
Abstract
Aim:
To evaluate expressed emotions (EEs) as perceived by the patients and its correlates among patients with bipolar disorder (BD).
Methodology:
One hundred patients diagnosed with BD were assessed on the Perceived Criticism Measure (PCM), Family emotional involvement and criticism scale (FEICS), Brief dyadic scale for expressed emotions (BDSEE) and Vulnerability for abuse screening scale (VASS) to assess EE and possible abuse by the caregivers. Caregivers were evaluated on family burden interview schedule and family coping questionnaire.
Results:
Longer duration of illness (Pearson’s correlation coefficient: −0.335; p = .001***) and longer duration of treatment (Pearson’s correlation coefficient: −0.317; p = .001***) were associated with significantly lower perceived criticism as assessed by FEICS. Higher use of coping mechanisms such as coercion, avoidance and resignation by caregivers were associated with the higher perception of EE, whereas the use of coping mechanisms such as information seeking, communication, and social involvement by the caregivers was associated with the perception of lower EE among the patients. Higher caregiver burden was associated with a higher perception of the EE by the patients. Higher perception of abuse by the patients was associated with higher EE.
Conclusions:
Present study suggests that higher use of maladaptive coping, caregiver burden, and abuse has a significant impact on the EE. Accordingly, psychosocial interventions need to focus on caregivers to reduce EE.
Introduction
Bipolar disorder (BD) is a disabling psychiatric illness with a high rate of recurrence, persistent symptoms, and impairment in functioning. The shift from institutional care to community-based care has resulted in the transferring of day-to-day care of patients to their family members, resulting in a psychosocial burden over the caregivers. Hence, BD not only affects the patient but also has a huge impact on the lives of the persons caring for them.
The problems of families and caregivers of a mentally ill person have been explored in various studies. The effect of BD on the caregivers in terms of burden of care, disability and distress have been evaluated in many studies (Nehra et al., 2005). Another important caregiver outcome is Expressed Emotions (EE). ‘EE reflects the extent to which the close family member of an identified patient expresses critical, hostile or emotionally overinvolved attitudes toward the patient during a private interview with a researche’ (Brown & Rutter, 1966). George Brown and his colleagues (Brown et al., 1958) identified five components of EEs, that is, critical comments, hostility, emotional overinvolvement, positive remarks (regard), and warmth. Although ratings of EE are often considered to be characteristic of relatives, EE is most appropriately regarded as a measure of the patient–relative relationship. EE is a measure of the family environment that is based on how caregivers or relatives of a mentally ill patient spontaneously talk about the patient (Butzlaff & Hooley, 1998). Examination of interaction patterns reveals that high levels of EE are associated with reciprocal negativity within the relationship. There has been considerable debate regarding the causality of EE, whether the disturbed behaviours of patient leads to critical and /or overinvolved attitudes among caregivers or living with the high-EE caregivers’ effects the patients in a negative way, thus contributing to relapse. Hooley and Richters (1995) suggested that there is a complex circular relation between EE and relapse with patient’s behaviours leading to high-EE among relatives, which in turn affects the course of illness (Hooley & Richters, 1995).Current models conceptualise EE within an interactional framework, with the characteristics of patients (e.g. uncooperativeness, negativity) engendering critical attitudes in relatives who are less flexible and tolerant and more inclined toward controlling behaviours, to begin with. It was seen that high-EE relatives are more likely to attribute the negative behaviours of patients to personal and controllable factors (i.e. personality, lack of effort) than are low-EE relatives, who are more likely to attribute the behaviours to uncontrollable factors (i.e. illness or external stressors) (Miklowitz et al., 2004).
It has been seen that symptoms of severe mental illnesses (SMI) like schizophrenia and BD generate certain attitudes among the caregivers, which can vary from hostility to warmth. Patient-caregiver interaction patterns have been shown to change the course of these illnesses. Studies involving caregivers of patients with schizophrenia show that EE has a significant negative impact on the course and outcome of schizophrenia and predicts relapses and poor treatment adherence (Nehra et al., 2005; Perlick et al., 2007). However, data in terms of EE among caregivers with BD is less well studied. Most of the studies which have evaluated EE among patients of BD suggest association of high EE with higher relapse rates (Barrowclough & Hooley, 2003; Lam, 1991; Miklowitz, 2007; Shimodera et al., 2012). Data from the metanalysis suggest a positive correlation between EE and relapse, with an effect size of 0.39–0.45 depending on the cut-off of 2 or 3 respectively for critical comments. These findings provide strong support for the role of EE in BD (Butzlaff & Hooley, 1998). Data also suggest that the impact of EE on the outcome is independent of patient medication compliance, treatment regimen, baseline symptoms, demographics, and illness history (Miklowitz et al., 2004). Occasional study suggests that high EE is associated with caregiver burden. Studies suggest association of EE with the number of past episodes of mania (Murkey et al., 2017). A recent study evaluated the various predictors of EEs in 98 BD patients in full remission and their relatives. EEs were evaluated on Family attitude scale (FAS) and Perceived criticism (PCM) scale. The factors that predicted the patient-rated FAS included the number of previous mood episodes, current self-rated manic symptoms and comorbid symptoms of Cluster C personality disorder. Relative-rated FAS was predicted by comorbid symptoms of Cluster A personality disorder (Lex et al., 2019). However, some of the studies suggest lack of association of high EEs with current illness severity and functioning (Coville et al., 2017) and clinical variables while patients are in full remission (Lex et al., 2019) and any of the patient characteristics (Yadav et al., 2018).
