
Abstract
Research on the psychological impact of war on affected populations is important for the planning and provision of interventions. However, most studies that address the effects of political violence have been restricted to Western countries, and even after six years of civil war in Syria, there has been no study addressing its psychological impact on the general population. The present study used an online survey to examine the level of psychological symptoms and correlates of distress in a sample of 387 subjects from different areas of Syria. We used t-tests to compare symptoms across zones with different levels of war activity, and multiple regression models to identify predictors of distress. Results indicate a high level of psychological distress indicative of psychopathology in all regions across the country. Rates were higher in areas with more intensive exposure (‘hot’ zones). Greater symptom severity was associated with living in a hot zone, female gender, older age, the number of potentially traumatic events, daily stressors, and (low) perceived feeling of safety; whereas social support, religiosity, and religious coping were associated with lower levels of symptoms. The elevated levels of mental health problems and direct relation between the level of exposure to violence and poorer mental health point to the need for mental health services. Reducing daily stressors and ensuring safety could contribute significantly to better mental health, although this does not replace the need for evidence-based psychotherapy. The planning and delivery of psychological interventions by NGOs should be informed by issues related to stigma, lack of understanding and acceptance of psychological care.
Introduction
Peaceful demonstrations against the ruling Baath party of President Bashar al-Assad, which started in March 2011 as the wave of the Arab Spring reached Syria, soon mushroomed into an armed conflict that has resulted in the worst humanitarian and refugee crisis in the world (UNHCR, 2016). Violent and brutal conflict in many parts of the country has claimed the lives of almost half a million people and continues to torment the population, with almost five million Syrians (of the estimated pre-war population of 23 million) fleeing the country and another 6.3 million becoming internally displaced (UNHCR, 2016). Apart from exposure to munitions, incendiary weapons, and indiscriminately destructive devices such as barrel bombs, Syrian individuals are constantly subjected to war-related traumatic experiences, such as imprisonment, torture, disappearances, forced displacement, landmines, etc. (Human Rights Watch, 2017)
Worldwide, many studies have investigated the impact of war on large populations (Cardozo et al., 2004; Charlson et al., 2016; De Jong, Komproe, & Van Ommeren, 2003; Murthy, 2007; Neria, Besser, Kiper, & Westphal, 2010; Pedersen, 2002; Priebe et al., 2010; Quosh, Eloul, & Ajlani, 2013), providing strong evidence of the association between war conditions and poor mental health. However, the main source of information about the impact of the war on mental health has been from studies on Syrian refugees. Naja, Aoun, Khoury, Abdallah, and Haddad (2016) found that 43.9% of Syrian refugees in Lebanon suffered from major depression, compared to a retrospectively estimated pre-war rate of only 6.5%. In a recent study, Kazour and colleagues (2017) estimated the lifetime prevalence of PTSD among Syrian refugees in Lebanon to be 35.4% and the point prevalence to be 27.2%. Similar results for PTSD were reported by Al-Ibraheem, Kira, Aljakoub, and Al-Ibraheem (2017), who found that 31.8% of a Syrian internally displaced person (IDP) sample met the criteria for an elevated PTSD symptomatology. These rates, obtained in samples of Syrian refugees and IDPs, are comparable to other refugee samples (Lindert, von Ehrenstein, Priebe, Mielck, & Brähler, 2009; Murthy, 2007) and are several-fold higher than the 2015 WHO Global Health Estimates for the general population worldwide (WHO, 2017).
Research on the mental health consequences of exposure to war has focused predominantly on its relation to trauma-related stress (McNeely et al., 2014). However, daily stressors and feelings of insecurity also have been postulated to have a major influence on mental health (Miller, Omidian, Rasmussen, Yaqubi, & Daudzai, 2008). Stressors such as lack of food and necessary daily supplements, lack of medical care, exposure to checkpoints, and other unpredictable events can have a tremendous effect on mental health. It follows that those who have not been directly exposed to war-related traumatic events, but who live under constant threat of trauma, may also be more vulnerable to mental health problems than those who feel less threatened (McNeely et al., 2014). Moreover, Miller and Rasmussen (2010) have suggested that intervention approaches in post-conflict settings, contrary to trauma-focused approaches that overemphasize the role of direct exposure to war, should address daily stressors, because these mediate the relation between exposure to war and mental health.
To investigate this finding in the Syrian context, we included a measure of the subjective feeling of safety in the online survey, in order to study its associations. Furthermore, the different level of, and intensity of exposure to, violence across different regions in Syria also needs to be considered. Analyses of areas with different levels of exposure have previously been utilized by Kazour and colleagues (2017), who found that refugees coming from Aleppo were twice as likely to present with PTSD as those who came from Homs.
