
Abstract
Background:
Caregiver burden has been associated with caregivers’ mental disorders and need for support and information. However, the lack of quantitative studies and formal interventions aiming to lower burden levels in this population reflect the current negligence regarding this important issue.
Aim:
To identify burden levels and associated factors in caregivers of young adults with bipolar and unipolar mood disorder.
Method:
This is a cross-sectional study nested within a population-based cross-sectional study with young adults. Caregiver burden was assessed through the Burden Interview. Information about caregiver mental disorders (Axis I) and alcohol abuse were obtained through the Mini International Neuropsychiatric Interview (MINI) and the Cut-Down, Annoyed, Guilty and Eye-Opener (CAGE) questionnaire, respectively.
Results:
Caregiver burden was associated to caregiver’s mood and anxiety disorders, suicide risk and being the caregiver of young adults with depression disorder and bipolar disorder. Also, burden was higher among caregivers of bipolar individuals. When excluding the control group from the analysis, only mood and anxiety disorders remained associated to caregiver burden.
Conclusions:
Caregivers are affected by the young adult’s disorder even before a diagnosis has been given, with serious impairments in their lives. Thus, this is a subject in need of designing relevant strategies aiming to provide them with care.
Introduction
Mental disorders affect a major part of the population worldwide, causing serious impairments to patients, their families and the community. A specific mental health report from the World Health Organization states that about 450,000,000 people suffer from neuropsychiatric disorders, including major depression and bipolar disorder (WHO, 2001).
Throughout the years, and especially due to the de-institutionalization movement, the number of patients under the care of family members has increased (Baronet, 2003; Cuijpers & Stam, 2000). However, these informal caregivers do not usually have the required information and resourcefulness to deal with the burden caused by the disorder, often making them markedly distressed themselves and likely to be socially isolated (Shimazu et al., 2011). In this matter, caregiver burden can be described as subjective and objective distress, which may include the effects of caregiving on the health, finances and activities of the caregiver, as well as worry, tension, insomnia and resentment (Heru & Ryan, 2004).
A review article pointed out that caregivers of individuals presenting psychiatric disorders experience high levels of depression and anxiety, and they also need support due to their own mental disorders caused by the caregiver role (Steele, Maruyama & Galynker, 2009). An important report revealed a 30.4% and 38.9% prevalence of minor psychiatric disorders among the caregivers of patients with bipolar disorder and depression, respectively (Tomasi et al., 2008).
Other studies reveal that caregivers of individuals with bipolar disorder may experience a different and greater burden when compared to caregivers of people with other disorders (Ogilvie, Morant & Goodwin, 2005); and that these caregivers may feel more strained, with lack/diminishment of pleasure in their daily activities, greater feelings of depression, inability to cope with difficulties and a greater use of prescribed medication (Goosens, Wijngaarden, Knoppert-van Der Klein & Achterberg, 2008).
Caregivers who report higher levels of burden have significantly higher levels of emotional over-involvement, which could indirectly influence the course of illness through the family’s affective response and the patient’s medication adherence (Perlick et al., 2004). Levels of expressed emotion in relatives are consistent predictors of relapse among bipolar and other mood-disordered patients (Kim & Miklowitz, 2004) and are correlated to symptom severity in adolescents with bipolar disorder (Griffiths, 2011).
Having considered this background, the development of strategies aiming at giving support to caregivers is crucial, as they are usually abandoned and burdened by the health system itself, playing a role for which they are not prepared. Furthermore, caregiver burden may contribute to the onset or exacerbation of psychiatric symptoms that give rise to important conflicts in several areas of their lives.
The aim of this study was to identify burden levels and related factors in caregivers of young adults with bipolar and unipolar mood disorders in the city of Pelotas, Brazil. More specifically, this investigation sought to compare the burden means among caregiver groups, comparing them with the socio-demographic information regarding patient and caregiver, as well as verifying the relationship between burden and psychiatric disorders, and the use of alcohol/psychoactive substances.
Methods
This is a descriptive cross-sectional study nested within a population-based study conducted with young adults in the city of Pelotas, Brazil. For the purposes of this study, there was an attempt to recruit every person with a past or current history of a manic or hypomanic episode – the target sample – from the population-based study. According to these criteria, 93 young adults had a current or prior history of bipolar disorder. Additionally, two groups of control subjects were recruited. People without any history of affective disorder were randomly selected and matched for gender, age and socio-economic situation – i.e. a healthy control sample. Importantly, people from this control group were not excluded on account of any other mental disorders. The second control group was composed of those with a current depression but no past history of (hypo)mania. This was, thus, an active control group. Of these, data on 227 subjects were obtained (81% of the original sample). In order to improve diagnosis reliability, the Structured Clinical Interview for DSM-IV (SCID) was used as the group-defining criterion for this study.
