
Abstract
Background:
The mental health treatment gap for youth in low- and middle-income countries (LMICs) is substantial; strategies for redress are urgently needed to mitigate the serious health and social consequences of untreated mental illness in youth.
Aims:
To estimate the burden of major depressive episode (MDE) and posttraumatic stress disorder (PTSD) as well as utilization of care among Haitian youth in order to describe the mental health treatment gap in a LMIC setting.
Methods:
We estimated the point prevalence of MDE, PTSD, and subthreshold variants in a school-based sample of youth (n = 120, ages 18–22 years) using a modified Structured Clinical Interview for DSM-IV-TR Axis I Disorders (SCID)-based interview and examined treatment utilization among those receiving one of these diagnoses. We assessed additional psychopathology with self-report measures to examine validity of study diagnostic assignments.
Results:
The combined prevalence of full-syndrome or subthreshold MDE or PTSD was high (36.7%). A large majority of affected individuals (88.6%) had accessed no mental health services in the health sector, and 36.4% had accessed no care of any kind in either the health or folk sectors in the past year.
Conclusion:
Findings demonstrate a high mental health burden among Haiti’s youth and that many youth with MDE and PTSD are not accessing mental health care.
Introduction
Mental and substance use disorders remain the leading health contributors to disability both globally and in low- and middle-income countries (LMICs; Institute for Health Metrics and Evaluation (IHME), 2016), but the majority of affected individuals in LMICs do not receive care for serious mental illness (Demyttenaere et al., 2004). For example, only 1 in 27 individuals with major depression in a LMIC receives minimally adequate treatment (Thornicroft et al., 2017). Although reasons underpinning the mental health treatment gap – the proportion of those with mental illness who do not receive care – are multi-factorial, developing and deploying strategies to expand access to quality mental health services are a focus for its redress (Becker & Kleinman, 2013). Strategies for improving care access across diverse regions and populations can be enhanced by understanding patterns of treatment utilization and particular barriers to care within demographics defined by age and local social context.
Mental disorders are the greatest contributor to disability in youth worldwide as well (Gore et al., 2011), but the majority of affected youth do not receive care for their mental illness (Patton et al., 2012). Unfortunately, untreated mental disorders in youth carry the risk for serious downstream health and social consequences. For example, a longer duration of mental disorder in adolescence is among the strongest predictors of adult disorder (Patton et al., 2014). Moreover, adolescent mental illness is associated with poorer social and economic outcomes 10 years later and greater risk for other noncommunicable diseases (Ngo et al., 2013). Because early detection and treatment can reduce the chronicity and severity of the primary mental disorder and prevent secondary disorders (Ghio, Gotelli, Marcenaro, Amore, & Natta, 2014; McGorry, Purcell, Goldstone, & Amminger, 2011; Patton et al., 2014), timely intervention for youth is critical for their future health and well-being. This treatment gap, moreover, is most pronounced in LMICs where an estimated 10%–20% of adolescents have a mental disorder (Kieling et al., 2011; Patel, Flisher, Nikapota, & Malhotra, 2008). Barriers to care include health systems constraints relating to an inadequate mental health workforce and public sector budget allocation to meet needs, as well as a variety of factors that influence help-seeking for mental illness. For example, relevant cultural factors include local idioms of distress and explanatory models that render care-seeking in the health or folk sectors germane (e.g. Kleinman, 1980). Similarly, social structural factors, such as political and economic disenfranchisement, impede help-seeking (Farmer, 2010). Impacts of the latter – such as legal factors, unaffordable costs, and poor access to transportation – are more pronounced for youth (Patton et al., 2016). Understanding factors underpinning user demand and accessibility of services are salient to the optimization of interventional approaches and targets to reduce the mental health treatment gap in LMICs.
This study seeks to characterize the local mental health treatment gap among youth in Haiti, a low-income country in the Caribbean. In 2010, a major earthquake centered near Port-au-Prince resulted in devastating casualties, infrastructural damage and displacement in Haiti. Given the elevated risk for depression and posttraumatic stress disorder (PTSD) following humanitarian emergencies and disasters (Goldmann & Galea, 2014; Marquez, 2016) and the likely impacts of this ‘acute-on-chronic’ event (Farmer, 2011) on mental health in the setting of longstanding social adversities (Raviola, Eustache, Oswald, & Belkin, 2012; World Health Organization (WHO), 2010), we expected depression and PTSD to be prevalent among youth in Haiti’s Central Plateau. Furthermore, although rigorous epidemiologic data on mental disorders in Haiti are quite limited (cf. WHO, 2010), post-earthquake data from self-report or inventory assessments support a high burden of depression and PTSD among youth (Blanc, Bui, Mouchenik, Derivois, & Birmes, 2015; Cénat & Derivois, 2014, 2015) and adults (Cerdá et al., 2013) living in Port-au-Prince, as well as prevalent depressive symptoms among adults in Haiti’s Central Plateau (Wagenaar, Hagaman, Kaiser, McLean, & Kohrt, 2012). Similar to the situation in other LMICs, accessibility to mental health services in Haiti has been severely constrained by resource shortfalls of all types and centralization of services in urban areas (WHO, 2010, 2011). Significant stigma toward mental illness also exists in Haiti, and there is little exposure to and endorsement of biomedical explanations of mental illness (Khoury, Kaiser, Keys, Brewster, & Kohrt, 2012; Wagenaar, Kohrt, Hagaman, McLean, & Kaiser, 2013). Nonetheless, there is inadequate understanding about help-seeking for mental illness among Haitian youth to inform development of community-based mental health care in Central Haiti to serve them (Raviola et al., 2012).
