
Abstract
Background:
User participation is advocated on the basis that consumers know their own needs better than anyone else. Photovoice is a participatory research method that empowers the grass-root population to give voice on concerned issues for eliciting social change.
Aim:
This study explores the experience and impact of user participation in mental health services (MHS) in Hong Kong through photovoice. It also examines the effects of this method in studying user participation.
Method:
In this qualitative inquiry, authors, two peer researchers and three participants were involved in the various stages of research design, data collection and data analysis. Participants took photos showing their perception and experiences of being involved in different MHS systems. They shared their narratives through these images and reflected on the participatory experience of photovoice.
Results:
User participation was experienced as a gradual process of assuming control that involved personal responsibility, connection with peers, collaboration with staff, redefinition of boundaries and social inclusion. Meaningful participation gave rise to a sense of contribution, interpersonal connection and self-worth and transformed one’s identity. Participants enjoyed the mutual interaction and derived benefit from the photovoice process. Issues such as consent and confidentiality arose in implementation.
Conclusion:
Participation entails partnership among service users, providers and peers. Photovoice opens up new space for unfolding expert knowledge. Further application of this participatory approach with the local community is suggested in order to develop person-centered care.
Introduction
People with serious mental illness are often seen as impaired and thus discouraged from moving forward in their recovery by mental health professionals (Davidson, Tondora, Lawless, O’Connell, & Rowe, 2009). They are marginalized and face significant stigma (Mizock, Russinova, & Shani, 2014) that hinders their recovery and engagement in a meaningful and autonomous life in the community (Corrigan et al., 2012; Davidson & Roe, 2007).
User participation in mental health services
User participation in mental health services (MHS) is seen as the marker of recovery-oriented care (Tse, Siu, & Kan, 2013), contributory to empowerment (Tambuyzer, Pieters, & Van Aidenhove, 2011) and overall recovery (Omeni, Barnes, MacDonald, Crawford, & Rose, 2014). Hickey and Kipping (1998) define user participation as ‘the participation of service users in the decision-making process’ (p. 84) in terms of their treatment and life circumstances. It ‘signals a democratization of the relationships between service users and professionals’ (Elstad & Eide, 2009, p. 674). Despite barriers to this paradigm shift to a new partnership (Borg, Karlsson, & Kim, 2009; McDaid, 2009; Patterson et al., 2009; Storm & Davidson, 2010; Truman & Raine, 2002), service users are increasingly seeking to have a greater influence in decision making (Becker, Reiser, Lambert, & Covello, 2014).
Photovoice
How can research allow autonomous decision making of research participants in studying the issue of user participation? Photovoice is a strategy that provides people with cameras to photograph their perceived health and work realities (Wang, 1999) ‘with the ultimate goal of impacting systems and policy’ (Becker et al., 2014, p. 190). Its three main goals are to facilitate people to record and reflect strengths and concerns of the individual and the community, to foster critical dialogue and knowledge about the concerned issues through group sharing and discussion of their photos and to make those accessible to policymakers (Wang, 1999). It is a valuable method for capturing the narratives and voices of marginalized groups (Mizock et al., 2014) that may not be easily accessed through traditional research methods (Cabassa, Nicasio, & Whitley, 2013).
Several studies have applied the photovoice method to understand the experience of mental illness and recovery (Cabassa et al., 2013; Clements, 2012; Fleming, Mahoney, Carlson, & Engebretson, 2009; Mizock et al., 2014; Thompson et al., 2008). It has not yet been used to understand user participation in MHS.
Method
Applied as a means of community-based participatory research (CBPR), this photovoice study is part of a larger qualitative inquiry that used multiple methods to explore the experience and impact of user participation at different contexts of MHS within the non-Western culture of Hong Kong through service users’ perspective. It also examines photovoice as a method for empowering this marginalized group in participation and knowledge generation. The underlying assumption is that this CBPR method offers an alternative for genuinely engaging the experiential knowledge of mental health service users (Becker et al., 2014) and obtaining a better understanding of their concerned issue to inform policy and practices.
