposure and response approach. This is not to downplay the many soft tissue injuries that occur across the body, but to highlight the predominance in the shoulder in particular of tendinous damage.
The rotator cuff muscles (supraspinatus, infraspinatus, subscapularis, teres minor) are highly vulnerable to damage due to the considerable functional and stabilization demands required during upper limb tasks. The prevalence of full-thickness rotator cuff tear increases with age, with over half the population suffering a tear by age 60 (Milgrom et al., 1995). Despite this prevalence, the absence of relevant tissue tolerance data, particularly for the supraspinatus tendon, has precluded setting exposure limits intended to protect soft tissues. Persistent debates regarding delineating shoulder occupational risk have produced few reliable guidelines for its avoidance. The United States National Institute for Occupational Safety and Health (NIOSH; Bernard, 1997) has suggested avoidance of work tasks requiring more than 60° of arm elevation. Additionally, a median upper arm velocity of 60°/s over an 8-hr shift has been recently suggested as a recommended threshold limit to protect workers from occupational upper limb disorders (Balogh et al., 2019). Animal models have attempted to establish pathomechanics of supraspinatus damage, in particular for longitudinal loading (Derwin et al., 1994; Gimbel et al., 2004), and proposed fatigue failure mechanisms due to repetition (Gallagher & Heberger, 2013) exist, but these findings have not been translated into actionable exposure thresholds for occupational purposes, in part due to the conundrum of establishing dose–response relationships.
Part of the difficulty of defining prospective adjuvant approaches to shoulder injury prevention stems from the nonspecific definition of occupational shoulder disorders and the multifactorial supposed workplace triggers. Indeed, generalized shoulder pain and specific pathologies are often linked to differential risk factors. Generalized shoulder pain has shown an association with several psychosocial factors, including insufficient colleague support (Beach et al., 2012), psychological distress (Nahit et al., 2003), and high job demand. A summary of additional psychosocial modulators can be found in Linaker and Walker-Bone (2015), though the authors emphasize that resolution of specific associations is generally low. Conversely, studies examining specific associations between mechanical loading factors and subacromial impingement and rotator cuff damage have identified several mechanisms, including both occasional and sustained arm elevation (see Section “Overhead Work” for additional details), repetitive work (Roquelaure et al., 2011; van Rijn et al., 2010), vibration (Charles et al., 2018), and manual handling (including pushing and pulling; Andersen et al., 2007), but a combination of exposures appears to have an accumulative risk increase (Linaker & Walker-Bone, 2015; Pope et al., 2001). Specific following sections of this review highlight some of the reasons for these particular risks in biomechanical terms.
The Special Relevance of the Subacromial Space
The subacromial space (acromio-humeral interval; SAS) is formed by articulations of the humerus, scapula, and clavicle. The superior surface of the humeral head comprises the inferior aspect of the SAS while the coracoacromial arch, specifically the anterior third of the acromion and the coracoacromial ligament, comprises the superior aspect (Neer, 1972). With the arm in a neutral resting posture, the superior–inferior (SI) width of this space ranges from 6 to 14 mm, and reduces to as little as 2–5 mm during multiplanar elevation (Bey et al., 2007; Cotton & Rideout, 1964; Golding, 1962; Graichen et al., 1999; Weiner & Macnab, 1970). Soft tissues of varying thickness reside within the space, including the supraspinatus tendon, subacromial bursa, long head of the biceps tendon, and shoulder capsule (Michener et al., 2003). The combined thickness of these tissues varies considerably in the population, and in healthy individuals with the arm at rest, they can occupy more than half of the available space (Michener et al., 2015). Thus, reduction of the SAS, increased thickness of the subacromial tissues, or both can pose elevated risk for tissue compression, leading to the development of subacromial impingement syndrome (SAIS) and tissue damage. However, it is important to consider that arm postures and their related musculoskeletal geometric changes critically modify SAIS risk assessment, as, although the minimum SAS width may be smaller at higher elevation angles, it may not pose high risk for rotator cuff impingement. Researchers have demonstrated that at elevation angles exceeding approximately 70°–90°, the minimum SAS width vector passes lateral to the supraspinatus tendon (Giphart et al., 2012; Graichen et al., 1999; Graichen, Bonel, Stammberger, Haubner, et al., 1999). This implicates midrange elevation as the most critical range for tissue compression and prompts consideration of kinematic alterations within this range (Lawrence, Braman, Laprade, et al., 2014; Lawrence, Braman, Staker, et al., 2014). The term SAIS as a clinical diagnostic label has been the topic of much controversy in recent literature (Braman et al., 2014; Derwin et al., 1994; Lewis, 2011). Historically, acromial shape was implicated as instrumental in rotator cuff pathology and thus a SAIS diagnosis was considered valid only if treated with surgical subacromial decompression. However, more recently, alternate hypotheses for rotator cuff damage have been suggested, which include both intrinsic and extrinsic mechanisms of SAIS, with associated interventions (Braman et al., 2014; Lewis, 2011; Seitz et al., 2011).
