
Abstract
Background:
One of the barriers to effective care in patients with depression is stigma associated with having a mental disorder, which also acts as a barrier to recovery and increases the disability.
Aims:
To study the stigma and disabilities experienced by the patients with depressive disorders seeking treatment in a tertiary care hospital
Methodology:
Fifty patients diagnosed to have depressive disorder as per ICD-10 were recruited by convenient sampling. To measure the stigma, the Discrimination and Stigma Scale -12 was applied. The severity of depression was determined by applying Hamilton Depression Rating Scale (HAMD). The disability was calculated by using WHO Disability Assessment Schedule 2.0
Results:
Fifty percentages of the participants reported unfair treatment and they experienced discrimination in at least one life domain. There was significant positive correlation between unfair treatment subscale of stigma and disability. Around one fourth of the participants reported to be treated unfairly by their own families. Seventy percent reported to have concealed their mental health problems, 54% have stopped themselves from having a close personal relationship and 32% didn’t apply for work in anticipating discrimination. Experienced and anticipated discrimination were significantly associated with concealing the mental health problem.
Conclusion:
Stigma due to having depression acts as a barrier to vocational & social integration and functional recovery. Concealment of the diagnosis of depression is itself barrier for help seeking and to receiving appropriate treatment. Small sample size and adopting the purposive sampling method are the limitations of the study.
Introduction
Worldwide, depression has been projected to be the second leading cause of disability by 2020. As per the World Mental Health Survey findings, the lifetime prevalence of major depression is 14.6% in high-income countries, 11.1% in the low- to middle- income countries and 9% in India (Bromet et al., 2011). The National Mental Health Survey of India found the lifetime prevalence of depression to be 5.2% and the current prevalence to be 2.7% (Gururaj et al., 2016).
However, it has been estimated that less than 50% of patients with depression are treated (Kohn et al., 2004). One of the barriers to effective care is stigma related to mental illness (Arnaez et al., 2019; Barney et al., 2006). Stigma is defined as a distinctive quality which an individual possess (or believed to possess) that conveys a characteristic, which is devalued in a social context (Crocker et al., 1998). Mental illness is associated with devaluation at many social situations including: workplace; healthcare settings; and personal relationships (King et al., 2007; Link et al., 1997). The general public also seems to dislike persons with mental illness more than persons with physical illness (Corrigan et al., 2003; Rüsch et al., 2005). There are three elements of stigma have been considered to present: (1) perceived stigma or one’s belief that other people hold negative attitudes towards him/her, (2) experienced stigma or incidents of discrimination related to a mental health problem and (3) self-stigma or assuming a stigmatized view of oneself (Brohan et al., 2010). The self stigma has been described as ‘the product of internalization of shame, blame, hopelessness, guilt and fear of discrimination due to having a mental illness’ (Corrigan, 1998). It has also been defined as a process of accepting lower expectations both for and by him or herself, either consciously or unconsciously (Caltaux, 2003). The research on stigma has mainly focused on measuring perceived stigma. A recent review of studies found that only one third measured self-stigma where as more than three fourth of studies measured of perceived stigma. More than half of the studies (52.6%) studied stigma on patients with severe mental illness and only 8.8% considered depression alone (Brohan et al., 2010). This suggests that there has been under-representation of depressive disorders in stigma research. There is also a limited focus on studying self-stigma in patients with psychiatric disorders. However, there is a growing interest in further examining the stigma related to common mental disorders (Alonso et al., 2009; Lasalvia et al., 2013; Rüsch et al., 2006).
A study on stigma found that participants with major depressive disorder experienced discrimination in more number of life areas than those with schizophrenia (Corker et al., 2015). Another study from Serbia assessed stigma in patients with depression using the discrimination and stigma scale. In this study, the participants reported that they had experienced discrimination in the field of family, friendship and holding a job. The participants reported a need to hide the mental health problems, which was stronger than the experiences being avoided and also higher than the overall score for experienced discrimination (Vidojević et al., 2015). In patients with social phobia and borderline personality disorder, self-stigma has been found to be associated with low self-esteem and other parameters of reduced psychological well-being (Rüsch et al., 2006). In patients with depression, self-stigma has been associated with poor quality of life (Yen et al., 2009), decreased self-esteem, reduction of morale (Ritsher & Phelan, 2004; Werner et al., 2009) and increased avoidance behaviors (Kanter et al., 2008). It has also been found to be associated with more severe form of depression (Kanter et al., 2008; Raguram et al., 1996; Rusch et al., 2008), more negative attitudes towards help seeking (Conner et al., 2010) and poor compliance to the treatment for depression (Fung et al., 2007).
