
Abstract
This systematic review examines the relationship between acculturation and health behaviors in African Americans. To meet inclusion criteria, studies published in English had to examine the relationship between acculturation and a health behavior among African Americans of any age (including children and adults). Twenty-one studies met criteria for inclusion. Studies assessed the relationship of acculturation to one or more of six different health behaviors: tobacco use, alcohol use, illicit drug use, risky sexual behavior, health-promoting behaviors (e.g., physical activity), and cancer screening. Although some studies found that a traditional African American orientation was associated with unhealthy behaviors, other studies found the opposite or no relationship. Also, for several health behaviors, only one or two studies were available, making it difficult to make definitive conclusions about the relationship of acculturation to these health behaviors. Thus, findings should be considered preliminary. Studies examining the relationship between acculturation and health behaviors among African Americans are needed.
In the United States, African Americans are disproportionately represented in myriad adverse health outcomes, and experience higher rates of disease, disability, and death for many health conditions in comparison with non-Hispanic Whites (Centers for Disease Control and Prevention, 2013). This includes higher mortality from cancer and cardiovascular disease (DeSantis, Naishadham, & Jemal, 2013; Pearson et al., 2013). In addition, more than 75% of African Americans in the United States are overweight or obese, and they account for close to half of incident HIV infections, while representing only 14% of the population (An, 2014; Laffoon, Satcher Johnson, Cohen, Hu, & Shouse, 2011; Rastogi, Johnson, Hoeffel, & Drewery, 2011).
Although there are multiple contributors to the adverse health outcomes experienced by African Americans, they are, in part, the result of health behaviors. For example, African Americans are more likely to use menthol cigarettes, which have been shown to have higher carbon monoxide concentrations than regular cigarettes, in comparison with non-Hispanic Whites, and are less successful in quitting smoking (Jones, Apelberg, Tellez-Plaza, Samet, & Navas-Acien, 2013; Trinidad, Pérez-Stable, White, Emery, & Messer, 2011). In addition, African Americans engage in physical activity at a lower rate than non-Hispanic Whites and have been shown to consume significantly fewer fruits and vegetables (Centers for Disease Control and Prevention, 2014; Grimm, Foltz, Blank, & Scanion, 2012). Also, HIV-positive African American men who have sex with men (MSM) are less likely to take antiretroviral therapy in comparison with HIV-positive non-Hispanic White MSM (Millet, Flores, Peterson, & Bakeman, 2007), perhaps contributing to the higher incidence of HIV among African Americans.
Acculturation provides a framework within which the health behaviors of ethnic minority or cultural groups can be explored, and may provide insight into the health disparities experienced by African Americans. The present review used the following definition of acculturation from the anthropology literature: [Acculturation is] culture change that is initiated by the conjunction of two or more cultural systems. Acculturative change may be the consequence of direct cultural transmission; may be derived from non-cultural causes, such as ecological or demographic modification by an impinging culture; it may be delayed, as with internal adjustments following upon the acceptance of alien traits or patterns; or it may be a reactive adaptation of traditional modes of life. (Social Science Research Council, 1954, p. 974)
The study of acculturation may help demonstrate how African American culture impacts health behaviors among African Americans. Furthermore, the study of acculturation has potential to highlight the heterogeneity of this ethnic group. Within the acculturation framework, a priori hypotheses can be developed and tested about the relationship of engagement in African American culture to health behaviors, and differences in health behaviors among African Americans can be examined.
Prior to the 1990s, the study of acculturation had been applied to many ethnic minority groups, yet no research had been conducted among African Americans (Landrine & Klonoff, 1996). Landrine and Klonoff (1996) argued that this occurred because (a) the field of psychology assumed that African Americans lack a culture because it was lost during slavery, and (b) African Americans have been typically regarded as a racial group and not as an ethnic group by the psychology field. Viewed as a racial group, physical differences were the focus of study; physical differences were used to explain differences seen in behavior within and across racial groups. On the contrary, for ethnic groups, cultural differences were the focus of study; cultural differences were used to explain differences seen in behavior within and across ethnic groups (Landrine & Klonoff, 1996). The concept of acculturation, which focuses on cultural differences, thus was not applied to African Americans because they were traditionally viewed as a racial group (Landrine & Klonoff, 1996). In addition, according to Parham, White, and Ajuma (1999), in the late 1950s and early 1960s, the deficit-deficiency model was used to suggest that environmental factors (e.g., racism, discrimination) were responsible for making African Americans deficient in several areas (e.g., intelligence, perceptual skills). From this model, a cultural deprivation hypothesis was formed, whereby African Americans were believed to lack a culture because they were not sufficiently exposed to Euro-American values and norms (Parham et al., 1999).
However, African Americans do indeed have a distinct culture that has developed from a unique history in the United States. Other social science fields such as anthropology and sociology have studied African American culture for several decades (e.g., Abrahams, 1970; Hersvokits, 1941; Magubane, 1987). Parham et al. (1999) argued that a change occurred in the psychology field, and African American culture became a focus of study with the rise of the multicultural model. The multicultural model “assumes and recognizes that each culture has strengths and limitations, and rather than being viewed as deficient, differences among ethnic groups are viewed simply as different” (Parham et al., 1999, p. 8). Parham et al. noted that within a multicultural framework, researchers began to focus on culture-specific models. The discipline of Black psychology emerged as a discipline to study the behaviors and culture of African Americans in a nonracist way (Parham et al., 1999). The study of acculturation among African Americans is an area within Black psychology that attempts to understand the impact of this dynamic process.
The acculturation literature has been critiqued for the assumption that acculturation is a phenomenon restricted to immigrant populations (Chun & Akutsu, 2003; Horevitz & Organista, 2013). A recent article on the construct noted that the process of acculturation may be particularly important for “visible-minority” individuals, even if they did not migrate to the United States themselves (Schwartz, Unger, Zamboanga, & Szapocznik, 2010). The assumption that the study of acculturation should be limited to immigrant populations stems from the belief that ethnic groups that reside in the United States, such as African Americans, do not have a unique culture that is distinct from the dominant American culture. African American culture, however, is unique from the dominant American culture in the United States. For example, in a qualitative research study among 53 African Americans, participants described food preferences among African Americans that were considered distinct from those of White Americans and linked to a sociopolitical history of African Americans in the United States (Airhihenbuwa et al., 1996). Participants also discussed particular uses assigned to foods among African Americans. For example, “pot liquor,” which was defined as “the juice from the greens that has all the vitamins in it that you don’t directly get from greens,” was noted to be given to adults who were sick or to infants as baby food. The authors (Airhihenbuwa et al., 1996) of the qualitative study noted, In fact, for African Americans, in the absence of more overt cultural symbols (language, dress or foods that are exotic in the American dietary context), maintaining cultural identity may involve perpetuating or creating subtle, private connotations of otherwise shared phenomena. (p. 246)
Thus, although soul food (e.g., greens) may be widely available in the United States, there are cultural meanings assigned to these foods that are unique to African American culture. Participants in the study also described cultural norms associated with food, for example, the symbolism of the kitchen as a private space (Airhihenbuwa et al., 1996). It was noted that entering someone’s kitchen without permission was disapproved of in the African American community. These food-related traditions and norms are examples of African American culture. Similar to an immigrant coming to the United States, African Americans have a unique culture that is distinct from the dominant White American culture that can, at times, result in discordance. Among African Americans, this discordance does not merely represent intergroup issues between minority and majority groups in the same society, but rather acculturation issues resulting from cultural differences between African Americans and the dominant American culture.