This review of literature suggests that there is limited data on EE in BD. There is lack of literature evaluating the relationship of EE with caregivers’ burden, coping, psychological morbidity and abuse. Evaluation of EE in patients with BD can help in understanding the role of this variable on the clinical course of the disorder. Further, understanding the association of EE with other caregiver variables like caregiver burden, coping and psychological morbidity among caregivers can help in designing intervention programs that can reduce the negative impact of these caregiver variables on the patients’ illness. In this background, this study aimed to evaluate EE as perceived by the patients and its correlates among patients with BD.
Methodology
This cross-sectional study was conducted at a tertiary care teaching hospital in north India. The study sample comprised of 100 patients with BD. Convenient sampling was used for the selection of patients with BD and their caregivers. Approval was sought from the Ethics committee of the institute and all the participants were recruited after obtaining written informed consent. This study evaluated EE, both from the perspective of patients and their caregivers. This paper reports the findings of EE as reported by the patients.
To be included in the study, the participants were required to be diagnosed with BD as per DSM-IV criteria (as ascertained by using MINI-PLUS), aged >18 years, with duration of illness of at least 1 year, in a state of clinical remission defined by score <7 on the Hamilton Depression Rating Scale (HDRS) and <7 on Young Mania Rating Scale (YMRS) and ‘clinical stability,’ that is, no exacerbations or relapses or greater than 50% hikes in medication dosages in the 3-month period prior to assessment for the study and able to read Hindi/English. Patients with organic brain syndrome, intellectual disability and comorbid substance dependence (currently using) other than tobacco dependence were excluded. The caregivers were required to be aged more than 18 years, living with the patient for at least last 1 year and actively involved in the care of the patient and able to read Hindi/English. Caregivers with intellectual disability were excluded.
All the patients with a clinical diagnosis of BD and their caregivers were approached. Patients and their caregivers who agreed to participate and provided written informed consent were assessed on selection criteria. Those meeting the selection criteria were recruited. Patients with BD were evaluated on Perceived Criticism Measure (PCM), Family emotional involvement and criticism scale (FEICS), Brief dyadic scale for expressed emotions (BDSEE) and Vulnerability for abuse screening scale (VASS) to assess perceived criticism and possible abuse by the caregivers.
