
Abstract
Background:
To understand if supported accommodations (SA) are promoting the recovery of people with serious mental disorders, quality of life (QoL) is an important outcome. This study aimed to analyse the association between QoL and experiences of care in general and to identify specific experiences of care that are associated with QoL in users of SA.
Methods:
A random sample of users of 42 SA was interviewed to obtain standardized measures of QoL and personal experiences of care. The sample was also characterized according to sociodemographic and clinical aspects. Linear regressions models analysed the association between QoL and experiences of care, adjusting for potential confounders. Results include estimated regression coefficients, corresponding 95% confidence intervals and p-values.
Results:
The number of users interviewed was 272. The median QoL was 4.9 (2.3–6.8) out of 7. Although 84.9% of users were satisfied with the care received, only 16.2% felt involved in their treatment. Feeling safe (β = .73; 95% CI [0.22–1.24], p = .006) and having privacy (β = .42; 95% CI [0.09–0.75], p = .014) influenced QoL. Involvement in care (β = .44; 95% CI [0.13–0.74], p = .006), safety and privacy (β = .72; 95% CI [0.44–0.99], p = 8.38e-07) and user-professional relationship (β = .42; 95% CI [0.14–0.69], p = .003) were also associated with QoL.
Conclusions:
Feeling safe, having privacy, feeling involved in care and having good user-professional relationships influence the QoL of users. These findings have implications from the political and economic level to the organizational and individual levels.
Introduction
People with serious mental disorders (SMD) may present complex social, economic and health needs and are especially vulnerable to exploitation and self-neglect (Asher et al., 2017; Killaspy, Priebe, et al., 2016). Housing, in particular, is a frequent need for people with SMD due to discrimination, poverty, and lack of affordable housing or adequate support (Farkas & Coe, 2019; Kyle & Dunn, 2008; Watson et al., 2019).
Supported accommodations (SA) provide residential support, ideally in the community, for people with SMD and complex needs (McPherson et al., 2018). They were initially developed in the context of deinstitutionalization, to help institutionalized people with mental disorders to go back to living in the community, focusing primarily on the development of living skills (Parker et al., 2019). These services developed unevenly across the globe, both within and between countries, and evolved into different types, generally ranging from high-support accommodations with 24-hour on-site staff to accommodations where staff is not permanently on-site, visiting only according to individual needs (mobile or outreach support) (McPherson et al., 2018). In Portugal, SA were first regulated in 1998 (decree 407/98), which led to their exponential development in the country (Despacho conjunto no. 407/98, 8328, 1998). In 2017, the Mental Health Integrated Continued Care network (‘Cuidados Continuados Integrados de Saúde Mental’) known as CCISM, was implemented, with the aim, among others, of transforming and improving the quality of care provided by the existing SA working under the previous decree and further developing new ones (Despacho no. 1269/2017, 2443, 2017). Currently, the majority of SA in the country are medium- to high-support accommodations with at least 12-hour on-site staff (Ministério do Trabalho, Solidariedade e Segurança Social [MTSSS], 2020). SA working under the decree 407/98 encompass 139 places and SA working under the CCISM 124 places (MTSSS, 2020). Many more SA operate under no agreement, but the total number of places is not publicly disclosed.
The disparity in services and the lack of a uniform terminology have hindered investigation and thorough comprehension of the field (Barbato et al., 2020; Krotofil et al., 2018). Most studies have focused on the effectiveness of SA, namely in terms of housing stability or progression to more independent living settings, decrease in hospitalization or improvements in social functioning, and, less often, in quality of life (Aubry et al., 2016; Killaspy et al., 2022; Killaspy, Marston, et al., 2016; Leff et al., 2009; Lora et al., 2004). However, few studies have focused on which characteristics of care predict quality of life (QoL) and other rehabilitation outcomes (Vita & Barlati, 2019).
This is an important gap, as QoL is a fundamental outcome to better understand if the SA is supporting people in their recovery process (Harrison et al., 2020). Furthermore, it provides indication on the satisfaction of users with care, and is an independent predictor of relapse in schizophrenia (Boyer et al., 2013; Harrison et al., 2020).
Among the few studies focusing on the characteristics of care associated with QoL, Baker and Douglas (1990) found an association with appropriateness of housing to users’ needs, Srebnik et al. (1995) with greater amount of choice, and Nelson et al. (2007) with the quality of housing, and with having control and choice over housing and support. However, some of these focused only on people living in independent housing with mobile support or with a previous history of homelessness. In addition, a limited number of characteristics of care were studied, and, in some, unstandardized measures were used.
The DEMoBinc study was an important research project in the field of supported accommodation.(Killaspy et al., 2009) This was a European study involving 10 countries from different socioeconomic and political backgrounds, which allowed for the development of the first standardized instrument to assess the quality of care for people with longer term mental health problems in psychiatric and social care facilities – the Quality Indicator for Rehabilitative Care (QuIRC). Within this study, and using the QuIRC, Killaspy et al. (2011, 2013) and Cardoso et al. (2016) explored which domains of quality of care were associated with users’ QoL in England and Portugal, respectively. Killaspy et al. found an association with the Living Environment and Self-Management and Autonomy domains, while Cardoso et al. found an association with the Therapeutic Environment domain. Different sample characteristics, namely age, diagnosis and social functioning, or different SA characteristics, such as location, may explain these differences.
Quality of care using the QuIRC is assessed by professionals. However, studying the characteristics of care as assessed by users is fundamental to better comprehend their preferences, and analysing their association with QoL may be helpful in understanding how SA are supporting people in their recovery process (Bengtsson-Tops et al., 2014; Harrison et al., 2020).
Most studies that focused on the users’ perspectives on characteristics of care used a qualitative methodology, and found that users valued choice and control, accessible and flexible support, less restrictions, supportive relationships with professionals, being respected, cleanliness of spaces, privacy, security, access to transportation and community amenities and stability (Barnes et al., 2022; Bengtsson-Tops et al., 2014; Brolin et al., 2015; Gonzalez & Andvig, 2015; Kirsh et al., 2011; Krotofil et al., 2018; Nelson et al., 2003; Watson et al., 2019). However, while qualitative studies may suggest what is important to users’ QoL and recovery, they do not allow the inclusion of larger and randomized samples nor the study of relevant statistically significant associations, such as the association with QoL. Moreover, they are seldom taken into account by care providers or policy makers (Krotofil et al., 2018).