Models of Acculturation
Conceptualizations of acculturation have represented the construct with unidimensional, bidimensional, and multidimensional models. Acculturation was originally conceptualized as a unidimensional process, with retention of one’s native culture at one end of the continuum, and adoption of a new culture at the opposite end (Cabassa, 2003; Lara, Gamboa, Kahramanian, Morales, & Bautista, 2005). The acquisition of a new culture was believed to parallel the loss of one’s native or heritage culture. Measures following a unidimensional model may consider cultural behaviors, attitudes, and beliefs when evaluating level of acculturation (Cabassa, 2003), but these measures typically utilize a total score, assuming that level of acculturation will be similar across these potentially disparate domains. Furthermore, measures based on the unidimensional model of acculturation force respondents to select between two cultures assuming that an individual is incapable of maintaining aspects of one’s native culture while also adopting a new culture. In addition, researchers using a unidimensional model of acculturation have often relied on proxy indicators to assess acculturation. Proxy indicators have been critiqued for their simplistic conceptualization of the construct that typically follow a linear trajectory (Horevitz & Organista, 2013). Furthermore, several of the most commonly used proxy indicators of acculturation, such as place of birth, years lived in the dominant culture, and language preference, cannot be used to study the construct among African Americans because, for the vast majority, their place of birth is in the same country (i.e., United States) as where the dominant/majority culture resides, and African Americans predominantly speak English, the primary language used in the United States (Ryan, 2013; United States Census Bureau, 2007).
In contrast to the unidimensional model, the bidimensional model of acculturation proposes that the acquisition of behaviors, attitudes, and beliefs from a new culture does not require the loss of one’s native culture. Rather, immersion into the dominant culture and participation in one’s culture of origin are characterized as two independent dimensions (Cabassa, 2003). Measures that follow a bidimensional model typically incorporate measurement of two major domains, one of which reflects immersion in a new culture and another that reflects retention of one’s native culture. A commonly used bidimensional model of acculturation is Berry’s model (Berry, 1980). Berry’s model of acculturation proposes that the two dimensions of the bidimensional model yield four possible acculturation typologies. The separation typology describes individuals who engage with the heritage culture and have minimal engagement with the mainstream culture. The assimilation strategy describes individuals who have minimal engagement with the heritage culture but engage with mainstream culture. Marginalization describes individuals who minimally engage in both the heritage and mainstream culture. The integration typology refers to individuals who engage in both the heritage and mainstream culture (Berry, 1980). The bidimensional model has been considered superior to the unidimensional model because it does not make the zero-sum assumption that immersion into the dominant culture requires loss of one’s native culture (Cabassa, 2003). However, the bidimensional model, like the unidimensional model, still has the shortcoming of collapsing potentially disparate acculturation domains into summary scores that preclude understanding of more specific cultural influences.
Finally, a multidimensional model of acculturation has been presented as an alternative to the unidimensional and bidimensional models (Abraído-Lanza, Armbrister, Flórez, & Aguirre, 2006). The multidimensional model conceptualizes multiple acculturation-related domains as potentially orthogonal, and underscores the importance of measuring each domain independently. For example, multidimensional measures of acculturation might simultaneously assess a variety of cultural behaviors, attitudes, and beliefs in separate subscales. In this multidimensional approach, an individual may be highly acculturated in their media and music preferences but have a low level of acculturation in regard to their social affiliations. Proponents of a multidimensional approach have called for the use of latent modeling techniques to advance the study of acculturation and health (Abraído-Lanza et al., 2006). Latent variables of acculturation allow for acculturation profiles to be created based on simultaneous measurement of multiple acculturation-related dimensions (e.g., social affiliation, media preferences, religious beliefs). These acculturation profiles can then be examined in relationship to health outcomes, for example, permitting assessment of how individuals who fit in certain acculturation profile groups (e.g., low social affiliation, high preference for African American media, and low religiosity versus low social affiliation, low preference for African American media, and high religiosity) may exhibit different health behaviors.
Numerous measures of acculturation have been developed based on these different models (Horevitz & Organista, 2013). The acculturation literature has been critiqued for the proliferation of acculturation measures, and in particular measures that do not present a clear operationalization of the construct and use proxy indicators or unidimensional and bidimensional models of the construct (Doucerain, Segalowitz, & Ryder, 2016). Multidimensional measures of acculturation developed for particular ethnic groups provide data that are more culture specific. Furthermore, culture-specific multidimensional measures allow for the study of mechanisms underlying the process of acculturation among particular ethnic groups (Doucerain et al., 2016).
Measures of Acculturation for African Americans
Unfortunately, there are few measures available to assess acculturation specifically among African Americans. The most widely used measures of acculturation for African Americans are the unidimensional African American Acculturation Scale developed by Snowden and Hines (1999), and the similarly named, but multidimensional, African American Acculturation Scale (Landrine & Klonoff, 1994) and its revised version, the African American Acculturation Scale–Revised (Klonoff & Landrine, 2000) developed by Landrine and Klonoff. To minimize confusion, the scale developed by Snowden and Hines will be referred to as the S&H-AAAS, and the original and revised version of the scale developed by Landrine and Klonoff will be referred to as the L&K-AAAS and L&K-AAAS-R. The S&H-AAAS is a 10-item self-report measure that was designed to assess immersion in African American social settings and interaction with African American culture (e.g., media preferences, social interaction patterns, and attitudes). The S&H-AAAS utilizes a unidimensional model of acculturation and produces a total score, presuming individuals range from having low to high levels of acculturation to the dominant culture in the United States. In contrast, the L&K-AAAS is a 74-item self-report measure that examines aspects of African American culture. A revised, shortened version of the scale was developed in response to criticism that some items were offensive; this resulted in 26 items (e.g., “I know how to play bid whist”) being dropped from the measure. After a principal components analysis of the remaining 48 items, one additional item was dropped, resulting in the L&K-AAAS-R, a 47-item measure with eight subscales (Religious Beliefs and Practices, Preference for Things African American, Interracial Attitudes, Family Practices, Health Beliefs and Practices, Cultural Superstitions, Segregation, and Family Values). A less widely used measure of acculturation for African Americans is the Measurement of Acculturation Strategies for People of African Descent (Obasi & Leong, 2010). The 45-item measure assesses acculturation bidimensionally among people of African descent living in the United States. Dimension 1 (D1) examines an individual’s maintenance of African ethnocultural heritage. Dimension 2 (D2) assesses an individual’s participation in Eurocentric, United States culture.
