
Abstract
Family environments are known to usually be better for children’s development than institutional care. China has experience with different forms of foster care, but none have been empirically evaluated, especially with respect to children’s outcomes. One form of foster care is ‘collective fostering’, in which many foster families live in a single apartment building on the grounds of the institution. The goal of this study was to evaluate the effectiveness of such a project operated by a children’s institution in a large city in China by examining changes in children’s height and weight from before to after entering foster care. Results (n = 102, mean age = 63 months) showed a significant positive quadratic relationship between time and height (p = .002), with height z-scores declining during institutional residency and then increasing after entering foster care. Further analysis on children (n = 23) who were enrolled in the fostering project for more than 65 months showed that their height and weight z-scores improved significantly while living in foster families compared to the last assessment before the transition. The study concluded that the collective foster care project, like the more widely practiced community foster care, had the potential for improving children’s development.
Introduction
In China, an orphan is defined as an individual under age 18 who has lost both parents through death or abandonment and is unsupported by others (Liu and Zhu, 2009). Currently, there are approximately 573,000 orphans under age 18 in China (National Statistics Bureau, 2006); female children and children with disabilities are overrepresented. The majority live in rural areas, and more than half receive some level of government assistance (Shang, 2002). Family environments are known to usually be better for children’s development (Smyke et al., 2010; Whetten et al., 2009, 2014), but children with disabilities are unlikely to be adopted by families. To provide family-like environments to orphans with disabilities, the Chinese government established a collective foster project in Chongqing institution in 2007. This study is an international collaboration between the University of Pittsburgh, the East China Normal University, and the Chongqing Child Welfare Institution, which evaluated the quality and the effectiveness of the collective foster program by collecting and analyzing information on children’s height, weight, and the child–caregiver relationship. To our knowledge, this is one of the first empirical evaluations of foster care programs in China.
History of orphan care in China
Since the advent of Chinese Communism in 1949, orphan care in China can be divided into two main eras, namely, before and after the economic reforms of 1978. Prior to this time, institutional care was considered the preferred form of care for orphans, and it was governed by the Chinese central government; foster care, broadly defined as temporarily placing children with unrelated families (Shang, 2002), was used only when institutional care was not available (Office of Policy Studies, Ministry of Civil Affair (MOCA), 1984). The foster care practiced by the Chinese government at that time was considered ‘informal’ foster care, which lacked a formal system of selecting and monitoring foster families.
During the economic reforms, the government’s social welfare budget was reduced (Shang, 2002; Wong, 1998). Over the subsequent years, many children’s institutions faced severe financial difficulties, and simultaneously there was a sharp increase in the number of orphans (Shang, 2002). The majority of orphans were female children and children with disabilities, which could be explained by at least five main factors. First, the social security system barely covered treatments for children, so many parents were not able to afford the expensive treatments needed by children with disabilities (Shang, 2002). Second, the one-child policy of 1979 allowed most married couples to have only one child; couples in rural areas could have a second child if the first one was a girl. Traditional Chinese families believed that only healthy male children could take care of their parents during their old age (Shang, 2002). Third, the Chinese traditionally favored males, because only sons could continue the patrilineal family line (Johnson et al., 1998).
Fourth, there was a flow of population from the rural areas (high rate of poverty) to the urban areas, and people became more aware of the children’s institutions. Therefore, more children with disabilities (mostly from rural areas) were being relinquished to the institutions in urban areas (Shang, 2002). Last, increased rates of divorce, broken families, and births outside marriage may have contributed to the increase in children without permanent parents (Shang, 2002).
Because of these factors, more and more domestic and international nongovernmental organizations (NGOs) became involved, and the balance of responsibility for orphans then shifted from the state toward society (Shang, 2002). In addition, foreign NGOs not only became more involved in providing institutional care for orphans, but they also introduced formal foster care to China in the early 1990s. Unlike the informal foster care system, formal foster care placed more emphasis on ensuring organization and the quality of care, including the selection process, training, transition, and support and monitoring after placement.
Current institutional care in China
Currently, institutional care in China is separated from society, insufficiently funded, and of relatively poor quality (Human Rights Watch, 1996; Zhang, 2003). Three main factors contribute to this. First, the majority of staff are recruited from society without prior knowledge and skills in childcare (Wang, 2007; Zhu and Cai, 2007), and limited training occurs after hiring (Liu and Zhu, 2009). Second, children-to-staff ratios are high in Chinese institutions: ranging from 2.99:1 to 4.18:1 according to the National Statistics Bureau (2006), and this number may represent the total number of caregivers employed in an institution; informal observation finds that the number of children per caregiver at any one time during the day can be much higher. Although this reported ratio is better than in many low-resource countries (Rosas and McCall, 2011), it is much higher than the 1.5:1 ratio in many affluent countries (National Statistics Bureau, 2006). Third, the staff turnover rate is high and monitoring for abuse and neglect is insufficient (Wang, 2007; Zhu and Cai, 2007).