Taking these facts into consideration, the authors of this paper decided to continue the work of Cardoso et al. with a different approach, and specifically focused on the impact the SA users’ perception of their experiences of care may have on QoL. In addition, the authors also intended to analyse whether this impact was different according to SA’s location or type of support.
Methods
Study design and selection of participants
The present study analysed data collected by the study of Cardoso et al. (2016), which was conducted in 2012 on SA for people with SMD in Portugal. Its methods are described elsewhere (25). In summary, all the SA with high or medium support levels (i.e., at least 12 hours on-site staff support per day) were invited to participate. SA that provided specialist care only (such as dementia, other severe cognitive impairment or intellectual disability specialized units) and SA with fewer than six residents were excluded. In SA with up to 10 users, all were invited to participate, while a randomized sample of ten users was obtained for SA with more than 10 users. Thirty-minute face-to-face interviews with the users who accepted to participate were conducted. Additional descriptive data on the service users’ sociodemographic and clinical characteristics was provided by the unit staff prior to the interviews. Data was collected from both staff and users between March and July 2012. The users’ interviews were conducted by experienced professionals trained for the purpose. In total, 42 SA participated in the study. The final sample consisted of 278 persons.
Dependent variable
QoL was the dependent variable and was collected using the Manchester Short Assessment of Quality of Life (MANSA) (Priebe et al., 1999). The MANSA consists of three sections. The first section considers stable personal details such as date of birth, gender, ethnic origin and diagnosis. The second section includes personal details that may change over time such as education, employment status, income, state benefits, living situation, other people whom the patient lives with and type of residence. The third section encompasses 16 questions to be asked every time the MANSA is applied. Four of those are objective (to be answered with yes or no) and 12 are subjective. The objective questions assess the existence of a close friend, number of contacts with friends per week, existence of an accusation of a crime and having suffered physical violence. The subjective questions address perceived satisfaction with life as a whole or with certain domains such as employment, financial situation, number and quality of friendships, leisure activities, accommodation, personal safety, people that the user lives with (or living alone), sex life, relationship with family, physical health and mental health. Satisfaction is rated on a 7-point scale (higher scores correspond to higher satisfaction) for each of the 12 subjective domains. The final score may be calculated either using the mean of the 12 individual item scores or by domain (varying from 1 to 7, total score from 12 to 84), with higher scores corresponding to higher QoL. For this study, the global score was used. Participants who failed to answer at least one of the subjective questions were excluded from the analysis.
Independent variables
Data on the users’ experiences of care was collected using the Your Treatment and Care (YTC) questionnaire (Figure 1), which includes 25 items related to care, classified as either being present or not, thus providing a total score between 0 and 25 (Webb et al., 2000). Higher scores correspond to better experiences. For this study, total score and scores for each individual item were used. Participants who failed to answer at least one of the items were excluded from the total score analysis. Some items were aggregated to create four categories: involvement in care, respect and acceptance, safety and privacy and user-professional relationship (Figure 1). A category was classified as being present if all its items were rated ‘yes’, and not present if any item was rated ‘no’. All other situations were considered missing values.
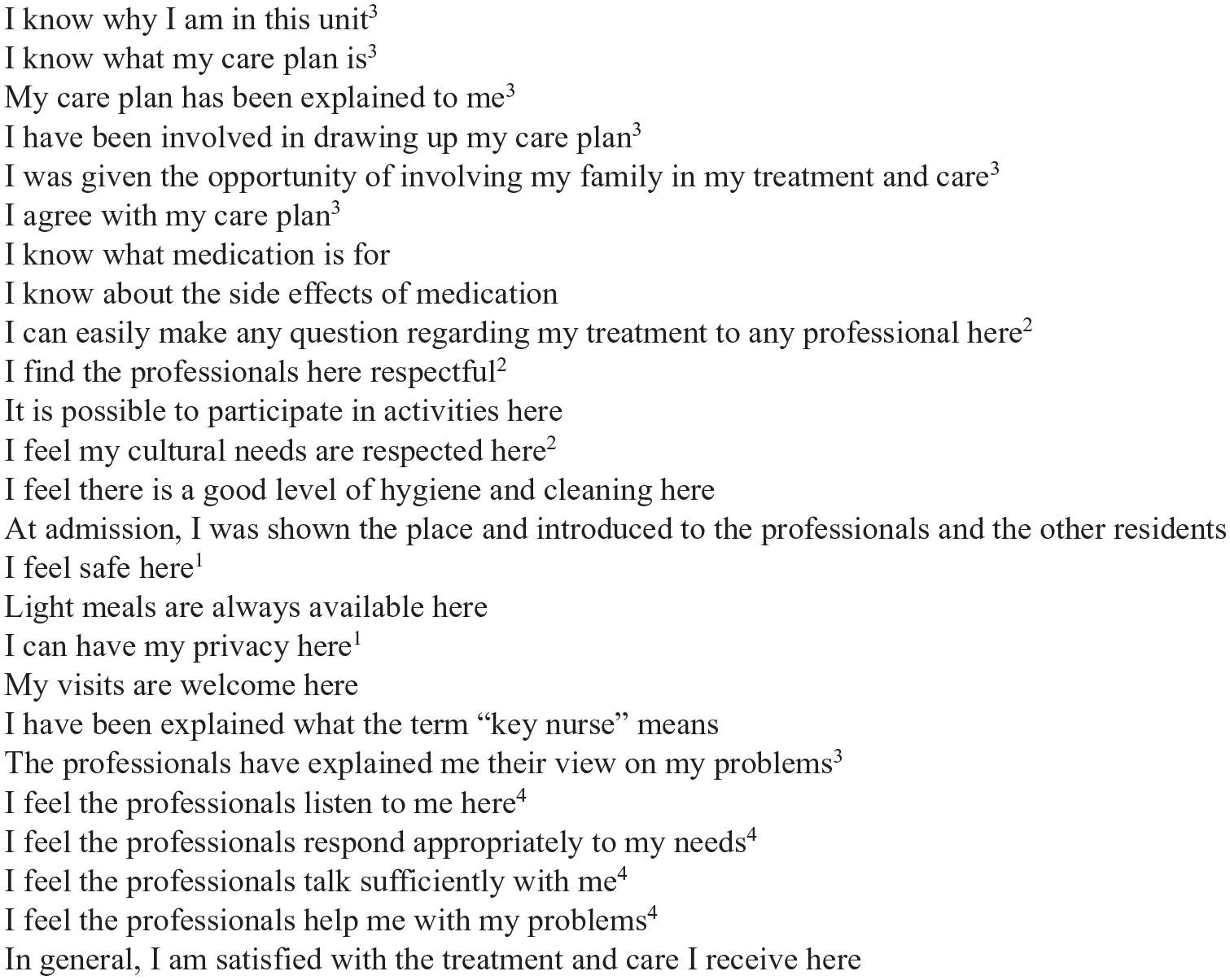
Your treatment and care items (Items included in the category: 1‘safety and privacy’, 2‘Respect and acceptance’, 3‘Involvement in care’, 4‘User-professional relationship’).