Although the S&H-AAAS (Snowden & Hines, 1999), the L&K-AAAS (Klonoff & Landrine, 2000; Landrine & Klonoff, 1994), and the Measurement of Acculturation Strategies for People of African Descent (Obasi & Leong, 2010) have all been shown to have strong psychometric properties, many studies have utilized self-developed measures to assess acculturation in African Americans, or have modified existing measures, precluding cross-study comparisons. Also, there are acculturation measures available that are designed to be used across ethnic groups, including African Americans, such as the Scale of Ethnic Experience (Malcarne, Chavira, Fernandez, & Liu, 2006), the Majority–Minority Relations Survey (Sodowsky, Lai, & Plake, 1991), and the Stephenson Multigroup Acculturation Scale (Stephenson, 2000). However, the study of acculturation among African Americans may be best conducted using a measure developed specifically for African Americans. An ethnic group–specific measure allows for more detailed coverage of aspects particular to African American culture (e.g., cuisine, superstitions, health beliefs, celebration of holidays). In addition, the study of acculturation among African Americans is unique given the history of slavery, forced segregation, and continued discrimination imposed on this ethnic group in the United States and its resulting social, economic, and health disparities (Watts, 2003). Furthermore, some of the measures that are designed to be used across ethnic groups (e.g., the Majority–Minority Relations Survey [Sodowsky et al., 1991], Stephenson Multigroup Acculturation Scale [Stephenson, 2000]) still contain items assessing use of the English language, which is not highly relevant to the study of acculturation among African Americans.
Acculturation and Health Behaviors
Researchers have theorized about the relationship between acculturation and health behaviors among African Americans, and higher levels of acculturation have been hypothesized to be associated with both health protective and health risk behaviors (Landrine & Klonoff, 1996; Nasim, Corona, Belgrave, Utsey, & Fallah, 2007). Landrine and Klonoff (1996) suggested that more traditional African Americans engage in more health risk behaviors because traditional African Americans may be perceived as more “stereotypically ‘Black’ than their acculturated counterparts” (p. 95). As a result, they may experience more racial stress and cope with this stress by engaging in unhealthy behaviors (e.g., substance use). However, others have suggested that adherence to African American culture may serve as a protective factor for health (Nasim et al., 2007). Traditional African American values and norms include a collectivistic orientation (e.g., familial interdependency) and religiosity, both of which have been found to serve a protective function against unhealthy behaviors such as substance use (Nasim et al., 2007). Furthermore, a collectivistic orientation may be protective against unhealthy behaviors because a collectivistic orientation considers the impact of health decisions on family or the larger community (Nasim et al., 2007).
It remains unclear how degrees of engagement in African American culture and adoption of the dominant/majority culture in the United States are associated with health behaviors among African Americans. This systematic review, the first to examine the relationship between acculturation and health behaviors in African Americans, synthesizes the current literature, and identifies whether more or less acculturated African Americans are at higher risk for engaging in specific adverse health behaviors. Researchers have called for community-based culturally tailored interventions to improve health in the African American community (Plescia, Herrick, & Chavis, 2008; Shaya, Gu, & Saunders, 2006). Most intervention programs aimed at changing health risk behaviors that have been developed have predominantly focused on middle-class, non-Hispanic White populations (Plescia et al., 2008). Intervention programs are needed that specifically target the health needs of the African American community. Identifying those African Americans at most risk for engaging in unhealthy behaviors is a first step in developing effective community intervention programs promoting African American health.
Method
Search Strategy
Both electronic and manual searches were conducted. Complete databases from PubMed/MEDLINE (1946 to present), PsycINFO (1887 to present), and CINAHL (1982 to present) were searched on October 15, 2015. These databases were broadly searched for English-language studies using the following search terms: (African American* OR Blacks) and acculturat*. Subsequently, reference lists of all articles that met selection criteria were screened for potential inclusion. Gray literature such as conference abstracts and dissertations were excluded.
Study Selection
Two investigators (S.D.M. and S.G.) evaluated studies for potential inclusion. Duplicate publications were removed prior to being screened for inclusion. Abstracts were initially reviewed to identify potentially relevant articles. Full articles were then screened to determine eligibility for inclusion in the review. To meet inclusion criteria, studies published in English had to examine the relationship between acculturation and a health behavior among African Americans of any age (including children and adults). Acculturation was broadly defined as a process of cultural and/or psychological change resulting from contact with a culture distinct from one’s own. To be included, studies needed to measure acculturation among African Americans with either a validated or nonvalidated scale; studies that examined acculturation via proxy variables, such as generational status, were excluded. Because ethnic identity is considered a distinct construct from acculturation, with ethnic identity reflecting conscious endorsement of membership in a particular group, and acculturation reflecting degree of orientation to more than one culture, studies that used measures of African American ethnic identity rather than acculturation were excluded (Tsai, Chentsova-Dutton, & Wong, 2002). Health behavior was broadly defined as an action that impacts one’s own health. Studies relating acculturation to mental health were excluded. In addition, studies with participants who self-identified as Black Hispanic, Caribbean, Afro-Caribbean, or African (not African American) were considered distinct from African Americans, and were thus excluded from the review. Previous research has discussed the different historical contexts (especially immigration vs. slavery) of these ethnic groups that have, in turn, resulted in distinct psychosocial and cultural experiences (Hunter, 2008; Waters, 1994). Thus, in an effort to focus on the specific cultural experiences of African Americans, and their relationship to health behaviors, the present review did not include studies of other ethnic groups with likely some overlapping, but also distinct, acculturation processes. Studies with ethnically mixed groups (e.g., Black Hispanics and African Americans) were excluded unless the study analyzed data for African Americans separately from the total sample.
Data Extraction and Assessment of Studies
A data extraction sheet was developed by the first author. The following information was extracted from all studies that met inclusion criteria: (a) sample characteristics (age, sex, total sample size, African American sample size, and location of study), (b) assessment of acculturation (measure used), (c) health behavior, and (d) direction of association between acculturation and health behavior. Then, standardized effect sizes (Cohen’s d) were calculated to examine the strength of the relationship between acculturation and health behaviors based on statistical values and descriptive statistics provided in all studies meeting review criteria.
An assessment of methodological quality was performed; see Table 2 for the list of criteria employed. A slightly adapted version of an evaluation rubric previously developed for a systematic review was used (Zhang & Wang, 2008). The original method evaluates studies across 10 criteria, but one of the criteria asked about language used when conducting study interviews. This criterion was removed because it was not relevant for this review, leaving nine methodological quality criteria that were evaluated for each study. Studies were reviewed for methodological quality only after meeting all inclusion criteria, as opposed to conducting an assessment of quality prior to inclusion.
Results
Search Results
The search process yielded 810 unique titles (see Figure 1). Twenty-one articles met all inclusion criteria for this review (see Table 1). Articles were most often excluded because they did not include African Americans or did not measure acculturation among African Americans. Studies relating acculturation to six health behaviors were identified: smoking, alcohol use, illicit drug use, risky sexual behavior, health-promoting behaviors (e.g., diet, physical activity), and cancer screening. For each health behavior, results from studies were summarized when the same acculturation measure was used across studies. When acculturation was assessed using different measures, results were presented separately. For some health behaviors, only a single study was identified in the review. The studies discussed in each health behavior category used different participant samples unless indicated.