In a conflict situation where severe human conditions prevail, there is a general expectation that everybody must be mentally ill. Barber (2013) refers to exaggerated expectations of widespread dysfunction as a universal response to adversity, although empirical evidence does not confirm such expectations. The study of resilience factors that allow individuals to successfully cope with severe conditions has gained much attention recently. Considering the importance of religion, spiritual life, family ties, and the collective social structure to Syrian society, both religious beliefs and practices used as coping mechanisms and social support should be major focuses of attention when trying to identify subpopulations associated with a higher or lower risk of poor mental health. Scholte and colleagues (2004) observed in a study conducted in Eastern Afghanistan that family support and religion were major sources of solace in the face of tragic events. Cardozo and colleagues (2004) found that engagement in religious and spiritual practices by Afghan people was associated with lower post-war psychiatric morbidity. Similarly, Berzengi, Berzenji, Kadim, Mustafa, and Jobson (2016) found that both positive and negative religious appraisals were inversely associated with severity of PTSD symptoms. The protective role played by religious coping (e.g., Hill & Pergament, 2003) and social support (Farhood & Dimassi, 2012; Maercker & Müller, 2004; Thoits, 2011; Wolf & Ratner, 1999) has also been scrutinized in many other studies. For further information on religiosity, stigma, and mental health services in the cultural context, please refer to Hassan and colleagues(2015, 2016).
In this study, we hypothesized that there is an increased prevalence of mental disorders in Syria in direct association to the intensity of the war conditions, mediated not only by exposure to war-related traumatic events, but also by other adversities like daily stressors and feelings of insecurity. In general, we expected a low acceptance of psychological intervention, but that greater severity of health conditions would be associated with greater acceptance. Furthermore, we hypothesized that both societal and family ties and religion would be important resources in aiding resilience among Syrians, as indicated by a positive association between social support and religious coping on mental health.
Methods
Sample and data collection
Due to the extreme difficulty of conducting personal interviews or paper-pencil based surveys under current conditions, mainly with regards to the safety of interviewers and interviewees, we decided to use an online survey. The encoded, secure, and anonymous nature of the online data collection reduced the risk of respondents and data collectors getting into trouble with local authorities. An active link that opened the online survey was disseminated via social networks and two local news websites. Additionally, a group of local activists, who as part of their jobs as reporters are trained regularly in matters of security and self-protection by the news agencies and research projects that recruit them, helped to randomly distribute the link via invitations on social networks within their respective localities.
Despite the obstacles, we tried to keep the sample size in each province approximately proportional to its population. Hence, 76.3% of the respondents in the sample reside in the most populated, so-called ‘mid-Syrian’ towns of Damascus, Rural Damascus, Aleppo, Idlib, and Hama, where more than 50% of the entire population lives (OCHA, 2014). The online survey consisted of 26 pages, with a total average processing time of M = 32.24 minutes, SD = 14.08. Only participants who filled in at least 10 pages were considered. To improve data quality, n = 16 cases were excluded due to extremely short processing time (less than 10 minutes for completers, which equates to an average of 23 seconds per page) and n = 7 cases were excluded for being underage. An informed consent, which appeared on the first page along with general information on the study, had to be affirmed in order to proceed. Those who showed suicide risk had the option to contact the research team and were also referred to an online therapy project that provides psychotherapy and counseling in Arabic. The study was approved by the ethics committee of the Technical University of Dresden (EK329082016).
Sample characteristics can be seen in Table 1. The sample consisted of N = 387 Syrian adults residing in Syria (Mage = 28.25, SD = 7.84, age range: 18–66, 69.7% male and 30.2% female). Half of the participants stated that they had migrated at least once during the last six years. The most frequently stated reasons for migration were escaping battles (55.3%), forced displacement (52.3%), and seeking a safer place (38.2%).
Sample demographics of N = 387 Syrian adult participants in the survey
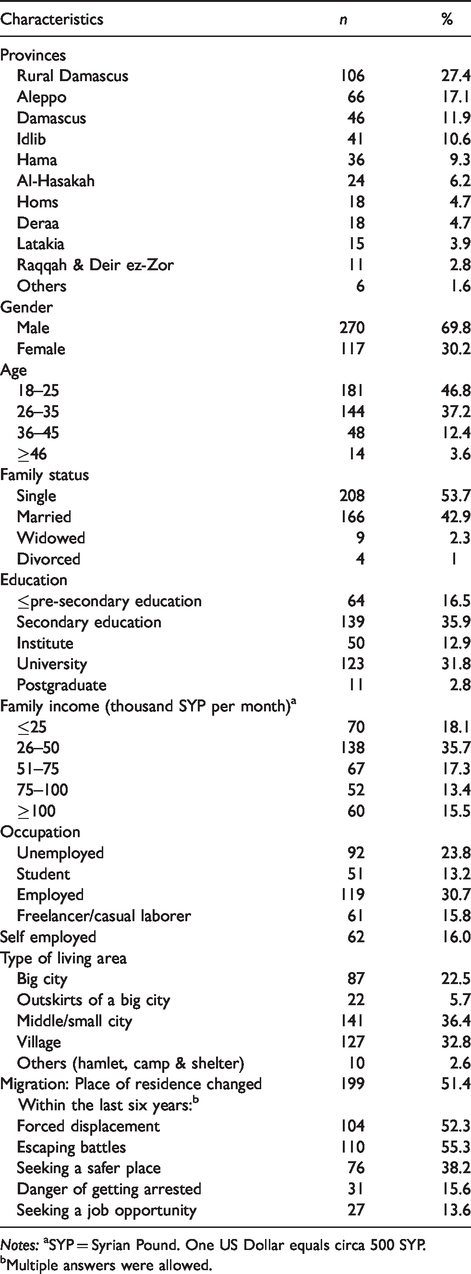
Notes: aSYP = Syrian Pound. One US Dollar equals circa 500 SYP.