In the SCID evaluation, the young were asked to identify their primary caregiver accordingly to previously established criteria (Perlick et al., 2004).
The identified caregivers (n = 227) were invited to take part in the present study; 40 of them refused or were considered losses. Thus, the sample of this study was composed of 187 caregivers who were divided into three groups: caregivers of young adults with bipolar disorder (n = 41); caregivers of young adults with depressive disorder (n = 72); and caregivers of young adults from the control group (n = 74). The study design is illustrated in Figure 1.

Study design.
Identification of caregivers and data collection occurred from March 2009 to May 2010. Only the caregivers who had signed the written informed consent form were included in the study. All participants diagnosed with a psychological/psychiatric disorder (according to the evaluation instruments) had been referred to treatment at the proper university department. This study was approved by the ethics committee of the Universidade Católica de Pelotas (UCPEL).
Caregivers were interviewed regarding socio-demographic situation, alcohol abuse, use of psychoactive substances in the 30 days prior to the interview, burden, and Axis I psychiatric disorders. The socio-economic classification was carried out through the Associação Brasileira de Empresas de Pesquisa (ABEP) classification scale (ABEP, 2003), which is based on the accumulation of material assets and on the schooling of the head of the household. It categorizes people into classes (A, B, C, D, E) according to the scores, where A refers to the highest socio-economic class and E to the lowest.
Burden evaluation was carried out using the Brazilian validated and adjusted version of the Burden Interview (Scazufca, 2002). It is a 22-item scale that assesses for caregiver’s subjective and objective burden regarding the patient’s functional and behavioural impairments. The score may range from 0 to 88, with a higher score corresponding to a greater burden. In order to identify Axis I disorders, the caregivers responded to the Mini International Neuropsychiatric Interview (MINI) Amorim, 2000), which is a short interview based on the DSM-IV and ICD-10 diagnostic criteria. Moreover, participants were evaluated regarding alcohol abuse through the Cut-Down, Annoyed, Guilty and Eye-Opener (CAGE) questionnaire (Masur & Monteiro, 1983).
The instruments were coded and then double-typed in EpiInfo 6, where the typing consistence was checked. The crude and multivariate analyses were carried out in SPSS 13 and Stata 9, respectively. In order to control for possible confounding factors, all variables that were associated (p < .20) to both the young adult diagnostic group (exposure) and caregiver burden (outcome) in the crude analysis were included in the multivariate analysis, which was performed through a linear regression.
Since the difference between the depression and bipolar disorder groups was very close, a Bonferroni pairwise comparison was performed. This revealed a significant difference between the three groups (p < .05), which confirms the meaningful difference in burden levels for different disorders.
Results
There were 52 refusals in the total number of young adults invited to participate in the SCID evaluation (n = 279). The final sample of the population-based study was composed of 227 young adults. The variables gender, age and socio-economic classification were considered in the pairing of the sample and despite the losses/refusals and the changes in the diagnosis (SCID), the groups continued to present a similar distribution (p > .05).
Regarding the present study, there were 11 refusals and 29 losses within the caregiver group. The losses were mostly related to: (1) the young adult lived alone and could not identify the caregiver according to the inclusion criteria for this study; (2) the young adult asked the research group not to invite the caregiver to take part in the study; (3) the caregiver was deceased or lived outside the urban area of Pelotas; and (4) it was not possible to contact the caregiver due to lack of information provided by the young adult.
Finally, the sample was composed of 187 caregivers of young adults with bipolar disorder, depressive disorder or from the control group. The mean age among the young adult group was 22 years (SD = 2.2), and they were mostly women, with nine or more years of schooling. The prevalence of suicidal risk/ideation was 24%. Concerning the diagnostic groups, 38.5% of the young presented depressive disorder and 21.9% were diagnosed with a bipolar disorder, whereas 39.6% belonged to the control group. The mean age among the caregiver group was 48.5 years (SD = 10.4) and most of them (86%) lived with the young adult. Concerning familial relationship, 82% were the young adult’s mother (n = 155), 9% their father (n = 17) and 8% their spouse (n = 15).
The analyses of the caregiver variables were designed to exclude the control group in order to avoid its interference over the results (n = 113). Nonetheless, important results regarding the three groups are also presented. According to the Burden Interview, the mean burden among the caregivers in this study was 20.1 (SD = 14.7) when considering the three groups, and 23.26 (SD = 15.3) when excluding the control group.