Instruments
Results
The mean age of patients was 42.07 (SD-13.01) years and the mean education in years was 10.72 (SD-3.85) years. The mean family income of the study sample was rupees 12,795 (SD-14,384.35). Majority of the study participants were male, married, on a paid employment, from urban background, Hindu by religion and middle socioeconomic status. There was nearly equal distribution of subjects from nuclear and extended/joint family set-up and those who educated above matric and up to matric. The mean age of caregivers was 46.64 (SD-10.44) years. The mean duration of education of the caregivers was 10.22 (SD-4.25) years and the mean income of the caregivers was rupees 9,000 (SD-14,664). Female caregivers outnumbered males. Majority of the caregivers were married (95%), educated up to matric (63%), were spouse (65%) of the patient, were supervising the medications (81%) and were themselves not suffering from any chronic physical illness (74%). Unemployed (55%) caregivers outnumbered those who were currently on paid employment (45%). Caregivers had been performing the role of a primary caregiver for the last 12.84 (SD 8.75) years and on an average spent about 3.24 (SD-1.69) hours each day in providing care to the patient. Caregivers accompanied their patients during the 79.84% of follow up visits in the previous 1-year (Table 1).
Socio demographic profile of patients and caregivers (N = 100).
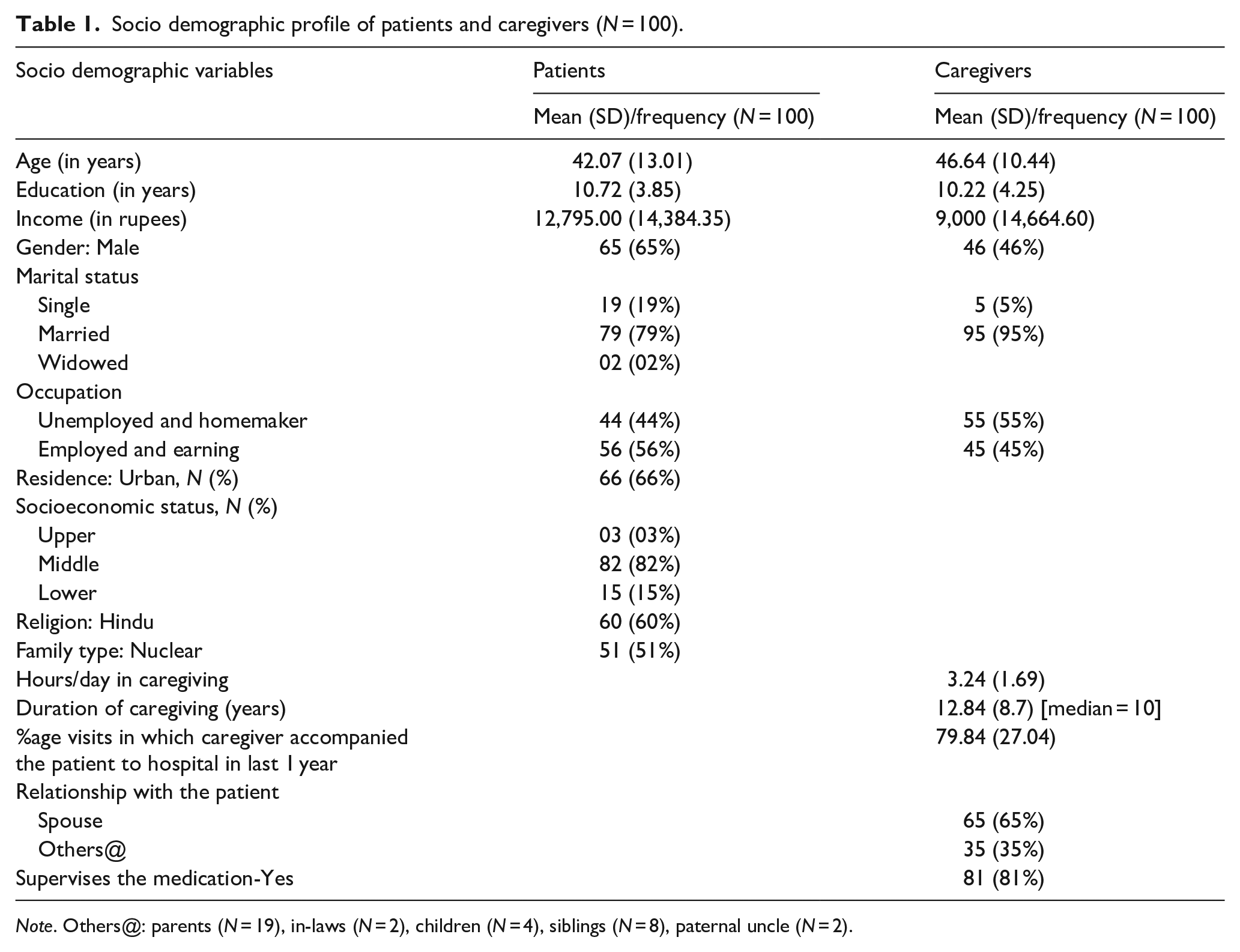
Note. Others@: parents (N = 19), in-laws (N = 2), children (N = 4), siblings (N = 8), paternal uncle (N = 2).
Clinical profile of patients
All patients were in clinical remission at the time of assessment, as per the selection criteria. The mean age of onset was 27.76 (SD-9.20) years and the mean duration of illness was 14.2 (SD-9.48) years. The mean duration of treatment in the lifetime was 7.49 (SD-6.16) years and the mean duration of untreated illness was 6.78 (6.79) years. The mean numbers of lifetime episodes prior to assessment were 5.91 (5.13), with mean number of manic episodes exceeding, mean number of depressive episodes. Other clinical details are depicted in Table 2.
Clinical profile of patients.
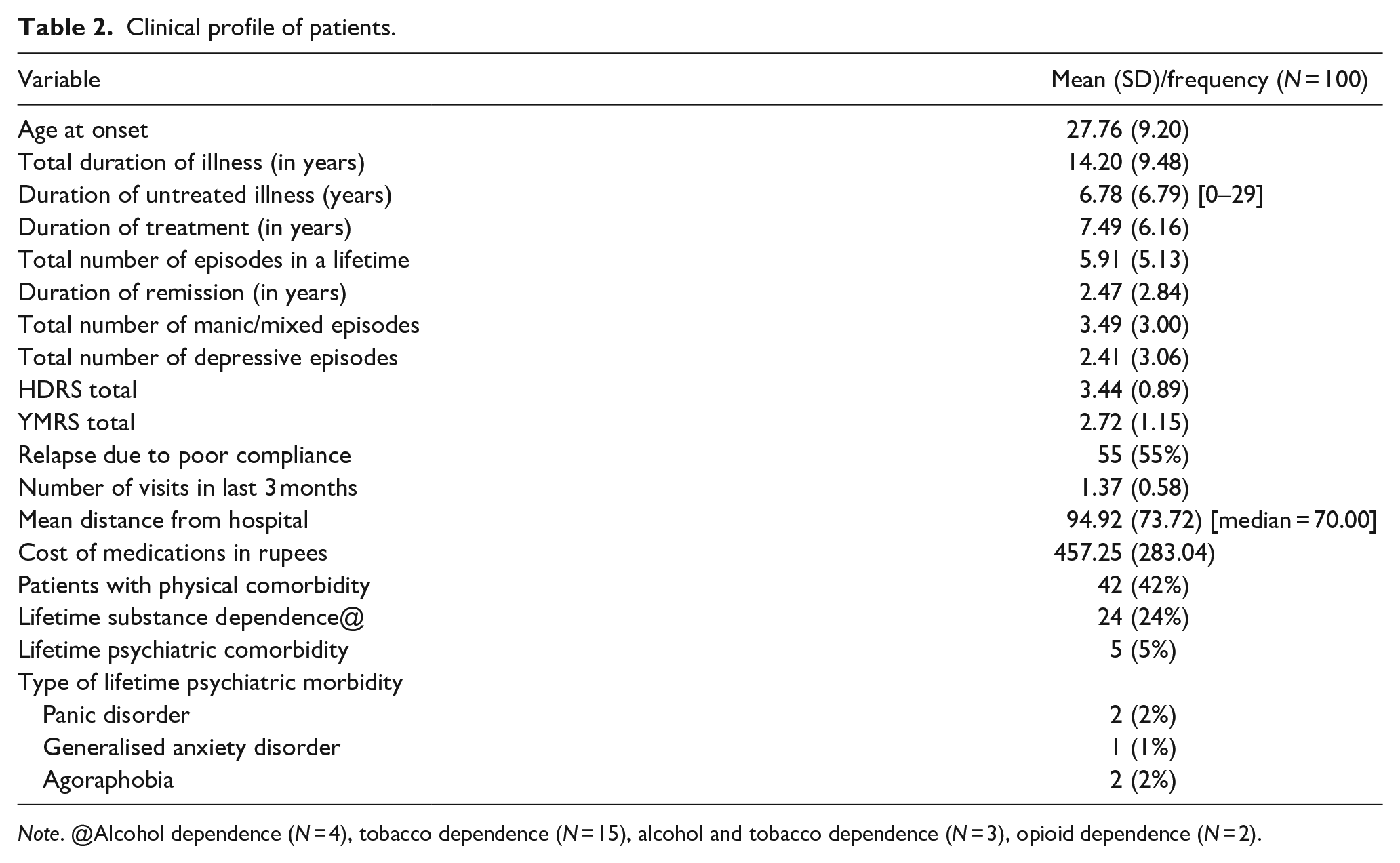
Note. @Alcohol dependence (N = 4), tobacco dependence (N = 15), alcohol and tobacco dependence (N = 3), opioid dependence (N = 2).
