
Abstract
Background:
The positive association between adverse life events and somatoform disorders is a consistent observation. But no systematic studies have evaluated the relationship between health-related life events (HLEs) in patients with somatic symptom disorder (SSD)/somatoform disorders.
Aim:
To examine the nature and relationship of HLE in patients with SSD and to assess the correlates of HLE.
Methods:
A total of 50 adult patients with SSD and 50 matched healthy controls from a Neuropsychiatric hospital were recruited. Sociodemographic interview, scale for assessment of somatic symptoms (SASS), Patient Health Questionnaire-15 (PHQ-15) and a semi-structured interview schedule to gather information on HLE were used.
Results:
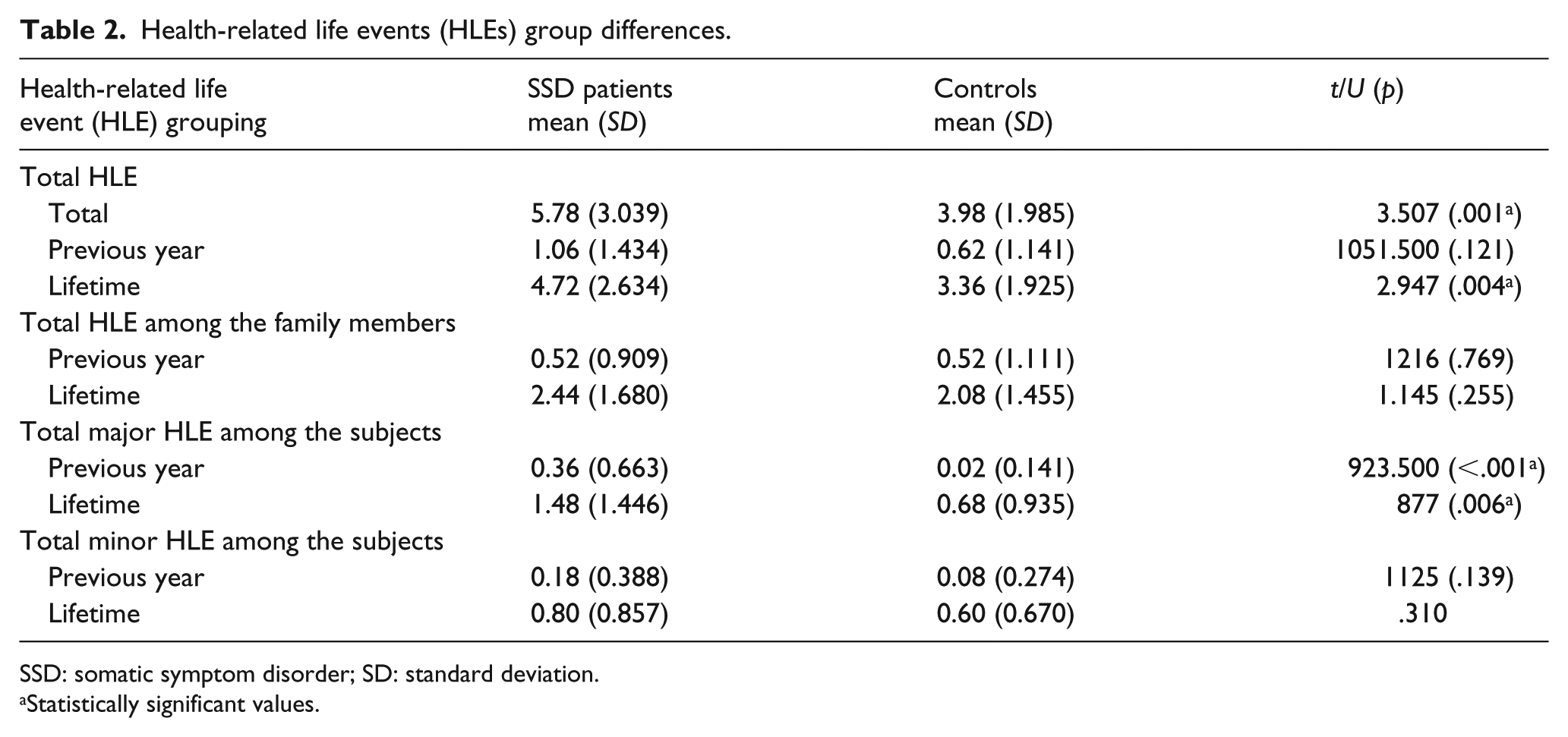
Patients in the SSD group had a significantly higher number of total HLE in general (4.72 ± 2.63, 3.36 ± 1.92; p = .004), major HLE (1.48 ± 1.45, 0.68 ± 0.94; p = .006), during their lifetime in comparison to controls. Infections, trauma, non-communicable diseases and reproductive system–related diseases were the more common types of HLE in SSD group.