Setting and participants
Participants were recruited from community MHS including a halfway house (HWH), an integrated community center for mental wellness (ICCMW) and a self-help organization (SHO) for persons in recovery in Hong Kong. The SHO was operated by persons in recovery together with professionals. The ICCMW and HWH were operated by multi-disciplinary teams to offer case management and individual care planning to service users. The ICCMW also provided a wide range of training activities to service users and caregivers, and education programs to the public. Purposive sampling was applied to allow the selection of participants who are able to describe their rich experience (Marshall & Rossman, 1999, p. 15). Five participants with varied degrees of involvement in MHS were engaged through social workers in three local service agencies. One of them dropped out before the research began because of work commitments and another one dropped out after signing the consent in the first session owing to an unforeseeable personal circumstance. One female and two males with lived experience of schizophrenia or early psychosis participated in the 5-month study. The woman was an executive committee member of an SHO for persons with mental illness. The two men were service users of an ICCMW and an HWH, respectively, and recent graduates of a peer support worker training course.
Design
Ethical approval was obtained from the Human Research Ethics Committee for Non-Clinical Faculties of The University of Hong Kong. The authors (with professional backgrounds in academic research) and two peer researchers (recruited from an SHO) worked together to shape the research design. The study was structured along an adapted version of the nine-step strategy developed by Wang (2006).
During the research design meeting, issues of concern such as the rationale of using photography, focus of the research topic, choice and autonomy in participation, informed consent and confidentiality, duration of the study and literacy in using the digital camera were raised and discussed among the research team. The peer researchers then tested out the procedures and contributed to the final protocol. They found photovoice a useful method for recording and sharing life experiences, thus giving the team more confidence in its application.
Data collection
The study took place between May and September 2014. Informed consent and permission to show or to publish the photos were obtained from the participants. Participants were also asked to obtain informed consent from other persons shown in the photos. Each participant attended one individual and five group meetings of a duration of 1.5–2.5 hours during the 5-month study.
At the beginning, the first author introduced the study and the photovoice method and obtained written informed consent. A volunteer professional photographer then provided basic training on photography and the use of the camera. Each participant received a new digital camera and a notebook for the fieldwork. In the second meeting, participants elaborated their concept of ‘user participation’ as (a) self-directed decision and taking charge, (b) citizenship and community contribution, (c) advocacy and education, (d) reducing stigma associated with mental illness and promoting social inclusion and (e) peers supporting each other. Based on these meanings, they returned to the field to take photos that illustrated their ideas and concerns, perceived barriers and enablers of participation in MHS. Photo sharing was conducted with the SHOWeD strategy (Wang, 1999) during the second, third, fourth and fifth meetings. Although group meeting was the usual practice of photovoice, the fourth meeting was held on individual basis to allow more space and time for eliciting a deeper narration of the visual data generated by each participant and for discussing the analysis with them. Finally, an evaluation of the participatory experience and a discussion on potential dissemination strategies was conducted. The participants produced a total of 18 original photographs. Apart from the strategy of oral discussions and narrations of the photos, they were invited to produce the written interpretations of the photos after the last meeting so as to preserve the authenticity of their ideas and thoughts. The aims and processes of the various meetings were illustrated in Figure 1.