Expressed emotions as per the patient
On PCM scale, the mean score was higher for getting upset with criticism and this was followed by mean score of perception of caregiver being critical of them and patients rated themselves criticising the caregivers as the least. On BDSEE, the mean weighted score was highest for perceived warmth was followed by emotional overinvolvement and perceived criticism. On FEICS, mean score for emotional overinvolvement was higher than the mean score for perceived criticism (Table 3).
Expressed emotions as perceived by the patients.
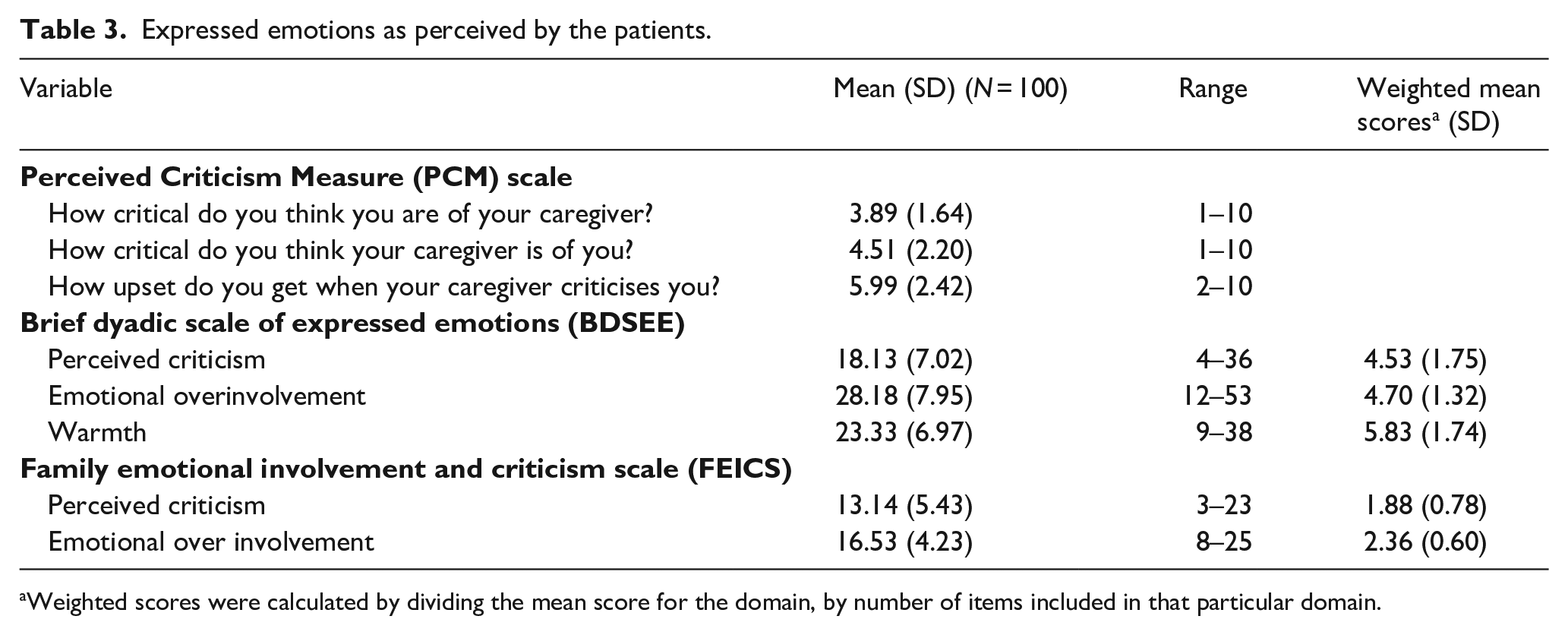
Weighted scores were calculated by dividing the mean score for the domain, by number of items included in that particular domain.