Stigma has also been recognized as a barrier to recovery of the illness and thereby increases the disability (Struening et al., 2001). This may lead to poor treatment outcome and poor prognosis causing impairment in functioning and increase the disability. In India, nearly 80% of patients with mental illness had not received any treatment despite the presence of illness for more than a year. As per the national mental health survey of India (2016), stigma has been found to be one of the barriers to access mental health care. Mental disorders are associated with a considerable amount of stigma in Indian society, leading to neglect and marginalization (Gururaj et al., 2016).
There is active need to reduce stigma related to depression. Worldwide many initiative have been taken to curtail down stigma which include many activities such as education, training, media campaigns, contact with people suffering from mental illness, use of peer services, use of social media, legislative and policy change or combination of all these strategies. Notable public awareness campaign carried out at national levels were Defeat Depression Campaign and Changing Minds program in UK, “Beyondblue” project in Australia, The Like Minds, Like Mine project in New Zealand which aimed to create awareness and reduce stigma in general public related to stigma (Dumesnil & Verger, 2009). Depression: A Global Crisis was the theme for the World mental health day, 2012 to encourage governments and civil society around the world to address depression as a widespread illness. In 2017 it launched ‘Depression: let’s talk’ to end mental health stigma by encouraging the public to talk about depression. In India along with conventional strategies government has also taken various initiatives at program and policy level such as passing the Mental Healthcare Act 2017. Along with these initiatives there is also need to study stigma in person with depressive disorder to formulate further action plan to reduce it in the community.
To the best of our knowledge, from India there are very few studies on stigma in depressive disorder (Raguram et al., 1996; Sahoo et al., 2018). One was done around two decades back. These studies it did not assess how the stigma affects the various life domains for example, work, family and education of patients with depression and also level of disability was not assessed, which we tried to address in this study.
Aim
To study the stigma experienced by the patients with depressive disorders attending the psychiatry outpatient clinic of a tertiary care hospital
Methods
Patients with depressive disorders seeking treatment at the outpatient clinic of Department of Psychiatry of a tertiary care hospital of North India were recruited. Non-random, non-stratified sampling was done. A total of 50 patients aged 18 to 65 years with depressive episodes diagnosed as per ICD-10 criteria were included in this study (WHO, 1993). Patients with co-morbid physical illness which hinder their participation, organic brain syndromes, psychotic symptoms and other psychiatric illness (except tobacco dependence) and families with more than one mentally ill member were excluded from this study.
All the cases selected as per the inclusion and exclusion criteria were assessed clinically. The socio-demographic and clinical details of the patients were recorded. Hamilton Rating Scale for Depression (HRSD) was used to measure the depression severity (Hamilton, 1960). The self stigma and discrimination was assessed by Discrimination and Stigma Scale (DISC). This is an interviewer-delivered measure of experiences of discrimination (‘unfair treatment’) due to a diagnosis of a mental illness. Participants report experiences of discrimination across 32 areas about aspects of everyday life including work, marriage, parenting, housing, and leisure and religious activities, on a 4-point Likert scale (range 0–3; 0 = no, 1 = a little, 2 = moderate, and 3 = a lot). The sub scales are unfair treatment/experienced discrimination (items 1-21), stopping self/ anticipated discrimination (items 22–5), overcoming stigma/coping method to overcome stigma (items 26–27), and positive treatment (items 28–32). The DISC has good psychometric properties (Brohan et al., 2013). Original version of the scale was used and it was not translated and validated in local language. The DISC scale has been used in a multi-centric study (35 countries) in which India was a centre (Lasalvia et al., 2013). The disability was calculated by using WHO Disability Assessment Schedule 2.0 (WHODAS 2.0). This is used to assess disabilities across all diseases, including mental, neurological and addictive disorders. It assesses the disability on a 5-point Likert scale (range 1–5). It is applicable across cultures, in all adult populations and its development was based on an extensive cross-cultural study spanning 19 countries around the world with collaborators from India (Ustün et al., 2010). The 12-items interviewer version was used in this study. Approval from institute ethics committee was taken. For continuous variables, means and standard deviations were calculated and for categorical variables, frequencies and percentages were calculated. For comparisons, chi-square test, t-test and Mann-Whitney U test were used. Relationship between stigma and disability was studied by using Pearson product moment correlations and Spearman’s rank correlation.
Results
The total number of patients with depression studied was 50. The socio-demographic and clinical variables of patients are given in Table 1.