bMultiple answers were allowed.
Measures
For this study, we used the Patient Health Questionnaire (Kroenke, Spitzer & Williams, 2001, 2002) for depression (PHQ-9) and somatization (PHQ-15), the PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 2013) for PTSD symptom severity, the Social Acknowledgment Questionnaire (SAQ; Maercker & Müller, 2004) for social support, the Brief Religious Coping questionnaire (RCOPE; Pargament, Feuille, & Burdzy, 2011) for positive and negative religious coping, the reduced version of the suicidality scale of the Mini International Neuropsychiatric Interview (MINI-Suicidality; Roaldset, Linaker, & Bjørkly, 2012; Sheehan et al., 1998) for suicide risk, the Afghan Daily Stressors Scale (ADSS; Miller et al., 2008), the EUROHIS-Quality of Life Index (QoL-8; Schmidt, Mühlan, & Power, 2006), the Duke University Religion Index (DUREL; Koenig & Büssing, 2010), and a modified list of potentially traumatic events from the Harvard Trauma Questionnaire-Iraqi Version (HTQ-IV; Shoeb, Weinstein & Mollica, 2007), in which items were reduced from 43 to 35. To account for acceptance of psychological intervention (API), five items rated from 0 (not at all) to 4 (absolutely) were chosen. The items addressed readiness among participants to benefit from psychiatric, psychopharmaceutical, psychotherapeutic, and telepsychological intervention. For the subjective feeling of safety (SFS), participants were asked to rate on a five-point scale ranging from 1 (never) to 5 (always) how often during the last month they had felt that their life, property, and the lives of family members were safe, and finally how often they had felt that their life was in danger (recoded). Separate factor analyses of SFS and API showed that all items loaded highly ≥.60 on the corresponding factor, explaining over 60% of the variance. Cronbach’s alpha of the scales in the current sample ranged from .67 to .91.
The survey was presented exclusively in Arabic. All originally English standardized questionnaires were translated and back translated by independent translators to detect and remove any discrepancies in meaning. A cultural expert reviewed the texts for cultural appropriateness and comprehensibility to the average participant.
Data analysis
Descriptive analyses
The data were analyzed using IBM-SPSS (version 23.0.0) (IBM, 2015). Drop-outs prior to the completion of the online survey yielded different Ns across the various analyses. We applied descriptive statistics to gain a general overview of the severity of the mental health burden on the population. A t-test was conducted, dividing the sample into hot and cold zones to identify significant differences between the two groups across the variables. This categorization is only a relative one and applies to the war situation at the time of data collection, from 20 August 2016 to 1 December 2016 (see Figure S1 in the supplementary files for a map of Syria displaying respective areas and territorial control as of August 2016). Additionally, potentially traumatic events and daily stressors were reported separately for cold and hot zones, so as to study differences in their type and intensity between the two zones.
Regression analyses
Three multiple linear regression analyses (using the enter method) were conducted to examine predictors. Demographic variables were entered in the first step. To account for the specific influence of the conflict situation, two zones that constitute opposite extremes were chosen: Idlib province was completely under opposition rule and therefore a conflict situation was prevalent in all parts of the territory. The safe zone included provinces that were experiencing comparatively less of the conflict, including Lattakia, Tartus, Suweidaa, and al-Hasakah. Perceived safety and daily stressors were entered in the second step, so as on the one hand to account for their contribution to psychopathology after controlling for demographics, and on the other to account for the contribution of traumatic events beyond daily stressors and perceived safety in the third step. Religiosity, in addition to its own importance as a predictor, was entered in the second step in order to partial out its confounding influence on social acknowledgment and on religious coping, which were then entered in the third step. The adjusted R2 was reported to reduce bias caused by the number of predictors.
