
Abstract
Background:
Psychological distress is an undersearched cause of poorer health in the Pacific island countries.
Aims:
The study aimed to investigate the prevalence and associated factors of psychological distress in a population-based survey among 18–69 year-old persons in Solomon Islands.
Method:
Cross-sectional nationally representative data of 2,533 18–69 year-old persons (38 years were the median age) from the 2015 Solomon Islands STEPS survey were analysed.
Results:
The results indicate that 18.9% of participants had psychological distress (⩾20 scores), 13.4% had mild (20–24 scores), 4.3% moderate (25–29 scores) and 1.1% severe (30–50 scores) psychological distress. In adjusted logistic regression analysis, being divorced, separated, or widowed (AOR: 2.76, 95% CI: 1.60–4.78), having had a heart attack or stroke (AOR: 3.34, 95% CI: 2.23–4.99), alcohol dependence (AOR: 1.72, 95% CI: 1.04–2.84), and sedentary behaviour (AOR: 1.90, 95% CI: 1.28–2.84), were positively and the consumption of 3–4 servings of fruit and vegetables (AOR: 0.62, 95% CI: 0.42–0.92), were negatively associated with psychological distress (⩾20 scores). In addition, in a sex stratified adjusted logistic regression analysis among men, current smokeless tobacco use (AOR: 4.95, 95% CI: 1.66–14.75), was associated with psychological distress. Furthermore, in the overall unadjusted analysis, stop smoking attempts in the past 12 months and consumption of too much salt was associated with psychological distress.
Conclusion:
Almost one in five participants were reported psychological distress and several factors were detected which could be targeted in intervention activities.
Introduction
The American Psychological Association (APA) defines psychological distress as ‘a set of painful mental and physical symptoms that are associated with normal fluctuations of mood in most people. It is thought to be what is assessed by many putative self-report measures of depression and anxiety’. Psychological distress has been measured with different screening instruments, such as the ‘Psychological Distress Scale’, K-6 or K-10 and the ‘General Health Questionnaire (GHQ-12)’, and is commonly used to describe the extent of population mental health (Drapeau et al., 2014). High rates of mental ill health have been reported in the Pacific island nations (Hunter et al., 2015; Lui et al., 2018; Peltzer & Pengpid, 2015), but there has been a lack of community-based national data on psychological distress in Pacific Island countries, such as in Solomon Islands.
In national population-based surveys, the prevalence of psychological distress was 26.8% in Japan (20–74 years old, K-6 scores ⩾5) (Sakurai et al., 2010), in Australia 11.1% in 2011/2012 and 10.0% in 2007 (18–64 years; K-10, scores 12 and over) (Enticott et al., 2016), in South Africa 23.9% (⩾15 years; K-10, scores ⩾20) (Mthembu et al., 2017), and 20.7% in Canada (⩾15 years, K10) (Caron & Liu, 2011).
Factors associated with psychological distress include sociodemographic variables, biopsychosocial stressors, and poor health behaviour. Sociodemographic factors associated with psychological distress include female sex (Cockerham et al., 2006; Kuriyama et al., 2009; Matud et al., 2015; Mthembu et al., 2017), older age in South Africa (Mthembu et al., 2017), younger age in South Australia (Chittleborough et al., 2011), not married (Mthembu et al., 2017; Takeuchi & Speechley, 1989), low education (Chittleborough et al., 2011; Enticott et al., 2016), low income (Caron & Liu, 2011; Chittleborough et al., 2011), lower subjective social status (Sakurai et al., 2010), lower socioeconomic status (Myer et al., 2008), lower wealth (Enticott et al., 2016), unemployed (Mthembu et al., 2017), and lower social capital (Chittleborough et al., 2011; Kuriyama et al., 2009; Myer et al., 2008).
Biopsychosocial stressors associated with psychological distress include stressful life events (Caron & Liu, 2011; Lui et al., 2018), history of serious disease, such as stroke, myocardial infarction, or cancer (Kuriyama et al., 2009), cardiovascular disease (Chittleborough et al., 2011), hypertension (Ojike et al., 2016), arthritis (Chittleborough et al., 2011), being HIV positive (Mthembu et al., 2017), general underweight (Kuriyama et al., 2009), functional disability (Okoro & Dhingra, 2014) and passive smoking (Bang et al., 2017).
