
Abstract
Background and aims:
Previous research on supported housing for people with serious mental illness focuses primarily on tenant/client experiences. The aim of this article is to present families’ perspectives on the role of supported housing in recovery, utilizing the CHIME framework of personal recovery.
Method:
Qualitative interviews were conducted with 14 families of individuals with serious mental illness living in supported housing. Participants were across five supported housing sites in four Canadian provinces.
Results:
Families credited supported housing with helping tenants redefine a positive sense of identity, re-establish social relationships and regain control over their lives. Families were less confident about supported housing facilitating future employment or ‘full’ recovery, focusing on stability rather than continual improvement.
Conclusion:
This is one of the first studies to report family perspectives on the role of supported housing in their loved one’s recovery processes – both strengths and weaknesses.
Introduction
The concept of mental health recovery (hereafter, ‘recovery’) emerged in the 1980s (Deegan, 1988) and has since become an international focus for mental health policy and service delivery. Recovery is defined as a ‘journey of healing and transformation enabling a person with a mental health problem to live a meaningful life in a chosen community while striving to achieve [their] full potential’ (Substance Abuse and Mental Health Services Administration (SAMHSA), 2004). Leamy, Bird, Le Boutillier, Williams, and Slade (2011) conducted a systematic review of the concept of ‘personal recovery’ and developed the CHIME conceptual framework in which five recovery processes occur: ‘Connectedness’, ‘Hope and optimism about the future’, ‘Identity’, ‘Meaning in life’ and ‘Empowerment’ (Table 1). Within the CHIME framework, recovery is understood as an active, individual and non-linear process (Leamy et al., 2011).
Sub-components of the CHIME recovery framework.
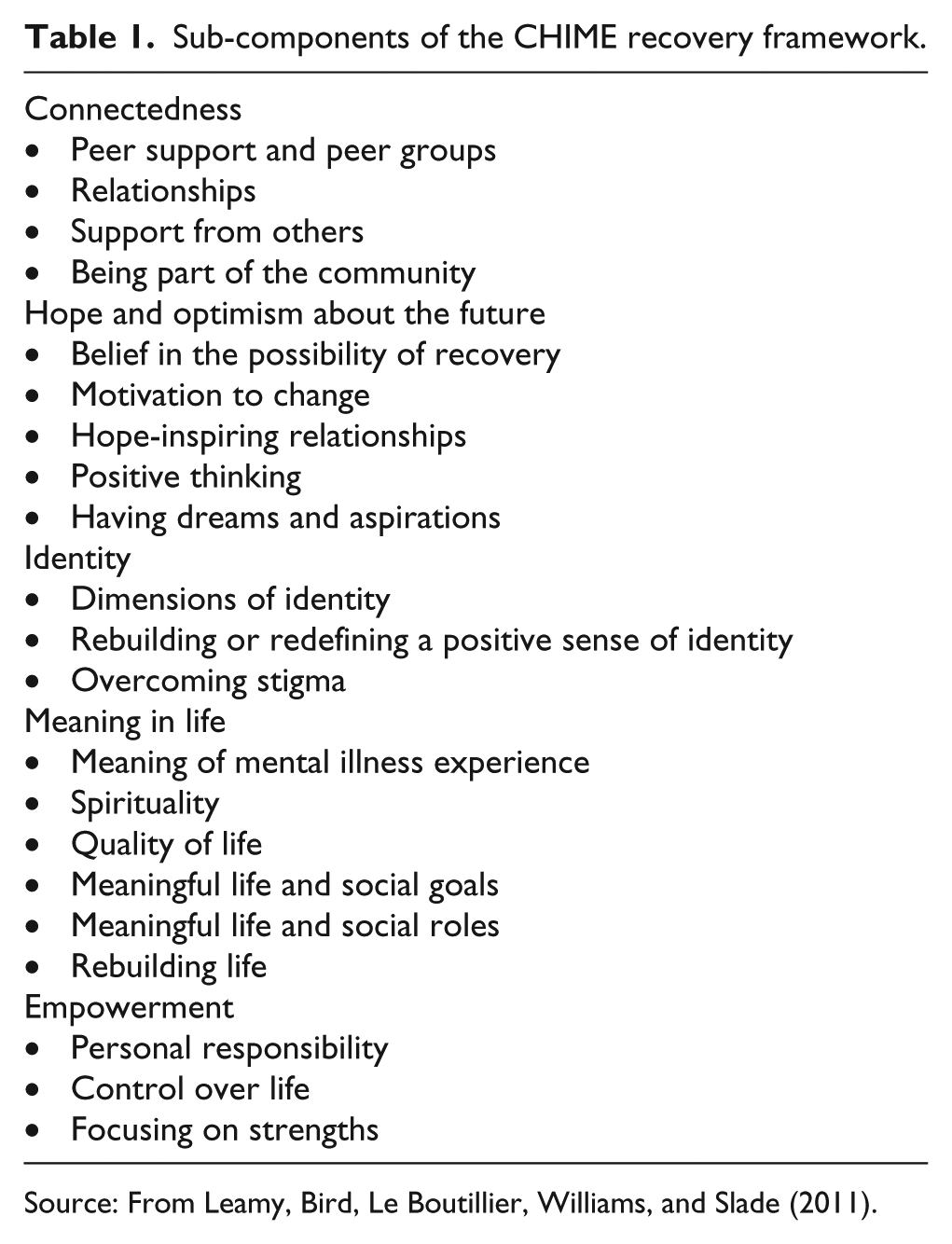
Source: From Leamy, Bird, Le Boutillier, Williams, and Slade (2011).
