
Abstract
Few studies have examined subgroup differences regarding the role of collective cultural strengths among Latinos, the largest minority population in the United States today. Based on cultural and social psychologists’ emphasis on their importance to minorities, this study explored the association of three cultural factors with self-reported mental and physical health for three Latino subgroups identified in the National Latino and Asian American Study (NLAAS). Relative to Cubans, Mexicans and Puerto Ricans experienced poorer physical health and, not surprisingly, more religious involvement. Cubans reported stronger ethnic identity and social support (SS) and were socioeconomically more affluent compared with both Puerto Ricans and Mexicans. Multivariate analyses revealed positive effects of religious attendance on the mental and physical health of Puerto Ricans, controlling for the negative role of discrimination and other known predictors. Racial/ethnic identity was linked with better mental health of all three Latino subgroups, whereas SS had no significant effect.
Keywords
In terms of race and ethnicity, Latino Americans (Latinos) constitute a highly heterogeneous population in the United States, which includes three major ethnic subcultures (e.g., Cubans, Mexicans, and Puerto Ricans; Ennis, Ríos-Vargas, & Albert, 2011). Within the past decade, Latinos have accounted for over half of the total U.S. population growth (Passel, Cohn, & Lopez, 2011), with increases especially observed in the two largest subgroups (Mexicans, 63%, and Puerto Ricans, 9.3%; Ennis et al., 2011). To design and implement culturally sensitive services, it is imperative to examine subcultural differences among Latinos, especially culturally protective factors for overall health. Leaders in counseling psychology highlight the need to emphasize cultural strengths in serving primarily collectivist racial and ethnic minority communities (Sue & Sue, 2013). Because of cultural diversity and ongoing disparities faced by minorities, these factors may play a salient role in their well-being at a group level, which necessitates acquisition of cultural competence for all psychologists (Fischer, Ai, Aydin, Frey, & Haslam, 2010; Sue & Sue, 2013). Failure to do so can lead to misinterpretation of symptoms and misdiagnosis among Latinos, resulting in the loss of trust with the providers.
In this study, we defined cultural strengths as collective traits embraced in shared sociocultural values and traditions of certain sociocultural groups, which may become psychosocial resources for group members to draw their strengths. Based on some psychologist assumptions (Fischer et al., 2010; Sue & Sue, 2013), cultural strengths of minoritized populations within a mainstream society may include, but are not limited to, interrelated group characteristics such as social support (SS), racial/ethnic identity (REI), and religious involvement. Evidence has shown that collective strength factors may benefit these populations through enhanced self-esteem and mental health, physical health, or coping skills for dealing with life stressors, including discrimination (Chatters et al., 2008; Kaslow et al., 2010; Sue & Sue, 2013). In particular, Ai, Aisenberg, Weiss, and Salazar (2014) found a strong association of REI with self-rated mental health and self-rated health (SRMH and SRH) among all Latinos in the National Latino and Asian American Study (NLAAS; Alegria et al., 2004; Heeringa et al., 2004). It is worth noting that the NLAAS is the first national community household representative sample survey study on the psychopathology and patterns of service utilization of Asian and Latino American populations (Alegria et al., 2004; Heeringa et al., 2004).
The present study extended Ai, Aisenberg, et al.’s (2014) investigation to the subgroup differences in cultural strength factors, using the same set of factors in the previous study. Our specific aim was to explore differential associations of cultural strength factors with SRMH and SRH in three major Latino subgroups (Cubans, Mexicans, and Puerto Rican). Because of the inherent racial diversity within many Latino subgroups (e.g., Black, biracial, and White individuals in Cubans and Puerto Rican), in this analysis we focused primarily on ethnic and cultural differences rather than on divergent ancestries. Below, we begin with the significance of addressing cultural strengths in understanding of Latino and other minorities’ overall health. Furthermore, we underscore the need to investigate cultural strengths in relation to these outcomes in subgroups. Based on the literature, we include the subgroup heterogeneity (e.g., social stratification and acculturation) as known covariates alongside demographics. Finally, we present the hypothesis in this study.