Health risk behaviours associated with psychological distress include low physical activity (Pengpid & Peltzer, 2019; Rees et al., 2012; Sloan et al., 2013), lower walking time (Kuriyama et al., 2009), low leisure-time physical activity (Chu et al., 2018), high sedentary behaviour (Chu et al., 2018; Pengpid & Peltzer, 2019; Sloan et al., 2013), hazardous alcohol use (Mthembu et al., 2017), frequent drinking in men (Cockerham et al., 2006), current smoking (Chittleborough et al., 2011; Kuriyama et al., 2009; Leung et al., 2011; van der Deen et al., 2011), unsuccessful smoking quitters (van der Deen et al., 2011; Leung et al., 2011), former smoking (Kuriyama et al., 2009), less often daily meat consumption in men (Cockerham et al., 2006), less often daily vegetable and fruit consumption in women (Cockerham et al., 2006; Hinote et al., 2009), and inadequate fruit and vegetable intake (Richard et al., 2015).
The study aimed to investigate the prevalence and associated factors of psychological distress in a population-based survey among 18–69 year-old persons in Solomon Islands. Several models will be used to assess the determinants of psychological distress: (1) mild to severe psychological distress (scores 20–50) as outcome, (2) psychological distress with different cut points (10–19 scores no distress, 20–24 mild, 25–29 moderate and 30–50 severe distress), and (3) psychological distress as a continuous outcome.
Methods
Sample and procedure
Cross-sectional data from the 2015 Solomon Islands STEPS Survey were analyzed (WHO, 2018). A multistage cluster sample design was used to produce representative data for the age range 18–69 years in Solomon Islands; the overall response rate was 58.4% (WHO, 2018). The questionnaire was administered through a personal digital assistant (PDA) (WHO, 2018). The Solomon Islands National Health Ethics Review Committee provided ethics approval of the study, and written informed consent was obtained from the study participants (WHO, 2018).
Measures
Outcome variables included psychological distress assessed with the Kessler Psychological Distress Scale (K10) (Kessler et al., 2002). The K10 is based on 10 questions measuring the frequency of nonspecific psychological distress symptoms during the past 4 weeks. For example, ‘During the past 4 weeks, how often did you feel sad or depressed?’ Response options ranged from 1 = none of the time to 5 = all the time. K10 item scores were summed to give a possible cumulative score range of 10–50. Total scores were categorised into four strata including: no psychological distress (10–19), mild (20–24), moderate (2–29), and severe psychological distress (30–50) (Kessler et al., 2002). Cronbach’s alpha for the K10 was 0.85 in this sample.
Sociodemographic information included sex (male, female), age (18–69 years), highest level of education (no formal schooling, less than primary school, primary school completed, secondary school completed, high school completed, college/university completed, and post-graduate degree) and marital status (never married, currently married, separated, divorced, widowed and cohabiting) (WHO, 2018).
Biopsychosocial stressor variables included alcohol family problems (‘During the past 12 months, have you had family problems or problems with your partner due to someone else’s drinking?’), passive smoking in the past 30 days (at home or in closed spaces at work) and history of ‘heart attack or stroke’. Hypertension was assessed based on measured blood pressure (BP) ‘(mean of the last two of three readings) defined as systolic BP ⩾140 mm Hg and/or diastolic BP ⩾90 mm Hg or currently on antihypertensive medication’ (WHO, 2018).
The health risk behaviour variables included current smoking, current smokeless tobacco use, past smoking, stop smoking attempts in the past 12 months, alcohol dependence, salt consumption (eating processed foods high in salt and how much salt consumed), consumption of fruit and vegetables per day, and based on the ‘Global Physical Activity Questionnaire’, sedentary behaviour and high, moderate and low physical activity (WHO, 2018). Physical activity was categorised by the median metabolic equivalent (METs) of performed activities as low (‘total physical activity METs minutes per week is < 600’), moderate (‘3 or more days of vigorous-intensity activity of at least 20 minutes per day OR; five or more days of moderate-intensity activity or walking of at least 30 minutes per day OR; five or more days of any combination of walking, moderate or vigorous intensity activities achieving a minimum of at least 600 MET-minutes per week’) and high (‘vigorous-intensity activity on at least 3 days achieving a minimum of at least 1500 METs minutes per week OR; seven or more days of any combination of walking, moderate or vigorous intensity activities achieving a minimum of at least 3,000 MET-minutes per week’.) physical activity (Armstrong & Bull, 2006, WHO, 2012). Alcohol dependence was assessed with three questions of the ‘Alcohol Use Disorder Identification Test = AUDIT’ (items 4–6), for example, ‘How often during the last year have you found that you were not able to stop drinking once you had started?’ Response options ranged from ‘0 = never to 4 = daily or almost daily’; total scores of 4 or more indicate alcohol dependence (Australian Government, 2020).