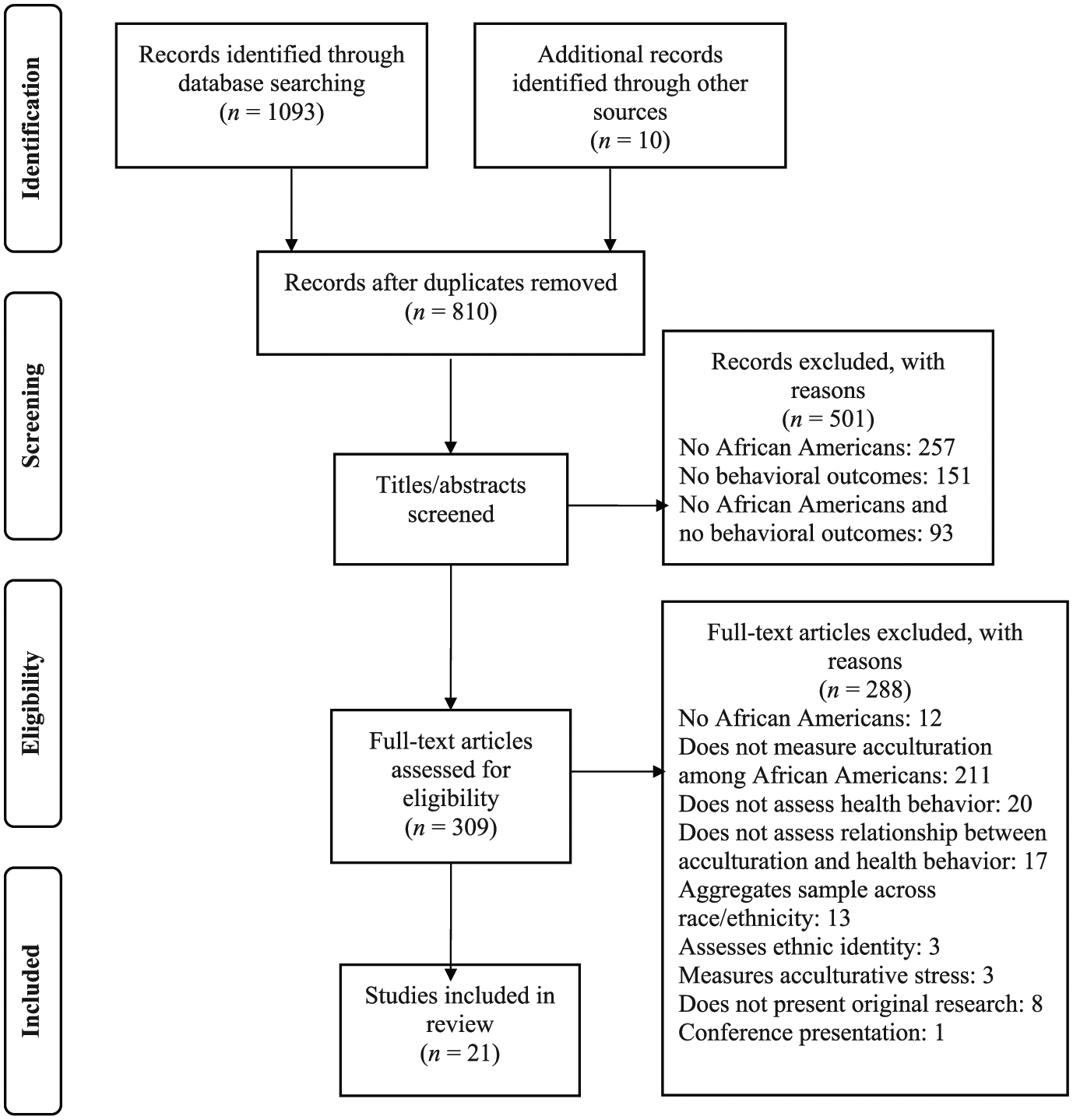
PRISMA diagram illustrating study identification and selection.
Health Behaviors
Smoking
Nine studies examined the relationship between acculturation and smoking in African Americans (Fernander, Schumacher, & Nasim, 2008; Fernander, Schumacher, Wei, Crooks, & Wedlund, 2008 1 ; Guevarra et al., 2005; Hooper, Baker, Ybarra, McNutt, & Ahluwalia, 2012; Klonoff & Landrine, 1996, 1999a; Landrine & Corral, 2014; Landrine & Klonoff, 1996; Nasim et al., 2007). Four of these studies measured acculturation with the total score of the L&K-AAAS (Landrine & Klonoff, 1994) or its revised version (L&K-AAAS-R; Klonoff & Landrine, 2000). In these four studies, with a combined sample of 1025 African American adults, smokers reported being more traditional while nonsmokers were more acculturated (Guevarra et al., 2005; Klonoff & Landrine, 1996, 1999a; Landrine & Klonoff, 1996). In addition, the relationship between acculturation and smoking status remained the same after controlling for education and income (Klonoff & Landrine, 1996, 1999a). Select L&K-AAAS and L&K-AAAS-R subscales were significantly associated with smoking status, in the expected directions.
Three studies only examined subscale scores of the L&K-AAAS or L&K-AAAS-R, as opposed to the total score (Fernander, Schumacher, & Nasim, 2008; Fernander, Schumacher, Wei, et al., 2008; Nasim et al., 2007). In two of these studies, opposing relationships were found between acculturation and smoking or smoking risk, depending upon which L&K-AAAS-R subscales were examined (Fernander, Schumacher, & Nasim, 2008; Nasim et al., 2007). In a study of 96 African American female smokers, no significant differences in level of acculturation were found among heavy and light smokers (Fernander, Schumacher, Wei, et al., 2008).
One study of 2118 African American men and women measured acculturation using three items of the L&K-AAAS (i.e., frequency of reading African American magazines and newspapers, frequency of watching African American television shows, and frequency of attending African American community events; Landrine & Corral, 2014). Controlling for income, employment, and education, there was a significant relationship between acculturation and current smoking status. Participants with a low level of acculturation were more likely to be current smokers (OR = 1.81, p = .013). When analyses were conducted for men and women separately, the significant association between acculturation and current smoking status remained only for women.
Another study compared the impact of a cognitive behavioral therapy (CBT) for smoking cessation intervention with a general health education group among 140 African American smokers (Hooper et al., 2012). The L&K-AAAS-R was used to assess acculturation. Participants (age: M = 44.4 years, SD = 9.62) were predominantly female (79%), and the majority had an income less than US$10,000. On average, participants smoked 13.7 cigarettes per day at baseline. The independent effects of sociodemographic variables, nicotine dependence, and acculturation on 7-day point prevalence abstinence were assessed using hierarchical linear regression for the total sample. After the 6-week counseling intervention, and at 3-month follow-up, the L&K-AAAS-R total score was the only significant predictor of smoking cessation. More traditional African Americans (i.e., less acculturated) were less likely to have quit smoking in comparison with less traditional African Americans. Acculturation was not a significant predictor of smoking cessation at 6-month follow-up.
Alcohol use
Two studies examined the relationship between acculturation and alcohol use among African Americans (Abdullah & Brown, 2012; Klonoff & Landrine, 1999b, 2000). 2 Klonoff and Landrine (1999b, 2000) used the total score of the L&K-AAAS-R to measure acculturation in 520 African American men and women (age: M = 28.2 years, SD = 10.01). Those who abstained from alcohol were more traditional compared with those who consumed one or more drinks in an average week.