Impact of institutional care and foster care on orphans
Institutions throughout the world provide different levels of physical care (health, nutrition, stimulation); however, nearly all of them provide a deficient psychological environment (Rutter et al., 2007; Van IJzendoorn et al., 2011). Psychological deprivation is characterized by the lack of warm, sensitive, and responsive interactions with a few consistent caregivers, the lack of structural and operational environments that support such relationships, and the lack of adequate stimulation (Rutter, 1998; The St. Petersburg-USA Orphanage Research Team, 2005, 2008). In some institutions, by the time children are 2 years old, they have experienced 60–100 different caregivers, and the time they spend with each caregiver is often too short for them to form personal relationships (The St. Petersburg-USA Orphanage Research Team, 2008).
Western studies of institutionally reared children consistently find higher rates of poor general development. For example, institutionalized children show delays in physical growth (Dobrova-Krol et al., 2008; Johnson and Gunnar, 2011; Miller et al., 2010; Vorria et al., 2003) and language and cognitive development (Van IJzendoorn et al., 2008). In addition, children living in institutions have higher rates of insecure attachment and indiscriminate friendliness (Bakermans-Kranenburg et al., 2011; Tizard, 1977; Tizard and Hodges, 1978; Tizard and Rees, 1975). Moreover, the negative effects of institutional care are worse the longer the children reside in institutions (McCall, 2011; Zeanah et al., 2011).
Fortunately, the negative effects of institutional care are not always permanent. Institutionalized children are known to improve in development after being transitioned to foster (Johnson et al., 2010) and adoptive families (Johnson and Gunnar, 2011; Miller et al., 2010), and their physical and mental development are related to better caregiver–child interactions (Johnson et al., 2010; Van IJzendoorn and Juffer, 2006). Studies show that institutionalized children improve in their cognitive function (Nelson et al., 2007) and attachment (Smyke et al., 2002; Zeanah et al., 2002) after living in foster families. And compared to children who remain in institutions, children who transition to family environment usually show better development (MacLean, 2003; Tarullo et al., 2007; Van de Dries et al., 2010).
Nevertheless, Johnson and Gunnar (2011) pointed out that not all children improved or improved at the same rate after being placed with families. The most significant improvements in height, weight, and head circumference were among those with the lowest initial developmental levels and those younger than 12 months. The Bucharest Early Intervention Project (BEIP) also found that the older the children were when placed in a family, the lower the probability that they developed secure attachments with their foster parents (Smyke et al., 2010). Generally, current research suggests that more time spent in institutions is associated with higher rates of poor developmental outcomes, and the younger age at family transition is associated with higher rates of better outcomes (Johnson and Gunnar, 2011; Van den Dries et al., 2009).
There is limited research on the effects of institutional care on children’s development specifically in China. Most existing studies were conducted on Chinese children adopted to North American. Based only on data collected within a few weeks after adoption, Chinese post-institutionalized children also exhibited general developmental delays (Cohen et al., 2008; Pomerleau et al., 2005; Robert et al., 2005). However, similar to children from other countries, Chinese children show rapid improvement in their physical, cognitive, motor, and language development after being placed in stable family environments (Cohen et al., 2008; Miller and Hendrie, 2000; Pomerleau et al., 2005), suggesting that the prior institutional environment did not support their early development as well as families would have.
Current foster care system in China
The Chinese government did not immediately respond to the concept of formal foster care when it was introduced in the early 1990s. After 10 years, the State Council issued ‘A Notice on Forwarding “the Opinion of Accelerating Socialization of Social Welfare”’ (Shang, 2002: 211), which stated that orphanages would still be mainly managed by the government, but societal donations, adoptions, and foster care were accepted and encouraged. During the past 20 years, the Chinese government has collaborated with NGOs and planned several alternative foster care projects, such as the Guangde Model, the Beijing Model, and the Shanghai Model. Each model adopted a different approach to family foster care with its own strengths and weaknesses. Although they reported improved well-being of children after being enrolled in the project (Shang, 2002), there was no report of any systematic measurements on the children to substantiate this claim.
