
Abstract
Background:
Social network size and strength is an important determinant of overall health.
Aims:
This study describes the extent and strength of the social network among a sample of individuals with serious mental illness (SMI) and explores the relationship between an individual’s social network and their experience of internal stigma and recovery attitudes.
Methods:
Over a 2-year period, consecutive new patients with SMI attending two community mental health clinics were recruited and interviewed using a comprehensive battery of assessments including assessment of internalized stigma, recovery attitudes and symptom severity.
Results:
Among the 271 patients interviewed, social network size was small across all diagnostic categories. In adjusted results, the number of friends and support from relatives and friends was significantly related to the personal confidence and hope recovery attitude (p < .05). The number of relatives and friends and support from relatives was significantly related to internalized stigma (p < .05). Frequency of contact with relatives or friends was not related to either recovery factors or internalized stigma.
Conclusion:
There is a significant positive relationship between the size and perceived strength of an individual’s social network and internalized stigma and some recovery attitudes. Clinical programs that address any of these factors could potentially improve outcomes for this population.
Introduction
Social networks and social supports reflect the objective and subjective experiences of a person’s social interactions. A strong, supportive social network has repeatedly been shown to be an important determinant in the overall health and well-being of an individual (Berkman, 1995; Brugha, 2010; Cobb, 1976). Mortality rates from myocardial infarctions (Ruberman, Weinblatt, Goldberg, & Chaudhary, 1984) and smoking cessation rates (Mermelstein, Cohen, Lichtenstein, Baer, & Kamarck, 1986) have both been linked to the presence, strength or type of social supports a person has and even susceptibility to the common cold has been linked to social relationships(Cohen, 2001). Additionally, how an individual adapts to, and copes with, difficult situations has been strongly linked to their social network (Solomon & Draine, 1995) and strong social networks can be protective against the negative effects of stress and trauma (Brugha, 2010).
For those who have a serious mental illness (SMI) social supports are particularly important although their social networks tend to be smaller than others (Goldberg, Rollins, & Lehman, 2003). Much past research has explored the association of social networks and social support in individuals with SMI, with their functioning, symptoms and service use (Albert, Becker, McCrone, & Thornicroft, 1998; Brugha, Wing, Brewin, MacCarthy, & Lesage, 1993; Erickson, Beiser, Iacono, Fleming, & Lin, 1989; Evert, Harvey, Trauer, & Herrman, 2003; Hamilton, Ponzoha, Cutler, & Weigel, 1989; Salokangas, 1997; Siegrist, Millier, Amri, Aballéa, & Toumi, 2015; Thorup, Petersen, Jeppesen, & Nordentoft, 2006). It has been repeatedly found that among those with schizophrenia, the presence of negative symptoms predicts a lower frequency of social contact (Hamilton et al., 1989; Siegrist et al., 2015) and a small social network is associated with more frequent hospitalizations (Albert et al., 1998). In contrast, a supportive social network is positively associated with functional ability (Salokangas, 1997). The presence of non-family social resources has been found to be positively related to overall outcome in those with first episode schizophrenia (Erickson et al., 1989) while small network size predicts severity of negative symptoms in this same group (Thorup et al., 2006). Among individuals with psychotic illnesses, a strong correlation has been reported between social networks and functioning in the area of self-care and employment (Evert et al., 2003). Brugha et al. (1993) found that outcomes are poorer for those with severe mental illness when their social networks are reduced. Indeed, the combination of a reduced social network and few social supports has been reported to lead to higher rates of hospitalization in this population (Brugha et al., 1993). Links between social networks, stigma and recovery have also been found in those with SMI (Byrne, 2000; Leamy, Bird, Le Boutillier, Williams, & Slade, 2011; Perry, 2011; Soundy et al., 2015). Studies have found that being labeled with a SMI tends to strengthen core social networks, but decreases social connections with acquaintances and strangers (Perry, 2011) and stigma can lead to secrecy which leads to a narrower and smaller social network (Byrne, 2000). In their review of factors promoting recovery in individuals with schizophrenia, Soundy et al. (2015) found that close social ties to family and friends are important for the recovery process. Similarly, Leamy et al. (2011) identified ‘connectedness’ as one of the important processes involved in recovery among those with mental health conditions.