Conclusion:
Our findings may implicate a role of major HLE of patients and HLE of their family members in the pathophysiology of SSD.
Introduction
Somatic symptom disorders (SSDs) are common mental disorders in which an individual has one or more distressing somatic symptoms at least for a period of 6 months along with any one of the following – disproportionate thoughts about its seriousness or persistent high levels of anxiety or excessive time and energy devoted to these symptoms (American Psychiatric Association, 2013). Patients with SSD often undergo an unending series of repetitive diagnostic and intervention procedures to find cause for their symptoms and may place strain on the health resources (Chaturvedi & Bhandari, 1989; Chaturvedi, Chandra, Issac, & Sudarshan, 1993; Chaturvedi & Maguire, 1998; Escobar, Hoyos-Nervi, & Gara, 2002; Hiller, Fichter, & Rief, 2003). Somatization has been described as bodily manifestation of underlying psychosocial stress. Adverse life events bring an enormous amount of stress within a brief span of time, often exceeding the coping abilities of a person, and do have a significant role in the etiology of many physical as well as psychiatric illnesses including the somatoform disorders. The positive association between adverse life events and somatization had been a study topic since the early 1970s. The limited available literature had explored the of role different aspects of life events in the process of somatization including the following: the nature or types of life events, its occurrence in the timeline of a patient’s life course (with respect to the onset of SSD), differential contributions of recent versus remote, cumulative effects of life events as well as the neurobiological and psychological mechanisms to explain such an association. Majority of the studies lack methodological rigor and issues with the diagnostic criterion they used as well the study group or the settings they studied (Chandrashekhar, Reddy, & Isaac, 1997; Fava & Sonino, 2005; Hartvig & Sterner, 1985; Park et al., 2014; Tak, Kingma, Van Ockenburg, Ormel, & Rosmalen, 2015). Among the available literature on life events in relation to somatoform disorders, we found a frequent positive association between a variety of health-related life events (HLEs) and somatoform disorders, such as an excessive occurrence of physical illnesses, deaths/accidents, hospitalizations, and surgeries among patients themselves and/or their family members (Hotopf, 2002; Park et al., 2014; Tak et al., 2015; Tschudi-Madsen et al., 2014). However, the studies have not specifically assessed HLEs.
HLE is a life event which primarily involves various aspects of a person’s health, and related to illness. There is no standard way of defining a HLE as there is no pre-existing definition available. It is biologically plausible to assume that HLE are more closely associated with perturbations in neuroendocrine (e.g. hypothalamic–pituitary–adrenal (HPA) axis alterations) and neuroimmunological (e.g. cytokine) systems than life events (LE) (Karlsson, 2008). Based on above, we hypothesize that the nature and type of HLEs in SSD patients is different from that of healthy controls.
Methods
Subjects and sampling
This cross-sectional, case-control design included 50 patients with SSD based on the Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5) criteria, receiving care from outpatient services, Department of Psychiatry (National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, India) over a 10-month period. Control group consisted of 50 healthy controls matched for age, gender and education (1:1 matching was done in these parameters).