Covariates
Sociodemographic characteristics of users were obtained using the first sections of MANSA (Priebe et al., 1999). These included gender (male/female), age (years), education (years), work situation (regular employment, protected employment, student, unemployed, retired, other) and income (euros/month). Data on clinical characteristics such as diagnosis (schizophrenia or schizoaffective disorders/other) and length of stay (years) was provided by the unit staff. Data on functioning was assessed by the interviewer using the Global Assessment of Functioning (GAF), which rates the person’s overall symptoms and functioning on a scale between 1 and 100, with lower scores corresponding to greater disability (Cardoso et al., 2016). Data on location (community or intra-institutional) and type of support (24 hours/day or 12–24 hours/day) was provided by the staff.
Statistical analysis
Absolute and relative frequencies were used for qualitative data, mean and standard deviation were used for normal distributed quantitative data, and median and min/max were used for non-normal distributed quantitative data.
Bivariate linear regression models were performed to study the association between QoL and sociodemographic and clinical characteristics. The variable ‘work status’ had more than two categories, and a likelihood ratio statistic was employed. Those with a significant effect on QoL were considered potential confounders in multivariate analysis.
To study the association between QoL and location or support of the SA, bivariate and multivariate linear regression models were performed between QoL and type of support and location. To study the association between QoL and experiences of care, bivariate and multivariate linear regression models were performed between QoL and the total YTC, and bivariate linear regression models were performed between QoL and individual and categorized experiences of care. Then, two models were considered: Model 1 considered the 24 individual experiences of care, and Model 2 the four categories of experiences of care. Multivariate analysis encompassing linear regression and using a stepwise selection method was conducted for each model relating QoL with the experiences of care. All analysis were adjusted for potential confounders. Goodness of fit was evaluated by linearity of data, normality of residuals, homogeneity of residuals’ variance, presence of influential values and R2. VIF analysis were used to investigate the possibility of multicollinearity. The results include estimated regression coefficients, corresponding 95% confidence intervals and p-values.
R software (version 3.6.2) was used for statistical analysis, as well as the dplyr 1.0.2 and MASS 7.3-54 packages.
Results
Descriptive analysis
The sample consisted of 272 users and their characteristics are presented in Table 1. The total median score of QoL was 4.9.
Sample characterization.
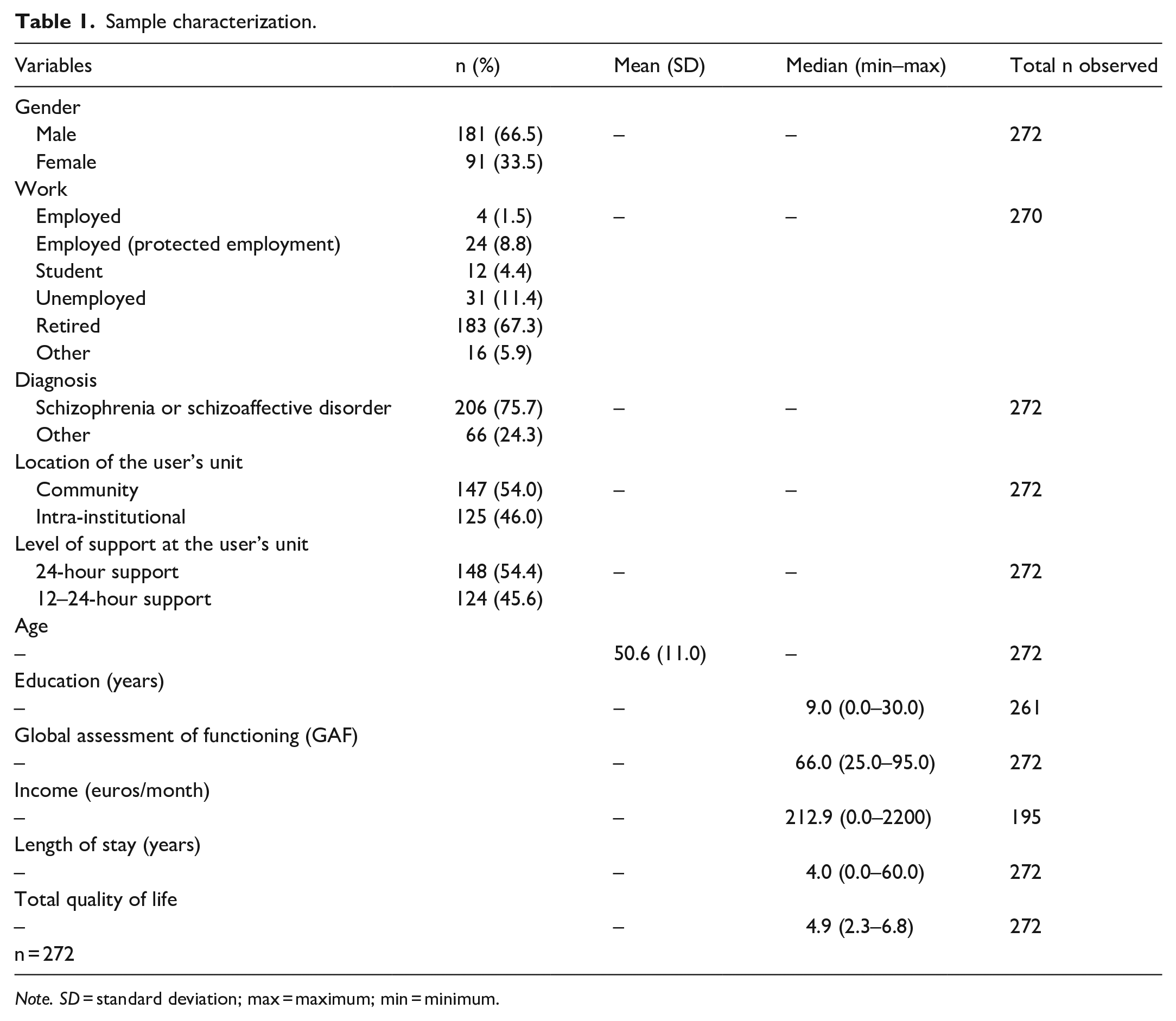
Note. SD = standard deviation; max = maximum; min = minimum.