However, past research has rarely examined the association of social network and social support with the individuals’ attitudes toward their illness, including attitudes toward recovery from mental illness and the strength of their adoption of societal beliefs about mental illness, and internalized stigma. Negative attitudes toward illness and perceived stigma may influence the individual’s interactions with their social network. In turn, social exclusion as a result of mental illness may influence the individual’s attitudes toward their illness, hope for recovery and internalized stigma. In this article, we describe the social networks of a sample of patients with serious mental disorders in two urban community psychiatry programs and explore the association of social network and social support with recovery attitudes and stigma in this group.
Methods
The sample and the design of the study has been previously described (Mojtabai et al., 2014; Nugent et al., 2015). Briefly, consecutive admissions between August 2008 and December 2012 to two urban outpatient psychiatric clinics in Baltimore, Maryland, were recruited as part of a longitudinal study on recovery in the SMI population. Adults with the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) clinical diagnoses of schizophrenia, schizoaffective disorder, schizophreniform disorder, bipolar disorder (type I or II), delusional disorder, psychotic disorder not otherwise specified (NOS), or major depressive disorder (severe with psychotic features) were included.
We aimed to recruit similar numbers of participants with the diagnoses of schizophrenia spectrum disorders and bipolar disorder. The bipolar stratum was filled in July 2011, after which recruitment effort focused on patients with schizophrenia spectrum disorders. A total of 874 clinic patients were eligible for the study of whom 271 (31%) agreed to participate and completed the assessment. In all, 30% did not want to participate and the remainder were either unable to be scheduled or not contactable. All participants provided written consent. The study was approved by the Institutional Review Board of the Johns Hopkins Bloomberg School of Public Health.
Social networks and relationships were assessed using an interview instrument previously used in the Epidemiologic Catchment Area (ECA) study in Baltimore (Maulik, Eaton, & Bradshaw, 2009) which inquired about the number of relatives and the number of friends that participants had kept in touch with, and the frequency of contact with friends or relatives, including physical meetings, e-mails, postal mail or phone in the past 6 months.
Participants were also asked a series of questions about the perceived quality of support from relatives, friend and spouse (or partner). Examples of the questions related to a spouse or partner were ‘How much does your (husband/wife/partner) really care about you?’ ‘How much can you rely on your (husband/wife/partner) for help if you have a serious problem?’ ‘How much can you relax and be yourself around your (husband/ wife/partner)?’ ‘How often does your (husband/wife/partner) make too many demands on you?’ ‘How often does (he/she) let you down when you are counting on (him/her)?’ ‘How often does (he/she) get on your nerves?’ Six questions were asked separately regarding relatives, friends and spouse/partner. Questions for spouse/partner were asked only from participants who reported having a spouse or partner. All questions were asked in reference to the past 6 months. Answers were recorded on a four-point ordinal scale. The responses were recoded so that a higher score indicates a more supportive relationship. A summary score was computed by summing up the response scores for relatives, friends and spouse. Possible summary scores ranged from 6 to 24, with higher scores indicating better quality of perceived support. The Cronbach’s alpha for these ratings ranged from .83 for spouse/partner ratings to .71 for relatives’ ratings and .65 for friends’ ratings. Consistent with past research for analyses (Maulik et al., 2009), responses were dichotomized based on the median score.
Attitudes toward recovery from mental illness were recorded using three scales from the Recovery Assessment Scale (RAS) (Corrigan, Salzer, Ralph, Sangster, & Keck, 2004) that assessed personal confidence and hope (nine items), goal and success orientation (five items) and no domination by symptoms (three items). Participants responded to statements such as ‘I believe I can meet my current personal goals’ using a 5-point ordinal scale (from strongly agree to strongly disagree), with higher scores reflecting greater recovery orientation. Summary scale scores were computed by summing the item scores on each scale. The RAS has shown positive correlations with measures of hope, self-esteem and quality of life, and it is negatively associated with psychiatric symptoms (Corrigan et al., 2004; McNaught, Caputi, Oades, & Deane, 2007; Salzer & Brusilovskiy, 2014).