Caregiver burden, coping, psychological morbidity, abuse, reasons for caregiving and perception of problematic behaviours
On FBI, maximum burden was perceived in the disruption of routine family activities and disruption of family leisure followed by disruption of family interaction, financial domain, effect on physical health of others and least burden on ‘effect on mental health of others’. On FCQ, the mean weighted score was highest for social involvement domain, followed by communication, resignation, information, social interests, coercion, and least for the domain of avoidance. Abuse faced by the patient was evaluated by using Vulnerability to abuse screening scale (VASS) and Caregiver abuse screen (CASE). VASS is rated as per the information provided by the patient and CASE is rated as per the information provided by the caregiver. On VASS, the mean weighted score was highest for the domain of dependence, followed by dejection and coercion and least for the domain of vulnerability. Majority of the patients had mean VASS score of ⩾3, which suggest presence of abuse. On CASE, the mean score for the study sample was 4.39 (SD 2.16) and three-fifth of the caregivers scored ⩾4, which suggest presence of abuse. On GHQ-12 the score for the study sample was 2.54 (2.55) and 59% of the caregivers scored >2 (Table 4).
Caregiver burden, caregiver coping, caregiver abuse and psychological morbidity among caregivers.
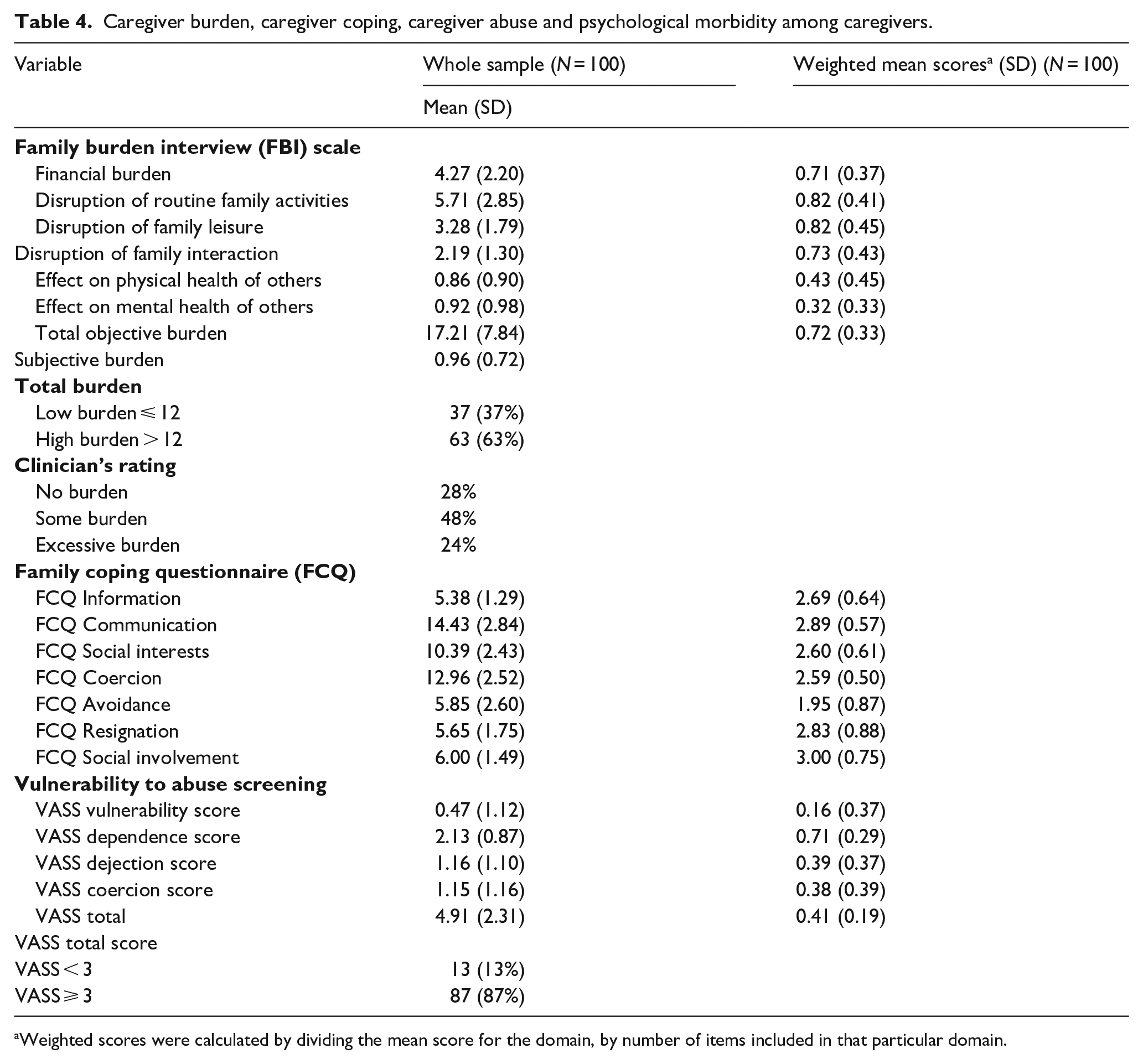
Weighted scores were calculated by dividing the mean score for the domain, by number of items included in that particular domain.
Factors associated with expressed emotions
None of the demographic variable of the patient and the caregivers had any significant association with EE. EE as assessed on PCM and BDSEE did not have any significant association with clinical variables. Longer duration of illness (Pearson’s correlation coefficient: −0.335; p = .001***) and longer duration of treatment (Pearson’s correlation coefficient: −0.317; p = .001***) were associated with significantly lower perceived criticism as assessed by FEICS. When the association of EE and caregiver burden, coping used by the caregivers, psychological morbidity in the caregivers and the abuse faced by the patient was evaluated, significant correlations were seen. In general use of coping mechanisms such as coercion, avoidance and resignation were associated with higher EE, whereas use of coping mechanisms such as information seeking, communication and social involvement were associated with lower EE (Table 5).