Individual Character Strengths and Collective Cultural Strengths
Why should we endorse the concept of cultural strengths in studying Latinos’ health? Positive psychologists have challenged the long-standing paradigm of focusing on psychopathology by scientifically investigating and facilitating positive human development and health (Seligman & Csikszentmihalyi, 2000). Peterson and Seligman (2003) endorsed the study of individuals’ character strengths (e.g., transcendence), given their crucial role for individuals’ prevailing in an individualistic society. Spirituality, for example, is viewed as one of individuals’ strengths On the contrary, psychologists of religion consider the merits of faith to be a source of significance in life and coping, which, thereby, functions as a fundamental element of cultural identity (Pargament, Magyar-Russell, & Murray-Swank, 2005). The latter culture-oriented assumption may be a more apt description for ethnic minority behaviors due to certain group-oriented spiritual practices from which they can draw strength for coping (Fischer et al., 2010; Sue & Sue, 2013).
Whereas Western culture highlights the individual “I,” ethnic minoritized populations tend to affirm the collective “we” as paramount in consciousness and behaviors (Fischer et al., 2010). Members in the latter groups thus retain their culturally group bound (e.g., Native Americans’ tribalism, Blacks’ church communities, and Latinos’ and Asian Americans’ familism) and related collectivist characteristics more strongly than those of the dominant culture. Social Identity Theory (Tajfel, 1982) suggests that personal goals and the well-being of members in ethnic minority communities tend to be subsumed under those of the collective (Sue & Sue, 2013). Within such cultures, deep respect and affection among a large social network, rather than the individual self, is emphasized (Markus & Kitayama, 1991). Especially for Latinos, cultural strengths derive from family and inform community-based beliefs, actions, and behaviors (Lorenzo-Blanco & Cortina, 2013; Schwartz, Unger, Zamboanga, & Szapocznik, 2010). This collectivist understanding differs from mainstream perspectives that prioritize assets like individual strengths and personal autonomy and achievement (Ai, Aisenberg, et al., 2014).
Ethnic minority groups tend to rely on their collectivistic values and strengths to preserve their cultural identity (Sue & Sue, 2013). Their collectivist strengths enable them to rally group efforts and/or to attain mutual support for maintaining their community solidarity and collective well-being (Fischer et al., 2010; Sue & Sue, 2013). In the United States, many ethnic minorities face the process of acculturation, meaning an evolutionary one by which minorities acquire cultural elements over time from the mainstream majority (Healey & O’Brien, 2014). During this process, a tendency is for people of ethnic minoritized communities to become less collectivist, more independent, better educated, and closer to an “American” identity reflected by the dominant Western culture (Schwartz et al., 2010). However, in acculturation the values and culture of many ethnic minority communities may face parallel challenges of integrating into the mainstream while seeking to maintain indigenous practices and customs (Lorenzo-Blanco & Cortina, 2013). Conceivably, many will preserve their traditional cultural strengths, whereas others may pursue Western values. Thus, the role of cultural strengths in well-being could vary with such divergent experiences and cultural origins of subgroups. Studying these differences is a crucial way to understanding Latinos (Lorenzo-Blanco & Cortina, 2013).
Three Cultural Strengths and Latinos’ SRMH and SRH
It is well established that social connection and support in terms of one’s social capital can benefit individuals across racial and ethnic groups (McShall & Johnson, 2015). Relationship quality in social networks tends to be positively associated with the physical health of Latinos’ nationwide. Among all Latinos, SS is especially tied to an emphasis on mutuality within extended families and intimate nonfamilial networks within their community (Lorenzo-Blanco & Cortina, 2013; Sue & Sue, 2013), evidently being conducive to their better SRMH and SRH (Mulvaney-Day, Alegría, & Sribney, 2007). These findings concurred with gender-specific studies showing an inverse link of family cohesion with general anxiety disorder in Latino women (Ai, Weiss, & Fincham, 2014) and coexisting family conflicts and psychopathology in both genders (Ai, Pappas, & Simonsen, 2015; Ai, Weiss, & Fincham, 2014).