Socio-demographic and clinical characteristics.
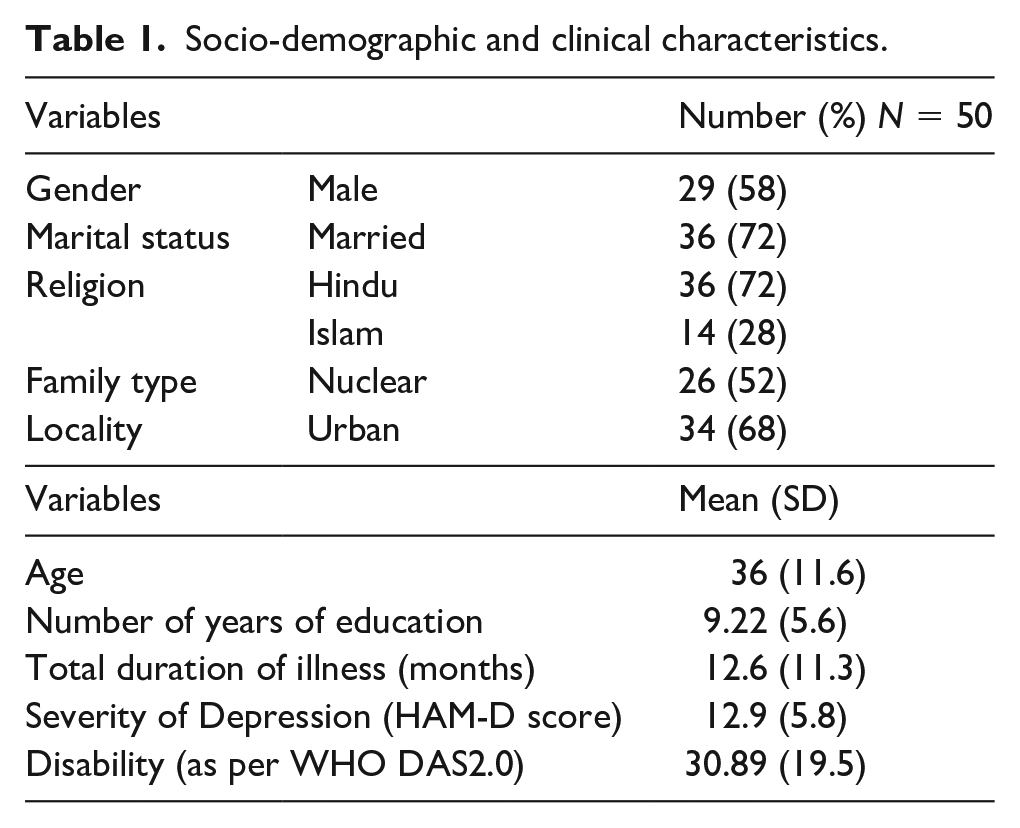
Out of the 50 patients, 14 (28%) were the only earning members of the family and 18 (36%) were the head of the family. Four patients (8%) had precipitating factors for their illness and seven (14%) had co-morbid physical illness. There was significant positive correlation between total duration of illness and severity of depression measured by HAM-D score (p = 0.017). There was also positive correlation between severity of depression (measured by HAM-D score) and disability (
The diagnoses of the patients are given in Table 2.
The diagnoses of patients.
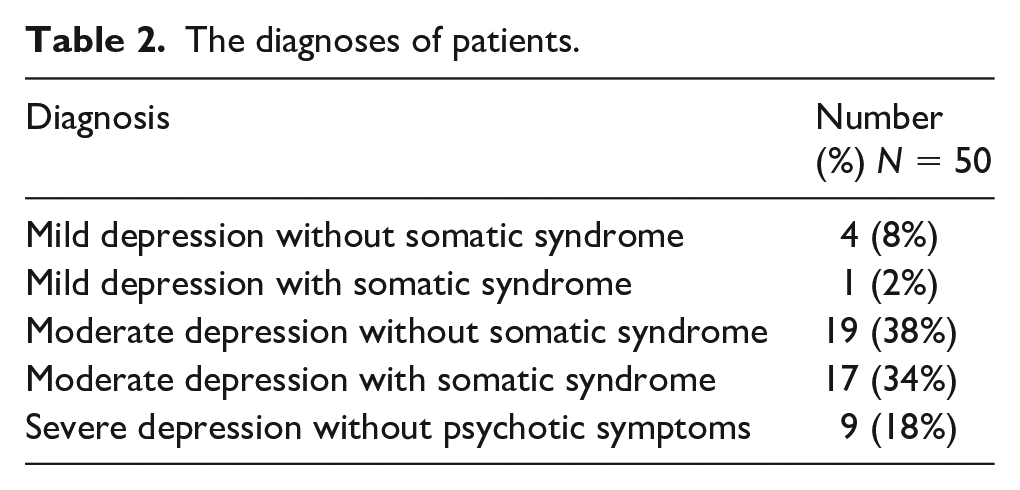
At the time of presentation to OPD, 21 (42%) patients were not on any treatment and rests were on treatment from outside, six (12%) patients were using tobacco and eight (16%) were using alcohol.