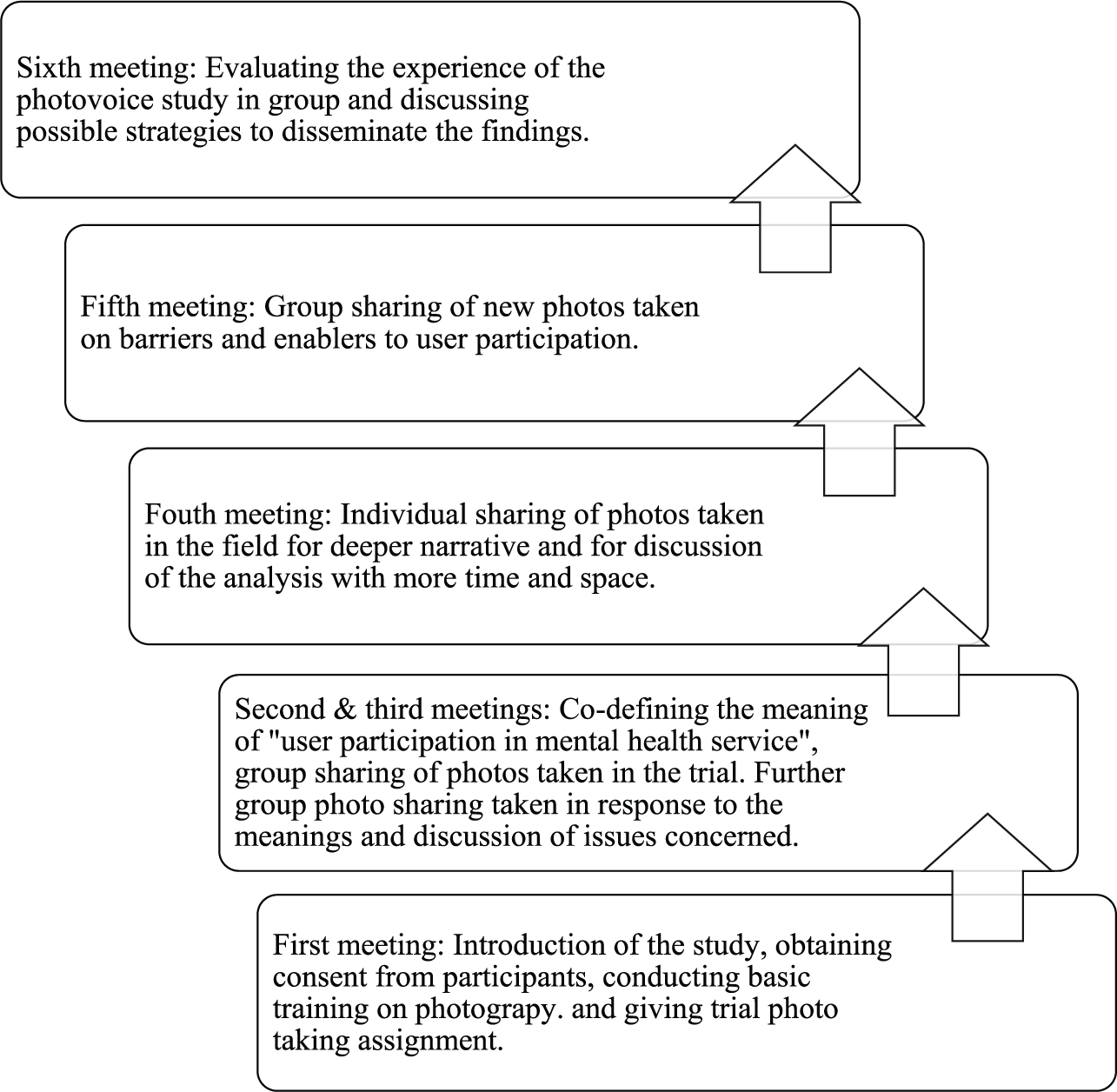
Flow chart showing the aims and process of the photovoice meetings.
Data management and analysis
The photovoice group and individual meetings were audiotaped. Transcription was done by a university psychology student who had received an instruction on how to conduct the transcription and signed a confidentiality agreement. To protect the identity of the research participants and others who appeared in the photos, the visual data were erased from the cameras once they had been imported to an encrypted computer designated for use in this research.
Thematic analysis was conducted with each participant’s photovoice pieces to give primary respect to the uniqueness of his or her individual idea and experience. The software NVivo (version 10.1.3) was used to support the analysis. The first author coded the transcripts of the meetings embedded with participants’ narrations of the photos, identified the key elements and clustered them into themes. The analysis was then reviewed by and discussed with the second author; deliberated and compared with the written narratives produced by the research participants. Agreement on the interpretations was reached between the researchers and the participants.