The Guangde Model was the first effort during the economic reform, and it suggested that adoption and foster care were better for children. The Save the Child Fund (SCF) created this model as an alternative to formal adoption. Starting in the Guangde Children’s Welfare Home, they created home units in the institution and placed one mother and two teachers in each home unit to take care of five children (Shang, 2002). This model influenced the current Chinese foster care policy, and it served as a model for providing family-like care to children with disabilities who were unlikely to be adopted (Wright, 1999).
The Beijing Model started in 1992 by recruiting three families as foster families for a few children. However, the government expanded the size of foster care after they observed that children’s health greatly improved after receiving foster care; moreover, the cost of foster care was cheaper than formal institutional care when the institutionalized children were placed in rural foster families. However, the Beijing Children’s Welfare Home had to send in doctors and teachers to the villages to ensure quality of healthcare and education (Shang, 2002).
The Shanghai Model, a collaboration among the government, civil society, and citizens, represented a community-based foster care project started by the director of the Shanghai Civil Affairs Bureau (SCAB) and a British NGO that provided training and consultation. It was the first foster care project that attempted to have professional foster care placement, childcare, and continuous post-placement supervision and support (Shang, 2002).
Regardless of models, finding qualified and suitable foster families is one of the most important requirements of successful foster care projects. Currently, China has a huge potential for recruiting foster families for several reasons (Shang, 2002). First, due to the one-child policy begun in 1979 (Kane and Choi, 1999), many middle-aged parents are experiencing empty nests. Many of them love children but could not have more children of their own, so they are good potential candidates for fostering children. Second, Chinese society has a positive view of those parents who qualify to foster children in need. Third, many families in the rural areas could benefit from extra income, and some foster care projects give monthly salaries and other material support to foster parents.
Although some aspects of formal foster care systems are adopted from Western countries, the Chinese system has its own unique characteristics (Shang, 2002). First, unlike many Western countries, Chinese government agencies retain legal guardianship of all the orphans or abandoned children placed in foster care. Second, many children receiving foster care have disabilities and thus are unlikely to be adopted. Third, children are placed with foster families on a temporary basis, but the projects intend to keep the children with the same families for as long as possible so that they can benefit from a permanent family environment.
Collective foster care project
China’s Ministry of Civil Affair provides training, program development, and operational support for orphan care programs in state-run welfare institutions throughout China. In 2007, a Family Village Program (which is referred to as collective foster care in this article) was established with six families living in former staff apartment housing. In 2009, the program expanded to a new apartment building (built specifically for this purpose) containing 24 apartments located on the grounds of the institution. Institution administrators recruited married couples who had to have prior experience raising their own biological children who no longer lived with them. Each qualified set of foster parents was assigned an apartment unit, and they fostered up to four children initially – between ages 5 and 158 months – who were transferred from the welfare home. Both foster parents completed 2 weeks of training led by professional trainers prior to fostering, and all foster mothers met weekly with a full-time Family Mentor for additional trainings and support. The foster fathers were allowed to work outside the welfare home during the day, and the foster mothers received a monthly stipend from the project in exchange for full-time parenting and ongoing attendance at training sessions. Wages for foster mothers made this program substantially appealing because most community foster parents receive payments only for children’s expenses.
During the day, all the foster children went to daycare, school, and specialty services (i.e. speech therapy, physical therapy) in the institution. The project initially started with six foster families in 2007 and expanded throughout the years. By 2011, the project grew to its full capacity of 24 families. Because children with disabilities are unlikely to be adopted in China, this foster care program intentionally enrolled children with mild physical and mental disabilities, so they could have a chance to experience and benefit from a permanent family environment. Children with extremely limiting disabilities were not selected for the program because the program believed that children with less severe disabilities were more likely to benefit from the program and show improvements in their development. Moreover, their relatively good status enabled each foster family to take care of four children.
Besides meeting the child’s basic needs, all foster parents were trained to be child-directed when interacting with children. Stability was another focus; the same group of children was kept with the same foster family for as long as possible. If parents withdrew from the project, all the foster children in the family were kept together and assigned to the next available foster family. Although most of the children were unlikely to be adopted due to their disabilities, a few were adopted and were excluded from this study. And when that occurred, project staff made sure that all the other aspects of the foster family stayed relatively stable.
The practice of ‘collective foster care’ has a number of benefits and overcame some of the challenges experienced by previous foster care models. First, the environment of foster care is much more similar to the typical family environment compared to institutional care. Second, living in the same apartment complex allows foster parents to form a community to support and help each other. Third, having foster families live near the institution allows project staff to monitor the quality of foster care and the children’s development more closely. Fourth, it is convenient and easy for project staff to provide regular training and continuous support to foster families when all families live in one place. Fifth, education and healthcare can be readily provided by the institution and its quality can be easily monitored. Sixth, collective foster care permitted the government to more easily fulfill its responsibility of monitoring the foster families and children’s development.