Data analysis
Statistical procedures were conducted with STATA software version 15.0 (Stata Corporation, College Station, Texas, USA), considering the multistage cluster sample design. Analysis weights were calculated by taking the inverse of the probability of selection of each participant. These weights were adjusted for differences in the age-sex composition of the sample population as compared to the target population (WHO, 2018). Several models are used to assess the determinants of psychological distress. First, binary logistic regression is used with mild to severe psychological distress (scores 20–50) as outcome, second, multinomial logistic regression with different cut points of psychological distress (10–19 scores no distress, 20–24 mild, 25–29 moderate and 30–50 severe distress; the latter two were collapsed because of too few cases in the severe distress category), and third Poisson regression with psychological distress as a contiuous outcome. In the binary logistic regression and the Poisson regression model, both univariate and multivariable models are presented, while for the multinominal regression model only the multivariable model is presented, with mild (20–24 scores) and moderate-severe (25–50 scores) psychological distress as outcomes and no psychological distress (10–19 scores) as reference category. Missing values were not included in the analysis and p < 0.05 was seen as significant.
Results
Psychological distress and sample characteristics
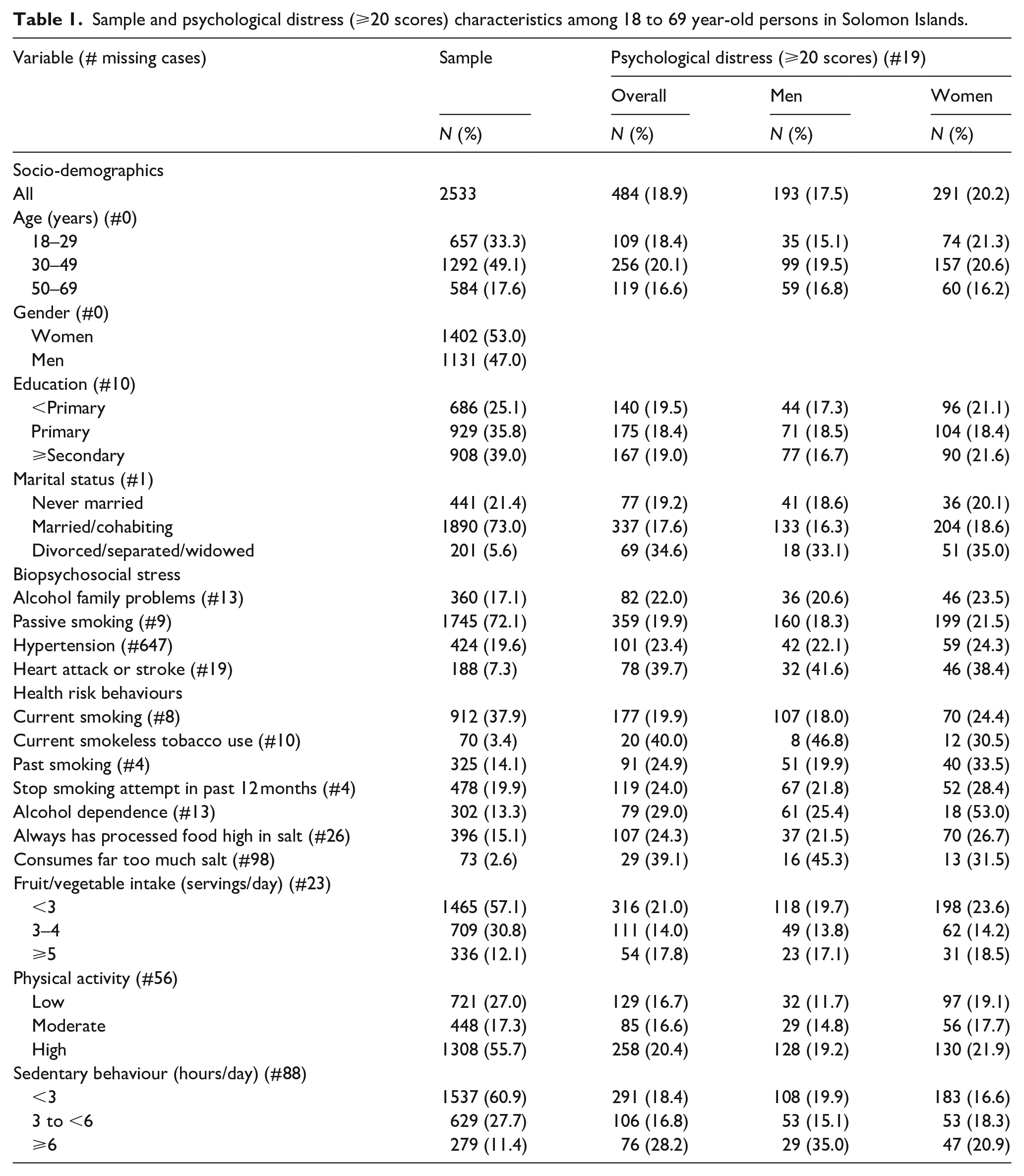
The study population consisted of 2,533 18–69 year-old adults (Median = 38 years, IQR = 29–48), 53.0% were female, 39.0% had secondary or more education, 17.1% reported alcohol family problems, 72.1% were exposed to passive smoking, 19.6% had hypertension and 7.3% had had a heart attack or stroke. More than