Supraspinatus Tendinopathy Origins
An ongoing debate over the pathogenesis of rotator cuff tendinopathy relates to the origins of the tissue degradation, namely whether the mechanism is intrinsic or extrinsic. An excellent review of the mechanisms can be found in Seitz et al. (2011), but the fundamental concepts are summarized here. While an intrinsic mechanism postulates that rotator cuff damage occurs through processes related to tendon morphology and age-related degeneration, an extrinsic mechanism attributes tissue damage to mechanical compression of the vulnerable tissues through altered upper limb kinematics and concomitant muscle responses (Seitz et al., 2011). Mechanical transverse tendon compression in concert with longitudinal compression is considered particularly problematic due to the innate vulnerability of the collagenous structure to transverse load (Cook & Purdam, 2012), which is likely exacerbated by longitudinal twist of the supraspinatus in many postures (Nakajima et al., 2004). Considerable tendon matrix degenerative changes occur consequent to fatigue overload generally, supporting a chronic overload mechanism (Shepherd & Screen, 2013). Ergonomic engineering interventions must necessarily focus on the modifiable aspects of the workspace and task performance, thus affecting exposures and subsequently extrinsic exposure modulators. The remainder of this review concentrates therefore on occupational extrinsic mechanisms.
Muscular Fatigue as a Candidate Precipitator of Occupational Rotator Cuff Disease
Muscular fatigue has been identified as a key mediator of shoulder kinematics that both increases and modifies challenges to shoulder structures. Two external fatigue-initiated mechanisms have the potential to reduce the width of the SAS. These mechanisms are (1) acromion rotation through scapular downward rotation, anterior tilt, and internal rotation (protraction) encroaching on the space from above (top-down); and (2) superior translation of the humeral head with respect to the glenoid cavity of the scapula, encroaching on the space from below (bottom-up). Evidence for these mechanisms is mixed, but themes emerge. Deleterious consequences of muscular fatigue for scapular kinematics and concomitant scapular dyskinesis and their influence on the width of the SAS are not universally reported. Tsai et al. (2003) reported that during humeral elevation in the scapular plane changes to scapular kinematics occurred that were consistent with SAS width reduction, promoting the development of SAIS. In conjunction they also found that the level of muscle fatigue, as quantified through reductions in muscle strength, correlated with increased anterior scapular tilt (Tsai et al., 2003). Conversely, results of other studies identified varying combinations of impingement sparing scapular rotations, which increased SAS width (Chopp et al., 2011; Chopp-Hurley, O’Neill, McDonald, et al., 2016; Ebaugh et al., 2006; McQuade et al., 1998; Tse et al., 2016). Yet other fatigue protocols yielded no measurable changes to scapular kinematics (Chopp et al., 2011; Noguchi et al., 2013). Compounding the complexity of fatigue-related kinematics further is the extensive interpersonal variability in responses to the same fatigue protocol. Recent work demonstrated substantial variability in the kinematic response of the scapula to the perturbation of muscle fatigue, both between participants and within the same participants across multiple test days (Chopp-Hurley, O’Neill, McDonald, et al., 2016; Mulla et al., 2018; Noguchi et al., 2013).
Apart from the interpersonal variability related to exposure-related responses, factors related to innate, personal, or morphologic factors can elevate the risk of upper limb disorders. Specifically, both increased age and body mass index are demonstrably related to upper limb pain and disorders (Miranda et al., 2001; Roquelaure et al., 2009). In fact, the risk of shoulder pain was nearly 3 times higher in the oldest grouping of participants, compared to the youngest group (Miranda et al., 2001). The authors attributed this finding to age-related degeneration. Bone and soft tissue geometry are also highly variable in the population, with research showing that SAS-reducing bony morphologic variants exist even among a young healthy population (Chopp-Hurley, O’Neill, & Dickerson, 2016). As well, the multiple scapular muscle attachments vary across persons, creating variable force production capabilities (Chopp-Hurley et al., 2014; Picco et al., 2010). These differences could lead to variable muscle fatigue patterns and thus variability in resulting scapular kinematics.