Association of EE with family coping, caregiver burden, abuse and psychological morbidity.
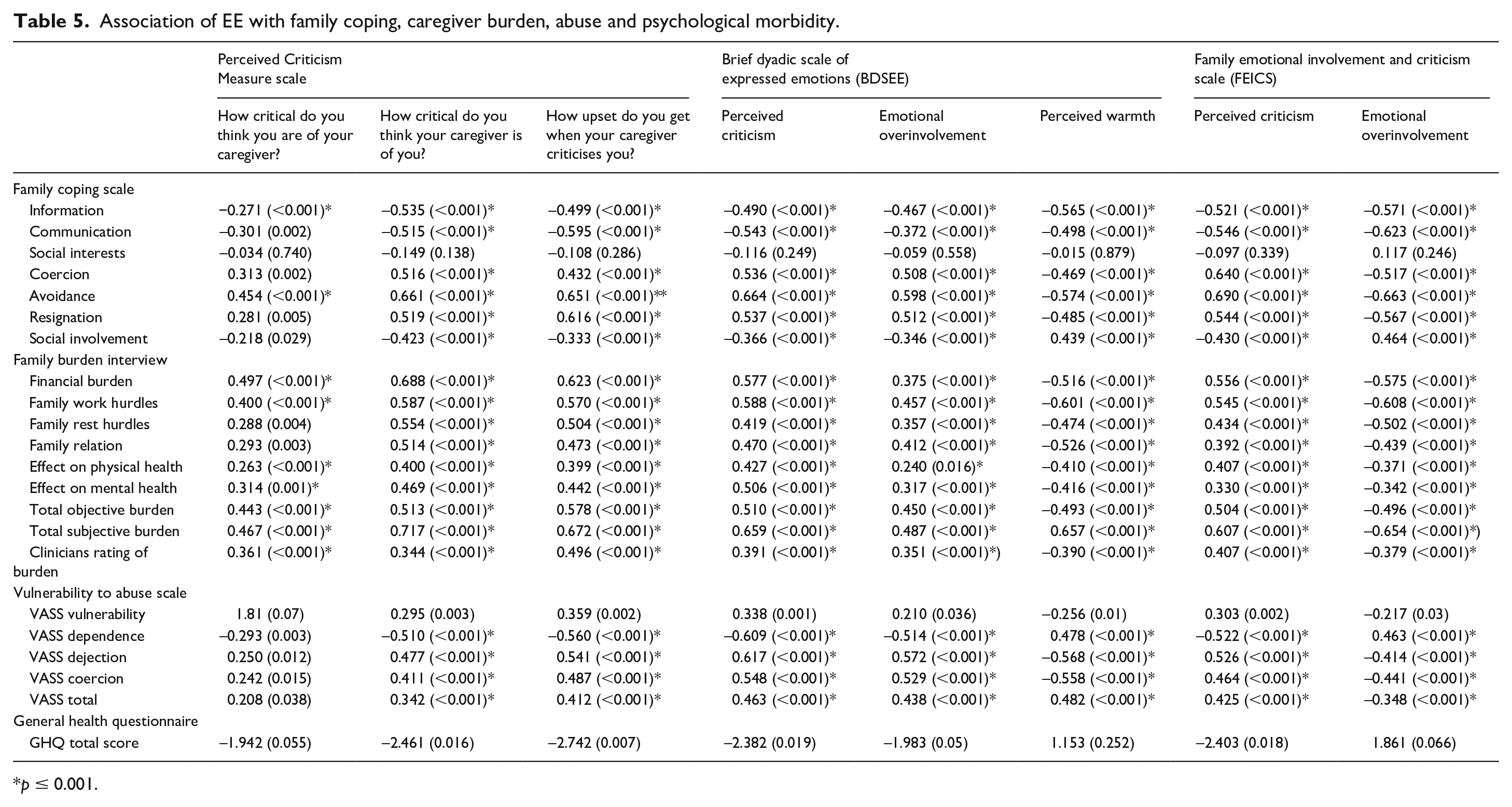
p ≤ 0.001.
In terms of caregiver burden, higher caregiver burden in all the subscales of objective burden, total objective burden, total subjective burden and burden as rated by the clinician were associated with higher EE, with occasional exceptions (Table 5). In terms of abuse, higher perception of vulnerability, dejection, coercion, total VASS score correlated positively with higher EE. For the abuse domain of dependence, the correlations were in the opposite direction, when compared to other domains of VASS. When those with VASS score of <3 and ⩾3 were compared no significant difference emerged on any of the scales of EE (Table 5).
When caregivers with and without psychological morbidity were compared, it was seen that patients of caregivers with psychological morbidity had higher perception of the EE on all the scales, except for the domain of perceived warmth on the BDSEE and significantly lower emotional overinvolvement on the FEICS. In terms of GHQ total score, higher GHQ score was associated with higher perceived criticism as per BDSEE an FEICS and higher emotional over involvement as per the BDSEE (Table 5).