The crude analysis concerning the three groups (Table 1) revealed that the characteristics from the young adults that were associated (p < .05) to greater caregiver burden were low schooling and belonging to the depressive or bipolar disorder diagnostic group. However, burden means in these two groups were too close, and therefore they were not significantly different according to the Bonferroni test (Table 1). Also, when stratifying the analysis to exclude the control group, this difference was not significant (p > .05).
Crude analysis: Young adult characteristics associated with caregiver burden.

Linear tendency.
Note: Statistical significance, by Bonferroni test, between control and depressive disorder groups (p = .002) and control and bipolar disorder groups (p = .011), but not for depressive disorder x bipolar disorder (1.000).
Concerning the three-group crude analysis (Table 2), the variables associated (p < .05) to caregiver burden were: feminine gender; low socio-economic classification; low schooling; use of psychoactive substance within 30 days prior to the interview (including cannabis, cocaine, heroin, sleeping medication with or without medical prescription, among others); mood and anxiety disorders; and suicide risk. Considering the mood and anxiety disorders separately, it is observed that the burden means were higher among the caregivers who presented only some kind of anxiety disorder, when compared to those who presented only some kind of mood disorder. Caregiver burden was also associated with familial relationship (p = .017); it was highest among the spouses (23.0; SD = 5.2), followed by mothers (20.8; SD = 15.0) and fathers (10.6; SD = 6.6).
Crude analysis: Caregiver burden and related factors according to the young adult’s diagnostic group (bipolar disorder and depression).
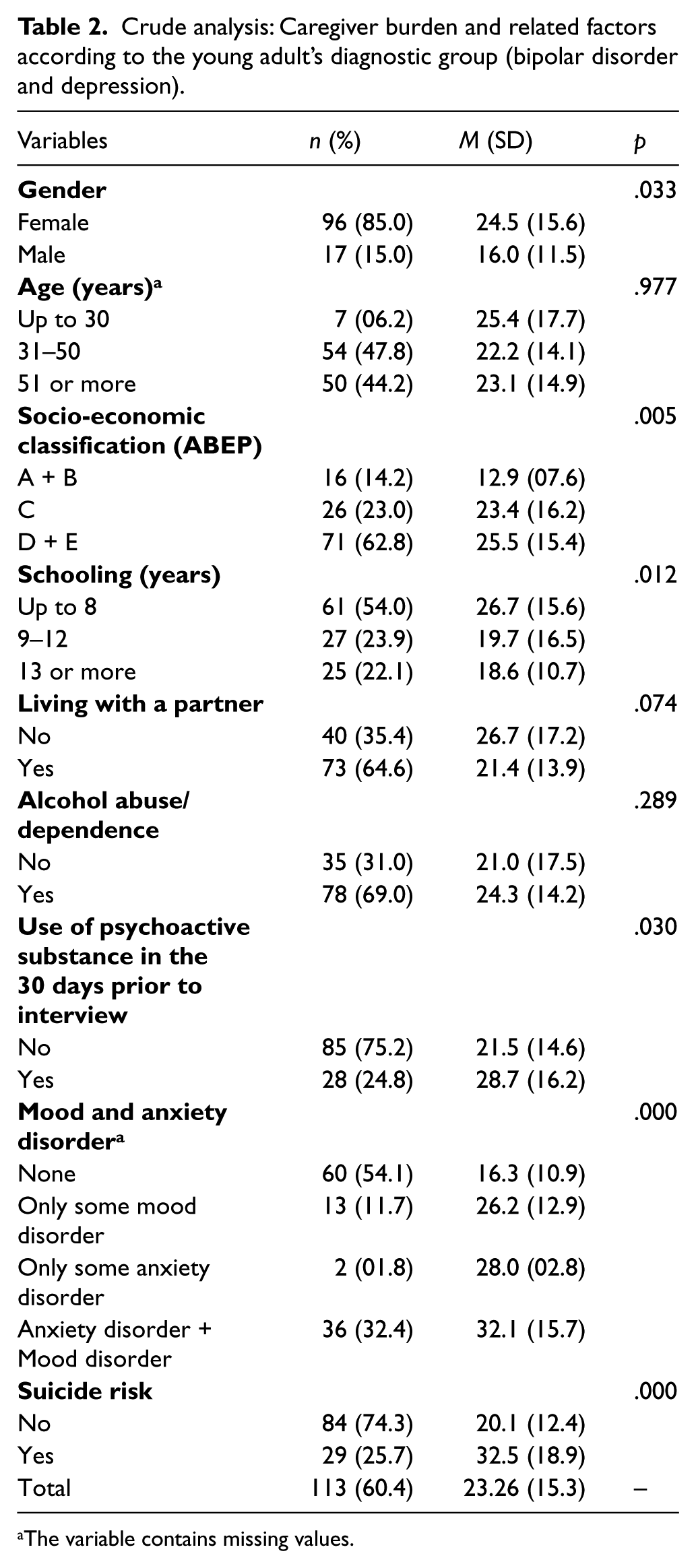
The variable contains missing values.