one in three participants (37.9%) were current smokers, 13.3% were dependent on alcohol, 15.1% had always processed food high in salt, 12.1% had five or more servings of fruit and vegetables per day, 55.7% had high physical activity and 11.4% engaged in ⩾6 hours a day in sedentary behaviour. Almost one in five participants (18.9%) had psychological distress (⩾20 scores), 13.4% had mild (20–24 scores), 4.3% moderate (25–29 scores) and 1.1% severe (30–50 scores) psychological distress (see Table 1). The mean score on the K10 are 15.0 (Standard Error 0.01) and the median scores on the K10 were 14.0 (interquartile range: 11–18).
Sample and psychological distress (⩾20 scores) characteristics among 18 to 69 year-old persons in Solomon Islands.
Associations with psychological distress (K10: ⩾20 scores)
In the adjusted logistic regression analysis, being divorced, separated, or widowed, having had a heart attack or stroke, alcohol dependence, and sedentary behaviour were positively and the consumption of 3–4 servings of fruit and vegetables were negatively associated with psychological distress. In addition, in sex stratified adjusted logistic regression analysis among men, current smokeless tobacco use was associated with psychological distress. Furthermore, in the overall unadjusted analysis, stop smoking attempts in the past 12 months and consumption of too much salt was associated with psychological distress (see Table 2).
Associations with psychological distress (⩾20 scores) in Solomon Islands.
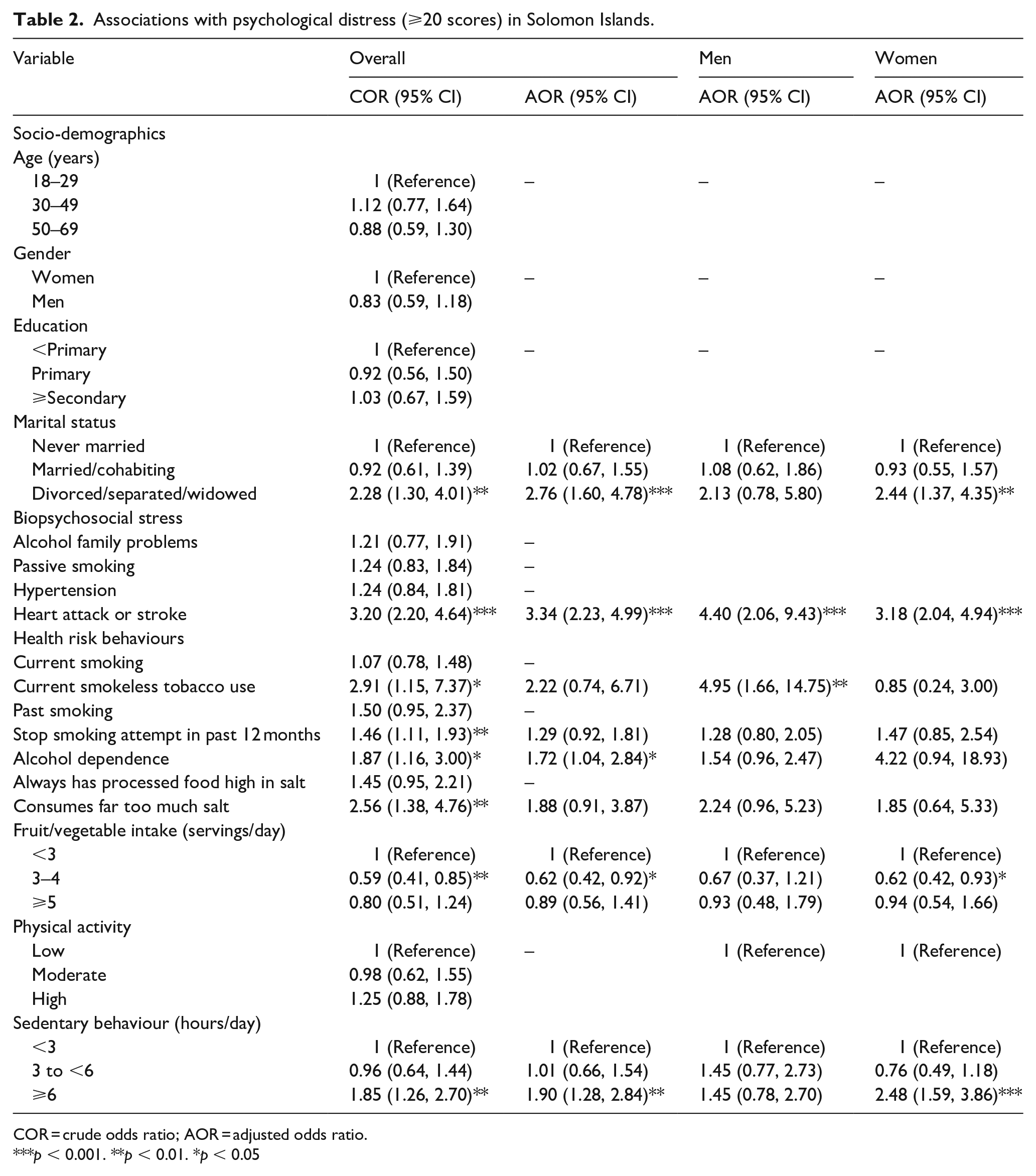
COR = crude odds ratio; AOR = adjusted odds ratio.
p < 0.001. **p < 0.01. *p < 0.05
Multinomial logistic regression and Poisson regression on psychological distress