Research rigor
Collaboration with the community (Creswell & Miller, 2000) and the democratization of knowledge construction (Balazs & Morello-Frosch, 2013) are strategies for enhancing research credibility. In this study, peer researchers were involved in the research design and formulation of protocols. Data collection was exclusively conducted by the participants themselves as a community-driven process. The transformation of traditional power dynamics gave rise to the collaborative knowledge generation. Moreover, the data analysis was not only carried out by the first author but also the participants and the second author in order to achieve triangulation. These procedures helped to strengthen the trustworthiness of the study findings.
Results
Analysis of the photographs and narratives generated from the community’s perspective offers unique insights into the experience of user participation in MHS and CBPR within the current culture under study. At individual level, participants conveyed the core message of user participation as a process that was enabled through personal responsibility, connection with peers, collaboration with staff, but deterred by staff control, nonperson-centered care, distance and hierarchy. At service delivery level, participants found education and social inclusion as facilitative to combat against stigma and support user participation. For the purposes of this article and given the word limit, excerpts of photos are presented. Table 1 gives a summary of the characteristics of the three participants. Pseudonyms are used but demographic characteristics have been retained.
Characteristics of the photovoice participants.

ICCMW: integrated community center for mental wellness; SHO: self-help organization; MHS: mental health services.
Participant 1: Winnie
Winnie is a 49-year-old woman with almost 20 years’ lived experience of schizophrenia. She relied on intensive family support and experienced isolation from the outside world in her early years of struggle with mental illness. Through the invitation of a peer church fellow, Winnie began to attend a support group in an SHO for persons in recovery, reconnected with peers and gradually took up a leadership position in the SHO. For over 10 years, she represented the organization and her peers in meetings with policymakers and service administrators. Her participation was more demonstrated at service delivery and policy levels.
Core themes: peer support and social inclusion
Winnie’s photos centered on the theme of support and connection with peers which sponsored her active participation in service planning and delivery in the SHO. She valued interaction with and working alongside peers. She was proud to be a contributory advocate and a staff member of the SHO. Her story reveals the transformation of identity from a dependent daughter to an active peer leader through participation (Figure 2).

Second home.
If not for the establishment of this group, I would not have got involved and I would not be able to speak for the peers.
By founding a mission to enhance people’s awareness of mental health and recovery, Winnie also engaged herself in the planning and delivery of mental health education for peers and the general public as a form of meaningful participation against stigma (Figure 3).

Be a fulfilled person in recovery.
Participant 2: Billy
Billy is a 23-year-old man who has lived experience of early psychosis since he was 15. He was a fresh graduate of a training program for peer support workers when he first engaged in the study. Later, he was hired as a peer support worker in an ICCMW. He saw himself as being in an advanced stage of recovery. His participation experiences were represented at individual care and service delivery levels. Billy spoke about his struggle over mental illness and saw significance of user perspective toward person-centered care.
Core themes: user perspective and power disparity, education against stigma and personal responsibility
Initially, Billy shared a photo showing the image of the ceiling above his bed to illustrate his struggle with the loss of personal development in the midst of mental illness and stigma. Without regular daily engagement, he found he had little energy and motivation to leave his bed. He hoped these days would come to an end. Through the metaphorical image of a spread of healthy food his mother had prepared for him and his brother without seeking their views, he commented that a professional perspective might not necessarily match the needs of service users and highlighted the significance of the service user perspective in the delivery of person-centered MHS. A power disparity within the MHS system was further illustrated by a close-up photo of a bell positioned at the counter of a community service center, used for summoning the staff. This image spoke of the distance, boundaries and differentiation between service providers and users, posing barrier to the engagement and involvement of the latters (see Figure 4).

Need to see the staff? Ring the bell!
After Billy had become a peer support worker, he shared a photo of his bookshelf with educational books on mental health (Figure 5). He began to acquire knowledge of mental health and advocated with the public to understand more about mental illness. This new involvement in service delivery not only expanded his connection with peers but also cultivated his empathy for them. Toward the end of the study, Billy highlighted the significance of personal responsibility in recovery and participation through a photo capturing the sunshine on the street outside the window of his home. A sense of personal agency was suggested as key to reclaiming control in life.