Despite the robustness of CHIME framework (Bird et al., 2014), research using CHIME has focused on service user’s personal recovery journey (Jacob, Munro, Taylor, & Griffiths, 2017). This is the first study to utilize CHIME to understand recovery processes from the perspectives of families of those with serious mental illness (SMI) living in supported housing.
Supported housing is an evidence-based, recovery-oriented housing for individuals with SMI (Rog, 2004). In contrast to highly structured group living and boarding home models managed by non-professionals and often for profit, supported housing provides full tenancy rights, including protection against eviction (PIAT, Sabetti, & Padgett, 2018a). Supported housing can take the form of independent units clustered in apartment buildings with programs and staff support or as ‘scattered-site’ units in regular apartments without designated programs and support as needed (PIAT, Sabetti, & Padgett, 2018b). While it is widely acknowledged that supported housing promotes tenant recovery (Hayes et al., 2018; Tsai, Bond, & Davis, 2010), to our knowledge, no studies have explored families’ views on the role of supported housing in recovery.
Families are key stakeholders in mental health care (Mehrotra, Nautiyal, & Raguram, 2018) consequently, much scholarly attention has been devoted to understanding and documenting the experiences of caregiving (Kumar, Suresha, Thirthalli, Arunachala, & Gangadhar, 2015; Ostman, Hansson, & Andersson, 2000) including caregiver burden and burnout (Poon, Harvey, Mackinnon, & Joubert, 2017; Susanti, Lovell, & Mairs, 2018). The negative impact of caregiving has been documented since the first waves of deinstitutionalization (Hayes, Hawthorne, Farhall, O’Hanlon, & Harvey, 2015; Schene, van Wijngaarden, & Koeter, 1998) when much of the costs and responsibilities of psychiatric care were deformalized (Talley, Fricchion, & Druss, 2014).
Beyond the context of caregiving, family perspectives on recovery have largely been ignored, despite family being recognized as an important ‘recovery domain’ (Choy-Brown, Padgett, Tran Smith, & Tiderington, 2016). Our study contributes to current knowledge by utilizing CHIME to map families’ views on personal recovery and to housing literature by exploring families’ perspectives on the connections between supported housing and recovery.