This study was a field study of the collective foster care project. To our knowledge, there was no prior systematic empirical study of the development of children transitioned to foster care of any kind in China. Having external ‘observers’ in any Chinese institution is unusual, so every effort was made in the current project to conduct this field study as quickly and as unobtrusively as possible. Thus, we relied on the institution’s records of physical growth measures; the institution’s growth records also provided longitudinal assessments before and after foster care for many children, which we would not have been able to collect ourselves. Throughout the study, we only made one direct observation on the foster families: we collected information on the children and their foster parents using the Caregiver–Child Social, Emotional, Relationship Rating Scale (CCSERRS; McCall et al., 2010), which was used to evaluate the quality of parent–child interactions. Based on existing literature, this study hypothesized that children would improve in physical growth after transitioning to foster care, the quality of caregiver–children interactions would be related to the amount of developmental improvement of children, and younger children at placement would improve the most (Johnson et al., 2010).
Method
Participants
The collective foster care project enrolled a total of 24 foster families, which have fostered 113 children. In all, 11 children’s records were excluded due to missing data; otherwise all children (102 children, 65 males) were included in the project. Each family hosted four children at a time, but some families have cared for more than four children over time because some children were adopted or had to be removed from the families for reasons unknown to us. According to the institution’s records, nearly all (93%) of the children had existing diagnoses of mild physical or mental disabilities according to the Chinese criteria, such as Down syndrome (10%), cerebral palsy (20%), intellectual disabilities (32%), and other health issues and disabilities (31%). The ages of the children ranged from 5 to 158 months (average 63 months) when transitioned from the institution to the foster families. The age distributions of the 102 children at transition to foster care are listed in Table 1.
Distribution of age at placement of children in foster care.

Assessment battery
Height and weight
Stunted growth was found to be an important and consistent predictor of education outcomes and other domains of child development, such as cognition and academic achievement (Grantham-McGregor et al., 2007). In this study, children’s height (cm) and weight (kg) were obtained from institutional records. Those measurements were taken by institutional staff over numerous years, and we could not independently verify the accuracy of such measurements. The only factor that could affect the accuracy of weight measurements is that children were weighted with clothes on, and some subtraction for the weight of clothes was made during the winter.
Height and weight measures were transformed into z-scores based on the standards provided by the Center for Disease Control and Prevention (CDC), which are commonly used throughout the world because of the precision of its measurements. Chinese growth standards were not used because the chart available to us only provided means and standard deviations of height and weight up to age 7, which would greatly decrease the amount of data available for analysis. Moreover, racial/ethnic differences are minor in the first years of life but increase with children’s ages (Dana Johnson, 2012, personal communication). However, we did compare the z-scores computed based on the CDC and China standards and found that the height z-scores were very similar, but the CDC standards for weight gave a substantially lower z-score fairly uniformly across age than did the Chinese standards (i.e. Chinese children are lower in weight than US children).
CCSERRS
The CCSERRS was created specifically for use in institutions to assess individual caregivers on a number of dimensions of caregiver–child interaction (McCall et al., 2010). Its original version contained 18 dimensions to be rated, but this study used a condensed version of nine items called CCSERRS-Brief. In the original scale, separate items existed for positive and negative displays of the same behavior, and these were combined into a single dimension in the briefer version. The nine items are divided into three categories. Items 1–5 focus on the caregiver’s behaviors, Items 6–8 pertain to the children’s response to the caregiver, and the last item reflects the caregiver–children relationship. Each item is rated on a 4-point Likert-scale (0–3), where 3 means the most positive. CCSERRS can be rated during three different activities: feeding, changing/dressing/bathing, and free play.
Previously determined reliability and validity were tested on the original 18-item CCSERRS (McCall et al., 2010). The inter-rater reliability showed that paired raters were identical or within 1 point difference on 96 percent of the cases. A significant difference (t(42) = 13.29, η2 = .78, p ⩽ .001) between caregivers in an intervention versus a nonintervention institution showed that CCSERRS is likely to have ‘construct validity for reflecting positive socioemotional interactions and relationships between caregivers and children’ (p. 213). Validity should not be systematically different for the briefer version of nine items because the two versions measure the same behaviors.