This study’s aims are to (1) estimate the point prevalence of depression and PTSD among a community-based sample of secondary school youth in the Central Plateau of Haiti, (2) estimate 12-month utilization of health system–based care for mental health, and (3) describe the unmet need for mental health treatment in this sample. An empirical understanding of local mental health burden and associated unmet need can strategically inform further development of approaches for promoting the mental health of Haitian youth and also has potential application for understanding and closing the mental health treatment gap among youth in other low-income settings.
Methods
Cross-sectional study data were collected during the baseline assessment phase of the Teacher-Accompagnateur Pilot Study (TAPS), a school-based pilot mental health intervention in Haiti’s Central Plateau in October and November 2013 (Eustache, Becker, & Ekip Wozo, 2014; Eustache et al., 2017). The corresponding study protocols – including components presented here – were approved by both the Institutional Review Board (IRB) of the Harvard Faculty of Medicine and the Zanmi Lasante (ZL) Ethics Committee. Methods described here represent those most relevant to this study’s aims (see Eustache et al., 2017, for additional details about study procedures).
Study sample
The study sample was drawn from four participating schools in Haiti’s Central Plateau. Students meeting eligibility criteria (actively enrolled in a participating school, ages 18–22 years) were randomly selected within each school from school registers (n = 33–41 per school). Across all schools, 145 eligible students were invited to participate, and of these, 121 students were enrolled in the study and completed the assessment. Subsequently, one participant withdrew consent and requested that his or her study data be discarded, yielding a revised study sample of n = 120. The response rate was 82.8% in total and at least 78.0% in each school. Study participants received lunch, but there was no monetary compensation for participation.
Procedures
After providing informed consent, participants responded to a battery of self-report psychosocial assessments and subsequently underwent a structured research interview. Assessments were in Haitian Creole at the students’ respective schools. The self-report assessments were proctored by members of the study team and completed during a single day. Research interviews were conducted by (or co-facilitated with) clinician–investigators with local experience in diagnostic assessment of mental disorders. In total, 85.8% of the interviews were completed within 2 days of a student’s self-report assessment, and all interviews were completed within 15 days of the self-report assessment. Following the research interview and independently of the study, study participants were encouraged to undergo an onsite clinical interview with a mental health clinician (see Eustache et al., 2017) to follow up on clinical concerns or questions and facilitate a path to care, if appropriate.
Assessments
With the exception of questions about health-care utilization developed for this study, study psychosocial assessments were drawn from or adapted for use from existing measures (Table 1). Written self-report assessments were translated from English to Haitian Creole using an iterative process involving contributions from three or more members of the study team as follows (cf. Bhui, Mohamud, Warfa, Craig, & Stansfeld, 2003): forward translation and independent back translation by two or more bilingual members of the study team, comparison for discrepancies by one or more native English-speaking investigators, and adjustments by one or more investigators to optimize idiomatic and readily comprehensible usage. Assessments were finalized after piloting them with an independently selected sample of Haitian students (n = 12).
Measures used for assessment.

WHO: World Health Organization, DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.); DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.).
Study criteria for diagnostic assignment of subthreshold MDE and subthreshold PTSD among participants not meeting full-syndrome criteria.
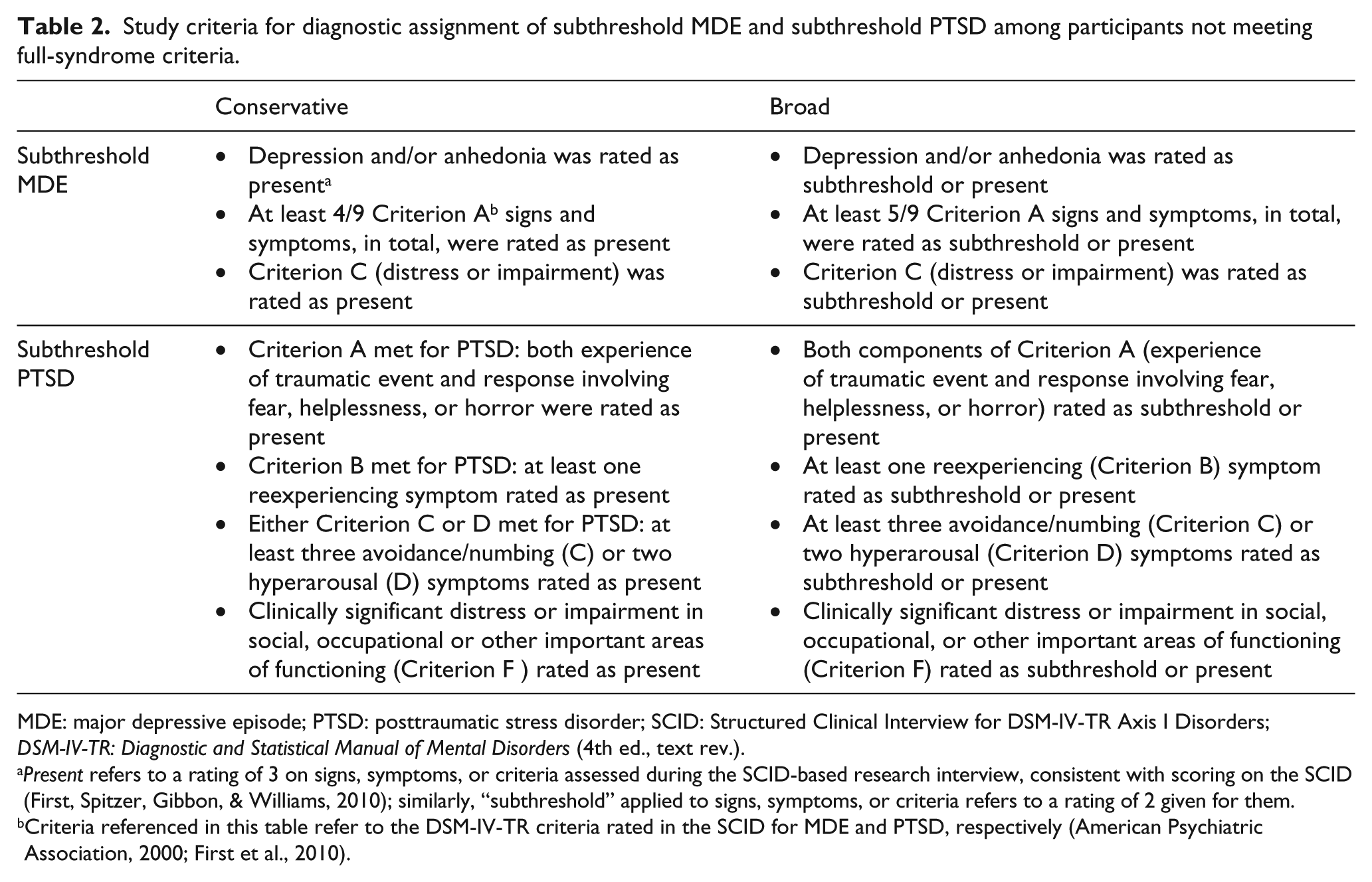
MDE: major depressive episode; PTSD: posttraumatic stress disorder; SCID: Structured Clinical Interview for DSM-IV-TR Axis I Disorders; DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.).