The total median score of the YTC was 22 (7.0–25.0) and 84.9% of users said they were, in general, satisfied with care (Table 2). Although 55.9% of users reported feeling respected and accepted, 67.6% reported feeling safe and having privacy and 64.0% reported a positive relationship with professionals, only 16.2% of users felt involved in treatment.
Experiences of care.
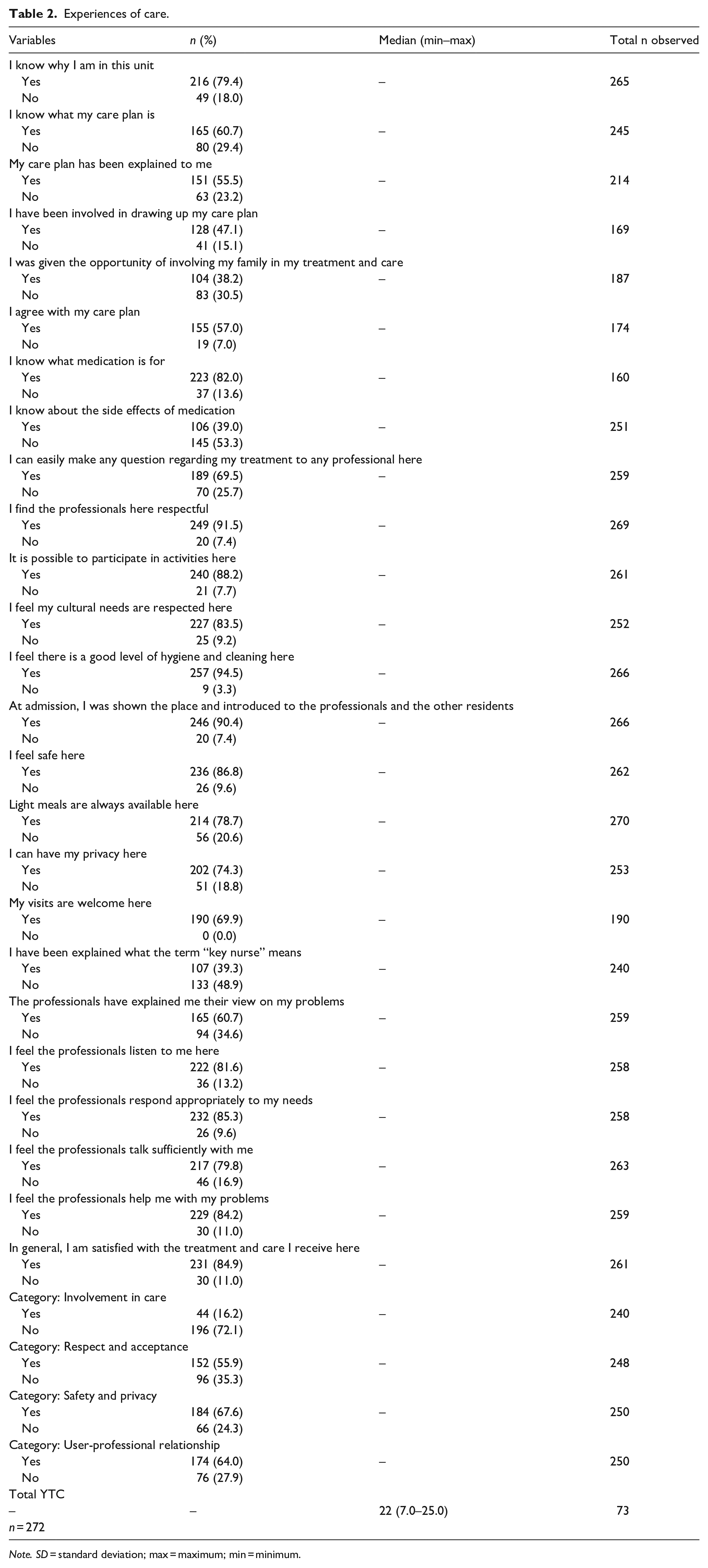
Note. SD = standard deviation; max = maximum; min = minimum.
Association between QoL and users’ sociodemographic and clinical characteristics
Significant associations between QoL and age (β = .01; 95% CI [0.00–0.02], p = .005), education (β = −.02; 95% CI [−0.04–0.00], p = .032), income (β = .00; 95% CI [0.00–0.00], p = .005), functioning (β = −.01; 95% CI [−0.02–0.00], p = 0012) and work status of users were observed (Table 3).