A faculty member and three graduate students from a Chinese university were trained on CCSERRS for 1.5 days (12 hours) by the assessment team, which included the authors of the CCSERRS. The training included the introduction of CCSERRS, in-person and video demonstrations, and role play. Reliability for the assessors in the current project was evaluated by the trainers. The mean percentage of paired ratings within 1 point for 10 pairs of the five assessors (one of the raters was trained for another project) on 10 videotaped segments of caregivers with children (after their training and discussion sessions) was 94 percent.
Procedure
The caregiver–child interactions for foster parents in families 1–16 were then assessed by three trained raters over a 2-day period using CCSERRS-Brief. Ideally, each rater would observe a foster parent interacting with their foster children as a group for 5 minutes at each situation of feeding, changing/dressing/bathing, or free play. Due to limited time and number of assessors, caregivers were observed engaged in at least one of these three activities, sometimes by two different assessors at different times or days. Consequently, none of the foster parents had ratings in all three activities – previous work by the authors with the CCSERRS indicated ratings were not much different as a function of the specific activity. For each CCSERRS-Brief item, the scores by different raters during the same activities were averaged, and these averages for the available activities were then averaged to give the caregiver’s final score.
Assessors obtained from institutional records the name, date of birth, gender, date of institution entry, date of foster family entry, foster family number, diagnosis, height, and weight on the 102 children assigned to the 24 target families. Most children in Chinese institutions are abandoned and do not have birth certificates, so their birthdays were estimated by orphanage doctors at the intake based on their growth status. During their stay in the institution and during foster care, all children had routine physical check-ups approximately every 6 months. Therefore, depending on their age and the length of their stay at the institution, many of them had numerous measures while they were in the institution and at least one measure after transitioning to families. A small group of children (the ones transitioned to the first six families at the beginning of the program) had additional measures approximately every 6 months for 65 months after transition.
Analysis plan
The analysis was conducted on three samples of families, each of which possessed different data of interest.
Families 1–24: Height and weight
The first sample included the total sample of 102 children in 24 foster families. Polynomial regression analysis was used to examine the trends of change in height and weight prior to and after foster family transition (Cohen et al., 2003). This sample had the advantage of having the largest number of children and foster families and the most assessments of children while residing in the institution before transitioning to foster care, but it had the disadvantage of having a variable number of assessments for different children. We treated each assessment as an independent data point in the regression analyses, although individual children contributed more than one measurement. This strategy violated the usual assumption of independence of all measurements, which affected estimates of the statistical significance but not necessarily the form of the regression relation. Thus, statistical significance for this analysis should be regarded as descriptive.
Families 1–16: Height and weight versus CCSERRS
The second analysis examined the relation between height/weight change of 64 children and the families’ CCSERRS scores in families 1–16 collected by three trained assessors (no children from families 1–16 were excluded in this analysis). These 64 children were placed in foster families at different times between years 2007 and 2011, so their length of foster family placement ranged from 6 to 55 months when CCSERRS data were collected in November 2011. Pearson’s correlations were calculated between children’s change in weight and height and family caregivers’ CCSERRS scores (i.e. caregiver scores, child scores, relationship scores, and the total score). Height and weight changes were calculated using the last measurement before and last measurement after foster family transition.
Families 1–6: Longitudinal data
The third sample consisted of children with multiple physical growth assessments after transitioning to foster care. The project started with six families in 2007, and it gradually expanded to 24 families by 2011. Therefore, children were placed in foster families at different times. Only the children who were placed and stayed in the first six families had multiple physical examination records after being placed in families. Therefore, in the third set of analyses, we selected 23 children with longitudinal data from families 1–6; two children were excluded due to their lack of longitudinal data. The 23 children had at least one physical growth measurement before transitioning to foster care (baseline) and seven measurements while living with foster parents (approximately 1, 7, 14, 20, 38, 55, and 65 months after family placement). We examined their trends of weight and height change over time during their stay with foster families using one-way within-subject analysis of variance (ANOVA). Additionally, a 6 × 8 within-subject analysis of covariance (ANCOVA) was performed separately on both height and weight as a function of family assignment and time of measurement, controlling for age-at-transition groups, and a 3 × 8 within-subject ANCOVA was performed separately on both height and weight as a function of age-at-transition group and time of measurement, controlling for CCSERRS relationship score. This sample had the advantage of being truly longitudinal and thus provided intra-individual change in response to the foster care intervention, but it was based on fewer children and families.