Abdullah and Brown (2012) used the Measurement of Acculturation Strategies for People of African Descent (Obasi & Leong, 2010) to measure acculturation among a sample of 203 predominantly female (65.2%), African American undergraduate students (age: M = 20.34 years). Hierarchical linear regression was used to examine the relationships of acculturation, religiosity, and gender to alcohol use frequency. There was a significant two-way interaction (D1 × D2; β = .22, p = .049). The authors interpreted this interaction as suggesting that participants who rejected both African American and mainstream United States culture (marginalization group) used alcohol less frequently in comparison with African Americans who favored participation in Eurocentric United States culture (assimilation group).
Illicit drug use
The relationship between acculturation and illicit drug use was examined in a cohort of 637 Puerto Rican and 695 African American adolescents in Grades 7 to 10 living in East Harlem, New York (Brook, Whiteman, Balka, & Hamburg, 1992; Brook, Whiteman, Balka, Win, & Gursen, 1997). Participants’ drug use was assessed once at baseline (Time 1) and again 5 years later (Time 2). Drug use was categorized into four levels. The lowest level consisted of no drug use. The next highest level consisted of legal drug use (i.e., alcohol and tobacco). The third level consisted of marijuana use but no use of other illegal drugs. At the highest level, illicit drugs other than marijuana (e.g., cocaine, crack, angel dust) were used. African American acculturation was measured using a questionnaire assessing engagement in African American activities developed for the study; however, individual items from the measure were not provided. Engagement in African American activities was not significantly correlated with drug use level at Time 1 or at Time 2 (Brook et al., 1992; Brook et al., 1997).
Nasim et al. (2007) examined the relationship between acculturation and marijuana use in a sample of 145 young adult African American women. Using multivariate analyses, the Traditional Religious Beliefs and Practices (OR = 0.38, 95% confidence interval [CI] = 0.19, 0.76) and Attitudes of Cultural Mistrust (OR = 0.51, 95% CI = 0.26, 1.00) subscales of the L&K-AAAS-R were each negatively associated with marijuana smoking. Specifically, higher levels of acculturation in these two domains were associated with not using marijuana. On the contrary, the Traditional Health Beliefs and Practices subscale (OR = 3.90, 95% CI = 1.74, 8.75) was positively associated with marijuana use, indicating that a more traditional orientation in the Traditional Health Beliefs and Practices domain was associated with using marijuana.
In a study of African American eighth- and ninth-grade students (N = 424) living in the Southeastern United States, structural equation modeling was used to examine whether the relationship between family factors (i.e., parental monitoring, mother–adolescent relationship, and father–adolescent relationship) and substance use (i.e., cigarette, alcohol, and marijuana use) was mediated by culture- and school-related latent factors (Clark & Nguyen, 2012). The culture latent factor consisted of acculturation, racial socialization, and ethnic identity measures. Acculturation was measured using the Measurement of Acculturation Strategies for People of African Descent (Obasi & Leong, 2010). Culture was found to partially mediate the relationship between family factors and substance use, whereby culture was a protective factor against substance use (Clark & Nguyen, 2012).
Risky sexual behavior
Three studies examined the relationship between acculturation and risky sexual behavior (Hines, Snowden, & Graves, 1998; Robinson, Scheltema, & Cherry, 2005; Snowden & Hines, 1998). Two studies reported on findings using the same sample of 923 African Americans (Hines et al., 1998; Snowden & Hines, 1998), with one reporting findings among only women in the sample (Hines et al., 1998) and the other study reporting on the men (Snowden & Hines, 1998). The majority of the female and male samples were sexually active, and most participants were between 18 and 29 years old. Statistical analyses were conducted only on those reporting sexual activity in the year preceding the interview. Acculturation was measured using 10 items focused on preference for African American media and in-group relationships originally developed by Herd (1989). This measure was subsequently psychometrically validated by Snowden and Hines (1999) and called the S&H-AAAS. Risky sexual behavior in the past year was assessed via several measures: (a) condom use, (b) number of sexual partners, and (c) nonmonogamous sexual behavior. A composite variable was also created, where participants were categorized as engaged in either high-risk sexual behavior (nonmonogamous, inconsistent condom use) or low-risk sexual behavior (celibate; monogamous, used a condom; monogamous, inconsistent condom use; nonmonogamous, used a condom). Among the African American women (n = 306), in bivariate analyses, there was no significant linear relationship between acculturation and risky sexual behavior. However, in multivariate analyses, there was a significant interaction between drinking and acculturation in predicting risky sexual behavior. Highly acculturated, heavy drinkers were more likely to report risky sexual behavior in comparison with low-acculturated abstainers (Hines et al., 1998). Among the African American men (n = 245), in bivariate analyses, high-acculturated participants were less likely to report risky sexual behavior in comparison with low- and moderately acculturated participants (Snowden & Hines, 1998). In multivariate analyses, there was also a significant interaction with drinking, whereby highly acculturated, heavy drinkers were more likely to report risky sexual behavior in comparison with low-acculturated abstainers. The discrepancy between the bivariate and multivariate analyses suggests that an individual’s level of alcohol consumption impacts the relationship between acculturation and risky sexual behavior. These findings suggest that alcohol consumption may be driving the direction of the relationship between acculturation and risky sexual behavior.
Robinson et al. (2005) used a six-item self-report measure adapted from Exner et al. (1995) to examine acculturation among 163 low-income African American women (age: M = 32.2 years, SD = 8.96). The adapted measure assessed acculturation by asking about participation in African American culture, interest in issues relevant to African Americans, and ethnic pride. Risky sexual behavior was assessed (a) based on consistent versus inconsistent condom use in the past 3 months and (b) with a composite variable based on condom use and number of concurrent partners. Consistent with Hines et al. (1998), Robinson et al. found no significant linear relationship between acculturation and risky sexual behavior among African American women.
Health-promoting behaviors
Higher levels of acculturation, as measured by a modified version of the L&K-AAAS-R, were positively correlated with health-promoting behaviors in a sample of 201 older African American women (age range: 65-102 years; Baker, 2011). The L&K-AAAS-R was modified so that higher scores on the measure were associated with a less traditional African American orientation. The Health-Promoting Lifestyle Profile II (Walker, Sechrist, & Pender, 1987) was used to assess the frequency of engagement in health-promoting behaviors including health responsibility, physical activity, nutrition, stress management, interpersonal relations, and spiritual growth. Using hierarchical linear regression, acculturation was a significant predictor (p < .001) of health-promoting behaviors even after controlling for age, educational attainment, and socioeconomic status. African American older women who were more acculturated engaged in more health-promoting behaviors (Baker, 2011).