Results
Descriptive results
The rates of mental health indicators in the current sample are significantly higher than in normal populations and are in line with rates in other war zones (Murthy, 2007). Descriptive statistics of the main measures are presented in Table 2. The mean score on PHQ-9 across the sample is M = 11.59, SD = 0.599. Almost half of the population (46.8%) were above the cut-off for PTSD. With 64% showing medium and 27.8% high somatic symptoms, the rates of somatization were higher than those for PTSD and depression. 27% of the participants were shown to display a low suicide risk, whereas 4.2% showed a medium and a further 4.2% a high risk. Although the present ADSS mean score of M = 49.13, SD = 9.75 is slightly lower than the mean score found in Afghanistan by Miller and colleagues(2008), there is a clear shift towards war-related stressors in Syria. Most of the top ten daily stressors are directly war-related, whereas in Afghanistan, family and socioeconomic stressors were dominant (see Table S1 in the supplementary files). The average number of potentially traumatic events in the sample amounted to M = 14.07, SD = 8.12 events. The absolute frequencies in the hot zones were higher than in the cold zones. The average score on SFS (M = 2.69, SD = 0.96) was low, indicating that individuals live under constant insecurity. The average quality of life score was expectedly low, at M = 3.24, SD = 0.62, which is significantly lower than the values found in the general populations of European countries (Schmidt, Muhlan, & Power, 2006). The low average score on API in the sample (M = 1.69, SD = 0.83) reflects stigmatized attitudes towards psychological interventions (Aloud & Rathur, 2009; Sewilam et al., 2015).
Descriptive statistics, cut-off values and t-test results
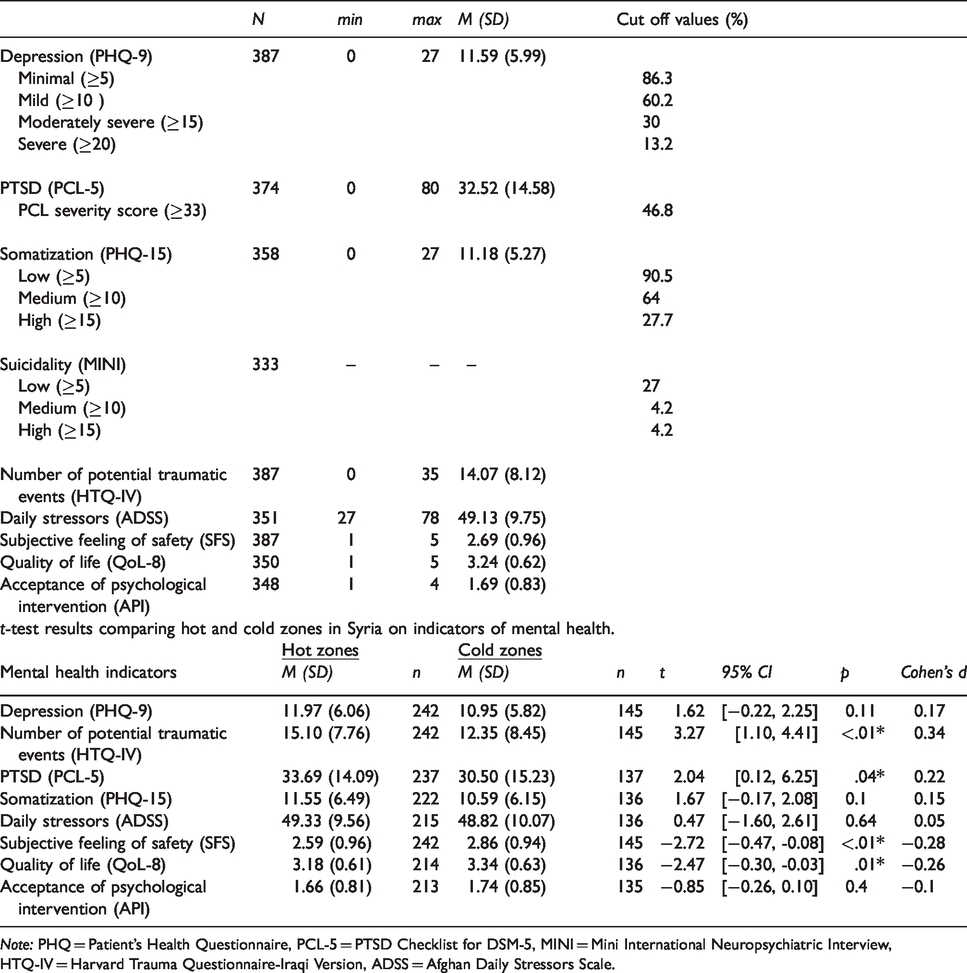
Note: PHQ = Patient's Health Questionnaire, PCL-5 = PTSD Checklist for DSM-5, MINI = Mini International Neuropsychiatric Interview, HTQ-IV = Harvard Trauma Questionnaire-Iraqi Version, ADSS = Afghan Daily Stressors Scale.