Present refers to a rating of 3 on signs, symptoms, or criteria assessed during the SCID-based research interview, consistent with scoring on the SCID (First, Spitzer, Gibbon, & Williams, 2010); similarly, “subthreshold” applied to signs, symptoms, or criteria refers to a rating of 2 given for them.
Criteria referenced in this table refer to the DSM-IV-TR criteria rated in the SCID for MDE and PTSD, respectively (American Psychiatric Association, 2000; First et al., 2010).
Data analyses
All statistical analyses were conducted in SPSS 23 (IBM Corp., 2015). Descriptive statistics were calculated as frequencies for categorical data and means with standard deviations (SDs) for continuous variables. For all diagnostic categories corresponding 95% confidence intervals were calculated using the Wald method except when n ⩽ 5, in which case the exact method was used. Chi-square tests were used to test for differences in prevalence by gender. In order to examine construct convergent validity of the Diagnostic and Statistical Manual of Mental Disorders (DSM; APA, 2000)-based study diagnostic assignments, we used self-report data from the following assessments (as adapted for this study; Table 1): Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977), Global School-based Health Survey (GSHS; WHO, 2013a, 2013b), Reaction of Adolescents to Traumatic Stress (RATS; Bean, Eurelings-Bontekoe, Derluyn, & Spinhoven, 2004b) and Stressful Life Events Checklist (SLE; Bean, Eurelings-Bontekoe, Derluyn, & Spinhoven, 2004a).
Data management
Raw self-report data were entered into an Excel file and verified. Missing data for the CES-D and RATS were handled as follows: We used mean imputation for observations missing 10% or fewer of responses and excluded observations missing >10% of responses (n = 9 and n = 5, respectively, for CES-D and RATS). Complete data were available for health-care utilization analyses. All other deviations from the sample size of n = 120 for individual items are noted in tables and text.
Interviews were completed by each respondent. Written ratings data recorded on the paper copies of the interview guides were entered into an Excel spreadsheet for analysis. In addition, we transcribed and translated all narrative responses as well as summary and margin notes recorded on the interview guides; these were also entered into a spreadsheet for review alongside numeric ratings. Our algorithm for diagnostic assignment handled missing data from the research interview as described in Table 1.
Procedures for study diagnostic assignment
We used data from interviews based on content adapted and abridged from the major depressive episode (MDE) and PTSD modules of the Structured Clinical Interview for DSM-IV-TR Axis I Disorders (SCID; First, Spitzer, Gibbon, & Williams, 2010) to make study diagnostic assignments. The interviewer’s summary assessment was the primary basis for a diagnostic assignment as MDE or PTSD. Members of the study team also considered all written information recorded on the interview form about symptoms, presentation, and context – including any narrative data, margin notes, and summary ratings data – to reach consensus about diagnostic assignments. In addition to the standard SCID diagnostic summary rating questions in the respective MDE and PTSD modules, we added a second study-specific item asking the interviewer to affirm whether the diagnosis was present. This item allowed additional response options (e.g. to indicate that only partial criteria were met or a diagnosis could not be ascertained). The interviewer’s summary assessment of the presence of a disorder in response to at least one of these items was required for a study diagnostic assignment of MDE or PTSD. In addition, we reviewed and considered interview margin and summary notes for contradictory or qualifying information.
Next, we systematically reviewed all of these interview data – including written summary ratings, narrative responses, and margin notes recorded on the paper copies of the SCID-based interview guides – for evidence of subthreshold MDE or PTSD. We followed study operational criteria (described below and in Table 2) and reached consensus among three or more study investigators regarding the presence of each of these subthreshold diagnoses for each participant.