Ethnic identity refers to a strong sense of belonging to a group, as determined at birth or assigned to one by others, on the basis of cultural background (Phinney & Ong, 2007). Its potential protection for marginalized minorities resides in boosted positive feelings about the membership of the group (Fischer et al., 2010; Hero, 1992; Tajfel, 1982). Among Latino adults, ethnic identity moderated the association between skin color and self-esteem (López, 2008), was positively linked with the SRMH and SRH (Ai, Aisenberg, et al., 2014), and was related to less perceived discrimination (Pérez, Fortuna, & Alegría, 2008), as did among other minority adults (Mossakowski, 2003).
Latinos are predominantly Christians (mostly Roman Catholic, though becoming increasingly diversified) and their religious involvement can function as a source of strength in dealing with daily stressors (Andrés-Hyman, Ortiz, Anñz, Paris, & Davidson, 2006; Sue & Sue, 2013). Social and cultural psychologists posit religious involvement as a collective social behavior based on its promotion for prosociality throughout human history (Norenzayan & Shariff, 2008). Religious involvement seems to buffer against the social-identity-related negative experiences (e.g., discrimination) faced by disadvantaged social groups (Fischer et al., 2010; Sue & Sue, 2013). Religious behaviors can be an adaptive coping resource in minority groups (Ai, Huang, Bjorck, & Appel, 2013; Chatters et al., 2008; Pargament et al., 2005). NLAAS studies revealed the positive role of religious involvement in Latinos’ health-related behaviors (Ransford, Carrillo, & Rivera, 2010) and mental health (Robinson, Bolton, Rasic, & Sareen, 2012), and in counteracting the impact of discrimination on overall health of other minorities (Ai et al., 2013; Chatters et al., 2008; Ellison, Musick, & Henderson, 2008). Yet, questions remain as to whether these cultural strength factors can be uniformly beneficial for all subgroups, given their diverse experiences.
The Need to Explore Subgroup Differences and Known Covariates in Latinos
Importantly, there are considerable variations in the role of ethnic identity and religious involvement in mental health across Asian American subgroups in the NLAAS, converging with contextual differences (Ai, Appel, & Lee, 2016; Ai, Nicdao, Appel, & Lee, 2015). Subgroup variation could also occur in Latinos, given that numerous factors (demographics, cultural roots, social stratification, immigration history, and acculturation status) may contribute to their intragroup differences (Blendon et al., 2015; Gonzalez-Barrera & Lopez, 2013). For example, among Latinos in the United States, Cubans generally enjoy the highest social status (Hero, 1992), whereas Mexicans and Puerto Ricans tend to be in danger of joining a prominent underclass area (Healey & O’Brien, 2014). The health benefit of higher wealth was evidenced for Cubans and Puerto Ricans, though lower wealth was the most important predictor of psychological distress for all Latinos (Xu, 2011). Chatterji, Alegría, Lu, and Takeuchi (2007) related employment status to Latinos’ psychiatric disorders and mental distress.
Moreover, less acculturation (e.g., shorter residency in the United States and non-U.S.-born) has been related to enhanced mental health compared with U.S.-born Latinos and those with long residency in the country (Ortega, Canino, & Alegria, 2008), especially in Mexicans (Vega et al., 1998; Xu, 2011). A national trend analysis linked higher levels of social stratification and acculturation with poor SRH of Mexicans (Zsembik & Fennell, 2005), whereas Viruell-Fuentes, Miranda, and Abdulrahim (2012) suggested that the stratification impact in SRH was explainable by discrimination. Darker-skin Latinos, many of whom belong to Mexican and Puerto Rican subgroups, reported more discrimination, because they were perceived to be less educated and more likely to have blue-collar jobs (Gonzalez-Barrera & Lopez, 2013; Passel & Cohn, 2009). Perceived discrimination has also played a critical role in poor mental health (Ai, Aisenberg, et al., 2014; Gee, Ryan, Laflamme, & Holt, 2006; Gee, Spencer, Chen, & Takeuchi, 2007) or physical health of Latinos and other minorities (Molina, Alegría, & Mahalingam, 2013), one that is more critical than acculturation stress (Vega et al., 1998; Vega, Sribney, Aguilar-Gaxiola, & Kolody, 2004). Given the known influences of social stratification and acculturation levels in Latinos’ mental health, these factors must be controlled in the current analysis.