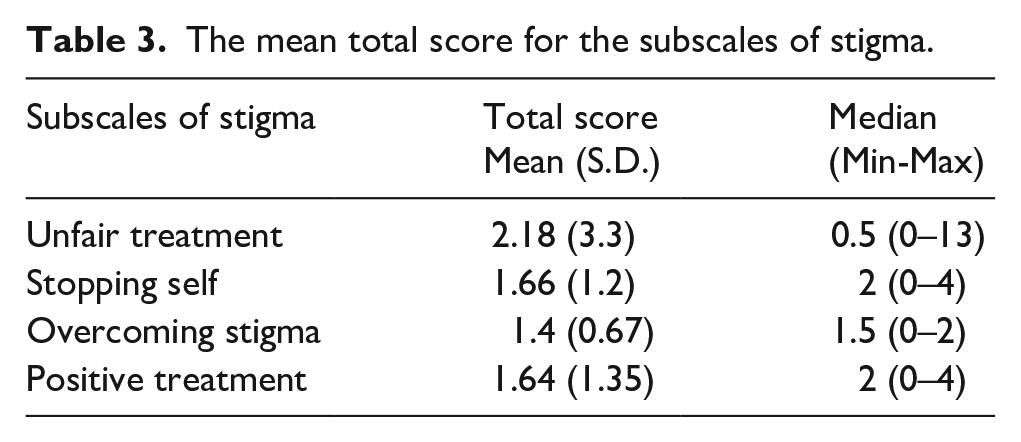
There was significant positive correlation between number of years of education and monthly income of the patient and family (p = 0.049), duration of unemployment and total duration of illness (p = 0.004), disability (p = 0.021) and severity of depression (p = 0.006). When the variables were compared between the mild, moderate and severe depression group using ANOVA, significant difference was found in the duration of treatment (F = 4.49; p = 0.017), in severity of depression measured by HAM D score (F = 4.343; p = 0.019) and in disabilities (F = 3.235; p = 0.048). After doing post hoc analysis, significant difference in duration of treatment was found between the moderate and severe depression group (p = 0.014) and in severity of depression measured by HAM D score between the mild and severe depression group (p = 0.015). The mean total score for the sub-scales of stigma are given in Table 3.
The mean total score for the subscales of stigma.
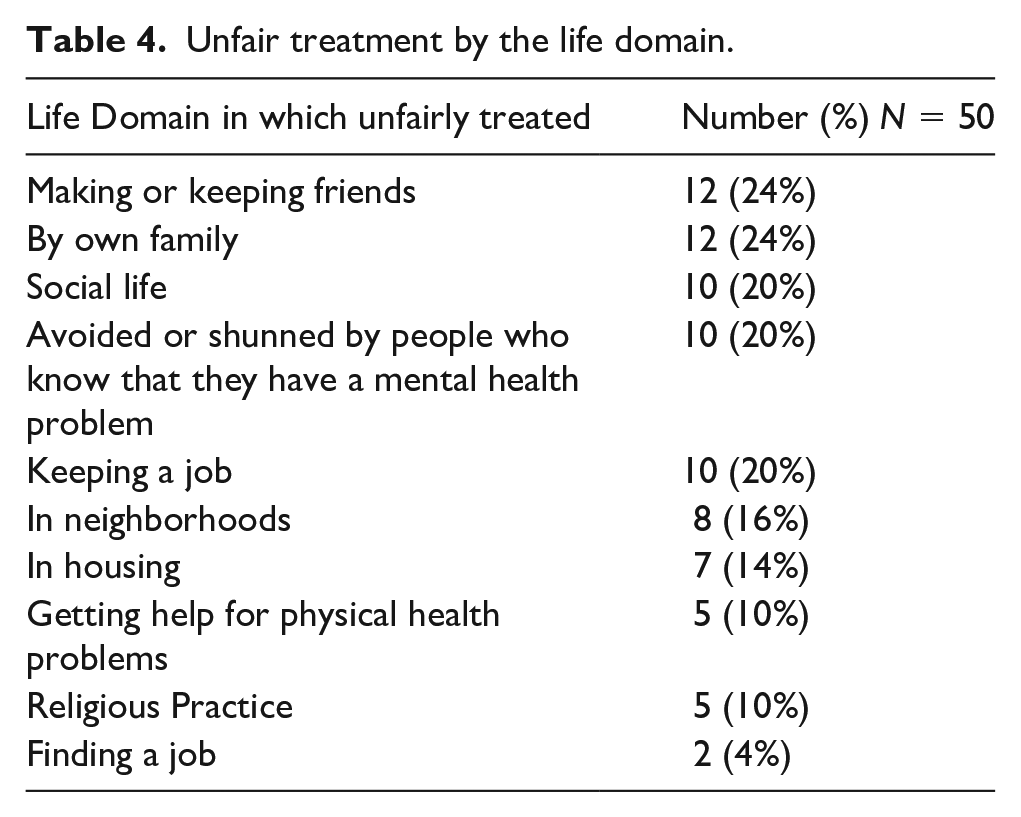