Methods
Sample and data collection
Family members were one of five participant groups (the other four were tenants, decision makers, housing staff and service providers) recruited as part of a pan-Canadian study on the move from custodial to supported housing in five project sites (Toronto, Montreal, Quebec City (two sites) and St. John’s). All tenants participating in the study (n = 24) were asked to recommend and contact a family member, inclusive of ‘chosen family’ (Muraco, 2006) to be part of the study. A total of 16 family members agreed to participate, while geographical distance or a lack of social ties precluded the remaining tenants from recruiting family.
Upon receiving ethics approval from the Research Ethics Board of the Douglas Hospital Research Ethics Board, and Health Research Ethics Board of Newfoundland and Labrador, 14 in-depth qualitative interviews were conducted between March and July 2015. The principal investigator and three research assistants trained in qualitative interviewing conducted each interview in person in a location chosen by the participant. Interview guides covered the following topics: tenant’s housing situation, the recovery orientation of services, choice and autonomy and community integration, stigma and discrimination.
Data analysis
All interviews were audio-recorded and transcribed verbatim. Transcripts were read several times and inductively coded in NVivo10 by two researchers working independently. Codes were based on the smallest meaningful entities as units of analysis (Chenail, 2012). All coded segments were compiled into a document; analytic summaries for each segment were written and then organized according to CHIME (Leamy et al., 2011). All researchers discussed analyzed data, and any interpretive ambiguities were resolved through consensus. Analytic rigor was insured by continuously revisiting transcripts to stay close to participants’ descriptions (Oliffe & Bottorff, 2007) and by triangulating the data according to multiple coders and setting (five socio-economically and geographically diverse housing sites).
Findings
Connectedness
Support from tenants
According to several family members (n = 6) support among tenants was central to creating a recovery-oriented ‘home environment’. Gino (Mario’s brother) and Amanda (Ian’s sister) explain that the opportunities to both provide and receive emotional support create a positive ambiance and make supported housing ideal for rebuilding one’s life. Amanda explains, ‘because there are other people that may be having the same [or similar] struggles as him […] they’re all kind of equal […] and they keep each other company’. Tenants also provide material support to one another, as Dorothée (Benoît’s mother) describes, ‘He goes to see the neighbor […] If they need him, they knock on his door, like he helped one of the neighbors put tires on his car [and] dug out his car last winter’.
Support from housing staff
Families appreciate the range and flexibility of support offered to tenants, including assistance with problem-solving and facilitating social engagement:
The staff [are] available if any real problems come up. [I]n Joseph’s case, they’re really friendly with him. Not so much helping him, but saying ‘hey come and help us garden, or we’re doing an art group, come and join us’. (Wanda, Joseph’s mother)
Several family members highlighted positive, interpersonal dynamics between tenants and housing staff, particularly those that struck a balance between providing necessary resources and encouraging autonomy. Joanne (Stéphane’s mother) describes multiple ways in which housing staff support her son, including spending quality time and referring to him as ‘family’. Alexandre (Julien’s father) similarly appreciates staff support, but stresses that it should be devoid of patronizing undertones and recognize what tenants can offer:
There is no need to […] force him like a baby to do this and that, it’s not his thing. Because he can teach them a lot of things, he has a black belt in Judo and is also a swimming teacher. So yes, they do their job, and he’s fine.
Relationships
Although many families (n = 9) view themselves as the primary source of support, they also describe shifting roles and a new emerging reciprocity between themselves and their family member. Families describe various ways in which tenants offer them support, often by spending time together or providing material assistance. Emily (Catherine’s mother) describes an increasing emotional connection with her daughter since her move into supported housing:
Every morning she calls me. We’re getting closer and closer because, well going back many years, I couldn’t put my arms around Catherine, she’d push me away. It was just terrible. There was absolutely no affection from her. [But now] it’s just the opposite, big kiss when she’s leaving, ‘I love you mom’ […] When she was at [previous housing], it was strictly every two weeks […] now, she comes by whenever.