The Present Study
In sum, there is scant published research to compare the role of collective cultural strengths in major Latino subgroups controlling for social stratification and acculturation levels. The present study addresses this research question:
Based on the literature, we hypothesized that religious involvement and ethnic identity would be related to better SRMH and SRH of Puerto Ricans and Mexicans, who were less affluent than Cubans (Fischer et al., 2010; Hero, 1992; Mossakowski, 2003; Norenzayan & Shariff, 2008; Pérez et al., 2008; Tajfel, 1982). We additionally anticipated that SS would function the same on SRMH and SRH across subgroups.
Method
The Data Source and the Sample
The NLAAS questionnaire is available in six languages, including Spanish. In face-to-face interviews, participants were requested to answer multiple-choice questions related to social demographics, acculturation and immigration, mental health screening and diagnosis, and patterns of service utilization. Thus, the NLAAS database was ideal for investigating cultural strengths adjusting known associates (Gee et al., 2007; Rosen-Reynoso, Alegria, Chen, Laderman, & Roberts, 2011). Previous publications described sampling procedures, including weights developed (e.g., attrition and weight) to correct for sampling bias in detail (Alegria et al., 2004; Heeringa et al., 2004). From May 2002 to December 2003, trained interviewers collected data in a total of 252 geographic areas across the 50 states and Washington, D.C. Institutionalized people and those living on military bases were excluded.
Among 27,026 sample housing units screened for the target population, 5,579 eligible respondents were identified. The information from the weighted NLAAS sample resembled that in the U.S. Census 2000 with respect to age, gender, education level, marital status, and living area. However, the NLAAS sample was more divergent in nativity (U.S.- vs. foreign-born) and included more Latino immigrants and lower income respondents, which is consistent with the reports of the underestimation of immigrants in the Census (Cook, Alegría, Lin, & Guo, 2009). The final NLAAS sample comprised 4,649 respondents with a completed interview, a response rate of 70.6%. Among the respondents, there were 2,554 Latinos aged 18 years or older. Included in our final model were 1,940 participants, including self-identified Cubans (n = 577), Mexicans (n = 868), and Puerto Ricans (n = 495). There were no significant differences in gender across the three Latino subgroups (Table 1). On average, Cubans were older, followed by Puerto Ricans and then by Mexicans.