Internalized mental illness stigma was measured by a scale consisting of items drawn from the Internalized Stigma of Mental Illness (ISMI) Scale (Ritsher, Otilingam, & Grajales, 2003). These items measured the person’s negative views of mental illness and of themselves as a result of having a mental illness and consisted of statements such as ‘I feel out of place in the world because I have a mental illness’. Six items from the ISMI Alienation subscale utilized self-specific phrasing (i.e. I am embarrassed or ashamed that I have a mental illness). Three items from the ISMI Stereotype Endorsement and Stigma Resistance subscales utilized general phrasing (i.e. mentally ill people tend to be violent). Two additional items from the Stereotype Endorsement subscale were modified from self-specific to general phrasing, and one item was changed ‘cannot’ to ‘can’ to make it a positively worded item (see Appendix 1). Participants indicated their endorsement of each item on an ordinal scale (strongly disagree, disagree, agree, strongly agree). The responses were scored on a scale from 1 to 4 and were averaged over items so that a higher score would indicate a greater level of internalized stigma. The Cronbach’s alpha for the 12-item scale in this sample was .81.
Psychiatric diagnoses for the clinic sample were extracted from medical records and were formulated by experience attending psychiatrists following a 90-minute clinical evaluation. Symptom severity was measured by the Positive and Negative Syndrome Scale (PANSS) which measures both positive and negative symptoms of schizophrenia as well as general psychopathology (Kay, Fiszbein, & Opler, 1987). Sex, age, race/ethnicity were also recorded and included in the adjusted analyses.
Analyses were conducted in two stages. First, the extent and quality of social network was assessed in the full sample and separately in each diagnostic group. Second, the associations of the extent and perceived quality of social networks with summary scores of recovery attitude measures and internalized stigma were assessed using linear regression models. Each social network variable was entered into the model individually. Both unadjusted and adjusted regression analyses were conducted. Two sets of adjusted analyses were conducted. The first adjusted model included age, sex, race/ethnicity and clinical diagnosis. The second model added an adjustment for PANSS scores. The perceived quality of social support was dichotomized for these analyses based on the median score following a previous study using the social support scale (Maulik et al., 2009). All analyses were conducted using Stata 14.
Results
A majority of the 271 participants were females (53%) and non-Hispanic Black (54%) or non-Hispanic White (34%). The average age of the participants was 42 years (standard deviation = 11). Only 22% were married or lived with a partner. The most common clinical diagnoses were bipolar disorder spectrum disorders (n = 123, 45%) and schizophrenia spectrum disorders (n = 89, 33%). Major depression with psychotic features (n = 40, 15%) and psychotic disorder NOS (19, 7%) were less common; consequently, we consider these two diagnostic categories together as ‘other psychotic disorders’.
The social network characteristics and the perceived quality of social networks of the sample as a group and according to clinical diagnoses are presented in Table 1. Except for the frequency of meeting friends, which was lower in the psychotic disorder NOS group, there were no significant differences between diagnostic categories. Taken as a group 9.6% reported not having any friends and the median perceived social support score varied from 17 to 19 depending on the social group.
Social networks and perceived social support levels among individuals newly admitted patients in the community psychiatry programs.

df: degree of freedom.
Possible scores range from 6 to 24, with higher scores indicating better quality of perceived support.
In unadjusted regression analyses, number of friends, perceived social support from friends and perceived social support from relatives were associated with the recovery attitude of personal confidence and hope (Table 2): the larger the number of friends and the greater the perceived social support, the greater the personal confidence and hope. These associations persisted when adjusted for age, sex, race/ethnicity and diagnosis (Table 2) but did not remain when PANSS scores were added to the model (Table 2).
Social network and perceived social support in relation to Personal Confidence and Hope Subscale summary score a on Recovery Assessment Scale.

PANSS: Positive and Negative Symptoms Scale; SE: standard error; df: degree of freedom.
Personal Confidence and Hope subscale summary score on RAS is based on the sum of ratings on nine items and ranges from 9 to 45.
Each social network variable was entered into a separate model adjusting for demographic variables and diagnosis. The regression coefficients for demographic variables and diagnosis reported in this table are from the multivariable model for number of relatives. The detailed results for the other models are available from the first author.
The number of friends and perceived social support from friends and relatives was also associated with the goal and success orientation recovery attitude (Table 3): the larger the number of friends and the greater the perceived social support, the more strongly the participants endorsed a goal and success orientation. All these associations, except for the association of perceived social support from relatives, persisted when adjusted for demographics and diagnosis (Table 3). However, when the PANSS domain scores were adjusted for, only the association with perceived social support from friends remained significant (Table 3).