Families report that living in supported housing increases tenants’ self-confidence, providing their loved ones with increased social, material and emotional resources to invest in (re)building relationships with their families. In other words, living in supported housing promotes changes in family–tenant relationships:
Since he is prouder of himself, he’s doing well; he comes to [and] is more willing to see us. He would be ready to receive us anytime […] This is his home, his bubble. He is very proud of where he is. (Nancy, Cyril’s sister) He is much more sociable, he communicates more with us. He goes to hockey and baseball with his father […] he participates in that and it interests him, [and] he calls us for recipes. He comes to eat here. (Lorraine, Marc’s mother)
Supported housing also facilitates social connectedness beyond family connections, providing opportunities for tenants to develop meaningful relationships with the broader community:
[Supported housing] is taking him out of his shell […] He’s more social, more active and he’s not just wrapped up in his own little world, especially with his mental illness […] all he would do is think and think, [but] now he’s so active, he’s so happy – it’s a total change in man. (Amanda, Ian’s sister)
Mary, Tony’s aunt, similarly reports that living in supported housing has facilitated both housing and community-based friendships:
He is more part of the community here […] because the community here is where he wants to be, where he can walk to church; he has friends in church […] The friends he has in this building are right next door and they drop in and then his other friend with a car comes and picks him up so yes, it is much better.
Hope and optimism
Belief in the possibility of recovery
Despite widespread agreement among family members that supported housing fosters their loved one’s recovery numerous families (n = 9) expressed little hope and optimism about the possibility of ‘full’ recovery. As Lorraine posits, ‘you have to be reasonable, you have to understand he’s like that, he’ll never heal. He’s a schizo, that’s the baseline. But he is functional, and he is tidy; for me, that’s what’s important’. Similarly, Gino (Mario’s brother) states,
He takes five steps forward and one back sometimes. I know it from him and from other mental illness people, from what I see they always try to get to that top where they think they’re going to fight it and everything is going to be over. It doesn’t happen.
Several participants stressed the challenges posed by addictions and continuing symptoms, which shape the limits and non-linearity of recovery in the context of supported housing. For instance, Jonathan (Beatrice’s friend) notes the sudden and unexpected nature of mental health crises, while Christopher (Danielle’s father) highlights the hurdles posed by addiction:
I’m afraid she’s falling back into the same problems [as] before […] because I don’t trust that she’s recovered, that it’s all in the past. I do not have the confidence yet. Maybe in the future, but it takes time. [Her] challenge is to pay attention to alcohol, friends, and drugs.
However, a few of participants (n = 3) did feel optimistic that recovery was possible; Wanda, for one, asserts,
I think his future is going to be rich […] I think with Joseph the only way to go is up. When he’s ready to do whatever it is he wants to do whenever he wants to do, he’s going to do it.
Having dreams and aspirations
Families also expressed skepticism about their loved ones’ ambitions and aspirations while living in supported housing, particularly concerning employment. As Olivia (Pierre’s mother) asserts, ‘A normal job is impossible, he would be incapable. He does not have health, he is not able, that’s for sure’. Gino also feels that ‘as far as looking for a job, it’s in his head but it’s not in his heart to do it because […] it’s done without the shovel in his hand’. Although Lorraine feels supported housing has facilitated her son’s recovery on multiple fronts, its beneficial impacts do not extend to employment or education:
He cannot work […] he is not able. He has tried several times, he has social workers who found him small jobs and it never worked out. Marc has problems focusing on things. So it’s useless to think about that, whether it’s in an apartment or a room, it changes absolutely nothing.