Descriptive Statistics and Intergroup Differences for the Three Major Latino Subgroups, Unadjusted for Survey Population Weights and Design Factors.
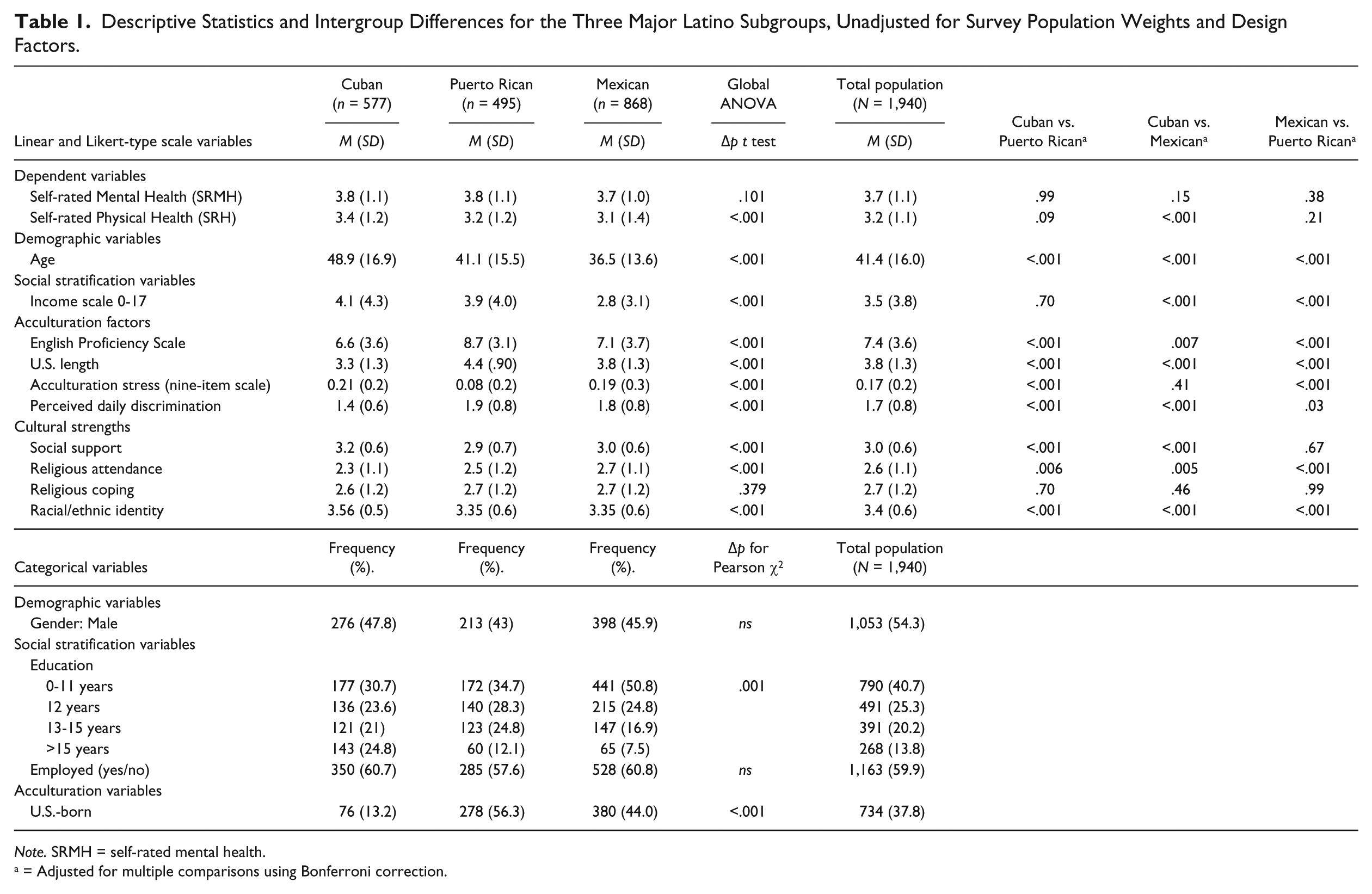
Note. SRMH = self-rated mental health.
a = Adjusted for multiple comparisons using Bonferroni correction.
Measures
The NLAAS adapted criteria used on the World Health Organization Composite International Diagnostic Interview (WHO-CIDI) to capture mental health history over the previous 12 months (WHO, 1998). The WHM-CIDI is a cross-cultural psychiatric epidemiologic protocol that systematically operationalizes the criteria of the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994). The criteria in CIDI are compatible to those listed in DSM-IV. In the present study, the dependent variable, SRMH, was measured on a 5-point Likert-type scale (1 = poor, 5 = excellent) by reverse coding the question (“How would you rate your overall mental health?”), as shown in Table 1. Similarly, SRH was measured on the same scale using one question (“How would you rate your overall physical health?”).
Among independent variables of major interest, we used religious attendance (RA) and religious coping (RC) to assess religious involvement. For respondents who had identified a religious affiliation on the question (“What is your religious preference, that is, Protestantism, Catholicism, Other Religion, and No Religion?”), RA was measured via an additional question (i.e., “How often do you usually attend religious services?”). The answers were scored on a 5-point Likert-type scale (1 = never, 2 = less than once a month, 3 = 1-3 times a month, 4 = once a week, and 5 = more than once a week). RC was measured via one question (“When you have problems or difficulties in your family, work, or personal life, how often do you seek comfort through religious or spiritual means, such as praying, meditating, attending a religious or spiritual service, or talking to a religious or spiritual advisor?”), with answers scored on a 4-point scale (1 = never, 2 = rarely, 3 = sometimes, and 4 = often). Respondents with no religious affiliation were initially coded as missing, but we recoded them as 1 to avoid exclusion of those responses.