In the adjusted multinomial logistic regression, being divorced, separated, or widowed, and heart attack or stroke were both associated with mild and moderate-severe psychological distress. Hypertension and sedentary behaviour were associated with mild psychological distress, and current smokeless tobacco use and alcohol dependence were associated with moderate-severe psychological distress.
In adjusted Poisson regression, being divorced, separated or widowed, heart attack or stroke, alcohol dependence, consuming too much salt, and sedentary behaviour were associated with higher psychological distress scores, while being male and consuming fruit and vegetables (3–4 sevings/day) were associated with lower psychological distress scores (see Table 3).
Multinomial logistic regression and Poisson regression on psychological distress.

ARRR = adjusted relative risk ratios; CIRR = crude incidence rate ratios; AIRR = adjusted incidence rate ratios
p < 0.001. **p < 0.01. *p < 0.05.
Discussion
The prevalence of psychological distress (18.9% scores ⩾20) among adults in Solomon Islands was higher than in Australia (11.1%, 18–64 years; K-10, ⩾12 scores) (Enticott et al., 2016), and lower than in Japan (26.8%, 20–74 years old, K-6 scores ⩾5) (Sakurai et al., 2010), in South Africa (23.9%, ⩾15 years; K-10, scores ⩾20) (Mthembu et al., 2017), and in Canada (20.7%, ⩾15 years, K10) (Caron & Liu, 2011). The results of this study confirm previously reported high rates of mental ill health in the Pacific island nations (Hunter et al., 2015; Lui et al., 2018; Peltzer & Pengpid, 2015). One way of improving the treatment of psychological distress is by improving or expanding primary mental health care (Bachmann, 2018), by ‘integrating mental health into general health services, strengthening family and community support systems and delivering services more equitably across the country’. (Maukera & Bligault, 2015; Orotaloa & Blignault, 2012).