Criteria for inclusion in the study were the following: (1) age group of 18–65 years, (2) either gender, (3) diagnosis of SSD according to the DSM-5 criteria and (4) providing informed consent. Exclusion criteria were as follows: (1) current medical illness that may significantly influence central nervous system function or structure (including intellectual developmental disorder, epilepsy and head injury), (2) Serious medical comorbidities such as cardiac decompensation, ischemic heart disease and cancers, (3) pregnancy or postpartum (<6 weeks after delivery/miscarriage), (4) family history of hereditary neurological disorders (such as Wilson’s/Huntington’s diseases), (5) comorbidities of DSM-5 based substance use disorder within the past 6 months, except tobacco consumption and (6) visual/auditory impairment. The study was approved by NIMHANS Institutional Ethics Committee (IEC) (Ref. No. NIMH/DO/ETHICS SUB-COMMITTEE 28TH MEETING/2016) and all the participants gave written informed consent.
B.R. did a systematic sampling by screening every alternate patient with a diagnosis of somatoform disorder. After ascertaining the SSD diagnosis, they were evaluated for suitability for the study. Out of 70 eligible patients, 54 patients (77%) consented to participate. Later, the data of four patients were excluded because of suspicion of comorbid neuropathy-related illness (two), recent alcohol use (one) and other reasons (one).
Our healthy controls were recruited from the hospital acquaintances. Among them, the majority were family members of patients with different psychiatric conditions (other than SSD) visiting outpatient services (of general psychiatry or de-addiction unit). The matched controls were selected by purposive sampling. History of mental illness or any physical illness was ruled out by an interview.
Clinical assessments
The socio-demographic details were recorded using a structured pro forma, including age, gender, socio-economic status, occupation, contact details, years of education, duration of illness, history of any medical illnesses, and treatment history including medications being used at present, drug dosage, duration and side effects.
Patients were administered the scale for assessment of somatic symptoms (SASS) which is used to measure somatic symptoms and their severity in clinical settings. This scale has four subscales, namely, pain-related symptoms, sensory somatic symptoms, non-specific somatic symptoms and biological function–related symptoms. The severity of somatic symptoms is rated from 0 to 3; 0 = Absent, 1 = Mild, 2 = Moderate and 3 = Severe. The somatic symptoms are said to be present if the symptoms have occurred during the previous 2 weeks. SASS scale has been validated in Indian settings (Desai, Chaturvedi, Dahale, & Marimuthu, 2015). PHQ-15 is a brief, self-administered questionnaire that is useful in screening for somatization and in monitoring somatic symptom severity in clinical practice and research. Subjects were asked to rate the severity of 13 symptoms as 0 (not bothered at all), 1 (bothered a little) or 2 (bothered a lot) in the last 4 weeks. Thus, the total PHQ-15 score ranged from 0 to 30 and scores of ⩾5, ⩾10, ⩾15 representing mild, moderate and severe levels of somatization. The reliability and validity of the PHQ-15 has been established in clinical settings (Kroenke, Spitzer, & Williams, 2002).
After the administration of rating scales, a clinical interview was conducted using a semi-structured interview schedule to assess HLE designed specifically for this study. As no prior studies had used any rating scales or interview schedules to assess HLE, we developed a semi-structured interview schedule called ‘the schedule for health-related life events’ (S-HLE; details of the schedule is in Supplemental Appendix 1) validated by consensus of experts. This interview consisted of open-ended questions to elicit details of the HLE.
Statistics
Socio-demographic data and clinical characteristics of the study population were computed using descriptive statistics such as mean, the standard deviation (for continuous variables) and percentages of frequencies (for categorical variables).
Frequencies as well as in the form of following four clusters – total number of HLE, total number of HLE among the family members, total number of major HLE and total number of minor HLE in the subjects with respect to the previous year and lifetime occurrence were derived. The Mann–Whitney U-test/unpaired t-test was used to compare the mean differences between the cases and controls across the above clusters. The subsequent analyses compared the HLE clusters with socio-demographic variables and SASS/PHQ-15 scores, using the Mann–Whitney U-test/unpaired t-test.