REI was assessed on a 4-point scale (1 = not at all, 4 = a lot; αCuban = .756, αPuerto Rican = .714, αMexican = .737) for three questions (e.g., “How much do you identify with others of the same racial/ethnic descent?”). The score was derived by reverse coding, summing, and averaging the three questions. SS was measured on a 4-point scale (1 = not at all to 4 = a lot; αCuban = .764, αPuerto Rican = .787, αMexican = .807) for eight questions (e.g., “How much can you rely on your relatives for help if you have a serious problem?”) to assess support received from spouse, family, and friends. The NLAAS coded certain items of unmarried respondents as missing. To avoid bias toward only the married, we recoded them as 1.
For controls, acculturation factors included three measures: English Proficiency (the sum of three items rating the ability to speak, read, and write English; 1 = poor, 4 = excellent; score was summed; αCuban = .978, αPuerto Rican = .962, αMexican = .974), Birthplace (0 = foreign-born, 1 = U.S.-born), and Years in the United States (1 = 0-4 years, 2 = 5-10 years, 3 = 11-20 years, and 4 ≥ 21 or born in the United States; see Gee et al., 2007). Nine items (e.g., “Do you find it hard interacting with others because of difficulties you have with the English language?”) constituting Acculturation Stress were dichotomized (0 = no, 1 = yes) and averaged to yield a variable ranging from 0 to 1 (αCuban = .633, αPuerto Rican = .600, αMexican = .756; Vega et al., 1998). U.S.-born respondents were not asked these questions. To avoid bias toward only married Latinos, we assigned U.S.-born respondents a value of “0.” Perceived daily Discrimination, based on the Detroit Area Study, was reverse coded. Respondents responded to nine questions (e.g., “People act as if they think you are not smart”; Alegria et al., 2004), on a 6-point scale (1 = never, 6 = almost every day), which were averaged to create a scale (αCuban = .886, αPuerto Rican = .893, αMexican = .910).
Demographic measures included Gender (0 = female, 1 = male) and Age (years, ranging from 18 to 95). Social stratification factors included Education (1 = 0-11 years, 2 = 12 years, 3 = 13-15 years and > 165 years), Income (a ratio to the poverty threshold for the corresponding family size in 2000, ranging from 0 to 17; U.S. Bureaus of the Census, 2006), and Employment (0 = unemployed or not in the labor force, 1 = employed)
Statistical Analyses
All analyses were performed using Stata 10 (StataCorp LP, College Station, TX, USA). NLAAS-developed sample weights were used in all regression analyses. We first calculated frequency distributions and means with standard deviations to describe all variables. One-way ANOVA tests and chi-square tests were performed to identify bivariate differences in predictive factors among the three subgroups (Table 1). We then conducted Kendall’s Tau correlations to demonstrate correlations among predictors in each subgroup. Finally, we conducted two sets of two-step linear multiple regression analyses to evaluate the association of cultural strengths and SRMH and SRH of each Latino subgroup, respectively, using NLAAS-developed sample weights. In Model 1, control factors were regressed on SRMH and SRH. In Model 2, three potential protective cultural strength factors were added into equations to test the hypothesis concerning whether these outcomes were differentially explained by religious involvement, REI, and SS, across three subgroups, above and beyond the effect of known predictors in the literature. We analyzed data involving RA and RC in separated models. Finally, we performed post hoc analyses to evaluate the potential interaction between strengths and discrimination to explore whether cultural strengths could be more protective for those who perceived greater discrimination within each subgroup, respectively. We computed all analyses using Stata 10 SE and established statistical significance at an alpha level of p < .05.