Table 3 presents the results of the stratified linear regression considering only the diagnostic groups depression and bipolar disorder. In this case, the only variable that maintained a significant association with caregiver burden in the multivariate analysis was Axis I – mood and anxiety disorders. Specifically, presenting only some mood disorder is associated with the highest increase in burden score, followed by comorbid mood and anxiety disorders and by only some anxiety disorder, all when compared to individuals who do not present these disorders.
Multivariate analysis (linear regression): Caregiver burden and related factors according to the young adult’s diagnostic group (bipolar disorder and depression).
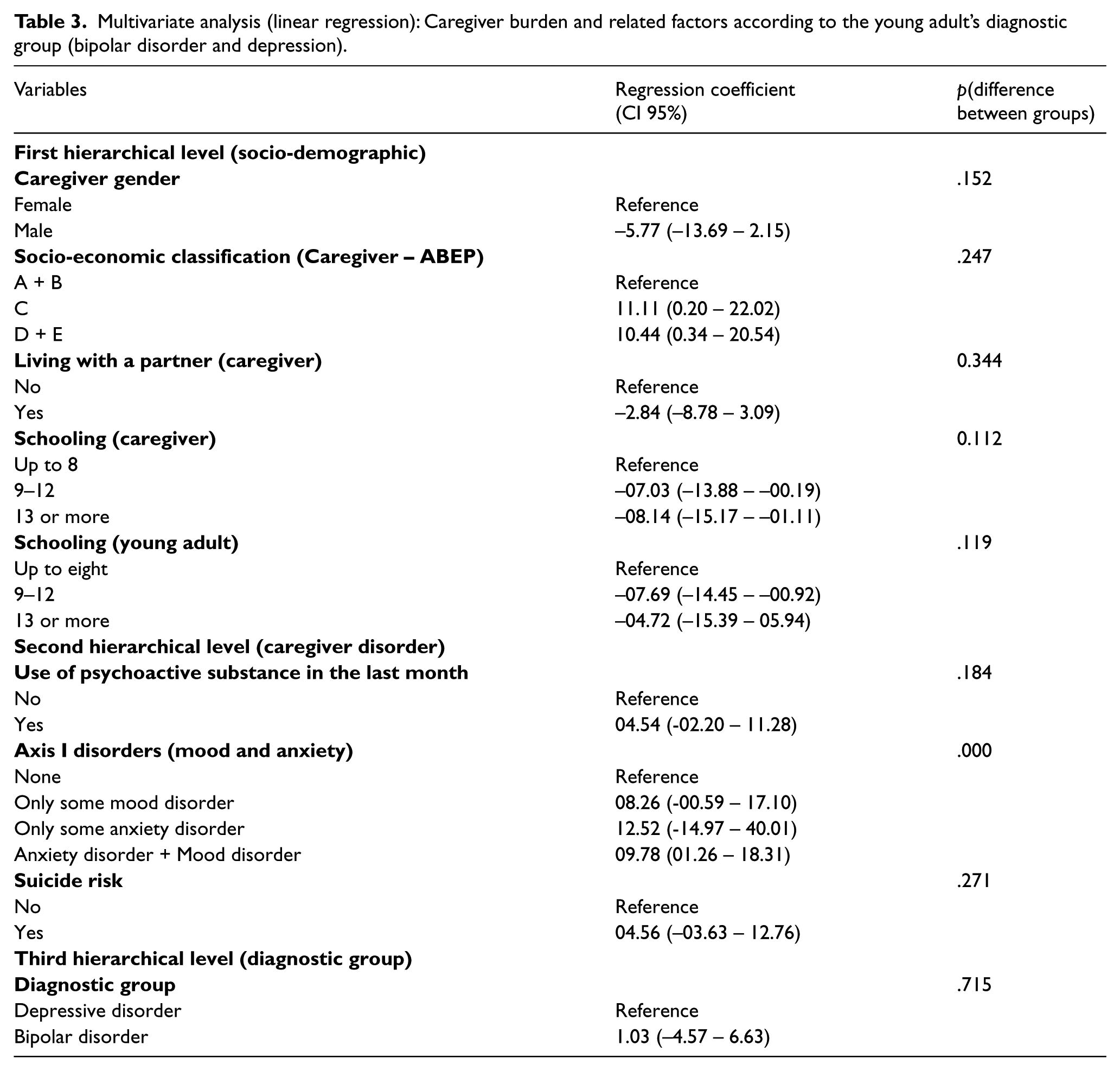
On the other hand, if the control group is considered, presenting comorbid mood and anxiety disorders is associated with an 11.5-point increase in caregiver burden score (p < .001). Moreover, there is a six-point increase in the burden score in caregivers who presented suicide risk (p < .05), which was not meaningful in the stratified analysis.