Learn before you judge.
Although it is uncertain whether this energy and more active self was directly associated with his participation in MHS as a peer support worker, this new role and experience seemed to demonstrate benefit and meaning to him.
Participant 3: Andrew
Age 25, Andrew has lived with the experience of schizophrenia since adolescence. He lived in a HWH where he was dissatisfied with the routine daily training and wished for real employment. On graduation from the peer support worker training, Andrew hoped to become a peer support worker to attain recovery and live a meaningful and independent life. His experience of participation was more exhibited at individual level. Personal responsibility, loss of control and collaborative position in service care were central to his photos and narratives.
Core themes: personal responsibility, power inequality and collaboration with staff
Similar to Billy, Andrew saw personal responsibility as key to recovery, participation and control in life. Through the image of a hawker making a rice roll with his own hands to earn a living, Andrew remarked that persons in recovery were responsible for their own mental health and social recognition. Despite his efforts, Andrew experienced barriers to achieving independent living and exercising free will in the hostel. He told of this feeling through a photo capturing a planter space in the hostel that could not be accessed by service users without staff permission. The feeling of being trapped and hope to fly away was reinforced in another photo showing the common area with fenced windows where he attended routine daily training (see Figure 6). His photos spoke of confined involvement and power inequality experienced in the service.

Common hall of my hostel.
Although Andrew was discontented over the service care, he chose to cooperate with staff rather than speaking up. To him, ‘being collaborative’ was a means to facilitate mutually beneficial outcomes. He took personal responsibility for maintaining communication with his occupational therapist about his own condition and goals in the recovery journey, indicating his sense of agency within individual care.
Andrew’s initial photo pieces expressed a strong sense of personal responsibility for recovery. However, he felt trapped in the services and experienced a loss of freedom, boredom and lack of meaning in life. His photovoice pieces suggested that participation could not be realized through personal responsibility alone but in collaboration with staff. Paradoxically, staff control and power inequality existed in the MHS and posed challenges to his meaningful involvement. After Andrew had graduated from the peer support worker training, he felt more hopeful and found himself climbing toward the hilltop to achieve his goal (see Figure 7), indicating that the anticipated opportunity and advancement of participation to service delivery offered him a sense of meaning in life.

Hilltop from my home.
In summary, photovoice pieces of the participants revealed that personality responsibility, peer support, collaboration with staff and social inclusion gave rise to user participation in individual care and service delivery while staff control, nonperson-centered care, distance and hierarchy posed hurdles to meaningful involvement. Participants also looked upon higher level of involvement in service planning and delivery.
Apart from the experience of being involved in MHS, participants found that photovoice could actualize autonomous participation, allow individualized expression and enhance self-understanding at the individual level. At the group level, it fostered interaction and mutual learning among participants.
Exercising free will and autonomy
Two participants highlighted that photovoice had allowed them to exercise autonomy and free will about what to capture. As Andrew described it,
Um, follow the mind. That is actually, the free flow of thoughts and then taking the photo with the feeling that comes. Intuition is very often a first person’s perspective.
They differentiated it from traditional methods of responding to predesigned questionnaires. Winnie described it as nonjudgmental:
Had no right and wrong. It is the subjective feeling. Um, you have great autonomy.
Actualizing authentic participation
As active agents rather than passive research subjects, participants experienced authentic participation and fluid interpersonal encounters with a sense of agency in the group meetings as Winnie described:
This is participation. That means we are personally involved in the process … This kind of process is pleasant. I also learned about the mind of the young persons … So compared to the questionnaire in which we only respond ‘agree’ or ‘disagree’, or give a score, I think [the difference] to me is the participation. Yes.
For Billy, the process had allowed him to give meaning to his experience:
It is the wish of making our own interpretation. So you and me, especially persons in recovery receiving services, we know and understand more about rehabilitation and hence identify different meanings.