Association between QoL and sociodemographic and clinical characteristics of users (bivariate analysis).
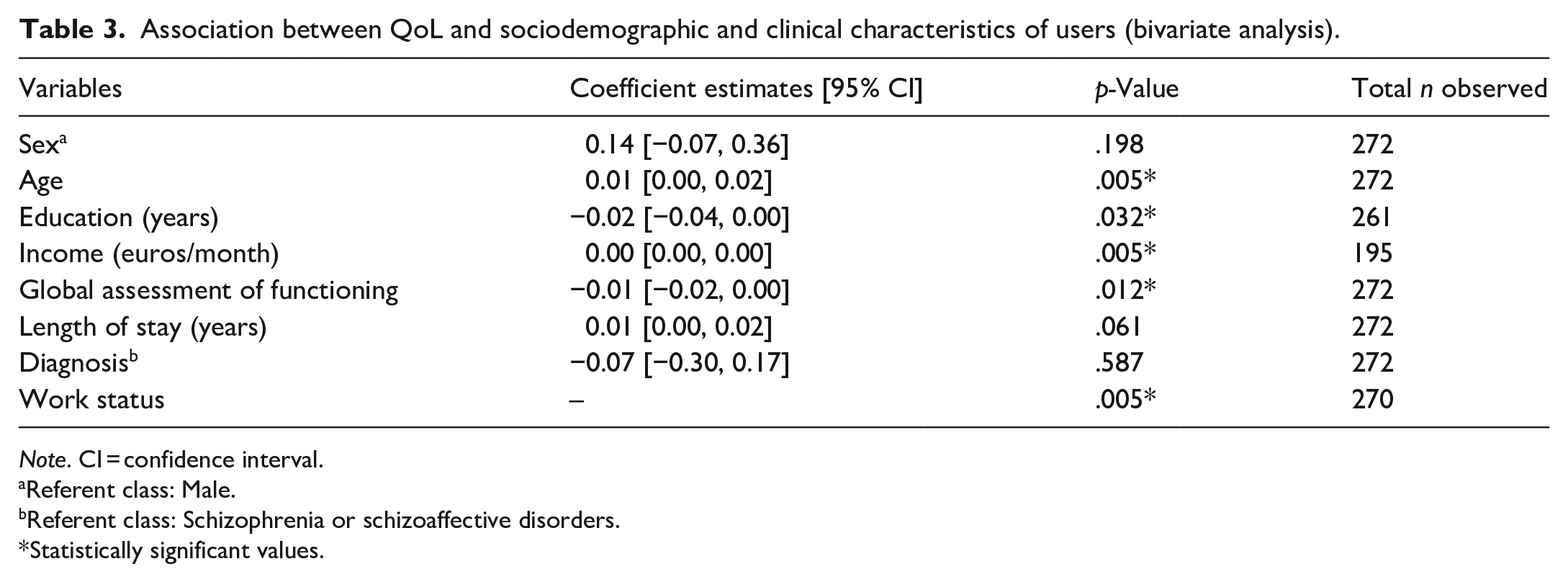
Note. CI = confidence interval.
Referent class: Male.
Referent class: Schizophrenia or schizoaffective disorders.
Statistically significant values.
Association between QoL and experiences of care
Experiences of care as a global score were significantly associated with QoL of users (β = .13; 95% CI [0.06–0.19], p = .001).
No significant associations between QoL and location (β = −.25; 95% CI [−0.50–0.00], p = .051) or the type of support (β = −.13; 95% CI [−0.38–0.13], p = .337) were observed.
In the analysis between QoL and individual or categorized characteristics of care, several individual experiences of care were significantly associated with QoL (Table 4). All four categories were positively and significantly associated with QoL of users.
Association between QoL and experiences of care (bivariate analysis).
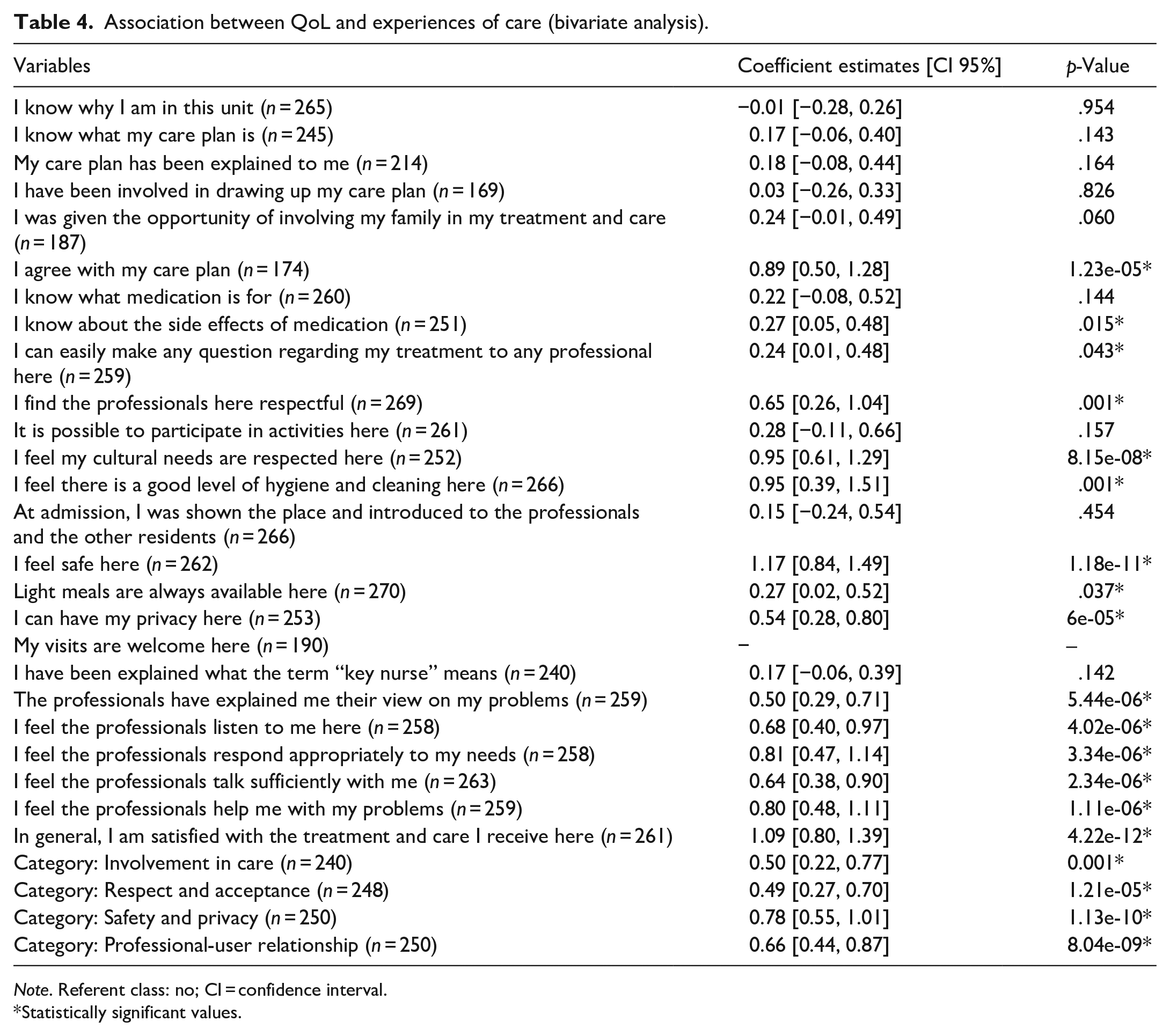
Note. Referent class: no; CI = confidence interval.