Diagnostic assignments of subthreshold MDE
When participants did not meet study criteria for MDE, we assigned a study diagnosis of subthreshold MDE to participants who nonetheless met either of the two sets of corresponding study criteria (Table 2). These criteria are based on guidance in SCID instructions that subthreshold diagnosis can be assigned when an individual is deemed likely to meet full criteria (First, Gibbon, Spitzer, & Williams, 2002). We operationalized our “conservative” criteria to assign a subthreshold diagnosis of MDE when Criteria A, B and C were met, except for the presence of only four of the five required neurovegetative symptoms. In addition, we assigned a study diagnosis of subthreshold MDE when clinicians had given a rating of at least subthreshold for signs and symptoms of Criteria A–C that would have, if all present, been consistent with full-syndrome MDE (cf. Schnurr, Friedman, & Rosenberg, 1993).
Diagnostic assignments of subthreshold PTSD
When participants did not meet study criteria for PTSD, we assigned a study diagnosis of subthreshold PTSD to participants who nonetheless met either of the two sets of corresponding study criteria (Table 2). Criteria sets were based on practices described in the literature. The first, which we termed “Subthreshold PTSD (Conservative),” was based on the approach described by Blanchard, Hickling, Taylor, Loos, and Gerardi (1994). We selected this approach given its established use (see Brancu et al., 2016; Franklin, Sheeran, & Zimmerman, 2002) and that it is conservative in requiring two full symptom clusters to be met (Cukor, Wyka, Jayasinghe, & Difede, 2010). The second, which we termed “Subthreshold PTSD (Broad),” is based on the approach described by Schnurr and colleagues (1993). This method allows for a subthreshold diagnosis to be assigned when signs and symptoms otherwise adequate to meet diagnostic criteria are present but do not reach threshold levels.
Validation of study diagnostic assignments
To assess the validity of study diagnostic assignments, we examined convergent validity by examining between-group differences (case vs noncase) with respect to measures of depressed mood and trauma exposure generated by self-report assessments. First, internal consistency reliability for the CES-D and RATS was estimated with Cronbach’s alpha. Wilcoxon–Mann–Whitney tests were used to compare (1) MDE cases versus noncases and (2) MDE cases and/or subthreshold variants versus noncases on CES-D- and GSHS-based measures of depressive symptomatology. A parallel set of Wilcoxon–Mann–Whitney tests were used to compare (1) PTSD cases versus PTSD noncases and (2) PTSD cases and/or subthreshold variants versus noncases on SLE and RATS measures of trauma exposure and PTSD-related symptomatology.