Fifty percentages of the participants reported unfair treatment in at least one life domain; 20% had reported that they had experienced unfair treatment in their social life. One fifth of patients reported that they had been avoided or alienated by people who are aware of their mental illness. Around one fourth (24%) of the participants reported to be treated unfairly by their own families, 24% reported that they had experienced discrimination in making or keeping friends and 10% also reported to experience discrimination when getting help for physical illness. The unfair treatment in various life domains to the participants has been given in Table 4.
Unfair treatment by the life domain.
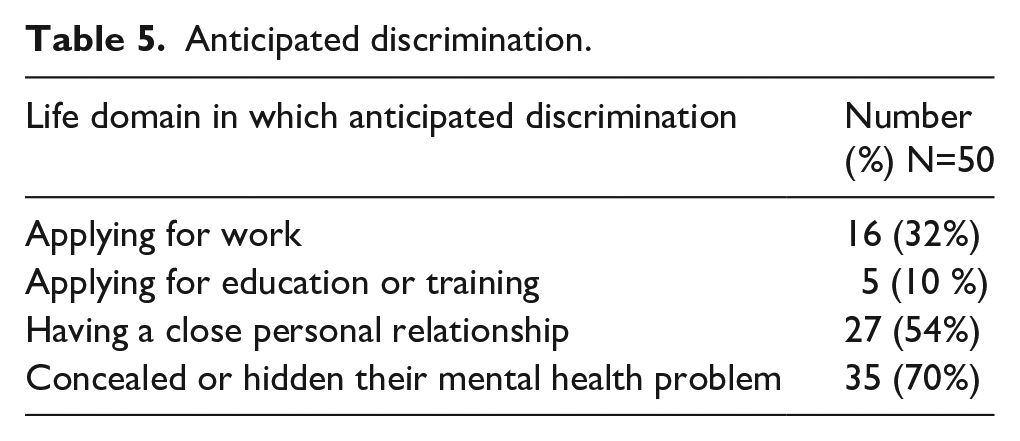
Seventy-six percentages of the participants reported anticipated discrimination and stopped themselves in at least one life domain. Seventy percent of the participants had concealed their mental health problems to others. Fifty four percent had stopped themselves from having a close personal relationship and 32% didn’t apply for work anticipating discrimination. The anticipated discrimination in various life domains has been given in Table 5.
Anticipated discrimination.