Results
Families 1–24: Height and weight
Polynomial regression analysis was used to examine the trends of change in height and weight prior to and after foster family transition for the maximum sample of families 1–24 described above (see Figure 1; Cohen et al., 2003). For the children’s height, the linear regression coefficient was not significant (R2 = .05, F(1, 599) = 2.984, p = .085), but the quadratic regression coefficient was significant and positive (R2 = .02, F(2, 598) = 6.181, p = .002), suggesting that z-scores for height decreased while children resided in the institution but increased after they were transferred to foster families. The trend for weight also appeared to be quadratic (Figure 1), but neither linear (R2 = 0, F(1, 599) = .07, p = .792) nor quadratic (R2 = 0, F(2, 598) = .051, p = .951) components were statistically significantly related to time.
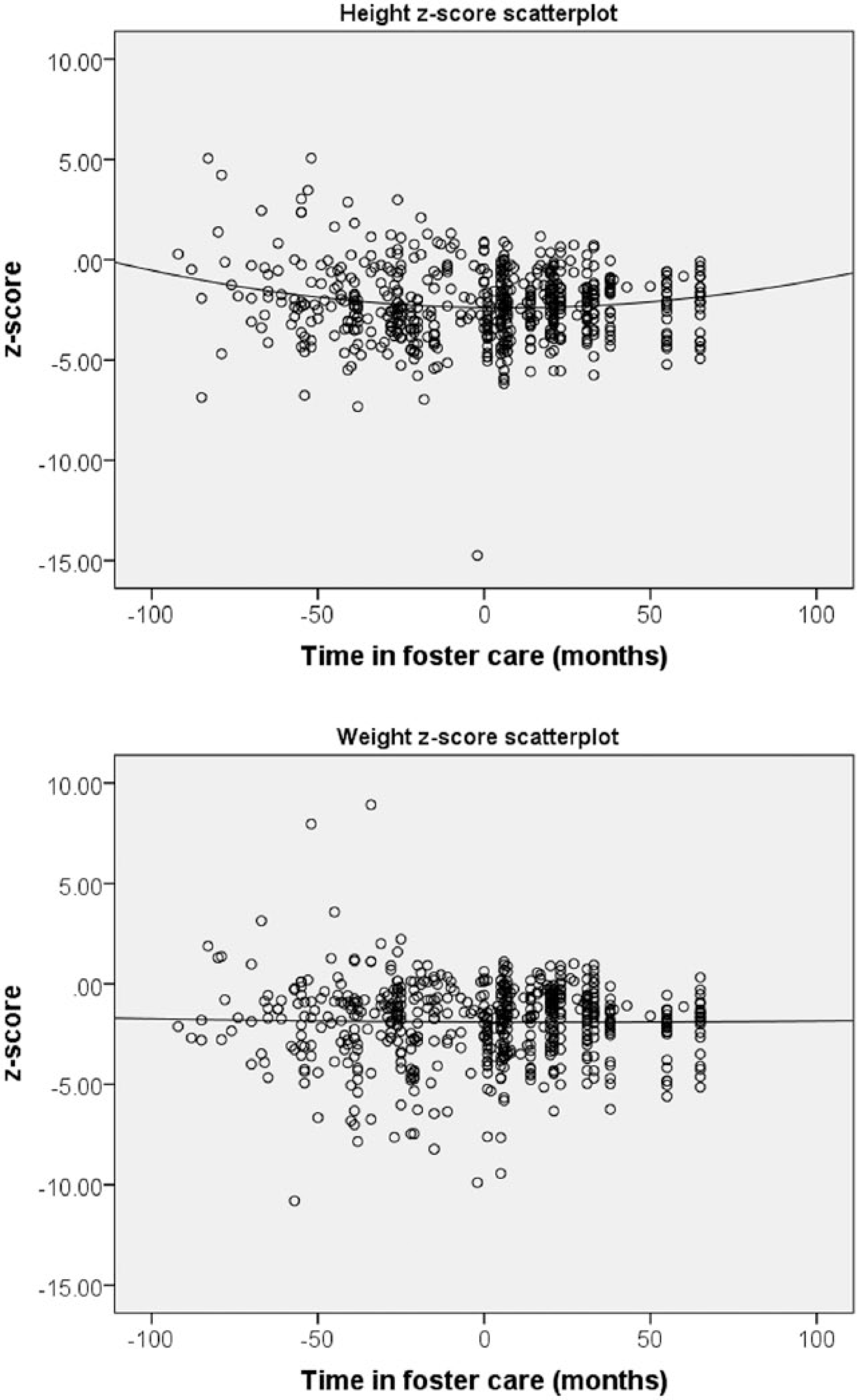
Scatterplot with regression line for children’s height and weight (families 1–24, N = 102).