Assessment of the gap between identified mental health needs and care utilization
We used self-report responses concerning health-care utilization to calculate the proportion of participants within each of these study diagnostic categories who had not accessed health care for any mental health problem in the past 12 months and who also had not accessed health care for any health problem during the same time period. We operationalized “unmet need” for mental health services as the former.
Results
Sociodemographic characteristics, health-care utilization, and barriers to care
Table 3 displays a summary of socioeconomic characteristics and health-care utilization among participants. Two-thirds of sample participants were male; the mean age was 19.5 years. Socioeconomic indicators consistent with poverty were notable for the prevalence of food insecurity and lack of indoor latrine as well as difficulty in affording health care, medicines, or transportation to health services. For example, three-quarters of respondents reported having at least 1 day without any food over the preceding 3 months, and one-quarter did not have a latrine in their home. Moreover, a majority of respondents (59.5%) reported difficulty in paying for hospital or clinic-based care or difficulty in paying for medicine (50.8%). Similarly, nearly one quarter of participants reported difficulty in paying for medicine from a healer or houngan.
Student sample characteristics, n = 120 unless otherwise indicated.
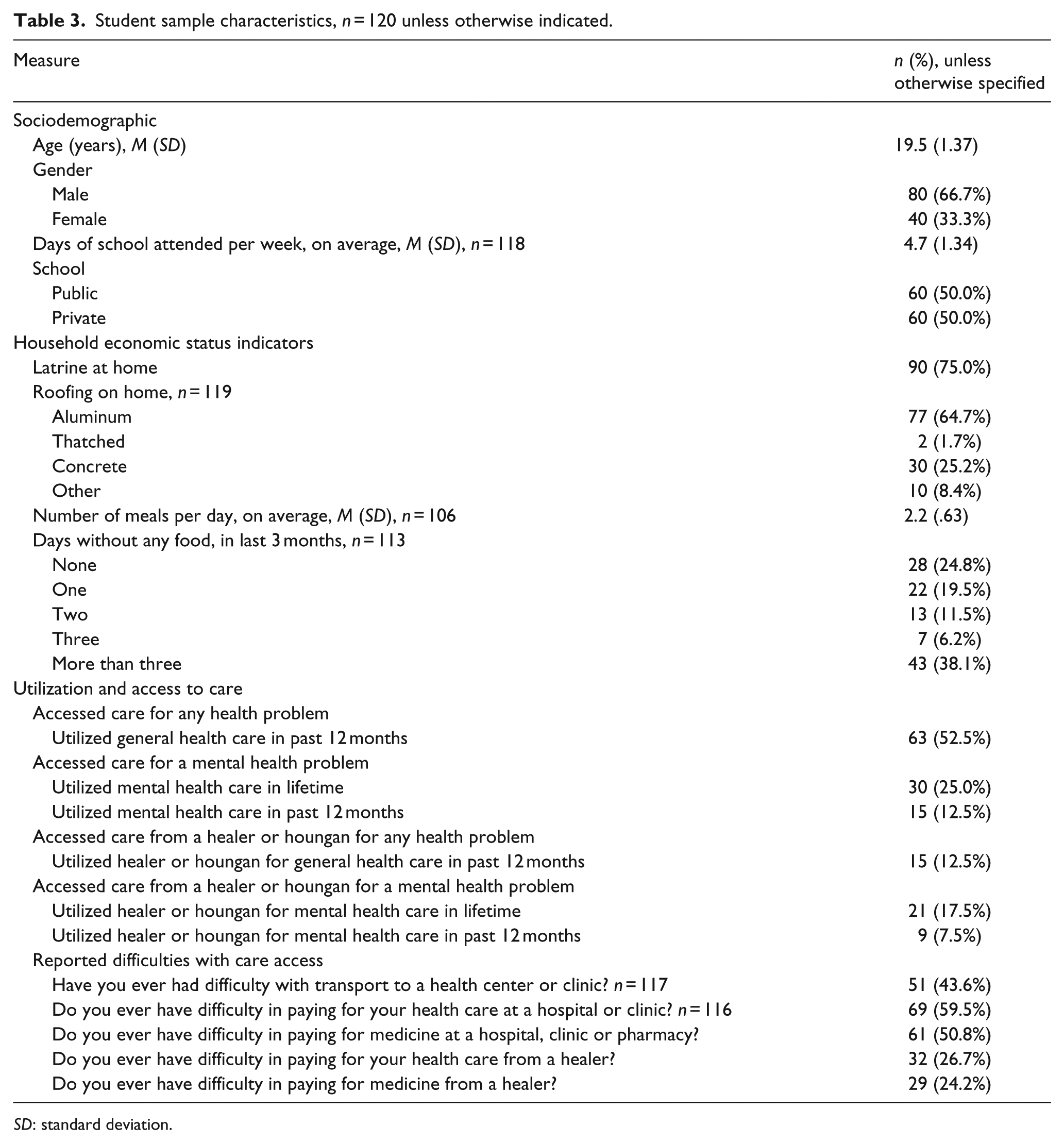
SD: standard deviation.
Health services were only accessed by slightly over half of the participants within the past year. During this timeframe, 55.0% of the participants accessed either general or mental health care through the health system, and an additional 4.2% accessed care only through the folk sector (i.e. by visiting healers or houngans); however, 40.8% of the sample did not access any of these kinds of care within the past 12 months (Table 4). Moreover, only 12.5% of the participants had accessed mental health care through the health system, and an additional 5.8% had addressed mental health problems with a healer or houngan. Thus, the majority of the participants (81.7%) had not accessed any specific mental health care in the past year.
One-month point-prevalence estimates and 95% confidence intervals for MDE, PTSD, subthreshold MDE and/or PTSD, and comorbid MDE and PTSD.
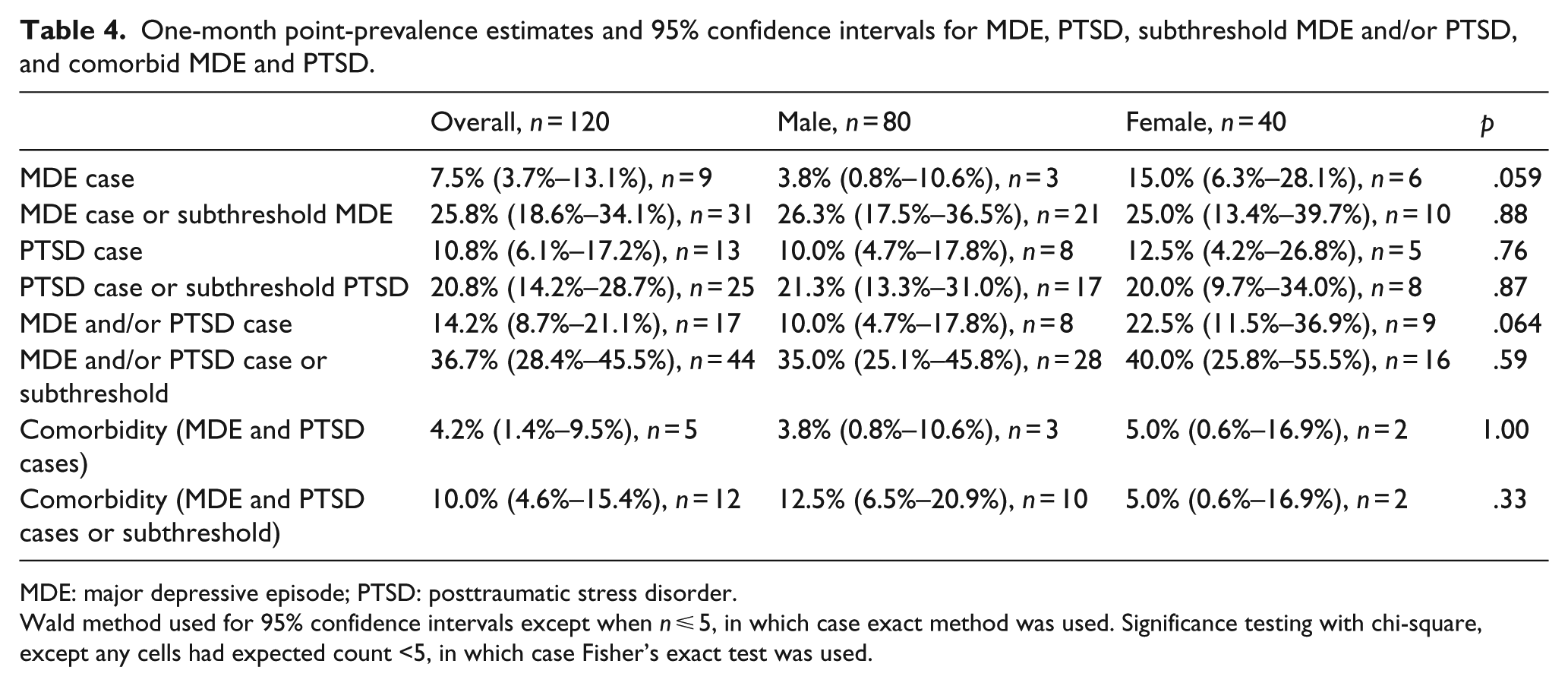
MDE: major depressive episode; PTSD: posttraumatic stress disorder.