There is significant difference in medication status at the time of presentation between the group who has concealed or revealed the diagnosis (p = 0.033). Those who had reported that they had concealed the diagnosis are more likely to be drug naive at the time of presentation. The group that concealed their diagnosis had higher unfair treatment (mean total score 2.86 [SD 3.75] vs 0.6 [1.2]; Mann-Whitney p = 0・011) and anticipated discrimination (mean total score 2.29 [0・82] vs 0・20 [0.41]; Mann-Whitney p < 0.001) than did those who disclosed their diagnosis. In the work domain, 38% of the participants anticipated discrimination despite 52% of these individuals not having experienced discrimination. The experienced and anticipated discrimination were significantly associated in the ‘work’ domain (χ2 = 14.34;
Relation between experienced and anticipated discrimination in ‘work’ domain.*
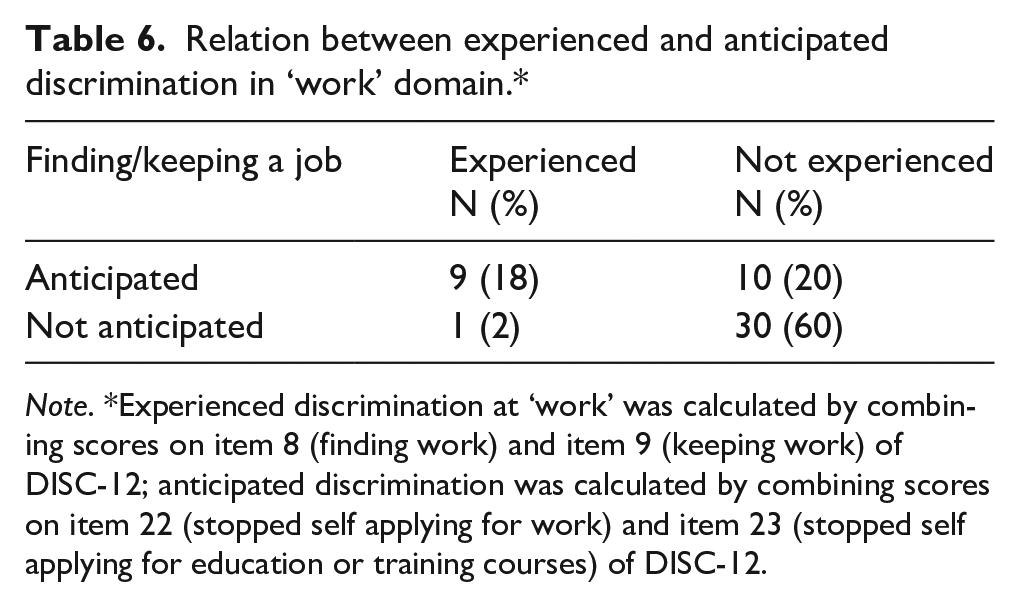
Note. *Experienced discrimination at ‘work’ was calculated by combining scores on item 8 (finding work) and item 9 (keeping work) of DISC-12; anticipated discrimination was calculated by combining scores on item 22 (stopped self applying for work) and item 23 (stopped self applying for education or training courses) of DISC-12.
The regression analysis shows that patients who experienced most unfair treatment were those who had longer duration of illness (β = 0.347; p = 0.022), more disability (β = 0.535; p = 0.041), history of alcohol use (β = −0.408; p = 0.006) and had lesser positive treatment (β= −0.473; p = 0.002). Overall, these variables accounted for 51.6 % of the variance. Table 7 shows the negative binomial regression models for experienced discrimination with the independent variables.
Regression models for unfair treatment.
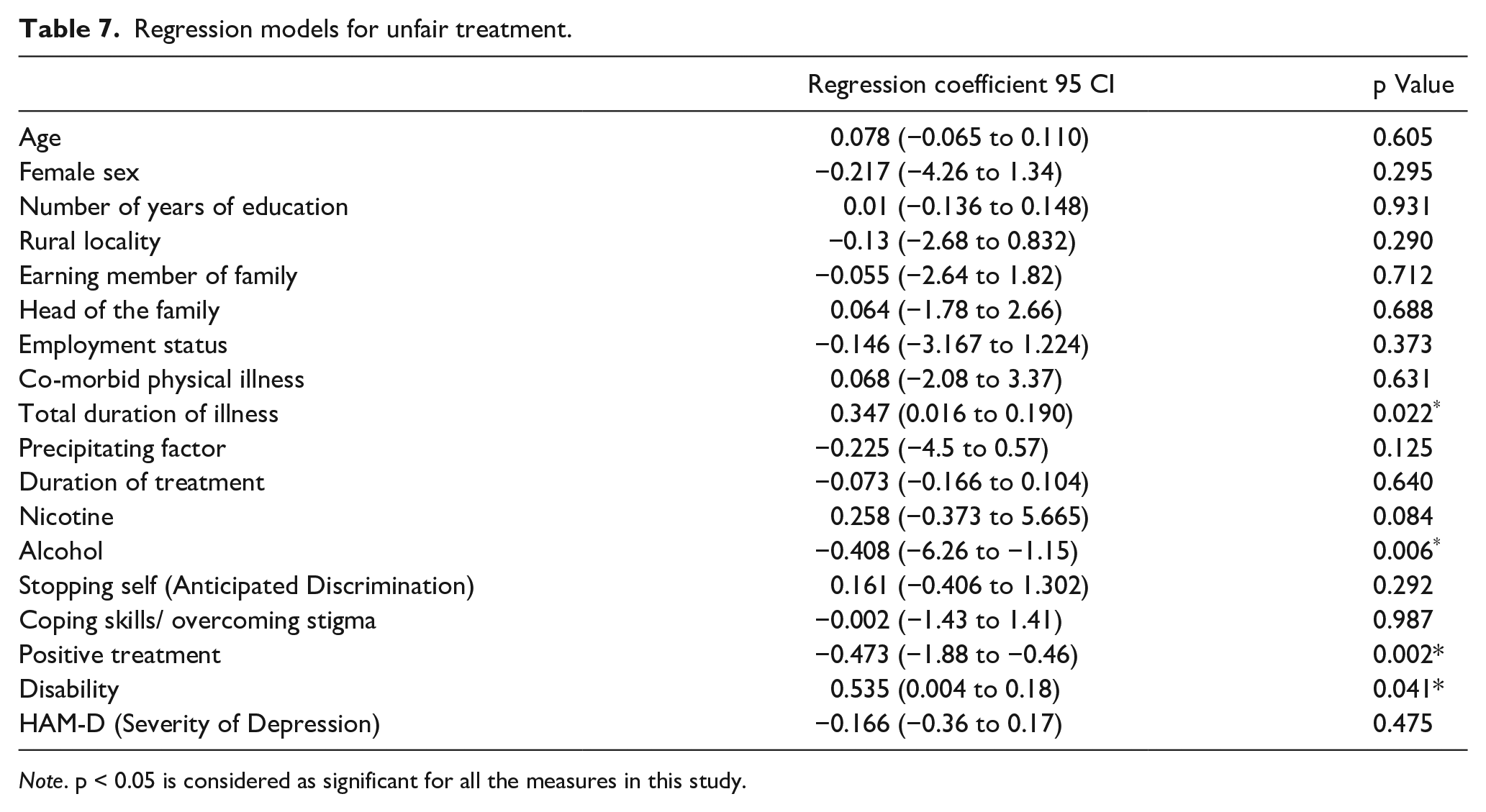
Note. p < 0.05 is considered as significant for all the measures in this study.
Ninety percentages of participants used their coping strategy to overcome stigma. Fifty-six percentages of participants reported to have used their personal skills or abilities to cope with discrimination due to mental illness and 84% of the participants had made friendship with people who did not use mental health services. Forty percentages used one coping strategy and 50% used 2 coping strategies to overcome stigma and discrimination.
However, in this sample 66% reported to be positively treated by their families due to the illness.
There was significant positive correlation between monthly income of family and anticipated discrimination (p = 0.026), unfair treatment and anticipated discrimination (p = 0.001), unfair treatment and coping strategies used to overcome stigma (p = 0.028) and anticipated discrimination and coping strategies used to overcome stigma (
Discussion