The t-test results in Table 2 showed a significant difference between hot and cold zones only in the number of potentially traumatic events (t(385) = 3.27, p < .01), PTSD (t(372) = 2.04, p < .05), SFS (t(385) = −2.72, p < .01) and quality of life (t(348) = −2.47, p < .01). The largest effect sizes were for the number of potentially traumatic events (d = 0.34), followed by subjective feeling of safety (d = −0.28).
The correlations shown in Table 3 demonstrate the expected pattern of high associations that reflect the comorbidity and overlap between PTSD, somatization, and depression. As postulated, these three indicators correlate negatively with quality of life, SFS, and social acknowledgment. Worth noting is the negative correlation of religiosity with API (r = −.31, p < .01), which may be due to the tendency for such communities to rely on religion (Aloud & Rathur, 2009), especially in light of the high positive correlation of religiosity to positive religious coping (r = .66, p < .01). Moderate positive correlations between API and mental health indicators is an interesting result, showing that although the general population is fairly skeptical about mental health assistance, increased symptom severity is associated with more willingness to benefit from psychological aid. Similar results were found in Jefee-Bahloul, Moustafa, Shebl, and Barkil-Oteo (2013).
Pearson correlations of the different indicators of mental health and their correlates

Note: PHQ = Patient Health Questionnaire, PCL-5 = PTSD Checklist for DSM-5, HTQ-IV = Harvard Trauma Questionnaire-Iraqi Version, ADSS = Afghan Daily Stressors Scale, SFS = Subjective Feelings of Safety, QoL = Quality of Life, SAQ = Social Acknowledgment Questionnaire, RCOPE = Positive and Negative Religious Coping, API = Acceptance of Psychological Intervention. DUREL-IR = Intrinsic Religiosity of the Duke University Religion Index.
Values ≥14 p < .01.
Values ≥11 p < .05.
Regression models
PTSD
Results of the three regression models are presented in Table 4. The proportion of explained variance ranged between 34% and 41%. Female gender, age, and level of education were significant predictors of PTSD. Participants located in Idlib province (β = .22, t(330) = 4.27, p < .01) seemed to be at a higher risk of developing PTSD compared to those in the safe zone (β = −.14, t(330) = −2.48, p < .05). As expected, daily stressors and perceived safety were highly predictive of PTSD, even after controlling for demographic variables and specific dangerous and safe zones. The number of potentially traumatic events indicated a significant contribution to PTSD, above and beyond daily stressors and perceived safety (β = −.20, t(330) = −4.0, p < .01). After partialling out the potential confounding influence of religiosity, social acknowledgment as victim also contributed significantly to PTSD (β = −.28, t(330) = −6.08, p < .01).
Multiple regression models of the outcome variables posttraumatic stress symptoms, depression, and somatization
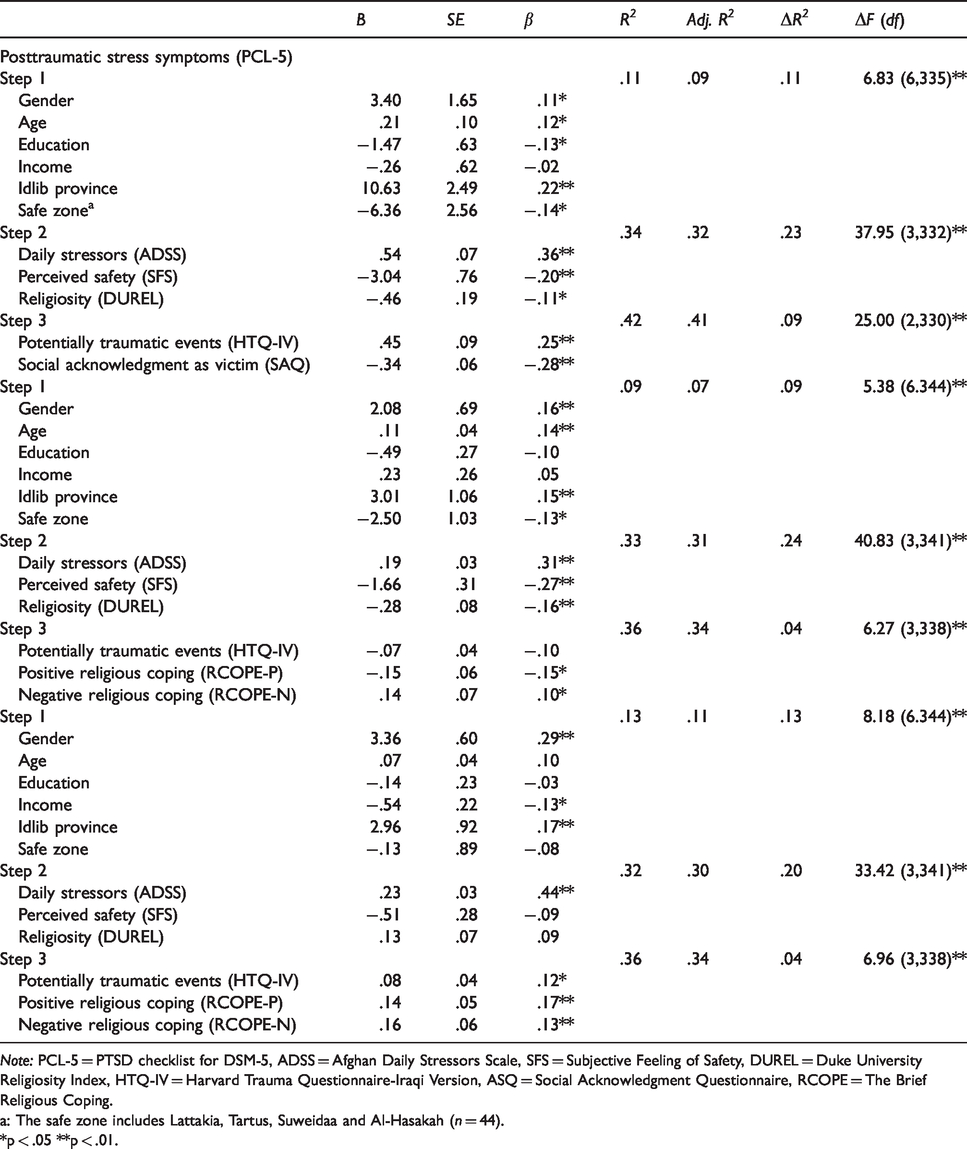
Note: PCL-5 = PTSD checklist for DSM-5, ADSS = Afghan Daily Stressors Scale, SFS = Subjective Feeling of Safety, DUREL = Duke University Religiosity Index, HTQ-IV = Harvard Trauma Questionnaire-Iraqi Version, ASQ = Social Acknowledgment Questionnaire, RCOPE = The Brief Religious Coping.
a: The safe zone includes Lattakia, Tartus, Suweidaa and Al-Hasakah (n = 44).
*p < .05 **p < .01.
Depression