Wald method used for 95% confidence intervals except when n ⩽ 5, in which case exact method was used. Significance testing with chi-square, except any cells had expected count <5, in which case Fisher’s exact test was used.
Prevalence of MDE, PTSD, and subthreshold variants
Table 4 displays the 1-month point-prevalence estimates for MDE, PTSD, and their respective subthreshold variants. The prevalence of MDE was 7.5%; the combined prevalence of MDE and MDE subthreshold variants was considerably higher at 25.8%. The prevalence of PTSD was 10.8%; the combined prevalence of PTSD and PTSD subthreshold variants was 20.8%. Overall, the 1-month prevalence of either MDE or PTSD was 14.2% in our study sample; the prevalence of any one of the study diagnoses (MDE, PTSD, and/or a subthreshold variant) was high at 36.7%. We noted that 4.2% of the study participants had comorbid MDE and PTSD. Although we did not observe a gender difference for either PTSD or comorbid MDE and PTSD cases, we observed a marginally significant higher prevalence of MDE for females (15.0% females vs 3.8% males; p = .059).
Convergent validity
Table 5 shows overall and group means for depressive symptomatology measured by the CES-D and GSHS questions across groups defined by diagnostic assignments relating to MDE. Also displayed are overall and group means for measures of stressful life events/traumatic exposures and PTSD-related symptomatology, across groups defined by diagnostic assignments relating to PTSD. MDE cases had significantly higher levels of depressive symptomatology than noncases. Similarly, the group comprising MDE case and subthreshold variants also had significantly higher depressive symptomatology than all others. Parallel analysis for PTSD showed similar results: PTSD cases had significantly higher stressful life event/traumatic exposures and PTSD-related symptomatology than noncases. The group comprising PTSD cases and subthreshold PTSD variants also had significantly higher stressful life event/traumatic exposures and PTSD-related symptomatology than all others.
Convergent validity of MDE and PTSD diagnostic assignments.
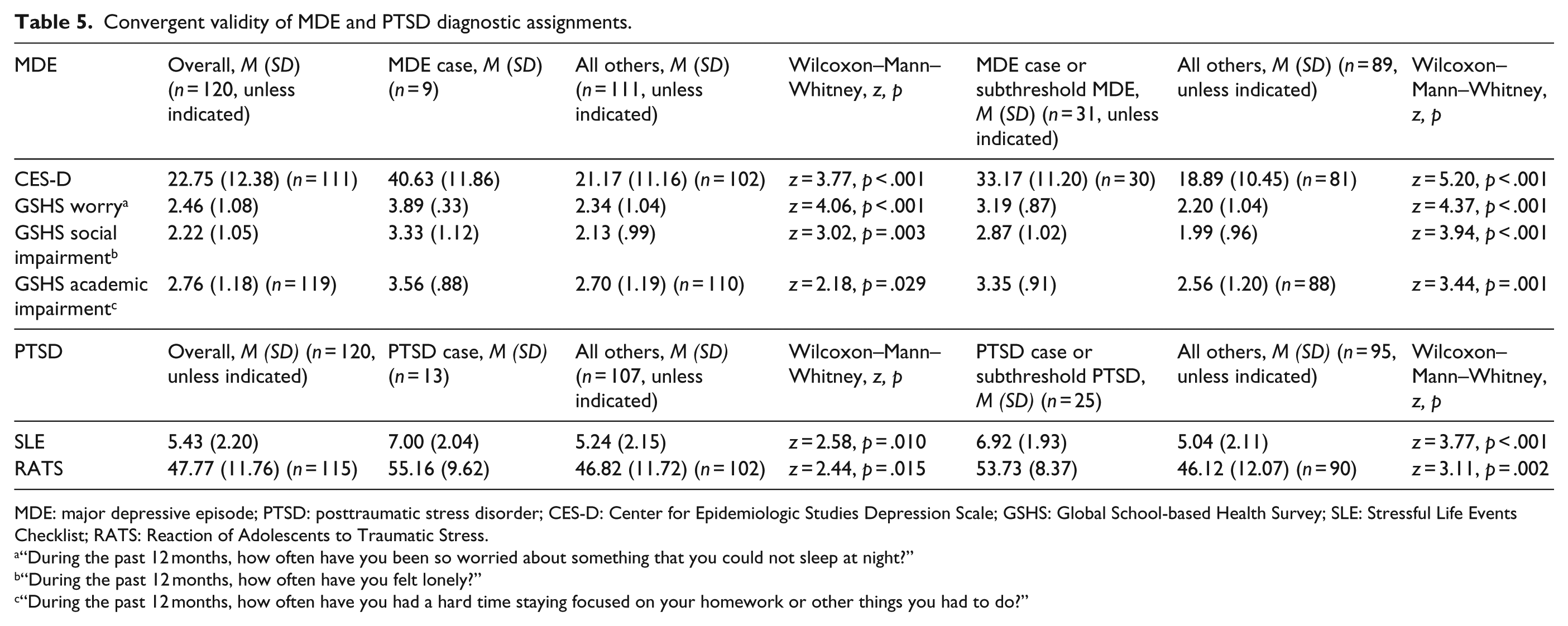
MDE: major depressive episode; PTSD: posttraumatic stress disorder; CES-D: Center for Epidemiologic Studies Depression Scale; GSHS: Global School-based Health Survey; SLE: Stressful Life Events Checklist; RATS: Reaction of Adolescents to Traumatic Stress.