Another study examined the relationships between parents/caregivers’ acculturation and their daughters’ weight concerns and weight control behaviors, physical activity, and dietary intake (Beech et al., 2004). Parents/caregivers’ mean age was 36.7 years (SD = 8.3), and daughters’ mean age was 8.8 years (SD = 0.8). Parents/caregivers’ level of acculturation was measured using items selected from two subscales (i.e., Preference for Things African American; Family Practices and Values) of the L&K-AAAS and its short form (Beech et al., 2004). Daughters’ weight concerns and weight control behaviors were assessed using items from the elementary school version of the McKnight Risk Factor Survey (Shisslak et al., 1998). Daughters’ physical activity levels were assessed via accelerometer. Dietary intake was examined via assessments of total energy intake (kcal) and percent energy from fat per day. Parent’s scores on the Preference for Things African American subscale had small, significant, negative correlations with daughters’ unhealthy eating behaviors (r = −.16, p < .001) and small, significant, positive correlations with daughters’ total energy intake (r = .14, p ≤ .05) and percent energy from fat (r = .14, p ≤ .05). A more traditional African American parent orientation in this domain was associated with fewer unhealthy eating behaviors by their daughters, and higher total energy intake per day and percent energy from fat. Parents’ scores on the Preference for Things African American subscale were not significantly associated with daughters’ physical activity. Items from the Family Practices and Values subscale were not significantly related with any of the daughters’ health outcome variables (Beech et al., 2004).
The relationship between acculturation and fruit, vegetable, and fat intake was assessed in a sample of 238 predominantly female (73.5%), middle-aged (M = 48.7 years, SD = 9.1), college educated (49.2%) African Americans (Ard, Skinner, Chen, Alckin, & Svetkey, 2005). Participants completed the L&K-AAAS-R and two nonconsecutive, unannounced 24-hr diet recalls. Scores on the L&K-AAAS-R accounted for 10% of the variance in nutrient intake. Study results differed based on the statistical analyses used. According to the canonical correlation analysis, more traditional African Americans ate less fruit, vegetables, milk, and dairy, but more meat and nuts. More traditional African Americans also consumed more calories from fat. However, when comparing mean nutrient intake by L&K-AAAS-R acculturation score using analysis of variance, significant differences across level of acculturation were only found for calories from fat (Ard et al., 2005).
Cancer screening
The relationship between acculturation and frequency of breast self-exam was assessed in a sample of 66 African American women (age: M = 45 years; SD = 10.70) who went to an inner-city cancer-screening clinic (Guevarra et al., 2005). Acculturation was assessed using the total L&K-AAAS-R score. Women who were classified as “underperformers,” or performed a breast self-exam less than once a month, were more acculturated. Breast self-exam “overperformers,” or those who performed a breast self-exam more than once during the prior 3 weeks, reported a more traditional African American orientation (Guevarra et al., 2005).
Another study examined the relationship between mammography use and acculturation, as measured by the L&K-AAAS-R total score, in a sample of 60 African American women aged 40 and older (Bryne, Mary, & DeShields, 2011). Participants were divided into two groups based on mammography use. Group A included women (age: M = 51.03; SD = 9.52) who had never had a mammogram or whose last screening had occurred more than 2 years prior to the study. Group B consisted of women (age: M = 52.13; SD = 5.87) who scheduled contact with a healthcare provider to learn about free breast cancer screening services. Groups A and B significantly differed on level of acculturation, t(57) = −2.75, p = .01. Participants in Group A were less acculturated (L&K-AAAS-R score: M = 240.60, SD = 48.45) in comparison with participants in Group B (L&K-AAAS-R score: M = 208.31, SD = 42.24).
Sociodemographics
Seven studies in this review examined the role of sociodemographics on the relationships between acculturation and health behaviors. For smoking, three studies focused on the role of gender, and findings were not consistent (Klonoff & Landrine, 1996, 1999a; Landrine & Corral, 2014). One study found that gender did not have a significant impact on the relationship between acculturation and smoking among a sample of 444 African Americans; smokers were more traditional irrespective of gender (Klonoff & Landrine, 1996). Another study found a significant acculturation by gender interaction among their sample of 520 African Americans, but reported that this finding was due to the greater number of women, as compared with men, who reported being traditional in their study, as there were no significant differences found in smoking by gender (Klonoff & Landrine, 1999a). In a study of 2118 African Americans, logistic regression models examining the relationship between socioeconomic (e.g., income, education) and sociocultural variables (e.g., acculturation) and smoking were examined across men and women separately. Acculturation significantly predicted smoking only in the analysis among African American women (Landrine & Corral, 2014).
For alcohol use, one study examined the role of sociodemographics (Abdullah & Brown, 2012). This study found a significant three-way interaction where the relationship between acculturation and alcohol use was impacted by gender and religiosity among a sample of 203 African American undergraduate students. Among female students who reported low levels of religiosity, a high level of acculturation was protective against alcohol use. On the contrary, female students who reported high levels of religiosity had low levels of alcohol use regardless of their level of acculturation. Among male students, for those who reported high levels of religiosity, a high level of acculturation was protective against alcohol use. Among male students who reported low levels of religiosity, a low level of acculturation was protective against alcohol use.
For risky sexual behavior, one study examined the role of marital status among a sample of 245 sexually active African American men (Snowden & Hines, 1998). In this study, marital status was found to significantly impact the relationship between acculturation and risky sexual behavior. More specifically, single men who reported a moderate level of acculturation were more likely to have multiple partners as compared with (a) single men who reported a high level of acculturation and (b) married men who reported a low level of acculturation. In addition, single men who reported moderate and high levels of acculturation were more likely than married men who reported a low level of acculturation to be nonmonogamous. Also, single men who reported a moderate level of acculturation were more likely than married men who reported a low level of acculturation to engage in high-risk sexual behavior.
For drug use, two studies examined the role of sociodemographics in a cohort of 637 Puerto Rican and 695 African American adolescents (Brook et al., 1992; Brook et al., 1997). The studies assessed drug use at baseline (Time 1) and again 5 years later (Time 2). At Time 1 and Time 2, gender, age, and mother’s education level were found to have no impact on the relationship between acculturation and adolescent drug use.
Effect Sizes
Effect sizes provide a quantitative measure of the strength of a relationship. In this review, standardized effect sizes (Cohen’s d) were calculated based on statistical values and descriptive statistics provided. Effect sizes were generally moderate to large across studies, suggesting that acculturation plays a significant role in the health behaviors of African Americans. For a summary of Cohen’s d values for studies, see Table 1. Because studies in the present review utilized different models of acculturation, the utility of effect sizes to compare studies is limited.
Summary of Reviewed Studies.

Note. AA = African American; CS = cross-sectional study; L&K-AAAS-R = African American Acculturation Scale–Revised (Klonoff & Landrine, 2000); RCT = randomized control trial; LS = longitudinal study; US = United States; L&K-AAAS = African American Acculturation Scale (Landrine & Klonoff, 1996); MASPAD = Measurement of Acculturation Strategies for People of African Descent (Obasi & Leong, 2010); NR = not reported.
Quality Assessment
Studies were assessed based on nine criteria reflecting methodological quality (see Table 2) and were given 1 point for each criterion met (possible range: 0-9). The mean quality score for the 21 studies was 4.90 with a range from 3 to 7. No study received the maximum possible quality score of 9. All studies provided an operational definition of the dependent variable, and all studies provided theoretical linkages discussing the relationship between the independent and dependent variables. Few studies (9/21) reported effect sizes, and only three used random/probability sampling. The majority of studies (19/21) tested the independent variables’ reliability or validity, but few examined the dependent variable’s reliability (7/21) or validity (3/21). Most studies (17/21) used multiple/logistic regression analyses as opposed to bivariate statistical analyses.
Quality Assessment of Studies Included in Review.