Social network and perceived social support in relation to Goal Orientation subscale summary score a on Recovery Assessment Scale.
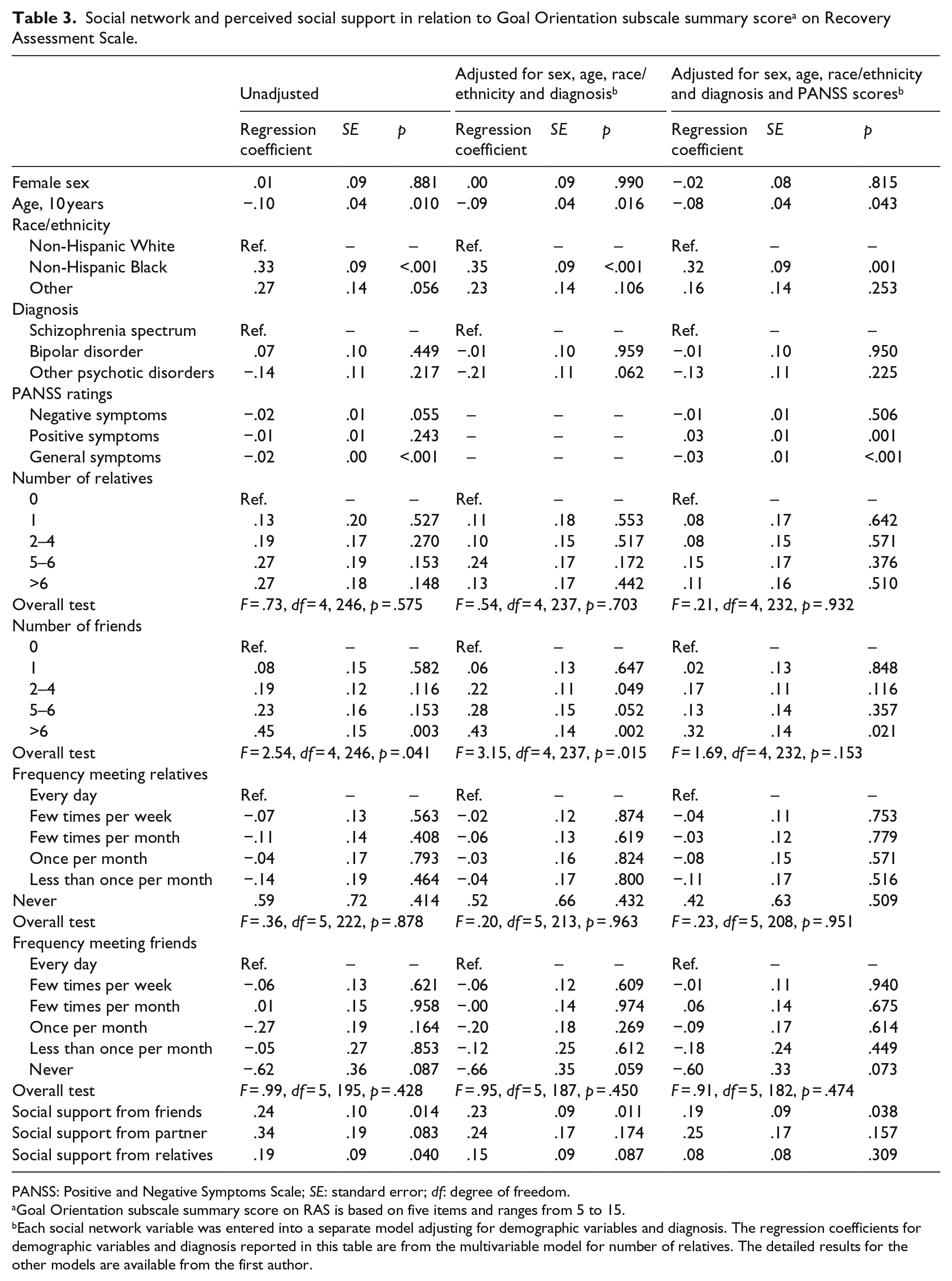
PANSS: Positive and Negative Symptoms Scale; SE: standard error; df: degree of freedom.
Goal Orientation subscale summary score on RAS is based on five items and ranges from 5 to 15.