As in the PTSD model, gender and age were significant predictors of depression. The standardized beta values for Idlib province (β = .15, t(330) = 2.86, p < .01) and the safe zone (β = −.13, t(330) = −2.43, p < .05) indicate a significant contribution of location. Again, daily stressors and perceived safety were significant predictors of depression. Together with religiosity, they explain 24% of the variance in depression (ΔF(3,341) = 40.83, p < .01). Negative and positive religious coping were both inversely related to depression.
Somatization
The only significant predictors of somatization among the demographic variables were female gender, income, and residence in Idlib province, thus demonstrating a different pattern than that found in the two previous models. The standardized beta coefficient of β = .44, t(337) = 8.59, p < .01 shows a strong association between daily stressors and somatization, whereas neither perceived safety nor religiosity were significant predictors. Contrary to their influence on depression, both positive and negative religious coping were positively associated with somatization as significant predictors.
Discussion
Studies of the Syrian population have previously depended exclusively on Syrian refugees abroad or internally displaced persons. This is the first study to investigate prevalence and predictors of psychopathology in the general population within Syria. Another important aspect of this study is that it was conducted during the war, thus providing a cross-sectional estimation of psychopathology, which will enable a comparison with these rates in studies that subsequently address the same subject in the post-war era.
The rates of psychological distress indicated by depression, PTSD, somatization, suicidality and quality of life suggest a significant elevation of mental health problems resulting from war conditions. The situation in hot zones is worse and the impact correspondingly higher. Furthermore, the results relating to daily stressors, the number of potentially traumatic events, and high rate of suicide risk are indicative of a highly distressed population in both the hot and cold zones. Further evidence for the direct positive relation between exposure to violence and mental health issues can be drawn from the significant contribution of Idlib province to PTSD, depression, and somatization. In addition to being completely outside of regime control (and because of this), Idlib has received a large number of IDPs from other opposition areas. This may have contributed to increased rates of psychopathology. Future studies in the area could focus on comparing IDPs with local groups, to account for the effect of displacement as one of the major negative outcomes of large-scale violence.
Among demographic variables, older age and female gender were consistently associated with a higher risk of psychological disorders. Specifically in Syria, where a functioning care system for the elderly did not exist, senior citizens had formerly relied upon informal social and physical support structures (Hassan et al., 2016), which are susceptible to collapse in war and crisis situations. In addition to being directly affected by war conditions in the same way that men are, women in Syria faced unique challenges that may have exacerbated a preexisting female vulnerability to depression and anxiety. These included becoming the sole care provider for the family when male family members migrated, were arrested, became disabled, or faced restricted ability to travel between different territories. Moreover, women felt more isolated due to the fear of unsafe conditions and restricted opportunities, and were at higher risk of sexual and gender-based violence (Hassan et al., 2016).