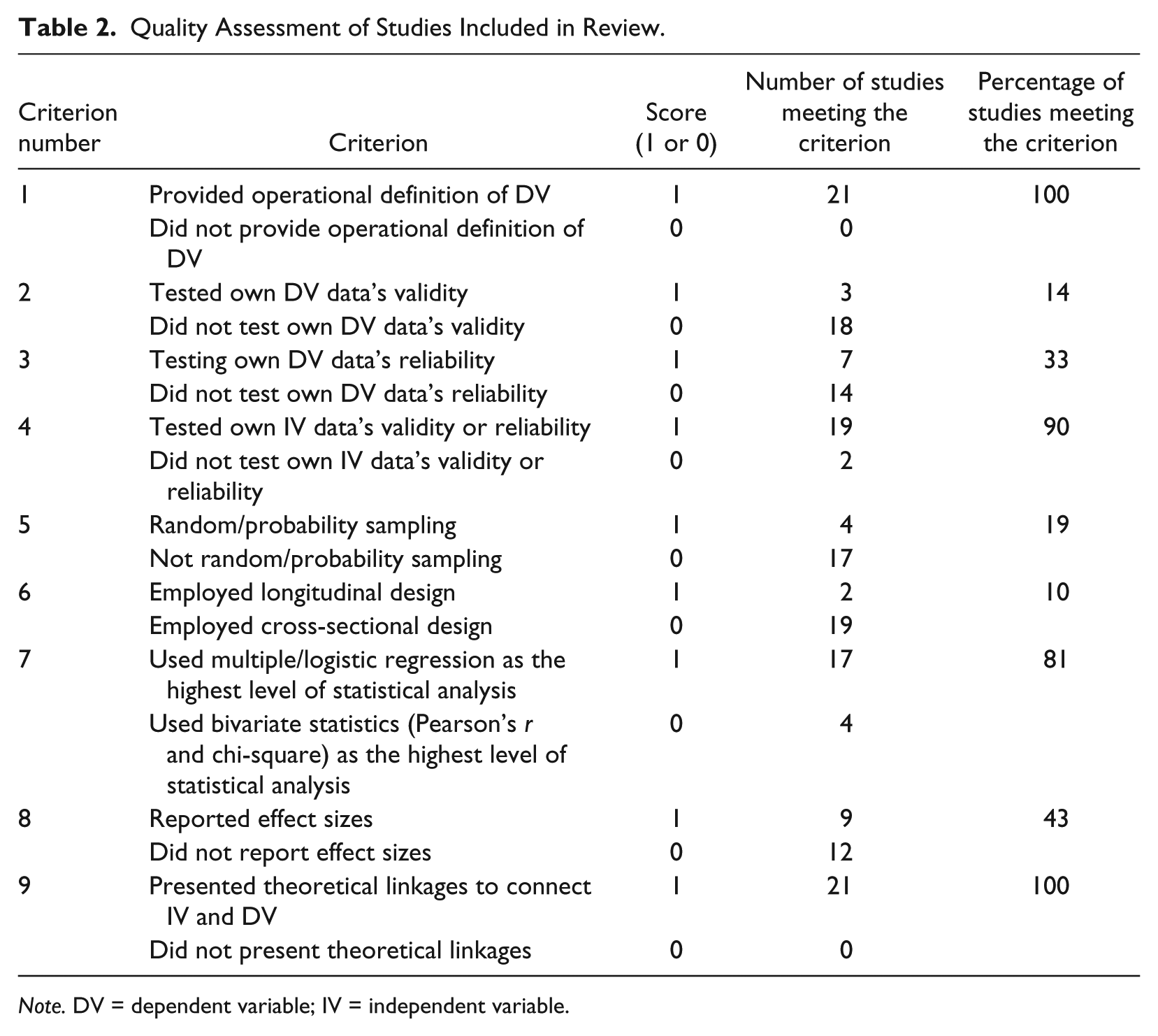
Note. DV = dependent variable; IV = independent variable.
Discussion
This systematic review examined the relationship between acculturation and health behaviors in African Americans. Twenty-one studies met criteria for inclusion, assessing the relationship between acculturation and six different health behaviors: tobacco use, alcohol use, illicit drug use, risky sexual behavior, health-promoting behaviors (e.g., physical activity), and cancer screening. For several health behaviors, only one or two studies were available, making it difficult to make definitive conclusions about relationships between acculturation and these health behaviors. In addition, studies used different models of acculturation to examine the construct, and some studies used nonstandardized measures of acculturation, or only considered select measure subscales, limiting cross-study comparison. Thus, findings should be considered preliminary and used to inform future studies.
Although some studies found that a traditional African American orientation was associated with unhealthy behaviors, other studies found the opposite or no relationship. Studies suggested that a more traditional African American orientation was associated with unhealthy behaviors such as smoking (Fernander, Schumacher, & Nasim, 2008; Guevarra et al., 2005; Hooper et al., 2012; Klonoff & Landrine, 1996, 1999a; Landrine & Corral, 2014; Landrine & Klonoff, 1996; Nasim et al., 2007), less healthy eating (Ard et al., 2005), less engagement in health-promoting behaviors (Baker, 2011), and less cancer screening (Bryne et al., 2011). Among African American men, a more traditional orientation was associated with more risky sexual behavior (Snowden & Hines, 1998).
Five studies found no significant relationship between acculturation and health behaviors. No significant bivariate relationship was found between acculturation and risky sexual behavior among African American women (Hines et al., 1998; Robinson et al., 2005). Among African American adolescents, there was no significant bivariate relationship between acculturation and drug use (Brook et al., 1992; Brook et al., 1997). Among African American female smokers, no significant differences in level of acculturation were found among heavy and light smokers (Fernander, Schumacher, Wei, et al., 2008). Another study examining the relationship between acculturation and marijuana use found mixed results among adolescent African American women, depending on which L&K-AAAS-R subscales were used (Nasim et al., 2007).
The relationship between acculturation and alcohol was unique in that a more traditional African American orientation was associated with alcohol abstinence, a health-promoting behavior, in one study (Klonoff & Landrine, 1999b). In another study, African American participants who rejected both African American and mainstream United States culture used alcohol less frequently in comparison with African Americans who favored participation in Eurocentric United States culture (Abdullah & Brown, 2012). Among African American adolescents, lower levels of acculturation were found to be protective against substance use (i.e., cigarette, alcohol, and marijuana use; Clark & Nguyen, 2012).
To make sense of inconsistent findings such as these regarding the relationship of acculturation to health behaviors, Landrine and Klonoff (2004) developed the operant theory of acculturation. The operant theory of acculturation allows for a priori predictions about changes in health behavior throughout the acculturative process based on the prevalence of health behaviors among the traditional ethnic group. The operant theory proposes that health behaviors with a high prevalence among traditional ethnic group members will decrease as one becomes more acculturated. On the contrary, health behaviors with a low prevalence among the traditional group will increase as one becomes more acculturated. For example, smoking has a high prevalence among traditional African Americans and, as expected, decreased with higher levels of acculturation. Alcohol use has a low prevalence among traditional African Americans and increased with higher levels of acculturation. Landrine and Klonoff (2004) have found support for the theory among multiple ethnic groups including African Americans, Asian Americans, and Hispanics/Latinos, and support for the theory was found in this review. The operant theory can be used to provide a more coherent framework from which to study the relationship between acculturation and health behaviors among diverse ethnic minority groups.