Regarding the burden means in the three groups, linear regression showed that even though the difference in burden means between the depressive and bipolar disorder groups was not significant in the crude analysis, there is a five-point (p < .05) and a four-point increase (p < .05) in the burden score among the caregivers of young adults with bipolar disorder and depressive disorder, respectively, in comparison to the control group. However, when excluding the control group from the analysis, the one-point increase in the burden score of caregivers of young adults with bipolar disorder when compared to the caregivers of those who were depressed was not statistically significant (p > .05)
Discussion
This is the first quantitative study in Brazil to evaluate burden in caregivers of young adults with depressive and bipolar disorder, originated from a population-based sample.
This study found greater burden among the caregivers of young adults with bipolar disorder and depressive disorder, when compared to the control group. This result indicates that in a paired sample according to age, gender and socio-economic classification, the young adult’s mood disorder may be a strong risk factor for greater caregiver burden. Furthermore, the mean burden was slightly higher among the caregivers of individuals with bipolar disorder, which is in accordance with other studies (Heru & Ryan, 2004; Ogilvie et al., 2005; Weinstock, Keitner, Ryan, Solomon & Miller, 2006).
Caregiver burden was considered high in the present study, given that this was a non-clinical sample where most of the individuals whose caregivers were evaluated (96.0%; n = 218) had not been previously diagnosed nor had received corresponding treatment or been admitted to a hospital or psychiatric ward for such disorders.
Despite the non-significant difference in the burden means between the bipolar disorder and depressive diagnostic groups given by the Bonferroni test, the multivariate analysis revealed a slightly higher burden score among the caregivers of young adults with bipolar disorder, in comparison to the caregivers of young adults with depression, even though this difference was not meaningful. One possible reason for the non-significance of such difference in the crude analysis is the group size, since there were more young adults with depression than with bipolar disorder. Moreover, caregiver burden was a little higher among the caregivers of young adults with bipolar disorder, despite the smaller number of participants and the greater refusal/losses in this group. Taking these factors into consideration, it may be thought that with a higher number of young adults in the bipolar disorder diagnostic group, burden could be even higher and the difference in burden means between the groups could be significant.
Regarding the other results, it was found that caregiver mood and anxiety disorders are associated with greater caregiver burden. This association may be influenced by several factors, including a caregiver disorder previous to the onset of the symptoms in the young adult, the caregiver’s coping skills regarding their own disorder, and the burden caused by the caregiving role. Therefore, despite the significant association, it is not possible to conclude that caregiver mood and anxiety disorders are caused only by the caregiver burden, since it is a cross-sectional study and the caregivers were not assessed before the onset of mood symptoms in the young adult. The same could be considered regarding the analysis including the control group where caregiver burden was associated to caregiver suicide risk. Also, it is possible that the same caregivers who are depressed present suicide risk.
In this study with caregivers of young adults without a previous depressive or bipolar disorder diagnosis and with a relatively low incidence of mood episodes in comparison to a clinical sample, burden was higher among caregivers of young adults who presented depressive and bipolar disorder when compared to the control group. There was also a significant association between caregiver burden and caregiver mood and anxiety disorders. These findings suggest that the caregivers are affected by the young adult’s disorder even before the diagnosis. This impact can lead to greater burden and may consequently be associated to serious impairments given by the burden itself and its associated factors. It may be also considered that caregiver burden differs accordingly to the disorder presented by the person under their care.
Taking all these results into consideration, it is reasonable to conclude that caregivers of young individuals with psychiatric disorders, specifically depressive and bipolar disorder, should be seen and targeted by an intervention process that it is not aside from the young adult’s treatment. At the moment, there are no programmes or intervention policies that guarantee the caregiver proper assistance and therefore the caregivers end up playing a role that they may not have the physical, psychological and financial support to cope with. Thus, it is expected that the findings presented in this study may contribute to further studies and to the creation of intervention strategies targeting the informal caregiver, since they suffer the consequences of the psychiatric disorder and the caregiving role on a daily basis, even when the patient is yet to be diagnosed.
Footnotes
Funding
This study was funded by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPQ) through the PROSUP/CAPES grant.