Predictors of expressed emotions
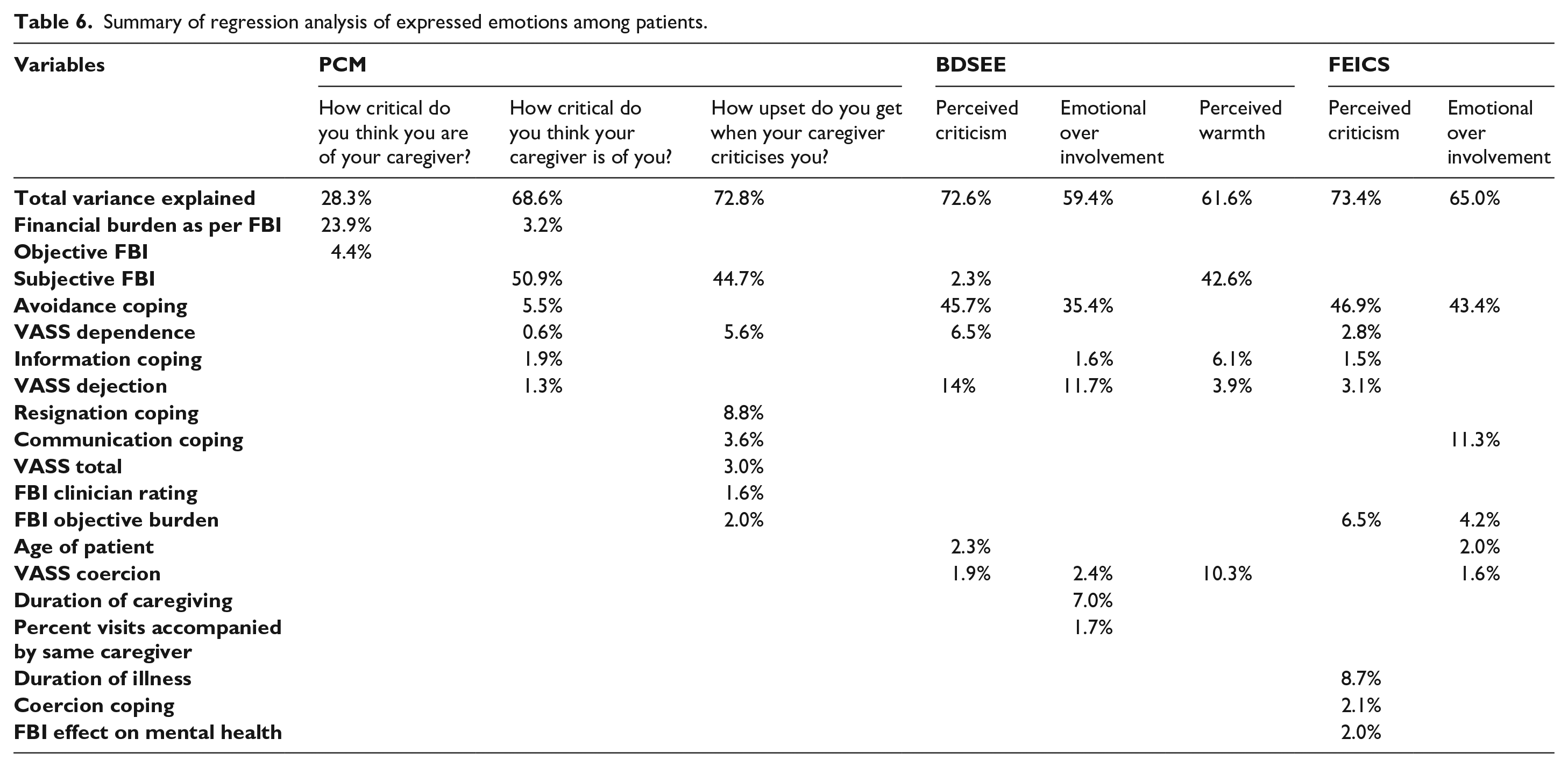
To study the effect of various independent variables on the expressed emotions as reported by the patients and their caregivers linear regression analyses with stepwise method were done (Table 6). Total variance explained by the different variables for each domain of EE across different scales ranged from 32.2% to 73.4% (Table 6).
Summary of regression analysis of expressed emotions among patients.
Discussion
BD is a complex mental disorder, with marked variability. The complexity and variability of the illness poses a challenge both for the individuals suffering from this illness and their families. Over the years there has been a breakdown in structure of Indian families. Due to this the number of family caregivers available to take care of the patients is depleting and the caregivers are often under lot of stress to deal with the problematic behaviours of the patients (Reinares et al., 2016). The distress among the caregivers often manifests as EE. Studies across the globe have shown that high EE in the family are often associated with adverse outcome in patients with schizophrenia and bipolar disorders (Barrowclough et al., 1994; Butzlaff & Hooley, 1998; Hooley & Richters, 1995; Millman et al., 2018; Ogilvie et al., 2005). Although, there are few studies from India and other parts of the globe on EE in bipolar families, little is understood about its correlates.
Accordingly, the aim of this study was to evaluate the extent of EE in families with one of the persons suffering from BD.
George Brown identified five components of EEs, that is, critical comments, hostility, emotional overinvolvement, positive remarks (regard), and warmth. As the available instruments, do not tap assessment of all the five domains of EEs, in the present study, an attempt was done to cover as many domains as possible, by assessing EEs by using more than one scale. Together, PCM, FEICS and BDSEE scales covered the domains of perceived criticism or critical comments, emotional overinvolvement and warmth. Participants were recruited in the phase of clinical stability and after a reasonable period of clinical remission. This was done to minimise the effect of acute exacerbation on EEs, which can actually lead to higher expression of EEs.