Fatigue-induced superior humeral head translation has been more consistently reported. Superior humeral head translation with respect to the glenoid occurs with muscle fatigue and arm elevation (Chen et al., 1999; Chopp et al., 2010; Chopp-Hurley, O’Neill, McDonald, et al., 2016; Cote et al., 2009; Teyhen et al., 2008). Prior to a fatigue protocol, increasing arm elevation angle resulted in superior humeral head migration during the first 45° of glenohumeral elevation, succeeded by a return to a more centralized position on the glenoid for the remaining 90° of elevation (Chopp et al., 2010). Following a fatigue protocol, superior translation persisted after 45° of elevation (Chopp et al., 2010). Measuring humeral head translation is challenging due to its subcutaneous motion and it is typically performed radiographically, making it limited to planar measurements. Recently, computational models have refined volumetric aspects of this mechanism (Chopp & Dickerson, 2012; Chopp-Hurley, Langenderfer, et al., 2016). In a simulation qualifying SAS changes associated with each fatigue mechanism (top-down, bottom-up) independently and in combination, humeral head migration generally decreased the SAS and scapular kinematics generally increased the width of the SAS, across 36 unique scenarios (Chopp & Dickerson, 2012), indicating that rotator cuff fatigue in particular is more problematic. More recent simulations suggest that humeral head translation may dominate SAS width at low elevation, due to the high deltoid shearing potential, while scapular changes become more prominent at higher elevation angles (Chopp-Hurley, Langenderfer, et al., 2016). The combined implication of these many studies is evidence that humeral translation, which is a consequence of rotator cuff fatigue, dominates SAS reductions subsequent to fatigue.
A limitation of investigations of these two mechanisms in isolation is that the majority of these studies did not directly measure the width of the SAS, and thus changes were inferred from changes to scapular and humeral kinematics. Chopp-Hurley, O’Neill, McDonald, et al. (2016) reported no significant mean changes to SAS width following a fatigue protocol and no significant fatigue–elevation angle interactions. However, on closer inspection between 39% and 57% of the participants exhibited disadvantageous fatigue-related changes. Small changes in SAS width can have important clinical implications. The occupation ratios of the combined thickness of subacromial tissue divided by the minimal SAS ranged from 21.6% to 108.9% (Chopp-Hurley, O’Neill, & Dickerson, 2016), indicating that even small changes to the width of the space should be considered. Conversely, Maenhout et al. (2015) examined SAS width in overhead athletes using ultrasound and found increased SAS width following a fatigue protocol. This variability may arise from the multifactorial nature of SAS changes, which was confirmed in a computational model where the variability in kinematic and morphologic parameters influenced predicted SAS variability (Chopp-Hurley, Langenderfer, et al., 2016). This agreed with the previous findings of variability in scapular changes following fatigue and helped explain differential injury risks observed between different workers performing the same tasks.
Upper limb posture can also modify the width of the SAS concomitantly with fatigue mechanisms. Humeral external rotation typically increases the width of the space (Longo et al., 2017), whereas humeral elevation decreases the width of the space (Chopp et al., 2010; Chopp-Hurley, O’Neill, McDonald, et al., 2016) in both nonfatigued and fatigued shoulders, though the decreased width persists at higher elevations in fatigued shoulders. Although they did not directly measure the SAS width, Picco et al. (2018) measured decreased posterior tilt in females during elevation. As posterior tilting generally increases the width of the SAS, reductions in tilt may contribute to the greater incidence of shoulder pathologies reported in females. These known muscular fatigue-induced SAS width influencers (scapula orientation and humeral translation changes) overlay the natural width changes associated with arm elevation (Figure 1). Overall, repeated humeral elevation to fatigue emerges as a pathway to tissue compression and subsequent tendinous damage.