In this study, we have measured self-stigma in patients with depressive disorders. We also measured the disability in these groups of patients, and the correlation between the self stigma and disability. To the best of our knowledge, this is the first study of its kind. Though there are some studies on stigma research, most of them are on perceived stigma and on experienced stigma (Koschorke et al., 2017) and a very limited focus on measuring self-stigma, and also most studies were on severe mental disorder (Grover et al., 2017; Pal et al., 2017). One of the strengths of our study is that the participants were clinically assessed by a consultant psychiatrist in face to face manner for making a diagnosis, assessment of disabilities and application of scale to measure stigma. In some of the other studies on stigma in depression, assessment was done by research personnel in community (Alonso et al., 2009; Lasalvia et al., 2013) or the diagnosis was self reported by the participants and only online assessment/communication was done (Brohan et al., 2010).
Fifty percentages of the participants experiencing discrimination in at least one life domain and 76% of the participants anticipating discrimination in at least one life domain suggestive of high self stigma in Indian patients with depression. A study from Europe found the subjects with first episode depression faced more discrimination than patients with schizophrenia in a greater number of life areas (meeting neighbors, dating, education, marriage, religious activities, physical health and acting as a parent). The authors of this study postulated that such high rates of discrimination in patients with depression as compared to subjects with schizophrenia could possibly be due to attitude of general public toward depression as being a less serious illness than schizophrenia that requires less care and help. Due to this, people may be less supportive toward subjects with depression, and hence, they feel being discriminated (Corker et al., 2015). Besides this an Indian study hypothesizes that, presence of insight and universal feeling of distress in patients with depression can cause increased stigma and the authors proposed to evaluate these variables among patients with various psychiatric disorders in the future (Sahoo et al., 2018). However, in the study by Lasalvia et al. (2013), 79% of the participants reported to have experienced discrimination in at least one life domain, most commonly the unfair treatment was by family which was 40%. In our study, the unfair treatment reported by the family was only 24% and 66% of the participants reported to be positively treated by their families due to their illness. This suggests that Indian families are less likely to treat unfairly with a family member with depression compared to global pattern. It has been highlighted that in India, family plays an important role in the caregiving process of the patients with psychiatric illness and provides support to the diseased family member (Chadda, 2014; Chakrabarti, 2016). In a study conducted by Sahoo et al. (2018) from India on stigma in first episode depression using Internalized stigma of mental illness scale (ISMI), found the discrimination experience to be 42% and the stereotype endorsement to be 62%. This value can be comparable with the finding of our study of 50% of participants experiencing discrimination.