Acknowledging individualized expression
Participants saw photography as an alternative and novel means that went beyond numerical data for expressing unique meanings, feelings and thoughts. Billy remarked,
I think there are things that numbers cannot represent. For example, on the notion of agreement, with 5 representing highly agree, if to say very agree but have some reservation, then to select 4 or 5? And does my 4 the same as your 4? Or my 5 the same as your 5? No one knows.
Enriching self-understanding
Participants described photovoice as a means for recording and reflecting their lives that served to enhance self-understanding and enabled others to access a deeper understanding of their thoughts and feelings. Andrew said,
It is something I want to tell my friend, reflecting on the details and process in life and what it is all about. Not to tell others what the photo represents with intention but what just comes from the mind.
In effect, participating in the study gave Winnie the opportunity to find out more about her capabilities and to stretch her limits:
It was, was a new attempt and new discovery. And in the process of photography, I realized that I was capable. Not to count whether the photos met the standard, … at least I stretched beyond my limits.
Although participants reported a sense of autonomy, interpersonal enrichment, personal reflection and breakthrough, the method also triggered uncomfortable feelings and met challenges in its implementation.
Concern about consent and confidentiality
In practice, participants expressed concern and found it challenging to obtain consent from other people appearing in the photos. As a result, two of them avoided taking photos of other people. This might suggest the complexity of observing research ethics in the participatory approach. As Andrew remarked, ‘some people might say they agreed on the surface but actually resist deep down. Then it would be embarrassing’.
Confidentiality was another concern indicated by participants. One who generated a photo in a service agency urged the researcher to hide any identifier of the organization when the findings were disseminated. Acknowledgement of these concerns and reassurance of confidentiality was essential in enhancing participants’ feeling of safety and involvement.
Psychological pressure
Winnie reflected on the demands of participation and the pressure of responsibility:
Um I think at this very moment, it is a relief to me. It is true because I have told you in the first meeting that I was unsure since my emotional and physical conditions, time and so on were hard to match … And now, it was accomplished. At least [I] accomplished all.
Moreover, participants also found it inconvenient to carry the camera around on regular basis and felt pressure to take care of it.
To summarize, the photovoice and group process enabled participants to stretch beyond their comfort zone and the traditional ways of being involved in research. It also facilitated mutuality and interpersonal connection among them despite the drawbacks.
Discussion
The results of this study are twofold. First, they extend our understanding of user participation in MHS in a non-Western culture of Hong Kong from the users’ perspective in a way that might not have been achieved using traditional research methods. Second, they reveal the benefits and challenges of using photovoice as a CBPR strategy. The process has a value in reaching a deeper understanding of factors that enable or deter user participation.
User participation in Chinese culture
From the photovoices of the three participants, it can be seen that user participation starts from being responsible for and involved in one’s own care and recovery. It is a gradual process of assuming control in services and in life that involves complex interactions with peers and care professionals. On one hand, findings indicate the presence of distance and power disparity between service providers and users, posing major hurdle to participation in individual care. On the other hand, a tendency to cooperate with professionals despite the lack of control was expressed by a participant. The parallel existence of these may suggest the Confucian influence of social hierarchy and paternalistic culture. It may also reflect the observant of Confucian doctrine for maintaining social order and harmony rather than a call for power shift.
These findings echo existing literature which highlights that relationship between service users and practitioners (Newman, O’ Reilly, Lee, & Kennedy, 2015), and staff control as influential toward user participation (Broer et al., 2014; Petersen, Hounsgaard, Borg, & Nielsen, 2012). In Hong Kong, service management largely remains in the control of professionals (Leung & Lam, 2014). There is skepticism around involving peers in service delivery (Ng, Pearson, Pang, Wong, & Chan, 2013). Such a deep-rooted paternalistic and relational culture is likely to challenge and complicate the enactment of personal responsibility in the process of participation and recovery. Enabling user participation thus demands the commitment of service systems (McDaid, 2009; Storm & Davidson, 2010), breaking boundaries toward mutuality and partnership between staff and service users (Leung & Lam, 2014). It would call for a paradigm shift among care professionals and the commitment of resources for peer support services and public education, in parallel with the cultivation of personal responsibility among service users.