“During the past 12 months, how often have you been so worried about something that you could not sleep at night?”
“During the past 12 months, how often have you felt lonely?”
“During the past 12 months, how often have you had a hard time staying focused on your homework or other things you had to do?”
Utilization of health care across groups identified by mental health needs
Among participants with a diagnosis of subthreshold or full-syndrome MDE and/or PTSD, 88.6% (n = 39) had not accessed health care for any mental health problem in the past 12 months; 43.2% (n = 19) had not accessed health care for any mental or other health problem during the same time period (Figure 1), and 36.4% (n = 16) had not accessed mental health care, other health care or folk sector care over the same one-year period. Health service utilization patterns were similar among participants with full-syndrome MDE or PTSD (no mental health utilization: 94.1%, n = 16; no utilization for any health problem: 41.2%, n = 7), MDE cases (no mental health utilization: 88.9%, n = 8; no utilization for any health problem: 33.3%, n = 3), PTSD cases (no mental health utilization: 100.0%, n = 13; no utilization for any health problem: 46.2%, n = 6), or not meeting at least subthreshold criteria (no mental health utilization: 86.8%, n = 66; no utilization for any health problem: 46.1%, n = 35) over the same one-year period.
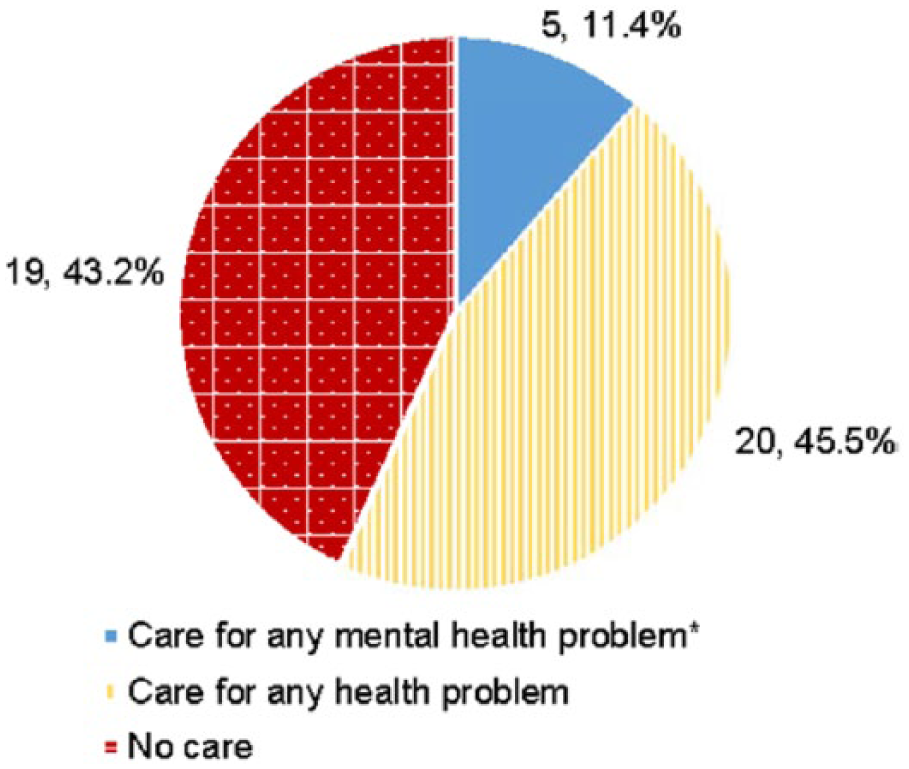
Health system–based care use in past year among participants with case or subthreshold MDE and/or PTSD, n = 44.
Discussion
In this community-based sample of secondary school youth in Haiti’s Central Plateau, the point-prevalence estimates of MDE and PTSD were 7.5% and 10.8%, respectively, with 14.2% affected by one or both of these disorders. Although the point prevalence of MDE in our sample was just slightly higher than the 5.3% 12-month prevalence of MDE in a community-based sample among 18- to 34-year-old adults in developing countries (Kessler et al., 2010), the prevalence of PTSD was substantially higher than the 0.7%–0.8% prevalence of PTSD reported among adults in LMICs (Karam et al., 2014). Furthermore, over one-third of our sample had at least subthreshold MDE and/or PTSD and, therefore, demonstrated clinically significant mental health treatment need. Diagnostic assignments based on the modified, abridged version of the SCID showed good convergent validity in comparisons based on several measures of symptomatology, including depression and PTSD screening tools, and an assessment of stressful events/traumatic exposures.