Results
Characteristics of the study population
A total of 50 patients with SSD and 50 healthy controls were matched for age (±1 year), gender and educational level (less than class 7; more than class 7). The mean age was 48.9 years (SD = 9.318) for patients with SSD with a range from 26 to 65 years. The mean duration of illness was noted to be relatively long (12.5 years (SD = 8.638)) with a minimum and maximum duration of illness were 1 and 33 years. Majority of them were Hindus (88%) and most of them (98%) were from lower socio-economic status and belonged to rural background (74%) in the SSD group and 58% were from urban background in the control group. Comorbid medical illness was noted in 7 (14%) person in SSD group and 10 (20%) in control group. The most common symptoms among the patients included – headache (50%), pain in the extremities (46%), backache (44%) and weakness of body (42%) on SASS scale. On the PHQ-15 scale, the most common symptoms were – headache (38%), backache (32%), pain in arms or legs or other joints (30%) and feeling tired or having low energy (26%). There was no statistically significant difference between patients and healthy controls in terms of age, gender, education, marital status, residence, socio-economic status and history of medical illnesses.
The mean severity score on SASS total was 15.72 (SD = 3.326) for cases with SSD. Mean scores on PHQ-15 total was 9.20 (SD = 5.178) for cases and 1.52 (SD = 1.992) for controls. A total of 42% of the cases had moderate to severe grades of somatic symptoms on the PHQ-15.
Comparisons of the HLE between the groups
Patients with SSD had a higher frequencies on certain clusters such as the HLE among the family members during lifetime, which means the family members had a higher number of surgeries (36% vs 26%), serious physical illnesses (26% vs 20%), sudden death (62% vs 44%) and higher expenditure for physical illnesses (44% vs 22%), whereas the control group had a higher frequencies for the rest of the categories, that is, deaths due to prolonged illnesses (40% vs 24%), hospitalizations (56% vs 52%) during lifetime, and serious diseases (12% vs 10%) and hospitalizations during previous year (24% vs 14%).
Details of the major HLE both lifetime and the previous year in persons with SSD in comparisons to healthy controls is given in Table 1. Patients with SSD had higher frequencies of certain minor HLE like falls/injuries (28% vs 14%) and minor surgeries (8%vs 4%) during the lifetime (Table 1).
Frequencies of health-related life events (HLEs).

The mean number of life events among the SSD group were higher for major HLE during the previous year as well as lifetime, total HLE in general and lifetime (Table 2).
Health-related life events (HLEs) group differences.
SSD: somatic symptom disorder; SD: standard deviation.
Statistically significant values.
Nature of the HLE
Among the types/nature of HLE, excluding the mental health–related issues, the frequencies of nature of HLE among persons with SSD and controls were infections (56% vs 50%), trauma-related diseases (26% vs 20%), non-communicable diseases (24% vs 6%), and reproductive system–related problems (26% vs 12%). There was no significant association of the demographic variable with total HLE. Among the infections, chikungunya fever, typhoid, malaria were common among patients with SSD, whereas pulmonary tuberculosis, diarrhea, sepsis were the common diagnoses among the family members.
Discussion
The most important finding of our study was that the patients with SSD had a significant occurrence of total HLE during their lifetime. Higher rates of major HLE were seen in the previous year as well as lifetime occurrence among patients with SSD. HLE among family members was not different between the cases and controls. Although the minor HLE of subjects did not differ between both the cases and controls, certain individual items of this cluster such as falls/injuries, minor surgeries were more common among the cases.
Patients with SSD had a higher frequencies of certain HLE like – the HLE of the family members during the lifetime, such as more number of surgeries, serious physical illnesses, sudden death, and a higher expenditure for physical illnesses which is in accordance with the existing literature reporting higher occurrences of medical illnesses among the family members of somatoform disorders (Gulhati & Minty, 1998; Poikolainen, Kanerva, & Lonnqvist, 1995). Psychological mechanisms like social learning have been consistently reported as an explanation (Jamison & Walker, 1992; Kozlowska, 2013; Van Tilburg et al., 2015).