Unlike some previous studies (Chittleborough et al., 2011; Cockerham et al., 2006; Enticott et al., 2016; Kuriyama et al., 2009; Matud et al., 2015; Mthembu et al., 2017), this survey did not find significant differences in the prevalence of psychological distress by age, sex and educational background. However, analysing psychological distress as a continuous measure showed that women had significantly higher psychological distress scores than men in this study. This result is confirmed in some other studies (Islam, 2019), showing no significant difference in the overall prevalence of any psychological distress but the severity of psychological distress was higher in women than in men. Compared to women who were never married or married in this study, women who were divorced, separated, or widowed had higher odds for psychological distress. Previous studies showed that being married was protective against psychological distress (Mthembu et al., 2017; Takeuchi & Speechley, 1989).
In line with previous research (Caron & Liu, 2011; Chittleborough et al., 2011; Kuriyama et al., 2009; Lui et al., 2018), this study showed that having a serious disease (heart attack or stroke) increased the odds for psychological distress. It is possible that an increase in disability in cardiovascular disease patients leads to an increase in psychological distress (Caponnetto, 2018). While a previous study showed an association between hypertension and psychological distress (Ojike et al., 2016), this study did not find a significant relationship.
In agreement with some previous investigations (Chittleborough et al., 2011; Cockerham et al., 2006; Kuriyama et al., 2009; Leung et al., 2011; Mthembu et al., 2017; van der Deen et al., 2011), this study found a positive association between alcohol dependence, and among men smokeless tobacco use, and in unadjusted analysis, stop smoking attempt in the past 12 months and psychological distress; however, current smoking was not associated with psychological distress in this study. The study also did not find an association between passive smoking and psychological distress, contrary to a previous study among adolescents (Bang et al., 2017). A possible explanation of a link between lower success in quitting smoking and psychological distress may be that distress smokers have greater nicotine addiction than mentally healthy smokers (Leung et al., 2011). Regarding alcohol dependence and psychological distress, Walter et al. (2005) note that ‘At the starting point of high alcohol consumption psychological relief due to the stress-reducing effects of alcohol is often assumed. A vicious circle begins, perpetuating psychosocial distress and reinforcing the anxious or depressive symptoms related to emerging distress syndrome’.
Consistent with previous research (Cockerham et al., 2006; Hinote et al., 2009; Richard et al., 2015), the 2015 Solomon Islands STEPS survey showed that more frequent fruit and vegetable consumption (3–4 servings) was protective against psychological distress. Fruit and vegetables are rich in antioxidants that reduce oxidative stress and decrease inflammation lowering depression (Ricard et al., 2015). Low physical activity has been shown to increase the odds for psychological distress in previous research (Chu et al., 2018; Kuriyama et al., 2009; Pengpid & Peltzer, 2019; Rees et al., 2012; Sloan et al., 2013), while in this study low physical activity did not increase the odds for psychological distress. Similar results were found in domain-specific physical activity analysis in this study. However, higher sedentary behaviour was overall and among women in this study associated with psychological distress, which concurs with former research (Chu et al., 2018; Pengpid & Peltzer, 2019; Sloan et al., 2013). People with sedentary behaviour may lack the beneficial effects of physical activity, impacting negatively on mental health (Hoare et al., 2016).
The study limitations included that this investigation was limited due to the self-report of data and the cross-sectional survey design. An additional limitation was that the STEPS survey in Solomon Islands had many missing values on household income (86.3%), anthropometric (29.4%), and biochemical (33.7%) measurements, and therefore these variables could not be included in the analysis. Furthermore, some other predictors such as history of mental disorder and exposure to adverse life events were not included in this survey.
Conclusion
This investigation showed among a nationally representative population of 18–69 years in Solomon Islands that almost one in five participants had psychological distress (⩾20 scores). Several associated factors for psychological distress were identified, such as being divorced, separated, or widowed, having had a heart attack or stroke, alcohol dependence, sedentary behaviour, and low fruit and vegetable consumption, which can be utilized in psychological distress prevention activities in the Solomon Islands population.
Footnotes
Acknowledgements
Authors’ contributions
“All authors fulfil the criteria for authorship. SP and KP conceived and designed the research, performed statistical analysis, drafted the manuscript, and made critical revision of the manuscript for key intellectual content. All authors read and approved the final version of the manuscript and have agreed to the authorship and order of authorship for this manuscript.”
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.