We also found striking evidence of a large mental health treatment gap. Across diagnostic classifications, nearly 90% of the participants in need of mental health treatment had not utilized services in the past year for the mental health problems we describe here. The magnitude of unmet need for Haitian youth identified in this study appears to be comparatively large (cf. Demyttenaere et al., 2004; Wang et al., 2007). This is unlikely to be attributable to lack of available mental health services since the participating schools were located in communities with ZL health centers offering mental health care. Nevertheless, participants endorsed difficulties with transportation as well as payment for care and medicine. Future exploration of these difficulties is warranted. Participant reports align with research indicating that accessibility of care is a key determinant of youth utilization (Ambresin, Bennett, Patton, Sanci, & Sawyer, 2013; World Psychiatric Association, World Health Organization, and International Association for Child and Adolescent Psychiatry and Allied Professions, 2005). Attitudes about mental health treatment among Haitian youth may be important to explore, given research suggesting that adults in the Central Plateau prefer nonhealth system–based care for mental disorders (Wagenaar et al., 2013). However, our data did not support that a substantial percentage of individuals with mental health needs who had not accessed mental health care through the health sector was accessing it through the folk sector instead.
Nearly half of the participants with full or subthreshold MDE or PTSD who had not utilized health services for a mental health problem had accessed general health care over the same one-year period. Like other rural Haitians (Keys, Kaiser, Kohrt, Khoury, & Brewster, 2012), our participants may be presenting for general health services with somatic problems that could represent idioms of emotional distress. Hence, incorporation of screening and treatment for mental disorders into primary health care through collaborative care programs guided by the Mental Health Gap Action Programme may improve case-finding and utilization of mental health care (Sharpe & Naylor, 2016; Wang et al., 2007; WHO, 2008).
There are a number of limitations of this study. School-based assessment in Central Haiti excludes youth who do not attend school or reside elsewhere in Haiti and limits the generalizability of our findings. Our study sample of transitional age youth within a narrow age range, moreover, does not encompass younger adolescents who may encounter different mental health barriers and needs. Nonetheless, there is growing recognition of a need to focus on early identification of mental health problems and effective interventions for youth who are making the developmental transition to greater independence and adulthood (Patton et al., 2016; Wilens & Rosenbaum, 2013). Although a SCID interview is commonly considered to be a gold standard for research diagnostic assessment, there were limitations to its implementation in this setting. Our study diagnostic assignments could have resulted in misclassification due to the use of SCID-based interviews in a setting for which it was not developed. Moreover, our use of an abridged interview for MDE meant that we were unable to discern the impact of medical illness, bereavement, food insecurity, and poverty on symptoms. Finally, because SCID content aligns with nosologic constructs developed outside of Haiti, it may not have captured clinically significant psychopathology that is expressed or manifested differently in the Haitian cultural context (Farmer, 1992; Keys et al., 2012; WHO, 2010). However, other qualitative research has demonstrated evidence of overlap between symptoms of MDE and PTSD experienced in Haiti and corresponding diagnostic constructs measured by the SCID (Bolton, Surkan, Gray, & Desmousseaux, 2012; Rahill, Joshi, Lescano, & Holbert, 2015; Rasmussen et al., 2015). Our approach integrating interviewer clinical judgment – based on local diagnostic experience – into our procedure for study diagnostic assignment was intended to identify locally salient presentations of MDE and PTSD (cf. Bhui et al., 2003). Similarly, we included subthreshold variants of MDE and PTSD in our analyses so as to encompass a broader range of psychopathology than is reflected in SCID-generated full-syndrome diagnoses. Our finding that groups defined by a study diagnostic assignment of MDE, PTSD, and subthreshold variants had greater levels of psychopathology as measured by standardized self-report assessments supports the validity of these assignments. Finally, our cross-sectional study design does not illuminate possible temporal trends in prevalence, either relative to the 2010 earthquake or many chronic social adversities confronting Haitian youth.
Notwithstanding these limitations, our finding of prevalent MDE, PTSD, and clinically significant psychopathology in our study population warrants concern and action. The remediation of unmet burden of mental disease arguably requires broad intervention beyond the clinical domain given the myriad impacts of poverty on health (e.g. Farmer, 1992). Like Haitian youth, many youth residing in LMICs face harsh social vulnerabilities that increase risk for poor mental health (Lund et al., 2010; Patel et al., 2008), such as absence of caregivers, poor physical health and nutrition, and low levels of education (Kieling et al., 2011; Smith Fawzi et al., 2012; Walker et al., 2007). Nonetheless, study findings underscore the importance of ensuring access to mental health services for youth in Haiti, and by extension, in other LMICs.
Conclusion
We observed a high prevalence of PTSD and substantial prevalence of MDE in this sample of secondary school youth in rural Haiti. Moreover, mental health care utilization was low among youth with clinically significant levels of MDE or PTSD symptomatology, suggesting a large mental health treatment gap for this population. This underscores the need to reduce barriers to help-seeking and increase human resources to provide mental health treatment for youth in Haiti and similar resource-limited settings.
Footnotes
Acknowledgements
We are grateful to the leadership of Zanmi Lasante as well as at the four schools who so generously accommodated the planning and implementation of the mental health training and its accompanying school-based pilot study. We thank Kate Boyd, Shin Daimyo, Georges Alexis, Elysee Noesil, Ernst Origene, Handy Petit-Homme and other colleagues at Partners In Health and Zanmi Lasante, as well as Claire Pernar and Megan Benson Stack at Harvard Medical School for their support of the planning, management and implementation of the study and trainings. We thank Marie-Christine Ouellet, PhD, and her team, École de psychologie, Université Laval, Québec, Canada, for providing the French translation of the SCID. We express here our profound gratitude to the student study participants for their time and generous feedback and from whom we learned so much.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by National Institute of Mental Health of the National Institutes of Health under award number R21MH093298 (Co-PIs, Becker and Eustache). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.