The results of this study shed further light on the significance of peer support, person-centered services and social inclusion as means of empowering participation. The findings also show that participation in advocacy, self-help and service delivery all brought forth a sense of contribution and interpersonal connection.
Benefits and challenges of the participatory experience
Methodologically, photovoice has demonstrated several benefits: autonomous and authentic participation, individualized expression, enriched self-understanding and personal breakthrough. These findings support and extend existing literature on the effects of visual images and narratives (Mizock et al., 2014) in facilitating marginalized groups ‘to access their experience and construct meaning of their experience in order to present their stories to themselves and to others’ (Clements, 2012, p. 789).
The interactive relation between the participants and the researcher also gave evidence to the enabling effect of mutual partnership toward participation. This was indicated by one of the participants, Winnie, who hesitated to commit in the study at the first group session because of her busy schedule, unstable emotional condition and lack of knowledge of photography but finally decided to join as the researchers acknowledged her concerns and respected her autonomous decision. By the end, she was happy that she had departed her comfort zone and produced visual images that told one’s journey of user participation in service delivery through peer support. The actual experience from this CBPR process proved the critical role of mutual relationship between the professional and the community in facilitating meaningful involvement and contributed to a richer understanding of the issue under study.
Although this study proved photovoice a useful, non-threatening and empowering CBPR method, several challenges were also faced. The application of CBPR demands a broad set of essential competencies and qualities from researchers (Faridi, Grunbaum, Gray, Franks, & Simoes, 2007; Michalak et al., 2016) and yet it is not often used in Hong Kong and other Chinese communities (Leung & Lam, 2014). While the lack of local experience and literature in this creative method provides flexibility and opportunity for implementation, research ethics and the use of digital cameras as data collection tools were novel to some peer researchers and participants, especially those in middle age. Some expressed anxiety despite the orientation and introductory training provided while some reported difficulties in carrying the camera around for data collection.
Time consumption is another issue commonly identified in conducting CBPR (Cornwall & Jewkes, 1995; Israel, Schulz, Parker, & Becker, 1998). This study confirms that the photovoice method demands a time commitment for rapport building, training, open dialogue and coordination. Participants also suggested various options for dissemination strategies including conference presentations, newsletters for MHS and sharing sessions with the community. However, time and resource constraints presented barriers to more extensive action. To support the full participation of service users in collaborative research, the allocation of research fund in this area is suggested.
To effect the future application of photovoice, the development of systematic training for researchers and community participants is recommended. Involving service users in the production of training materials may help bring the method closer to their understanding and learning. Careful consideration should be given to addressing participants’ ethical concerns, prior knowledge of information and communication technology, and identifying user-friendly devices for data collection in order to avoid the risk of pressure and disengagement. Ongoing discussion on options for coping with the potential challenges against obtaining consent is also recommended.
Limitations and conclusion
This study was the first photovoice inquiry conducted to understand the experience of user participation within the context of MHS in Hong Kong. Such a creative approach was well suited to exploring the phenomenon in depth in a way that would be difficult to achieve using structured questionnaires (True, Rigg, & Butler, 2015). Findings generated from the original perspectives of research participants have expanded our understanding of MHS user participation in a non-Western culture and prompted to barriers that needed to be addressed.
However, some limitations should be noted. First, participants were involved in MHS not only as service users but also as providers and advocates. The perspectives of service users with a lesser degree of participation were not captured. Second, this study was conducted without a formal research grant. Owing to the constraints on funds, time and other resources, the project size was confined. Moreover, peer researchers and participants were not involved in every aspect of the study as is stipulated in CBPR (Schneider, 2012).
Participation entails a partnership between professionals and grassroots members to stretch the boundaries beyond the traditional status quo. Using the photovoice method, this pilot study illustrates the complementary rather than competing values of expert and empirical knowledge (Roe & Davidson, 2005). Further and larger scale of research in this domain may help contributing to wider and deeper understanding of the issues and effects identified in this study. We hope that more researchers and mental health practitioners will explore the use of participatory approaches with the community for advancing knowledge and practice toward quality care.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.