In our study, 70% of the participants reported that they had concealed their mental health problems to others in anticipating discrimination. This is similar (71%) to the previous study by Lasalvia et al. (2013) and by Vidojević et al. (2015) (67.3%). In our study, 42% of participants were drug naïve at the time of presentation and the participants who had reported that they had concealed their diagnosis they are more likely to be drug naive at the time of presentation. They experienced higher unfair treatment and anticipated discrimination than those who disclosed their diagnosis. These findings suggest that, experienced and anticipated discrimination can affect concealing or disclosing the mental health problems which in turn can affect the treatment seeking behavior. A recent study has found that stigma is strongly linked to barriers to mental health care in patients with depression (Arnaez et al., 2019).
Raguram et al. (1996) also found that more somatization was associated with less stigma scores. Patients viewed depressive, but not somatic, symptoms as unfavorable within society. Somatic symptoms were considered to be less stigmatizing since they resembled physical illness that most people could expect to have from time to time which is culturally acceptable. As we did not assess the somatization level, we cannot comment on this aspect. We found that participants who experienced most unfair treatment were those who had longer duration of illness (β = 0.347; p = 0.022). One previously conducted study from India also found that longer duration of depressive episode was associated with higher stigma (Sahoo et al., 2018).
In our study, 54% of participants had stopped themselves from having a close personal relationship and 32% had anticipated discrimination while applying for work and didn’t apply. This figure is more than the earlier study by Lasalvia et al. (2013) which was 37% (stopped themselves from having a close personal relationship) and 25% (stopped themselves from applying for work). This could be due to the cultural differences of the participants or clinical characteristics of the participants included. In the study by Lasalvia et al. (2013), they have included patients with recurrent depressive disorders in addition to patients with major depressive disorder and also their study participants had history of inpatient hospitalization. We include only patients with first episode depression from outpatient facility. However, in another study from Serbia 59.6% of participants stopped themselves from looking for a close personal relationship (Vidojević et al., 2015) which is similar to the findings of our study (54%). In our study, we found that in the work domain the anticipated discrimination is more than the experienced discrimination which is also similar to the study by Vidojević et al. (2015).
However, in spite of facing and anticipating discrimination 90% of the participants used their coping strategies to overcome stigma. The use of coping strategies is found to be positively correlated with the unfair treatment (p = 0.028) and anticipated discrimination (
There was significant positive correlation between the unfair treatment sub-scale of stigma and severity of depression measured by HAM-D score (p = 0.03). There was also significant positive correlation between unfair treatment subscale of stigma and disability (p = 0.03) and severity of depression and disability (
There were some limitations in the present study which should be kept in mind while interpreting the results. First, the study had small sample size and it includes only treatment seeking population. Studies which have assessed stigma in psychiatric disorders (Raguram et al., 1996; Sahoo et al., 2018) had larger sample size as compared to our study. Second limitation pertains to impact of depression severity. At the time of assessment participants in the study were not in remission thus the severity of depressive psychopathology and associated cognitive distortion could have an impact on self perceived stigma and discrimination. Lastly, there could be selection bias as purposive sampling was used. This can reduce the generalizability of the findings.
Conclusion
In people with mental illness, the distress, dysfunction and disability faced are due to the mental illness per se and also due to its associated stigma. Stigma causes a barrier to treatment seeking and again causes a barrier to recovery. These feelings of stigma and discrimination are endorsed and internalized by the patients also. Our study shows that stigma is higher among persons who are more severely ill and ill for a longer period and less in educated people. Thus, early and effective treatment expected to reduce self-stigma.
Footnotes
Acknowledgements
We acknowledge the patients who consented to be participate in this study
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an intramural research grant from AIIMS, New Delhi