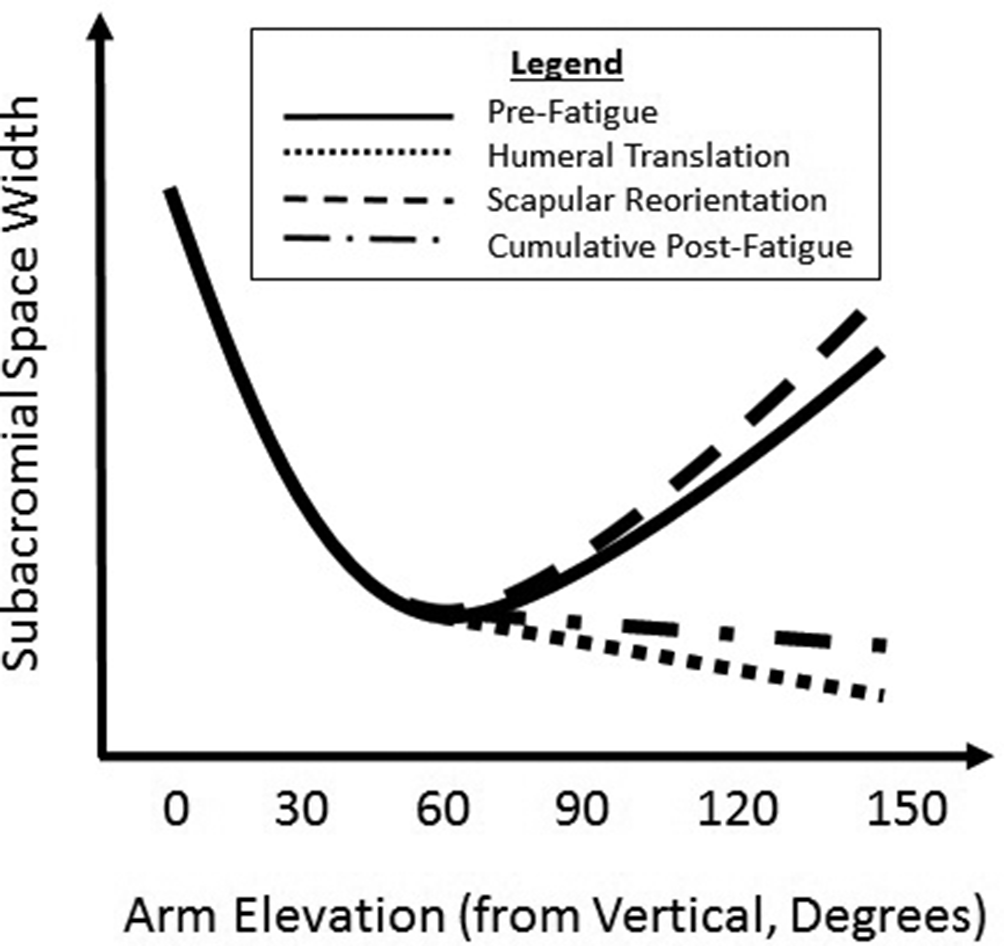
Conceptualized mechanisms of fatigue-induced kinematic compensations on subacromial space reduction while elevating the arm. In the initial phase of arm elevation (0–60°), the space narrows with relative humeroacromial motion regardless of fatigue state. As the arm elevates above 60°, the space widens in a nonfatigued shoulder (solid line); however, in a fatigued state, the humerus translates superiorly (dotted line), while the scapula reorients to increase the space (dashed line), resulting in a net decrease in the width of the space (dash-dot line). The major implication is that there is a substantial decrease in the space in a highly elevated fatigued shoulder.
Contextualization of Primary Mechanisms Within Occupational Scenarios
These general insights inform key risks to musculoskeletal shoulder health across scenarios, but three will be highlighted in this review.
Overhead Work
Working overhead has been identified as a musculoskeletal risk factor in field studies across industrial sectors. A systematic review evaluating the relationship between physical and psychosocial exposures with the prevalence of common occupational shoulder impairments highlighted both upper arm elevation >90° and working above shoulder height for ≥1 hr/day as risk factors for SAIS (OR, 1.27–4.70) (van Rijn et al., 2010). Similarly, an epidemiology study assessing physical risk factors and upper limb disorders among assembly line workers showed that for every 1% of time with the arms working above 90°, there was a significant (7%) increase in neck/shoulder symptoms observed (Gerr et al., 2014). In particular, risks of developing a shoulder disorder in automotive assembly are 2–3 times higher in jobs that require these overhead postures in a work cycle (Palmerud et al., 2000). In addition, work with overhead requirements relates to shoulder pain, discomfort, and limited productivity for construction workers (Rosecrance et al., 1996), orchard workers (Sakakibara et al., 1995), carpenters (Astrand et al., 1968), and simulated field welding (Herberts & Kadefors, 1976; Järvholm, Palmerud, Kadefors, et al., 1991). Recently, Loew et al. (2019) compared symptoms, function, and rotator cuff tear prevalence in experienced painters (mean, 21 years) whose work involved overhead arm postures 63.6% of the time. Compared to age-matched controls, painters had restricted range of motion, greater functional symptoms, and reduced strength, in addition to higher rotator cuff tear prevalence (OR, 11.3) (Loew et al., 2019). Though the specific work done in all of these applications varies, the common factor is the existence and challenge of overhead work and its relatedness to negative health outcomes.