Statistically significant values.
In the multivariate analysis (Table 5), in model 1, feeling safe (β = .73; 95% CI [0.22–1.24], p = .006) and having privacy (β = .42; 95% CI [0.09–0.75], p = .014) were significantly associated with QoL of users, even after adjustment. Patients who mentioned feeling safe have, on average, 0.73 higher QoL units than patients who did not feel safe. Being able to have privacy in the residence increased, on average, 0.42 units of QoL.
Association between QoL and experiences of care (multivariate analysis).
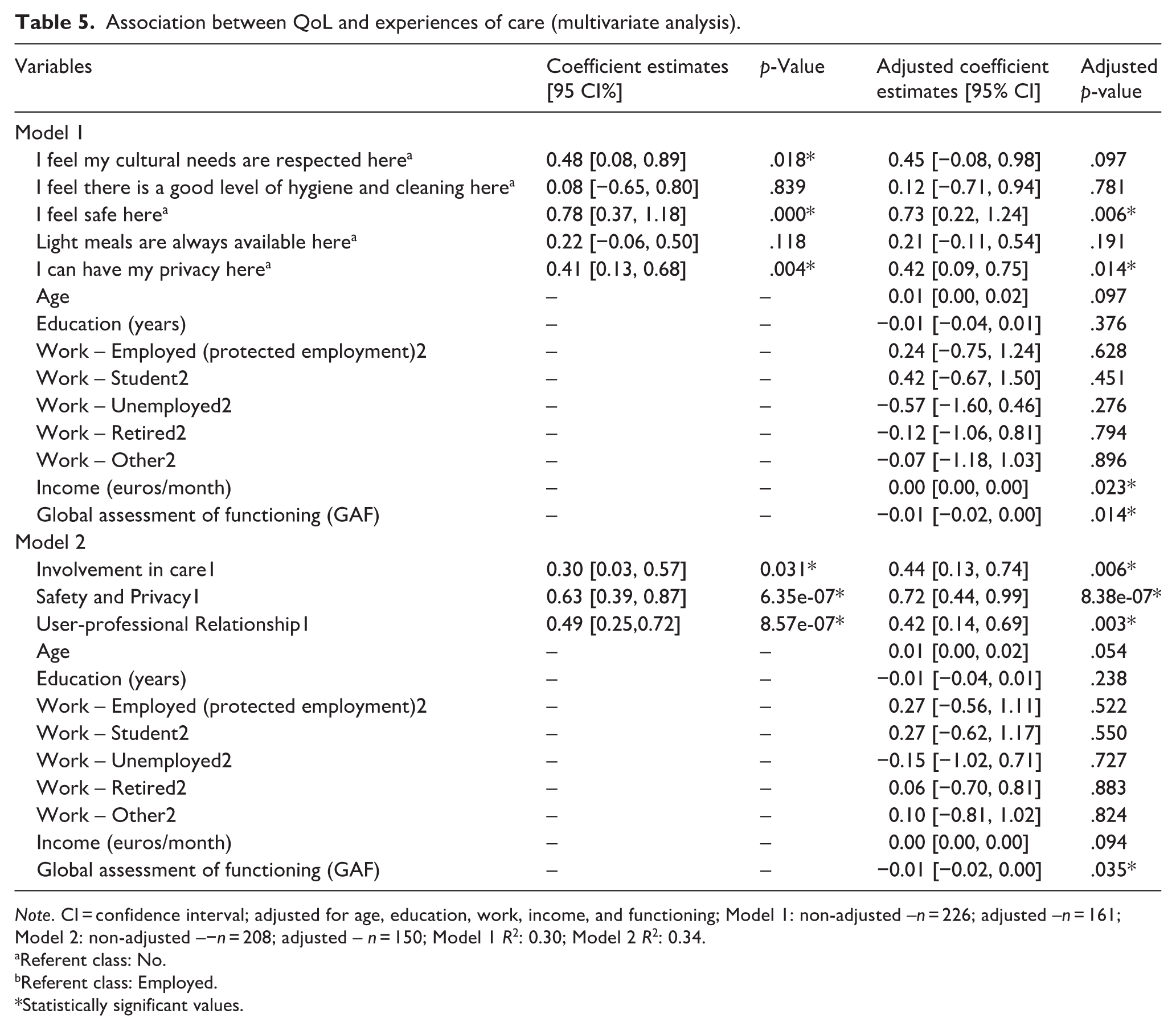
Note. CI = confidence interval; adjusted for age, education, work, income, and functioning; Model 1: non-adjusted –n = 226; adjusted –n = 161; Model 2: non-adjusted –−n = 208; adjusted – n = 150; Model 1 R2: 0.30; Model 2 R2: 0.34.