In the current study, the significant contribution of feelings of safety, daily stressors, and region of residence is evident throughout the analyses, which indicates a significant influence on overall psychopathology beyond direct exposure to war-related traumatic events. Pedersen (2002)refers to the problem of conflating the term “trauma” with PTSD in both public and scientific thought, when epidemiological studies show that only a fraction of those who are exposed to trauma develop a PTSD (Breslau, 1998; O’Brien, 1998). In the current study, the greatest risk for developing PTSD was observed among those who named imprisonment as their worst wartime experience. This is an expected result given the human rights conditions in Syrian prisons, which are considered among the worst in the world (Amnesty International, 2016). Nevertheless, the general lack of security and safety, generated by multiple factors such as, for example, living in an area targeted by air raids, can be expected to have a strong impact on vast proportions of the population (see Table S1). An overemphasis on the effects of direct exposure may tend to overlook cultural, contextual, and resilience factors (Barkil-Oteo et al., 2018), which are important in terms of research, public awareness, intervention designs, and treatment plans.
In the current study, although there was an average of 14 war-related traumatic events per person, less than half of the respondents scored above the cut-off value for PTSD. In the studies by Al-Ibrahim and colleagues(2017) and by Alpak and colleagues (2015), which used clinical interviews, lower rates of PTSD were found amongst Syrian IDPs and refugees. In addition, questionnaires are known to overestimate prevalence (Richardson, Frueh, & Acierno, 2010). We would therefore expect that in a study using clinical interviews, the percentage of people who fulfill the diagnostic criteria for the relevant disorders would be lower than the rates presented here. On the other hand, the response to traumatic events may tend towards somatic symptoms rather than merely intrusive memories and avoidance, especially when the adverse events, daily stressors and trauma conditions are still ongoing (Barkil-Oteo, et al., 2018). This, in addition to the clear association between somatization and PTSD, might explain the high rate of somatization in the current sample.
The current findings confirm the postulate that daily stressors contribute to psychopathology (Miller et al., 2008). However, whereas the contribution of daily stressors to symptom severity seems quite equal across PTSD, depression, and somatization, the contribution of the number of traumatic events was more specific to PTSD. Worth noting is that some of the most severe daily stressors in the current sample, such as the security situation in the country and roadblocks, were heavily war-related, unlike those found by Miller and colleagues (2008). Considering this overlap, we can say that the actual contribution of traumatic events is in fact greater. There is no doubt, as Miller and colleagues (2008) argue, that reducing daily stressors would enhance mental health in war-afflicted countries, due to the unspecified but significant influence of these daily stressors on mental health, even if, as Neuner (2010) points out, it would be an exaggeration to claim that the provision of humanitarian assistance to alleviate hardship and daily stressors alone can heal psychological disorders.
Although not in itself an indicator of mental health, the community’s acceptance of psychological assistance ought to be a key concept in epidemiological studies, because of its crucial implications for the planning and provision of psychological intervention. In a highly distressed population, a condition of psychological suffering becomes almost the norm (see Barkil-Oteo et al., 2018, for a cultural account of this tendency). It is therefore important that efforts at rebuilding and providing health care draw attention to the consequences of untreated mental illness and help individuals to recognize the differences between a normal state and a state of suffering. In a study by Jefee-Bahloul and colleagues(2013), comparatively low acceptance of psychological intervention was found, indicative of negative attitudes.
Many studies have pointed out the high rates of stigmatization towards mental illness (Coker, 2005; Shahrour & Rehmani, 2009; Al-Adawi et al., 2002; Struch et al., 2008; Altindag, Yanik, Ucok, Alptekin, & Ozkan, 2006). Worth noting is that, in the current study, as well as work by Jefee-Bahloul and colleagues(2013), an elevated level of distress was associated with higher acceptance of intervention. However, both studies addressed the readiness to benefit from such services, rather than just the attitude towards them. Therefore, this result may include those who are willing to visit a psychiatrist despite having negative attitudes towards psychological treatment. Moreover, as the correlations show, those who tend towards negative coping strategies have a generally higher acceptance, whereas those who accept and rely upon positive ways of coping have lower acceptance. Further evidence of this tendency is provided by the negative correlation between religiosity and API, which may be due to the role of religion in giving its own account of mental health, including meaning, coping, and explanatory models (Hassan et al., 2015). In particular, practitioners working with highly religious populations must be aware of these local explanatory models for mental health and rely on a non-stigmatizing attitude to help facilitate higher acceptance (Hassan et al., 2015)
Whereas (positive) religious coping has consistently been shown to play a protective role (Pargament, et al., 2011), evidence has not been consistent when studying religiosity. In the current sample, religiosity seemed to protect people against depression and PTSD but not against somatization, while Naja and colleagues(2016) found no meaningful association between religiosity and depression. In this regard, it is not clear which aspect of religious life plays a protective role. Religious people are expected to have a higher level of activation thanks to their religious engagements, such as praying, meeting other people in the community, or going to the mosque. It would be useful to ascertain whether this activation is responsible for the protective role of religiosity, or rather if other aspects of religious living are responsible, such as feeling part of a community, practical or emotional support from the community, or the role of religious coping. The multifaceted nature of religious belief may be responsible for the inconsistencies pertaining to its association to mental health. The measure we used here was the intrinsic religiosity subscale of DUREL. Despite being developed in a Western context, the three intrinsic religiosity items are neutral, in that they do not include any reference to a specific religion. The DUREL measure has also previously been used in the Arab context (Baroun, 2006; Koenig & Büssing, 2010). Arabic religiosity scales (Khalaf et al., 2014; Abdel-Khalek, 2017) that were developed later include or repeat the intrinsic items found in DUREL. However, these scales seem to amalgamate religious practice, religious coping, and religiosity, which we regard as distinct aspects that need to be treated separately when analyzing the influence of religious life on mental health.