Families 1–16: Height and weight versus CCSERRS
For the sample of families 1–16 that had CCSERRS assessments on their foster parents, Pearson’s correlations were calculated between children’s change in weight and height and family caregivers’ CCSERRS scores (i.e. caregiver scores, child scores, relationship scores, and the total score). Height and weight changes were calculated using the last measurement before and last measurement after foster family transition. The correlations between height change and CCSERRS child score (r(64) = .30, p = .017) and CCSERRS relationship score (r(64) = .31, p = .013) were statistically significant. The correlations between weight change and CCSERRS relationship score (r (64) = .26, p = .036) were also statistically significant. However, the correlations between weight change and CCSERRS child score (r(64) = .20, p = .115) and the correlations between height change (r(64) = .10, p = .447) and weight change (r(64) = .08, p = .512) and the CCSERRS caregiver score were all positive but not significant.
Families 1–6: Longitudinal data
For the true longitudinal sample of families 1–6, there were 23 children with at least one physical growth measurement before transitioning to foster care (baseline) and seven measurements while living with foster parents. These longitudinal data, despite the relatively few cases, allowed examination of intra-individual change in height and weight over 5.4 years of foster care. In addition, children were divided into two main age-at-transition groups: 2–6 years (n = 12) and 6–8 years (n = 11).
A one-way within-subject ANOVA was performed on height (z-scores) and separately on weight as a function of time spent in foster families. There was a significant improvement in height, F(7, 154) = 12.868, p < .001, η2 = .369, and weight, F(7, 154) = 13.938, p < .001, η2 = .388 (Figure 2), with fairly substantial effect sizes over time spent in foster families. Note, however, that growth did not improve immediately after transitioning to foster care. Specifically, during the first month after transitioning to foster care, 61 percent (14/23) of the children showed a decrease in height z-score and 30 percent (7/23) showed a decrease in weight before improvement occurred. When comparing the improvements in height and weight, the range of z-score increases between baseline and the highest z-score after intervention was larger for weight (2.20) compared to height z-score improvement (1.35). A 6 × 8 within-subject ANCOVA was performed separately on both height and weight as a function of family assignment and time of measurement, controlling for age-at-transition groups. A 3 × 8 within-subject ANCOVA was also performed separately on both height and weight as a function of age-at-transition group and time of measurement, controlling for CCSERRS relationship score. Neither analysis produced significant results, indicating that the general increasing trend during foster care was not different as a function of family or age at transition.

Height (z-score) and weight (z-score) change from baseline to 65 months postintervention (N = 23).
Discussion
This study shows that collective foster care has the potential for improving children’s physical development, which is consistent with the literature on the more widely practiced community foster care (Johnson et al., 2010). Children’s height decreased while residing in the institution but increased after being placed in foster families, with the lowest point of the curve around the time of foster family placement. This meant children’s height became more delayed compared to the standards for non-institutionalized children the longer the children remained in the institution; nevertheless, relative height improved after transitioning to foster care. However, weight did not display a statistically similar trend in the larger cross-sectional sample but did so for the smaller longitudinal sample. One factor that may have affected the weight measure was that children kept their clothes on during physical check-ups. Although staff reported that adjustments were made for clothing, the accuracy of that adjustment could not be determined.
Furthermore, the CCSERRS relationship score showed the largest positive correlation with height and weight change. This meant that the better the relationship between caregivers and children, the more improvement children showed in both height and weight. This finding is also supported by previous studies on family interventions (Johnson et al., 2010; Smyke et al., 2010). The CCSERRS caregiver score had a weaker correlation with physical growth than the relationship score. One possible explanation is that the CCSERRS observations were not distributed evenly over different activities, and some activities (i.e. free play) may require less caregiver involvement compared to other activities (i.e. feeding). The relationship rating may be less influenced by activity differences.
When we conducted analyses on longitudinal height and weight change of 23 children from families 1–6, we found that both their height and weight improved significantly while being cared in foster families. Which family a child lived with did not have a significant effect on the children’s weight and height improvement, perhaps because all six foster parents provided high quality of care to children; specifically, 98 percent of all CCSERRS items across different settings for those six families were in the 2–3 range.
Previous literature on institutionalized children indicated that the maximum gains for intervention occur in the first 12 months of life (Johnson and Gunnar, 2011). Although our longitudinal data analysis (families 1–6) found that children’s age at family entry was not significantly associated with their weight and height improvement, both the weight and height curves showed that the younger group (ages 2–6) started with a higher z-score and remained essentially a constant amount higher than the older group (ages 6–8). These data plus the existing literature (Johnson and Gunnar, 2011) suggest that institutions should consider placing children in family environment as young as possible.