Referent class: No.
Referent class: Employed.
Statistically significant values.
In Model 2, involvement in care (β = .44; 95% CI [0.13–0.74], p = .006), safety and privacy (β = .72; 95% CI [0.44–0.99], p = 8.38e-07) and user-professional relationship (β = .42; 95% CI [0.14–0.69], p = .003) were significantly associated with QoL, even after adjustment. Feeling safe and having privacy increased, on average, 0.72 units of QoL, feeling involved in care increased, on average, 0.44 units of QoL and having good user-professional relationships increased, on average, 0.42 units of QoL.
Discussion
A main finding of this study was that the median QoL of users was high, which is reassuring. In addition, most users reported being satisfied with care in general, although this must be interpreted with caution. Users are generally reluctant to report negative aspects of care within their accommodation (Krotofil et al., 2018). Furthermore, less than one third of users answered all the questions of the YTC, and results may not reflect the view of the majority. Less than one fifth of users reported having been involved in their own care, which is worrisome and may seriously compromise recovery (Leamy et al., 2011). In contrast, feeling respected and accepted, feeling safe and having privacy and having a positive relation with professionals were encouraging aspects reported by more than 50%. However, the lack of involvement of users suggests that user-professional relationships may be unbalanced, with the preponderance of a paternalistic model of care. This is reinforced by the previous findings of Cardoso et al. (2016), who observed a low recovery-based practice in these SA.
As anticipated, better experiences of care in general were associated with better QoL. Surprisingly, no significant association between QoL and location or type of support were observed, although the association with location almost reached statistical significance. Based on this result, no distinction between location or type of support was made when analysing the experiences of care associated with QoL, contrary to what was initially intended. This lack of association may be due to a lack of sensitivity of the MANSA to distinguish small variations between QoL. However, the fact that all SA had at least 12 hours of support, probably meant that the difference in support was not sufficiently relevant to impact QoL. Moreover, analysing specific characteristics of support and care may be more informative than analysing the number of hours of support or the location. This concurs with other studies who failed to find a difference in QoL between type of support or SA (Brunt & Hansson, 2004; Harrison et al., 2020; Horan et al., 2001; Killaspy, Priebe, et al., 2016; Kyle & Dunn, 2008; Lehman et al., 1991; Oliver & Mohamad, 1992). Indeed, we further analysed data and verified that experiences of care in general were not associated with type of support or location, even after adjustment. This contrasts with the findings of Cardoso et al. (2016), who found significant differences in quality of care assessed using the QuIRC between community and intra-institutional SA. Community SA scored higher on the Living Environment, Treatment and Interventions and Self-Management and Autonomy domains. Although quality of care assessed using the QuIRC was associated with the experiences of care of users in the study by Cardoso et al. (2016), it is possible that differences in quality of care perceived by professionals are not sufficiently relevant to translate into pertinent differences in experiences of care and in QoL of users. This is aligned with the findings by Killaspy et al. (2012), in which a 10% increase in any QuIRC domain led to a maximum increase of 1.1 units in the users’ experiences of care scores, using the YTC. The suggestion that QoL of users is more impacted by care as experienced by users than by care as assessed by professionals reinforces the need to involve users in planning, delivery, and evaluation of care, which is seldom considered in Portugal.
In the model that studied experiences of care as single items, safety and privacy were significantly associated with QoL. Feeling safe is one of the most valued experiences of care by users of SA (Barnes et al., 2022; Bengtsson-Tops et al., 2014; Forchuk et al., 2006; Gonzalez & Andvig, 2015; Kirsh et al., 2011; Padgett, 2007; Piat & Lal, 2012; Roos et al., 2016; Whitiey et al., 2008). Unfortunately, it is likely that feelings of safety have often been absent throughout the lives of people with SMD due to stigma, family conflicts, relapses and frequent hospitalizations and poverty, among others. SA may not only act as a barrier from the outside world providing physical safety, but also mean having a stable place, the safety of constant relationships and the provision of consistent and readily available support, contributing to feelings of psychological and social safety (Krotofil et al., 2018; Padgett, 2007). Constancy and safety in the material and social environment leading to a sense of being at ‘home’ is the ground for the development of ontological security, considered paramount in the recovery process (Krotofil et al., 2018; Padgett, 2007). Therefore, it seems understandable that safety was the experience of care with the highest impact on QoL. This has several implications at the practical level. Ideally, SA should be located in safe neighbourhoods, which, unfortunately, is frequently impeded by financial issues. Support must always be readily available to users, regardless of the type of accommodation or how it is delivered. The constancy of professionals and non-stigmatizing attitudes should be fostered by creating motivating work environments and continuous education. Relationships between users should be promoted and emerging conflicts should be promptly dealt with.
The importance of safety that evolves from constancy needs to be considered in stepwise SA care. Overemphasis on move-on or short maximum lengths of time may be detrimental to recovery and independent living. In Portugal, a maximum length of stay of 12 months has been recently established for all types of SA working under the CCISM, independently of type of support, although an extension may be requested (Portaria 311/2021, 2021). Time-limits may be important when establishing goals with users and families and in fostering action from users and professionals towards independent living. However, 12 months may be an unreasonable timeframe, as the process of adaptation, constructing relationships, developing feelings of safety and constancy and engaging in the process of working towards recovery requires time and cannot be hastened. In addition, this process varies with the needs and clinical severity of users, making the establishment of the same time-limit to all types of SA incomprehensible.