When the findings of the present study are compared with the existing literature, studies that have used these scales among the patients with BD, findings are comparable and suggest that patients with BD face high level of EE (Coville et al., 2017; Lex et al., 2019; Yadav et al., 2018). However, an important aspect to note is that in the present study the mean weighted scores were highest for the domain of warmth, followed by emotional involvement and least for perceived criticism on the BDSEE. Similarly on FEICS, mean weighted score of emotional overinvolvement was higher than that of perceived criticism. These findings possibly reflect the traditional behaviour of the Indian families, who make all the efforts to take care of their ill relative and show their affection and caring attitude toward the patient, despite being in the adverse situation (Avasthi, 2010). The higher scores on overinvolvement also reflect the similar attitude of Indian families of caring for their ill relative.
In general, sociodemographic variables of patients and the caregivers were not associated with EE. This finding is supported by the existing literature, which also suggests lack of association between severity of EE with demographic factors (Batra et al., 2016; Coville et al., 2017; Yadav et al., 2018).When the association of EE as perceived by patient and clinical variables was evaluated, longer duration of illness and longer duration of treatment were associated with significantly lower perceived criticism and lower emotional over involvement as perceived by the patient. These associations possibly reflect that with passage of time, caregivers and patients get used to each other’s behaviour and resultantly, reach to a newer level of balance in the interaction. It is also possible that with passage of time, the caregivers understand that what works and what does not work for the patients and accordingly, change their own behaviour to form a new homeostasis with the patient. The other explanation for these could be that, with longer duration of illness and treatment, possibly patients start valuing the role of the caregivers in their life, in terms of help received in remaining well. Further, possibly start understanding the well-meaning intentions of the caregivers in correcting them.
Present study suggests that use of adaptive coping such as information, communication, social involvement are associated with lower EE and use of maladaptive coping such as coercion, avoidance and resignation are associated with higher EE. These findings are in the expected lines. Although studies evaluating the role of coping mechanisms of caregivers in EE could not be found, specifically for patients with BD, but findings of the present study are supported by data from schizophrenia literature (Nehra et al., 2005; Magliano et al., 1999). In the present study, coping mechanisms such as resignation, communication, and avoidance emerged as important predictors of various components of EE. In fact, avoidance coping alone explained 46.9% of variance of perceived criticism and 35.4–43.4% of variance of emotional over involvement as perceived by the patients. However, it is important to note that mean weighted scores were least for the avoidance domain of coping, in the univariate analysis, suggesting that it was one of the least commonly used coping mechanism. This finding suggests that, although, it is least commonly used coping, but when used has significant negative impact on the EE. However, in the present study, resignation and coercion were used as frequently as other coping mechanisms. These findings suggest that, in their effort to take care and improve the outcome of the patients, caregivers at times resort to coercion and when despite all their effort, when they fail to get the desired response, then feel dejected and give up to the situation. All these have detrimental effect on the patient’s perception of the EE. Accordingly, it can be said that clinicians managing patients should focus on evaluating the coping mechanism of the caregivers, as this forms the most important variable, which mediates EE. Clinicians should encourage the caregivers to more often use the adaptive coping mechanisms and should discourage the caregivers to use the maladaptive coping mechanisms. While evaluating the coping, the clinicians, should specifically focus on all the efforts made by the caregivers for the patient and their reactions to the resistance from the patient to comply or failure of treatment response. This would possibly help in reduction in the EE faced by the patients with BD.
In the present study higher caregiver burden was associated with higher EE as perceived by the patients. In the regression analysis, subjective caregiver burden and financial objective burden emerged as the most important predictors of EE, with subjective burden explaining a significant proportion of the EE. Findings of the present study are supported by the existing literature, which also suggest that EE have a significant positive correlation with the total burden of care in the caregiver (Murkey et al., 2017). These findings suggest that caregiver burden plays an important role in manifestation of EE in the caregivers of patients with BD. Hence, it is important to assess the caregiver’s of patients of BD for the perceived burden, specially the subjective burden. Accordingly, it can be said that addressing caregiver burden should be an important part of the psychosocial intervention for patients and caregivers of patients with BD.
Present study suggests that higher perception of abuse, is associated with more EE. In the regression analysis too, abuse emerged as an important predictor of EE. Abuse faced by the patient, per se can be considered as part and parcel of manifestation of EE and these associations are in the expected lines. Previous studies involving patients with BD have not looked at this association. Accordingly, it can be said that the clinicians managing patients with BD should always enquire about the possible/threatened/experienced abuse by the patients and overt abuse of the patient by the caregivers and should make efforts to address the same.
This study has certain limitations. The study included outpatients attending a General Hospital Psychiatry Unit. So, the results cannot be generalised to other patient populations. Assessment was cross sectional. So this study does not tell anything about change in EE over time and impact of expressed emotions on course and outcome of BD. Study was limited to those patients, who were in clinical remission; hence, the study does not provide any information about the EE, during the episodes. No attempt was made to study the association of expressed emotions with the personality of the caregivers. Further, the study was limited to family caregivers. An attempt must be made in future studies to overcome these limitations.
To conclude, present study suggests that in general sociodemographic and clinical factors do not have significant influence on the EE faced by the patients with the BD. Among the psychosocial variables, coping, caregiver burden, abuse and psychological morbidity among caregivers have significant impact on the EE. Accordingly, it can be said that psychosocial interventions, especially designed for the caregivers should be developed which should focus on enhancing adaptive coping and discouraging maladaptive coping. Additionally, these programmes should focus on reduction in the caregiver burden and abuse of the patients. These interventions will help in reducing the EE faced by patients with BD.