Additional fundamental investigations into overhead working tasks across industrial groups have supported these specific findings. Bjelle et al. (1979) found that about 69% of monitored shoulder pain patients described being required to work at or above shoulder level and later suggested that working with hands above shoulder level may lead to disorders of the shoulder through an increase in muscular workload (Astrand et al., 1968). When comparing work at shoulder level to that below across several industrial worker groups, Hagberg and Wegman (1987) found an odds ratio of 11 for the incidence of rotator cuff tendonitis for elevated work. Evidence also suggests that both current and lifetime accumulated exposures to work above shoulder height are causal factors for disabling and nondisabling shoulder pain, as well as supraspinatus tendonitis (Svendsen et al., 2004). These cross-sectional studies demonstrate that while overhead work-related health issues might be more pronounced in some occupations, they are also present in the working population at large.
Some disparity exists regarding the magnitude of elevation that is problematic. For example, the notion that musculoskeletal injury occurs with severe shoulder flexion or abduction above 90°, but not below (Punnett et al., 2000), contrasts with other findings (Järvholm, Palmerud, Karlsson, et al., 1991; Järvholm, 1988). Upper limb muscular load and intra-articular pressure in the glenohumeral joint, both measures of exposure, increase with elevation until 90°, but then decrease in the above 90° range, a range which has been identified as problematic by Punnett et al. (2000). Recent evidence investigating the relationship between physical exposure and upper limb disorders found that upper arm velocity, rather than posture, was associated with upper limb diagnoses (Balogh et al., 2019). They attributed not finding an association with posture to the participant sample, stating that overhead work was not common in the included occupations. Thus, although no definitive elevation magnitude has been unequivocally tied to injury, routinely performing overhead work appears to present an increased risk of developing shoulder disorders.
Office Ergonomics
Office work, particularly computer use, is commonly associated with shoulder pain or injury (Ardahan & Simsek, 2016; Jensen et al., 2002). General factors that increase risk of MSD development in the office space include gender, amount of time spent using the computer (amount daily and/or years working), specific tasks performed (i.e., data entry, graphics/design), lack of knowledge about ergonomics, and inadequate rest breaks (Ardahan & Simsek, 2016; Ayanniyi et al., 2010). Office workers often maintain static postures while performing low-load, repetitive tasks. These work tasks can lead to fatigue development and overuse of specific muscles and tissues. For example, upper limb muscle fatigue, particularly for trapezius and anterior deltoid, and elevated ratings of discomfort were elicited with workstation heights above elbow height compared to below (Lee et al., 2015). Stretching breaks can be an effective intervention to reduce self-reported upper limb pain (Jepsen & Thomsen, 2008). Ergonomic interventions to modify desk configurations may reduce the risk of MSD development. Factors that may modulate muscle demand and perceived fatigue or pain include keyboard position, mouse position, mouse design, desk shape and adjustability, and sitting posture (Alavi et al., 2016; Kotani et al., 2007; Rempel et al., 2006; Sako et al., 2017; Straker et al., 2008). An area of particular interest to shoulder MSD development is the use of forearm rests while performing computer tasks. Forearm support has been found to both decrease or increase shoulder pain in computer workers (Aarås et al., 2001; Cook et al., 2008; Rempel et al., 2006), suggesting interactions with other desk configuration parameters. Without forearm supports, the shoulder musculature must endure static loading to maintain typing postures, but supports in a poor position can lead to mechanical contact stresses and elevated shoulder postures. Both scenarios can contribute to shoulder MSD development over time. With advancements in technology, computer work is no longer confined to an office, creating new ergonomic challenges. Portable computers (i.e., laptops or tablets) can be used on any surface and, if not properly configured, can create opportunities for awkward postures leading to overloading of the shoulder tissues and subsequent MSD injuries. Using a modified keyboard for example can reduce the associated shoulder pain (Malińska & Bugajska, 2010), likely due to improved typing postures. Police officers, in particular, are required to use mobile data terminals (MDT) within their cruisers. Enabling self-selected MDT placement within the cruiser reduced shoulder demands in a laboratory simulation study (McKinnon et al., 2012). Overall, the risk factors for MSD development during office and computer tasks vary by body region (Alavi et al., 2016), making their prevention a complex challenge.