Despite recognizing supported housing’s critical role in recovery, several family members (n = 3) saw it as the ‘best case’ scenario, rather than a stepping stone to truly independent living:
This is as close to an ideal living situation as Beatrice is ever going to find […] she would love to have a house and garden of her own […] But I would be very worried if she had that, because she wouldn’t be able to keep it […] this is what’s possible for Beatrice. (Jonathan) Let it go on like this. I do not see anything better than this. If [housing situation] stays as stable as it is now, I’ll be satisfied [….] Where he is right now is good. (Lorraine)
Identity
Rebuilding/redefining a positive sense of identity
Families view supported housing as a concrete means to build a more ‘normal’ sense of self beyond the confines of an illness-based identity. Family participants (n = 5) describe the value being ‘like everyone else’ held for their loved one:
Living in his own apartment has made things so much better [….] he feels like a full citizen again [….] he is prouder, happier […] he was jumping for joy in the apartment. It had been years since I had seen him do that. (Lorraine) They are autonomous, always within their limits, but he sees himself more like everyone else. [Previous housing] was a place where the people have a mental health disability. While here, in an autonomous apartment, it’s not written on their face, do you see? […] being in an apartment like anyone else here, it’s a big plus. (Dorothée)
In addition to promoting a sense of normality, the stability of supported housing provides the foundation for rebuilding a positive sense of identity:
She could not talk about herself in any depths without crying constantly. That’s depression […] It’s been a long time since we’ve had one of those conversations [because] the need for [housing] is much less pressing. (Jonathan)
Participants also attributed identity (r)evolutions to the exercise of personal responsibility and subsequent development of autonomy in supported housing. For instance, Mary contends, ‘it makes such a difference to your whole persona, your whole concept of self to be in a place where you’re independent or can become independent’. The connections between a positive sense of identity, personal responsibility and overall autonomy were frequently made:
His home is totally clean, he is proud to say that he can do his grocery shopping, the budget, a real daily life, Cyril living without his illness […] It’s a huge source of pride, to live as an individual, not as a person with something. (Johanne, Cyril’s sister) The difference between supervised and autonomous housing is: ‘I am capable, all alone […] I am worth something’. […] It is not about forgetting the schizophrenia that he has, but […] to be able to say: ‘Yes I am suffering from mental illness, [but] I am becoming autonomous and self-sufficient; I am someone’. (Nancy) He feels like a somebody. He doesn’t need [his parents] to tell him well, ‘do this, go to bed at this time, do not forget to take out your trash’. It comes from him. Often he calls me and says: ‘Mother, today I have to sweep my floor, my bathroom is done’ … It comes from him. That’s important; he feels important, [and] he is proud: ‘See, I did my washing, I did my housework, I cleaned my cat’s litter’. (Joanne)
Meaning and purpose
Quality of life
Family members noticed an increase in their loved one’s quality of life since moving into supported housing. For some tenants, housing plays a direct role in improving physical and mental health: ‘[this apartment] was exactly what he wants. That’s what makes him happy, nothing else’ (Alexandre). For others, supported housing provides the resources that facilitate improvements in health and well-being, as Olivia explains,
Here he goes to the gym, which is something he never would have done before. He’s been doing that for 1 ½ years, he’s lost 70 pounds. It’s amazing, I’m happy about that, because it gives him something to do […] it’s good for [his] mental and physical health.
Aspects of tenants’ independent living space also directly improve their quality of life:
He is eager to take care of his apartment; all of his things are his […] It is much more beautiful [than previous housing]. For him, to live in a beautiful environment is in part what allows him to appreciate life, to appreciate being empowered. (Dorothée)
Rebuilding of life
Maintaining housing stability is a major contributing factor that helps tenants rebuild their lives and foster personal recovery. Some families understood recovery itself in terms of housing stability:
It’s a good place for her to get her life back, and to maintain that life. I cannot imagine a better living situation for Beatrice [….] If the future holds nothing more for Beatrice than what she has now I think that that would be okay; she’s in a good place, [this is] the best I’ve ever seen her. (Jonathan)
Several participants also noted the role of financial stability in helping tenants rebuild their lives, which was achieved through rent geared to income and developing money management skills.