Each social network variable was entered into a separate model adjusting for demographic variables and diagnosis. The regression coefficients for demographic variables and diagnosis reported in this table are from the multivariable model for number of relatives. The detailed results for the other models are available from the first author.
The no symptom domination orientation was only related to perceived social support from relatives: the greater such perceived support the stronger the endorsement of this orientation (Table 4). The association remained statistically significant in analyses adjusted for demographics and diagnosis (Table 4), as well as PANSS domain scores (Table 4).
Social network and perceived social support in relation to No Symptom Domination subscale summary score a on Recovery Assessment Scale.

PANSS: Positive and Negative Symptoms Scale; SE: standard error; df: degree of freedom.
No Symptom Domination subscale score on RAS is based on three items and ranges from 3 to15.
Each social network variable was entered into a separate model adjusting for demographic variables and diagnosis. The regression coefficients for demographic variables and diagnosis reported in this table are from the multivariable model for number of relatives. The detailed results for the other models are available from the first author.
In unadjusted analyses, the number of friends and perceived social support from relatives were significantly associated with internalized mental illness stigma: the larger the number of friends and the greater the support, the lower the stigma (Table 5). The number of relatives was associated with internalized stigma at a trend level (p = .082). The association with the number of relatives became statistically significant at p<.05 in the analyses adjusted for demographics and diagnosis and the associations with number of friends and perceived support from relatives remained statistically significant (Table 5). These associations continued to remain significant after the PANSS score was also adjusted for (Table 5).
Social network and perceived social support in relation to internalized stigma summary score. a

PANSS: Positive and Negative Symptoms Scale; SE: standard error; df: degree of freedom.
Internalized stigma summary score is based on 12 items and ranges from 12 to 48.
Each social network variable was entered into a separate model adjusting for demographic variables and diagnosis. The regression coefficients for demographic variables and diagnosis reported in this table are from the multivariable model for number of relatives. The detailed results for the other models are available from the first author.
Discussion
The results of this study provide insights on the size and perceived quality of social support among those with SMI. Additionally, they demonstrate the potential connections between an individual’s social network and support and their perception of, or attitude to, their own recovery and their experience of stigma.
As previously found, the social network size of individuals with SMI is small especially when compared to the general population (Goldberg et al., 2003). Overall, 22% had none or only one relative and almost 40% had none or only one friend. Across all diagnostic categories between 15% and 18% had regular contact with six or more relatives and 5% and 17% had regular contact with six or more friends. In comparison, previously published data from the Baltimore ECA study found that only 3%−5% had none or one relative and only 13%−14% had none or one friend (Maulik et al., 2009). Additionally, over half of the general population participants in the ECA had regular contact with more than six of their relatives and about one-third had contact with more than six friends within the previous 6 months (Maulik et al., 2009).
Participants also tended to report a lower level of perceived social support compared to the general population sample (Maulik et al., 2009). For example, approximately, half of a general population sample from Baltimore scored 20 or higher on the scale for social support from friends (potential range was 6–24), whereas, about 25% of the clinic sample scored in that range.
These comparisons with the general population sample should, however, be considered with caution because the samples were collected at different time periods and had somewhat different socio-demographic profiles (Maulik et al., 2009). Nonetheless, the findings still highlight the significant lack of perceived social support and smaller network size experienced by individuals with SMI.
In their review of common explanations for the reduced social networks among those with schizophrenia, Eklund and Hansson (2007) noted various factors including impaired development of social skills, presence of positive and negative symptoms, lack of opportunity to socialize, limited resources and external stigma. These authors sought to identify socio-demographic, clinical and health-related factors that were important for the social interactions of those with SMI and concluded that factors such as self-esteem, quality of life and living with others played a role in social interactions which are probably bi-directional in nature. Likewise, in this study, we found a relationship between an individuals’ recovery attitude, their level of internal stigma and the size and strength of their social network and perceived support. Subjects who positively endorsed statements such as ‘I have a purpose in life’, ‘I have goals in my life that I want to achieve’ and ‘I am hopeful about my future’ were more likely to report feeling supported and connected with others and they were more likely to negatively endorse statements such as ‘having a mental illness has spoiled my life’ and ‘I am embarrassed or ashamed that I have mental illness’. It is possible that this relationship is somewhat dynamic such that a lower level of internal stigma would facilitate a more extensive social network which in turn would reinforce the sense of hope and optimism which is part of perceived recovery. It is noteworthy that, in this study, the frequency of contact with an individual’s social network was not as important to stigma or recovery as either the extent or perceived strength of their social support.