Privacy was also found to be one of the most valuable experiences of users, in line with previous research (Bengtsson-Tops et al., 2014; Brolin et al., 2015; Forchuk et al., 2006; Krotofil et al., 2018; Nelson et al., 2003; Padgett, 2007). In general, users prefer having their own private space, whether a room or an apartment (Krotofil et al., 2018). A private space means that users can have a refuge when they want to be away from other people, and to retreat from social and practical activities (Bengtsson-Tops et al., 2014; Krotofil et al., 2018). It also means having a space where users can feel calm and peaceful (Bengtsson-Tops et al., 2014). For these reasons, it is not surprising that privacy has a significant influence on QoL, which has important implications. Ideally, all congregate-living SA should have predominantly private rooms available. Double rooms should be only for users who express such will, and users must be able to choose whom they want to share their room with. Unfortunately, financial issues are also a frequent impediment to the availability of single rooms. More than half of the SA included in this study had no single rooms, and, in 38%, more than two people shared a room (Cardoso et al., 2016). The CCISM established the limit of two people per room, but more support from the government is needed for SA to be able to offer decent and dignified conditions, and the necessary privacy (Portaria 311/2021, 2021).
In the model that studied experiences of care grouped into categories, safety and privacy remained significantly associated with QoL, and with the highest impact. Two other categories influenced QoL: involvement in care and user-professional relationship. Decisions concerning the lives of people with SMD have often been made by others. However, users value SA that offer choice and control and foster their participation, and involving users in care promotes empowerment, self-management and motivates them in the process of recovery (Brolin et al., 2015; Gonzalez & Andvig, 2015; Krotofil et al., 2018; Leamy et al., 2011). Therefore, it is not surprising that involvement in care impacted QoL. Alarmingly, only 16.2% of users felt involved in their care. Continuous training, supervision and evaluation seem essential to improve care and to modify attitudes and ways of working. The CCISM reinforces the need to involve users in their individual plan of care, and foresees periodic monitoring of recovery-based practice, which may help to increase the involvement of users in care. However, problems concerning definition and collection of these indicators have been observed (Equipa de Acompanhamento das experiências piloto CCISM, 2020; Portaria 311/2021, 2021).
Users of SA frequently do not have other supports in the community and they often experience feelings of loss and rejection (Gonzalez & Andvig, 2015; Krotofil et al., 2018). As a consequence, they value stable, trusting and supportive relationships with professionals (Krotofil et al., 2018). Feeling listened to, understood, encouraged and emotionally supported by professionals are important needs that are met by good relationships, and may offset feelings of isolation and loneliness (Bengtsson-Tops et al., 2014; Gonzalez & Andvig, 2015; Krotofil et al., 2018). The significant association found between user-professional relationships and QoL is also comprehensible. The fact that roughly two thirds of the users reported good relationships with professionals is positive. However, the fact that other findings suggest a relationship imbalance towards a paternalistic way of care is worrisome and may foster dependence (Krotofil et al., 2018). Involving people in care and offering them choice and control is important to balance user-professional relationships and foster autonomy.
This study has several strengths. It is, to our knowledge, the most comprehensive study on the association between QoL and characteristics of care experienced by users of SA in Portugal. All the medium and high-support units in the country were included, and a randomized sample of users was interviewed. In addition, standardized instruments were used and administered by trained professionals. Most data on SA comes from the United States, Canada, Australia and the United Kingdom, with little input from other countries. Having data on SA from other countries, with diverse socioeconomic and political contexts, is fundamental to better comprehend SA. The fact that Portugal is a not so wealthy country within the European Union and that its first Mental Health Plan has less than 15 years, makes the study of this country’s mental health care technically relevant from an organizational point of view.
The present study has some limitations. It did not include independent living with mobile support. In addition, QoL and experiences of care may be impacted by other individual, social and contextual factors that were not included. Due to the used methodology other relevant experiences of care may have been neglected and the direction of the relationship between QoL and experiences of care cannot be confirmed. Data was collected in 2012 and may not cover possible changes occurring in SA with the implementation of the CCISM. However, the development of the CCISM has been much slower than expected, currently, encompassing the lowest number of places of all SA in the country. Therefore, it seems unlikely that paramount changes in care delivered by national SA have occurred.
Conclusions
Studying which experiences of care of users of SA influence QoL may contribute to better understand how these services should be organized to promote recovery. Feeling safe, having privacy, feeling involved in one’s own care and having good user-professional relationships were found to impact QoL of users of SA. Therefore, these are important dimensions SA should be able to provide. Implications of these findings require action from the political and economic level to the local organizational and individual levels. Governments must provide more financial support for SA to be able to develop adequate housing conditions that ensure safety and privacy. When establishing maximum lengths of stay, unreasonable and unjustifiable timeframes must be avoided. Involving users in the planning, delivery and evaluation of care at all levels is fundamental. Continuous training, supervision and evaluation are essential to improve care and modify attitudes and ways of working.
Highlights
- QoL perceived by users is not related to type of support or location.
- QoL perceived by users is probably more impacted by care as reported and experienced by users versus when assessed by professionals.
- QoL is positively associated with feeling safe, having privacy, being involved in care and having good user-professional relationships.
Future implications
- Governments must provide more financial support for SA to be able to provide adequate housing conditions that ensure safety and privacy.
- When establishing maximum lengths of stay, governments and SA must avoid unreasonable and unjustifiable timeframes.
- Involving users in the planning, delivery and evaluation of care at all levels is fundamental
- Continuous training, supervision and evaluation are essential to improve care and modify attitudes and ways of working.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the General Health Directorate of the Ministry of Health, which was not involved in any of the study aspects – design, data collection, analysis and interpretation, writing of the paper and submission to publication. Authors Bárbara Pedrosa and Ugnė Grigaitė are PhD candidates funded by Fundação Ciência and Tecnologia (FCT) (UI/BD/151072/2021 and (UI/BD/151073/2021, accordingly) and author Deborah Aluh is a PhD candidate funded by LaCaixa Foundation (LCF/BQ/DI20/1178001).
Data availability statement
The data are not publicly available due to privacy or ethical restrictions. Data are available to investigators outside the Lisbon Institute of Mental Health after request and approval by the principal investigator of the original study.
Ethical considerations
This study was approved by the Ethics Committee of NOVA Medical School of the NOVA University of Lisbon. Written informed consent was obtained from every participant and data confidentiality were guaranteed.