In contrast to the results for depression, where negative religious coping increases symptoms and positive coping reduces them, both positive and negative religious coping were associated with higher somatization. Since religious coping, regardless of whether the content is positive or negative, contributes to more somatization symptoms, it could be seen as an expression or a result of suffering, overlaid with a religious content. In reference to the study conducted by Berzengi and colleagues (2016), who found an association between religious appraisals and trauma-related appraisals, the mechanisms underlying the association between religious coping and mental illness might be the same as for cognitive appraisals, except that in a religious society the content of these appraisals happens to be religious. Further studies dedicated to this issue are needed to scrutinize different aspects of religiosity and religious coping.
The postulated protective role of social acknowledgment as a victim against developing PTSD is evident in the current study. People who received more recognition and support were less likely to develop PTSD symptoms compared to those who received disapproval, denial, or less support. This speaks to the protective role of social support in relation to PTSD symptomatology (in line with Maercker, Povilonyte, Lianova, and Pöhlmannl, 2009), which many be independent of whether that support is provided in a religious context, as the present findings suggest.
Limitations
This study has major limitations. All data used in this study were collected using an online survey. Despite their advantages, online surveys exhibit the problem that the researcher cannot control when and where respondents fill in their data. However, the method offers several means of compensating for this and enhancing data quality, such as the exclusion of overly fast responses. Although self-filling questionnaires are important tools for gaining information on symptoms and their severity, the use of clinical standardized interviews is to be preferred where circumstances allow. The study did not compare subgroups, such as IDPs vs. locals, as our main objective was to account for mental health factors in the general population irrespective of displacement within the country. However, displacement is a major contributing factor to impairment in mental health, which needs to be considered. Areas under Islamic State control and under the Syrian regime control were especially underrepresented in this study. Nevertheless, until circumstances allow for a nationwide representative assessment, this study provides a good point of orientation and is, for the time being, the study with the broadest coverage. This being said, and setting aside the importance of representative studies, further cohort studies are needed to address populations that have been through unique circumstances with specific characteristics, such as former prisoners, cities under Islamic State control, East Aleppo residents during the escalations in 2016, residents in areas that were besieged over longer periods, and the victims of chemical weapons attacks. Finally, although we have present potential causal interpretations, all our data are cross-sectional, and longitudinal studies are needed to examine these associations and causal directions.
Conclusion
To our knowledge, this study is the first population-based estimation of the prevalence of psychopathology among Syrian residents after six years of civil war in Syria. In addition to covering key clinical symptomatology along with highly relevant social issues and aspects of daily life relevant to coping and reslience, such as religiosity and religious coping, social support, stigma, daily stressors, and perceived safety, the study provides insights that can assist policy making and the design and provision of mental health services.
The high rate of psychological distress, including but not limited to suicide risk, in the Syrian context is alarming and requires urgent intervention. Given the security situation in the country, which has included the targeting of health care facilities (Heisler, Baker, & McKay, 2015), and the high threshold for seeking face-to-face therapeutic aid due to stigmatization, online-based intervention (e.g., a suicide hotline, online psychotherapy) may be a useful method of overcoming political and geographical borders. Women and the elderly are two vulnerable groups that need specific protection. In order to improve the efficiency of health care provision, thereby overcoming the lack of trained therapists and other mental health resources, future research could engage in the development of screening methods to identify those who would already benefit sufficiently from basic humanitarian and therapeutic aid (stabilization, reducing daily stressors, and providing means of safety) and those who would need a more elaborative psychological intervention. Modified approaches to evidence-based interventions, such that they could be provided by local lay therapists, should be encouraged (e.g. Murray et al., 2014).
Footnotes
Acknowledgements
The authors received no funding for this work. We declare no competing interests.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.