The majority of studies included in the present review used the L&K-AAAS or its revised version to measure acculturation. Two studies used the S&H-AAAS, and two studies used the Measurement of Acculturation Strategies for People of African Descent. Others adapted or developed a measure of acculturation for a particular study. Researchers should take caution when adapting or developing their own measures for use in a study (Schwarz, 1999). Without psychometric validation, it is unclear whether the measure reliably and validly assesses the construct of acculturation among African Americans. Furthermore, the use of a modified or nonvalidated measure limits cross-study comparison. The L&K-AAAS was the first measure of acculturation developed for African Americans, and the measure has demonstrated strong reliability and validity in several studies (Klonoff & Landrine, 2000; Landrine & Klonoff, 1994, 1995, 1996). Although strong psychometrically, the original measure consists of 74 items and the revised version has 47 items. Researchers are often limited by time, and in effort to reduce participant burden may not use a longer measure such as the L&K-AAAS. Other measures of acculturation for use among African Americans include the shorter, 10-item S&H-AAAS and the 45-item Measurement of Acculturation Strategies for People of African Descent (Obasi & Leong, 2010). Although the S&H-AAAS is brief and efficient, Snowden and Hines (1999) conceptualize acculturation as a unidimensional construct, limiting the measure’s utility. Obasi and Leong’s (2010) measure provides a bidimensional conceptualization of acculturation but is as long as the multidimensional L&K-AAAS-R. Although the present study was limited to measures of acculturation developed specifically for African Americans, there are also measures of acculturation that are meant for use across ethnic groups, as described earlier. More recently, researchers have called for measures of acculturation developed for particular ethnic groups that focus on specific aspects of that group’s culture, as this is likely to provide more culture-specific information (Horevitz & Organista, 2013). However, use of acculturation measures developed for particular ethnic groups limits comparison of study findings across ethnic groups. Studies are needed that compare the use of culture-specific acculturation measures and those developed for use across ethnic groups among African Americans. Future studies should examine whether the patterns of relationships found in the present review remain when acculturation is examined with a measure that is not culture-specific. A comparison of these measures and their relationships to health behaviors may provide additional evidence of construct validity and support for the present review’s findings.
Few studies examined the role sociodemographics play in the relationship between acculturation and health behaviors (Abdullah & Brown, 2012; Brook et al., 1992; Brook et al., 1997; Klonoff & Landrine, 1996, 1999a; Landrine & Corral, 2014; Snowden & Hines, 1998). In this review, studies examined the impact of sociodemographics on the relationships between acculturation and smoking, alcohol use, risky sexual behavior, and drug use. Studies examining the impact of gender on the relationship between acculturation and smoking were inconsistent (Klonoff & Landrine, 1996, 1999a; Landrine & Corral, 2014). The relationship between acculturation and alcohol use was impacted by gender and religiosity in one study (Abdullah & Brown, 2012). In another study, the relationship between acculturation and risky sexual behavior was impacted by marital status (Snowden & Hines, 1998). A study of adolescents found that gender, age, and mother’s education level did not impact the relationship between acculturation and drug use (Brook et al., 1992; Brook et al., 1997). Given the limited literature available, future studies should consider the role sociodemographic characteristics may play in the relationship between acculturation and health behaviors among African Americans.
The mean quality score for the studies was low (4.90), and the range in scores was large (3-7). All studies failed to meet some methodological quality criteria. For example, few studies reported effect sizes. Effect sizes quantify the size of the difference between two groups without the confounder of sample size. Effect sizes are a critical aspect of research findings, and should be included along with reports of statistical significance because of the information they provide about practical significance (Thompson, 2006). In addition, most studies were cross-sectional, precluding discussion of causality. Acculturation is a dynamic process, and longitudinal studies are needed that examine the impact of acculturation on health and health behaviors as it develops and changes over time. The Snowden and Hines’s (1998) study received the highest quality ranking and found that acculturation was significantly associated with risky sexual behavior in African American men, with small to moderate effect sizes. On the contrary, the study with the lowest quality ranking found no significant differences in level of acculturation among heavy and light African American female smokers (Fernander, Schumacher, Wei, et al., 2008). This study (Fernander, Schumacher, Wei, et al., 2008) was one of the few included in this review to find a nonsignificant relationship between acculturation and smoking.
This review has several limitations. A broad definition of acculturation was used when considering studies for inclusion, and studies that used nonvalidated measures of acculturation were included in the review. To date, acculturation has been studied using different models, and thus, the definition and measurement of the construct has been inconsistent across studies. Despite the limitations of acculturation measures that use unidimensional and bidimensional models, the present study opted to include these measures because of the limited literature. The majority of studies in this review used the L&K-AAAS or its revised version to measure acculturation. Although the L&K-AAAS and its revised version were developed according to a multidimensional model, a total score, as opposed to an evaluation of the measure subscales, was only examined in some studies. A total score limits the measure to allow for only a unidimensional understanding of the construct of acculturation. This approach has been heavily critiqued for the limited and potentially biased conclusions that may be drawn when examining the relationship between a unidimensional measure of acculturation and health behaviors. Using a unidimensional approach precludes understanding of different aspects of culture and presumes that an individual’s level of acculturation is the same across different cultural domains. Future studies should use multidimensional measures of acculturation and examine the subscales provided by the measure, as opposed to just the total score. In addition, few studies in this review discussed to what culture African Americans were acculturating. Researchers have discussed operationalization challenges of the construct of acculturation, one of which is defining exactly what is the heritage or traditional culture and the majority or dominant culture. Future studies that examine African American acculturation should clearly define the heritage and dominant culture. The present review was designed to be more inclusive because this is, to date, the first systematic review assessing the relationship between acculturation and health behaviors among African Americans, and because so few studies were expected to meet even broad inclusion criteria. Most studies were limited to adults. The relationship between acculturation and health behaviors may be different among children and adolescents. Also, this review may have been subject to reporting bias. Few studies reported nonsignificant relationships between acculturation and health behaviors among African Americans. Given the potential for biases in peer-reviewed journals to present significant findings, there may be studies that found nonsignificant relationships with acculturation but did not present them in the manuscript, or were not published. In addition, many studies included in this review came from the same research team (Klonoff & Landrine, 1996, 1999a, 1999b, 2000; Landrine & Klonoff, 1996). Only two of their studies used the same sample population (Klonoff & Landrine, 1999a, 1999b). However, all but one of Klonoff and Landrine’s participant samples included in this review came from Southern California, potentially limiting generalizability of study findings.
This review demonstrates that acculturation plays an important role in a variety of health behaviors among African Americans. Furthermore, this review underscores that African Americans are not a homogeneous group. Findings from this review should be used to develop more effective interventions to target specific groups of African Americans that are at high risk for engaging in adverse health behaviors. In addition, this review highlighted several areas where research is needed. Only 21 studies were identified for inclusion, and for several health behaviors, only one or two studies were available. More studies are needed that examine the impact of acculturation on heath behaviors among African Americans. Future studies should use validated measures of acculturation to allow for cross-study comparison. Additional studies are needed that examine how changes in acculturation over time impact health behaviors among African Americans.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.