Although most family members believed that supported housing enables tenants to rebuild their lives, some highlighted limitations. For some, the increased autonomy in supported housing may present new challenges for tenants who struggle with addictions, for instance,
I wouldn’t say [current housing] is the best place […] other residents cause Jerry to do things he shouldn’t do […] He’s gotten involved with some of them and he has consumed alcohol to excess and when that happens his behaviour becomes very disturbing and I think other people enable him to do that by making easier for him to get alcohol or providing companionship when he’s drinking. (Jerry’s doctor)
Structural and macro-level issues such as social welfare may also pose barriers to life rebuilding:
[I]t would be great if Beatrice could get a job, right? Get a bit of autonomous income, partly because she could need the money and partly because it’s a healthy thing to do in all kinds of ways. It’s self-validating, you meet people and you participate in society, [but] I wouldn’t want to see her get her welfare cut off because ‘oh now you’re making $5000 a month so we aren’t going to give you the $850 anymore’. (Jonathan) People who really need [government subsidies] like Joseph, he really contributes to society, and other people he knows like some friends of his here, they’re the people that need a little extra, not the guy that’s already got several million. (Wanda)
Empowerment
Personal responsibility
Although living independently in supported housing requires a high degree of personal responsibility, families described the changes in tenants’ desire and ability to develop the necessary skills to meet these demands:
I think it’s brought out her sense of initiative! […] she’s really using her initiative now whereas she didn’t have to before. Her meals were prepared, there was no grocery shopping to do […] She’s empowered because she’s able now to make her own decisions on these things whereas before they were made for her, so she didn’t have to even put forward any effort […] I think it’s nurturing her independence and sense of responsibility. (Emily)
Family members such as Olivia and Gino also discussed how these ‘real-world’ skills such as grocery shopping, cooking and cleaning have led to tenants’ increased self-confidence since living in supported housing. However, a minority of family members (n = 3) describe how tenants with addictions face difficulties in maintaining fiscal responsibility:
When he first moved in, I thought he was capable of handling his [cable] and telephone and so I put the account in his name and he did not do well with that and overspent wildly […] He has difficulty handling money; money gets used for other things and sometimes not the things that it should be used for. (Dan) His [stipend] is not enough for him because he smokes too much. He burns his money […] He is smoking more and more So his money, poof! He can burn $25 in a day or two for cigarettes, it’s horrible. (Alexandre)
Control over life
Most families (n = 11) attribute their loved ones’ increased autonomy and control over life as a central change engendered by supported housing. As Wanda asserts, ‘particularly [for] people who’ve had mental health problems, there’s often a feeling of helplessness and a feeling of not being in control. And [supported housing] gives the control back to the residents’. Family members stressed the importance of flexible daily scheduling, with tenants being able to do ‘anything they want, whenever they want’. Others emphasized the importance and recovery potential of having freedom:
He’s free where he is […] I think it’s mostly that, in my opinion; when he got there, the freedom that he had at home to arrange his apartment to his liking, that’s important to him. Over there it was already arranged […] While here, it’s ‘I can put my TV there’, there’s room. It’s important for him. (Joanne) I feel that he feels more free, he does what he wants when he wants […] he goes at his own pace […] and he does his cleaning and laundry, when he feels like it. (Lorraine)
Discussion
Families’ views on the role of supported housing in personal recovery align well with the CHIME framework. Participants report how supported housing has helped to rebuild and redefine their loved ones’ identities and has improved the quality of their lives, enabling them to reinforce their personal resources and social connections. Families also describe how living independently in supported housing has developed and strengthened tenants’ sense of normalcy, autonomy and empowerment. Families repeatedly stressed the impact of supported housing on enabling tenants to (re)gain control over various facets of their lives, a connection also noted by others (Corrigan, 2003; Nelson, Hall, & Walsh-Bowers, 1998). However, our data highlight important facets of recovery processes, particularly in relation to Connectedness and Hope and Optimism, which have not been fully specified or addressed by CHIME.
Our first key finding is the role of supported housing in (re)building and strengthening relationships between tenants and their families. Our findings reveal that the move into supported housing catalyzes shifts in tenant–family dynamics. One reason for this shift is the stability and security supported housing offers, which avails tenants of the opportunity to pursue ‘higher order’ needs and goals, such as connection with others and striving toward self-actualization (Clarke, Oades, & Crowe, 2012). That said, housing-related resources are not a panacea: tenants continue to require financial and other forms of support from family after moving into supported housing. Nonetheless, tenants now have more material and emotional resources necessary to (re)build relationships with their families. This increased social reciprocity reflects and fosters broader growth and recovery processes.