The severity of symptoms, as assessed by the PANSS, had little impact on the findings. This was particularly the case for internalized stigma where regardless of symptom severity those who felt supported by relatives and who had larger numbers of friends and family experienced less internalized stigma. Likewise with two of the three recovery factors the link between perceived social support from either family (no symptom domination) or friends (goal and success orientation) was not affected by how severe an individual’s symptoms were.
Previous studies have linked recovery among those with SMI to the individual’s social network (Leamy et al., 2011; Schon, Denhov, & Topor, 2009; Soundy et al., 2015). Others have explored the role that internal stigma plays in this relationship (Chronister & Liao, 2013; Perlick et al., 2001). Our results raise the possibility that the relationship between the strength and size of an individual’s support network and their recovery could be mediated by their attitude toward recovery, as assessed by the RAS, and their level of internalized stigma. Additionally, the severity of their symptoms does not appear to contribute significantly to this association.
Targeting internal stigma, promoting recovery attitudes and encouraging development of social networks are still not widely adopted as part of the treatment plan for individuals with SMI. Rusch, Angermeyer, and Corrigan (2005) proposed strategies to reduce self-stigma and others have reported on the results of interventions they implemented to address stigma and promote recovery in a clinic setting (Corrigan & Rao, 2012; Sibitz, Provaznikova, Lipp, Lakeman, & Amering, 2013). Our results would suggest that the implementation of these types of interventions could positively affect the social network and perceived support of those with SMI. Additionally, having providers directly promote and facilitate an individual’s engagement within their community could potentially expand their social network. Individual therapy focused on developing social skills, referral to community organizations such as clubhouses or drop-in centers could all help achieve this goal.
The strength of this study lies in its comprehensive assessments of recovery attitudes, social network and symptoms in participants recruited from two inner city community psychiatry clinics. The majority of participants were disabled, had medical problems in addition to mental health problems (Mojtabai et al., 2014), were single and from racial/ethnic minority groups. As such, this patient population represents a highly disadvantaged group with many unmet needs for formal and informal care. Support from family and friends is especially important for these individuals who may need help with accessing the needed social resources and services and management of their daily lives. The results of this study further suggest that the extent and quality of their social network is also related to how they view their illness and the process of recovery from it.
The study has some limitations. The data are cross-sectional in nature, preventing causal inference. There is also some overlap between the constructs of internal stigma and an individual’s recovery attitudes or perception of recovery and this should be considered when interpreting our results. Furthermore, assessment of social network size and strength is based on self-report which is open to social desirability and recall bias. Additionally, the comparison group results were obtained at a different time and among a slightly different socio-economic group.
Despite these limitations, the study’s findings do highlight the need to move beyond symptom control when working with the SMI population. While we cannot conclude that recovery attitudes and internal stigma constructs are independent of each other there does appear to be a dynamic relationship between them, and an individual’s social network and perceived support. Addressing stigma, promoting hope and optimism and encouraging engagement with others as part of the overall management of individuals with SMI may all have the potential to positively impact their experience of recovery. Services addressing these aspects of a patient’s care need to be incorporated into the treatment setting.
Footnotes
Appendix 1
Items assessing internalized mental illness stigma.

| 1 | I feel out of place in the world because I have a mental illness |
| 2 | Having a mental illness has spoiled my life |
| 3 | People without mental illness could not possibly understand me |
| 4 | I am embarrassed or ashamed that I have a mental illness |
| 5 | I am disappointed in myself for having a mental illness |
| 6 | I feel inferior to others who don’t have a mental illness |
| 7 | Mentally ill people tend to be violent |
| 8 | Mentally ill people shouldn’t get married |
| 9 a | People with mental illness can live a good, rewarding life |
| 10 a | It is possible to identify a person with mental illness by the way they look |
| 11 a | People with mental illness need others to make decisions for them |
| 12 | People with mental illness make important contributions to society |
Wording changed slightly from the Internalized Scale of Mental Illness (Ritsher et al. 2003).
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Center for Mental Health Initiatives at the Department of Mental Health, The Johns Hopkins Bloomberg School of Public Health.