Children’s height growth rates did not improve immediately (i.e. in the first month) after being placed in foster families (see Figure 2). Specifically, 61 percent of the children dropped in height z-score during the first month in foster families. A drop in such scores indicated that these children were growing at a rate slower than would be expected of same-age mates who were reared in families. These initial drops in height appear to contradict Miller et al.’s (2010) finding, which showed that most children improved in physical growth during the first 6 months after adoption. In addition to the fact that Miller used a 6-month instead of the current 1-month time span after placement, it is possible that an initial drop reflects a short period of adjustment to a substantial transition to a new living arrangement, peers, and caregivers. Prior studies found that Institutionalized young children’s Battelle developmental scores plateaued or did not rise as much during a span of time in which children were transitioned to a new group of peers and caregivers (McCall et al., 2010, 2012). An important implication of this finding is that future researchers and evaluators of new living interventions may need to allow children enough time for adjustment before determining program effectiveness.
Limitations
This study was a field evaluation of an existing program, and we were not able to create a comparison group. However, the observation that children of a great diversity of ages displayed relatively slower growth rates while residing in the institution before being transitioned to foster care strongly suggests that an institutional comparison group would likely display the same declining trend in contrast to the rising trend observed during foster care. Second, due to limited resources and our involvement in the project after the foster care environment had been created and implemented, we were only able to collect existing physical and other data from children’s institutional records (physical growth data that consisted their height and weight). In our experience with international institutional records, this institution and foster care program had relatively organized and complete records of the children’s physical growth, but we had no check on their accuracy. Nevertheless, their advantage was the existence of measurements before the foster care intervention was begun.
Third, the generality of the findings is limited due to the unique design of collective foster care. Children in this program were selected for, rather than randomly assigned to, foster placement, and some children were selectively adopted out of foster care. Furthermore, children with the most severe disabilities were not placed into foster care. Also, unlike community foster care, all foster parents were closely monitored by professionals and all the children continued to receive education and physical care in their familiar institutional environment. However, the results are consistent with both the one random assignment study of a highly professional foster care system in Romania (Johnson et al., 2010) and a review of literature of foster care as typically practiced (Julian and McCall, 2011) in showing the superiority of foster children’s development relative to those in traditional institutions.
Implications for practice
This study has several implications of institutional and collective foster care for children. First, the quality of relationship between caregivers and children moderates children’s physical development. Therefore, the quality of caregiver–child interactions and relationships needs to be emphasized and closely monitored in any care arrangements, which includes providing frequent trainings on relationship-based care to foster parents and institutional staff. Second, the initial drop in children’s height after transitioning to foster care implies that practitioners, researchers, and evaluators may need to allow children enough time to adjust to new environments before determining program effectiveness. Third, children’s height decreased while residing in the institution and their height and weight increased after transitioning to foster families. This means that, compared to institutional care, foster care as practiced here better supports children’s healthy development, but the quality of care is important in any caregiving context. Finally, although children in our study improved in height and weight after receiving foster care despite their age at transition, their height and weight do not reach the median CDC standards even at their highest points. This may be related to the older ages at which these children were transitioned to foster care. Therefore, we would recommend institutions place children into family arrangements as young as possible.
Future directions
There is currently limited research on the nature and quality of foster care and the development of foster children in low-resource countries. Therefore, we encourage systematic collection of caregiver–child interaction and child-development data in both institutional and foster care internationally. To our knowledge, China is currently implementing a variety of foster care models without collecting systematic measurements on children’s development. It is essential to have empirical evaluations conducted on those foster programs to determine their impacts on the children enrolled and their performance on the intended outcomes. Besides measuring children’s overall development, researchers also need to examine at least three additional areas in those studies. First, a better understanding of how children’s characteristics affect their levels of improvements in foster care is needed. The child characteristics that researchers need to address in their studies include, but are not limited to, the children’s age, disabilities, and length of stay in the institutions. Second, in order to recruit the most appropriate parents for children currently receiving institutional care, the foster care programs need to know more about how the foster parents’ background (including prior childrearing experience, age, educational background, and social/economic status) affect their performance as caregivers. Third, the field needs to have a better understanding of the cost efficiency of programs, for example, the maximum number of children that each foster family could care for without affecting the quality of care. The program may also want to know the number of foster care units each program needs to have to be cost efficient. Such information will not only advance our knowledge in foster care, orphan care, and child development, but it will also allow practitioners and policy makers to design and implement the foster care programs that best support the development of orphans in China.
Footnotes
Funding
This evaluation study was supported by a grant to McCall from the Society for the Psychological Studies of Social Issues of the American Psychological Association, the Chongqing Child Welfare Institute, and the University of Pittsburgh.