Historically, much psychiatric research has cast families under a pathological gaze (Aldersey & Whitley, 2015). More recent research recognizes the economic, instrumental and emotional support families provide (Clark, 2001; Cohen et al., 2013) but often represents those with SMI as passive recipients of this support (Reupert, Maybery, Cox, & Scott Stokes, 2015). This study builds on the small but growing body of work highlighting the reciprocal nature of relationships between those with SMI and their families (see Hamera, Cobb, & Burris-Fish, 1998; Haselden et al., 2017; Pernice-Duca, 2010), illustrating how these relationships evolve within – and partially because of – supported housing. The centrality of relationships in our findings supports current research focusing on mutuality and reciprocity as key to personal recovery (Deering & Williams, 2017). It contributes to this literature by being the first to detail how reciprocity and mutuality in familial relationships support recovery in the context of supported housing. Our findings also support recent calls for a ‘relational’ understanding of mental health recovery, which cast it as an inherently social (rather than individual) process (Reupert et al., 2015; Tew et al., 2012).
Our second central finding concerns families’ views on their loved one’s aspirations and future. While families felt that supported housing has facilitated other components of recovery such as Connectedness, Identity and Empowerment, they expressed skepticism about the future, stressing the limits of recovery. Research has identified biogenetic explanations for mental illness as common among families (Aldersey & Whitley, 2015), which may partially explain their ‘cautious optimism’ (Tweedell, Forchuk, Jewell, & Steinnagel, 2004). Curiously, their skepticism coalesced with assertions of improvement in most other areas of tenants’ lives.
There may be several underlying explanations for why families are skeptical about the future and lack hope and optimism. First, families may have become accustomed to witnessing or helping their affected family member through crises or problems and may not allow themselves to think about the future or have deep doubts that anything will eliminate their loved one’s mental health problems. These families have likely experienced long-term and intense stress and conflict with their loved one in the past and thus remaining cautious about the future may be a self-protective strategy. Second, professionals with whom families have dealt over the course of their loved one’s illness may have never encouraged them to be hopeful: the traditional approach has been ‘don’t expect your loved one to be able to work, live on their own, or have a relationship/family’ (Vistorte et al., 2018). Finally, perhaps families lack ‘champions’ or examples of others in similar positions who have hopes and aspirations for loved ones with similar conditions. Without a ‘reference point’, perhaps families do not incorporate hope and optimism into their personal schemas concerning mental illness.
Families’ lack of hope and optimism for a ‘full’ recovery including future employment or future educational pursuits has implications for conceptualizations and operationalization of personal recovery. Psychiatric research to date has often framed personal recovery in terms of hope, optimism and resilience, at the expense of acknowledging difficulties and complexities inherent to recovery processes (Hancock, Smith-Merry, Jessup, Wayland, & Kokany, 2018). The lack of attention to continuing symptoms and morbidity has led some to critique CHIME as too optimistic (Connell, O’Cathain, & Brazier, 2014; Stuart, Tansey, & Quayle, 2017). In our study, family perspectives highlight the non-linear understandings of recovery, where the goal is not necessarily ‘getting better’ or ceasing to need support (Slade et al., 2014). Our findings also suggest a reworking of the CHIME framework to better account for continuing difficulties and setbacks that may be experienced in recovery.
Limitations
As with all qualitative research, first, the findings of this study are limited in their generalizability and should be considered with reference to the specific housing sites, provincial settings and national contexts in which they are embedded. Second, our sampling strategy precluded interviewing family members who may be estranged or geographically distant from tenants living in supported housing and therefore may not capture the full scope of family perspectives.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This research was funded by the Canadian Institutes of Health Research Grant Award #299123.