Pushing and Pulling
Pushing and pulling exertions are commonly performed across many different industries and place demands on the shoulder complex. The design of pushing and pulling tasks in the workplace impacts workers capabilities, joint loads and muscle activity, and perceived comfort and exertion levels. Pushing and pulling capabilities are impacted by movement speed, hand locations, exertion direction, angle of pull, and upper extremity and whole body postures (Chow & Dickerson, 2009, 2016; Cudlip & Dickerson, 2018; Garg & Beller, 1990; Lin et al., 2013). Increasing humeral abduction angle reduces pulling strength capabilities by up to 30% (Cudlip & Dickerson, 2018), suggesting that not only is task design important but allowing workers to self-select postures can be effective in increasing their capabilities. These design parameters may be more important for female workers, who have less pushing and pulling strength than males (Chow & Dickerson, 2016; Lin et al., 2013). These capabilities are also reflected in the required muscle activation during submaximal pushing and pulling. Shoulder muscle activity can be interpreted as a reflection of the internal loads. Muscle activity during pushing and pulling tasks is affected by hand location and posture, force direction, and required force level (Alasim et al., 2019; Bennett et al., 2011; Brookham et al., 2010; McDonald et al., 2012). Further, elevated muscle activity is present not only in the muscles responding to external load demands, but also in glenohumeral and scapular stabilizing musculature (McDonald et al., 2012). Repetitive pushing and pulling tasks can therefore lead to muscle fatigue development, which subsequently impairs shoulder stability maintenance and contributes to injury development. Similarly, perception of comfort and effort is impacted by task design factors such as hand location, pulling angle, pulling speed, and exertion direction (Alasim et al., 2019; Garg & Beller, 1990). As well, a dose–response relationship between occupational pushing and pulling exposure and shoulder complaints has been identified, with high exposure related to shoulder ache, pain, and discomfort, in addition to pain intensity and disability (Hoozemans et al., 2002).
Distillation of Current Knowledge and a Call for Action
Strong evidence suggests relationships between work requirements, muscular demands, fatigue, and biomechanical tissue loads, motivating more targeted and effective physical work surveillance methods. Injury mechanisms are a combination of the intricate arrangement of the shoulder complex, tendon responses, and modern occupational demands, of which several were highlighted in this review. A potentially valuable focus for future research is the deliberate development of a reliable means of quantifying shoulder muscle, tendon, and joint loads for both existing and future tasks. Although attempts have been made to quantify and estimate shoulder muscular activity using computational models (Charlton & Johnson, 2006; Chopp-Hurley et al., 2014; Dickerson et al., 2007; Dul, 1988; Garner & Pandy, 2001; Högfors et al., 1987, 1991, 1995; Tse et al., 2016; van der Helm, 1994b), a standard method for evaluating shoulder muscle exposures during occupational tasks does not exist. Further development of these and similar tools that incorporate dynamics, cumulative task, and workday demands, in addition to interpersonal variability in musculoskeletal responses to occupational exposures, could provide a means to simulate task differences across an enormous range of postures, hand loads, and working conditions. This will broaden consideration of the connections between work parameters, tissue exposures, and tissue failure mechanisms across a diverse population, ultimately leading to better designs and prevention of shoulder tissue damage and accompanying disability.
Key Points
Muscular fatigue resulting from overexertion can create mechanical impingement risk.
Overhead exertions are known precipitators of shoulder muscular fatigue.
Several aspects of shoulder bony and muscular morphology combine to make it vulnerable to occupational tasks.
Shoulder tissue damage is often to soft tissues, especially the rotator cuff tendons, leading to lengthy recovery and high costs to industry and society.
Footnotes
Author Biographies
Clark Dickerson is a professor of kinesiology and the Canada Research Chair in shoulder mechanics at the University of Waterloo. He received his PhD in biomedical engineering from the University of Michigan in 2005.
Alison McDonald is a post-doctoral fellow at the University of Waterloo. She received her PhD in biomechanics in the Department of Kinesiology from McMaster University in 2017 and is funded by an NSERC PDF award.
Jaclyn Chopp-Hurley is an assistant professor at York University. She received her PhD in biomechanics in the Department of Kinesiology from the University of Waterloo in 2015.