However, while interpreting this finding, we acknowledge that the recruitment of healthy controls from hospital acquaintances, may have led to higher frequencies of mental health–related HLE among the family members of healthy control. This possibly affected all other components of the domain because recruitment of the healthy control from de-addiction unit (i.e. healthy family member of a patient belonging to the ‘de-addiction unit’) can affect all the subcomponents of this domain of ‘HLE interview schedule’.
Patients with SSD had higher frequencies of certain minor HLE like falls/injuries and minor surgeries during the lifetime (Hotopf, 2002; Weck, Neng, Göller, & Müller-Marbach, 2014). One prior published study did not find such an association between the HLE and the group with somatoform disorders, where they had studied illness-related life events among the 16- to 19-year-old adolescents. But another study found a positive association, that is, higher occurrences of childhood/past experiences of medical illnesses (Bonvanie, Janssens, Rosmalen, & Oldehinkel, 2017).
Patients with SSD had higher frequencies of all types of HLE like infections, trauma-related, reproductive system–related problems and non-communicable diseases in comparison to controls. This high occurrence of infections like chikungunya fever among the SSD patients would hypothesize a role to the immune-inflammatory pathways in central pain processing circuitry. Prior research has postulated that neuroimmune factors like cytokines can modulate central pain processing pathways and can cause alterations in HPA axis, thereby has a role in the etiology of SSDs (Frodl, 2016; Kleinman, 1982; Kozlowska, 2013).
Among the reproductive system–related illnesses, patients with SSD had a four-fold higher frequencies of dysfunctional uterine bleeding, total abdominal hysterectomies, tubectomies and polycystic ovarian syndrome (PCOD) diagnoses. Studies have reported that women with somatic symptoms do link their somatic symptoms with reproductive system–related symptoms like abnormal bleeding, vaginal discharge (Chaturvedi et al., 1993).
Wide-ranging types of non-communicable disease were present among the family members of patients, but strokes and cancers of the upper aerodigestive tract were the most common occurrences.
Despite strengths like the exclusion of comorbid psychiatric disorders, and having a homogeneous sample, our study has certain limitations. The semi-structured interview in this study to assess HLE may be a relative limitation, hence the interpretation of the results of the associations need to taken with caution. However, as there are no specific tools to assess HLE at present, this information from the semi-structured interview may add a broad framework for development of an instrument/scale to assess HLE. The mean duration of illness in our patient population was 12.5 years, and this may present difficulties in the interpretation of cause or effect relationship of the HLE in somatization. In addition, the temporality of association is difficult to establish with this design; a prospective design can answer it. It should be noted that the nature of family structure was not recorded. It is possible that some of the subjects from rural areas may have extended or joint families. We did not assess the nature of relationship with the family members which could have influenced the reporting of HLE. Future research should include this variable of family typology and the nature of relationship. Last but not least, recall and attentional bias cannot be ruled out in our study as with most life event researches.
Conclusion
This study found that patients with SSD have higher rates of HLE in comparison to healthy controls, such as major HLE and HLE among the family members. Cumulative physical illnesses or life events are known to be associated with the modulation of HPA axis which also had an influence on the neuroimmune factors like cytokines, which in turn can affect the central pain processing pathways (Fava & Sonino, 2005; Frodl, 2016; Kozlowska, 2013). Therefore, our finding may implicate a theoretical support to the neurobiological research of SSD in finding how these repeated/cumulative HLE can be translated in the etiopathogenesis, although further studies needed to confirm the cause or effect nature of these HLE.
Supplemental Material
supplementary-HLE_Schedule – Supplemental material for Health-related life events in patients with somatic symptom disorders: A case control study
Supplemental material, supplementary-HLE_Schedule for Health-related life events in patients with somatic symptom disorders: A case control study by Balaswamy Reddy, Santosh Kumar Chaturvedi, Geetha Desai, Narayana Manjunatha and Srinivas Guruprasad in International Journal of Social Psychiatry
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.