Results
Descriptive Statistics
Table 1 presents the results of descriptive statistics for both continuous scale and categorical predictors and outcome measures across the three subgroups. An ANOVA with post hoc tests adjusted for multiple comparisons (Bonferroni) found no significant difference in the SRMH between any two of the subpopulation groups. Cubans reported a significantly higher level of SRH than Mexicans (p < .001), but there were no significant differences between Puerto Ricans and Mexicans or Cubans and Puerto Ricans. For cultural strength factors, Mexicans reported the highest level of RA, and the percent reporting no RA for Cubans, Puerto Ricans, and Mexicans, respectively, was 30.7%, 25.9%, and 16.2% (overall average 22.9%). The average REI and SS scores were highest among Cubans. Regarding demographics, Mexicans had the lowest levels on both Education and Income. As for acculturation factors, Puerto Ricans and Mexicans perceived higher levels of Discrimination than Cubans, as expected. Puerto Ricans had the highest level of English Proficiency, were more likely to be U.S.-born, and have longer residence in the United States, as compared with Mexicans or Cubans.
Bivariate Correlations
Bivariate correlations showed both similarities and differences across subgroups, as shown in Tables 2 to 4. SRMH and SRH were significantly correlated across all three subgroups. RA and SS were not correlated with either SRMH or SRH of any Latino subgroup. REI, however, was correlated with significant increases in SRMH for Mexicans (r = .069, p < .01). Being U.S.-Born was correlated positively with SRMH in all three subgroups and was significantly correlated with SRH among Cubans and Puerto Ricans but not Mexicans. Acculturation Stress was correlated negatively with SRMH for all three subgroups and related to reduced SRMH and SRH for Cubans (r = –.124, p < .001; r = –.071, p < .05) and Puerto Ricans (r = –.068, r = –.072, ps < .01). Length in the United States was statistically significantly tied to increased SRMH for Mexicans (r = .069, p < .01) but had no effect for Cubans and Puerto Ricans. Discrimination was not related to either SRMH or SRH in any subgroup.
Kendall’s Tau Correlations for Cubans (n = 522).

Note. 1 = self-rated mental health; 2 = self-rated physical health; 3 = sex; 4 = age; 5 = education; 6 = income; 7 = employed; 8 = English proficiency; 9 = U.S.-born; 10 = U.S. length; 11 = acculturation stress; 12 = discrimination; 13 = religious attendance; 14 = social support; 15 = racial/ethnic identity.
p < .05. **p < .01. ***p < .001.
Kendall’s Tau Correlations for Puerto Ricans (n = 465).

Note. 1 = self-rated mental health; 2 = self-rated physical health; 3 = sex; 4 = age; 5 = education; 6 = income; 7 = employed; 8 = English proficiency; 9 = U.S.-born; 10 = U.S. length; 11 = acculturation stress; 12 = discrimination; 13 = religious attendance; 14 = social support; 15 = racial/ethnic identity.
p < .05. **p < .01. ***p < .001.
Kendall’s Tau Correlations for Mexicans (n = 821).

Note. 1 = self-rated mental health; 2 = self-rated physical health; 3 = sex; 4 = age; 5 = education; 6 = income; 7 = employed; 8 = English proficiency; 9 = U.S.-born; 10 = U.S. length; 11 = acculturation stress; 12 = discrimination; 13 = religious attendance; 14 = social support; 15 = racial/ethnic identity.
p < .05. **p < .01. ***p < .001.
Age correlated negatively with both SRMH and SRH in all subgroups, with stronger correlation for Cubans (rSRMH = –.132, rSRH = –.202, p < .001) than for Puerto Ricans (rSRMH = –.076, p < .05; rSRH = –.140, p < .001) and Mexicans (rSRMH = –.052, p < .05; rSRH = –.089, p < .001). Education, Income, Employment, and English Proficiency were correlated positively with both SRMH and SRH for all subgroups but were stronger for both Cubans and Puerto Ricans (Tables 2-4).
Multivariate Analyses
Tables 5 and 6 display the standardized linear coefficients and p values for the multivariate analyses of SRMH and SRH and the differential associations of RA and REI with those outcomes. As shown in these tables, after listwise deletion, 1,818 respondents were included in the final step of regression models. 1
Standardized Coefficients for the Regression of Self-Rated Mental Health on Variables and Covariates.

p < .05. **p < .01. ***p < .001.
Standardized Coefficients for the Regression of Self-Rated Physical Health (SRH) on Variables and Covariates.
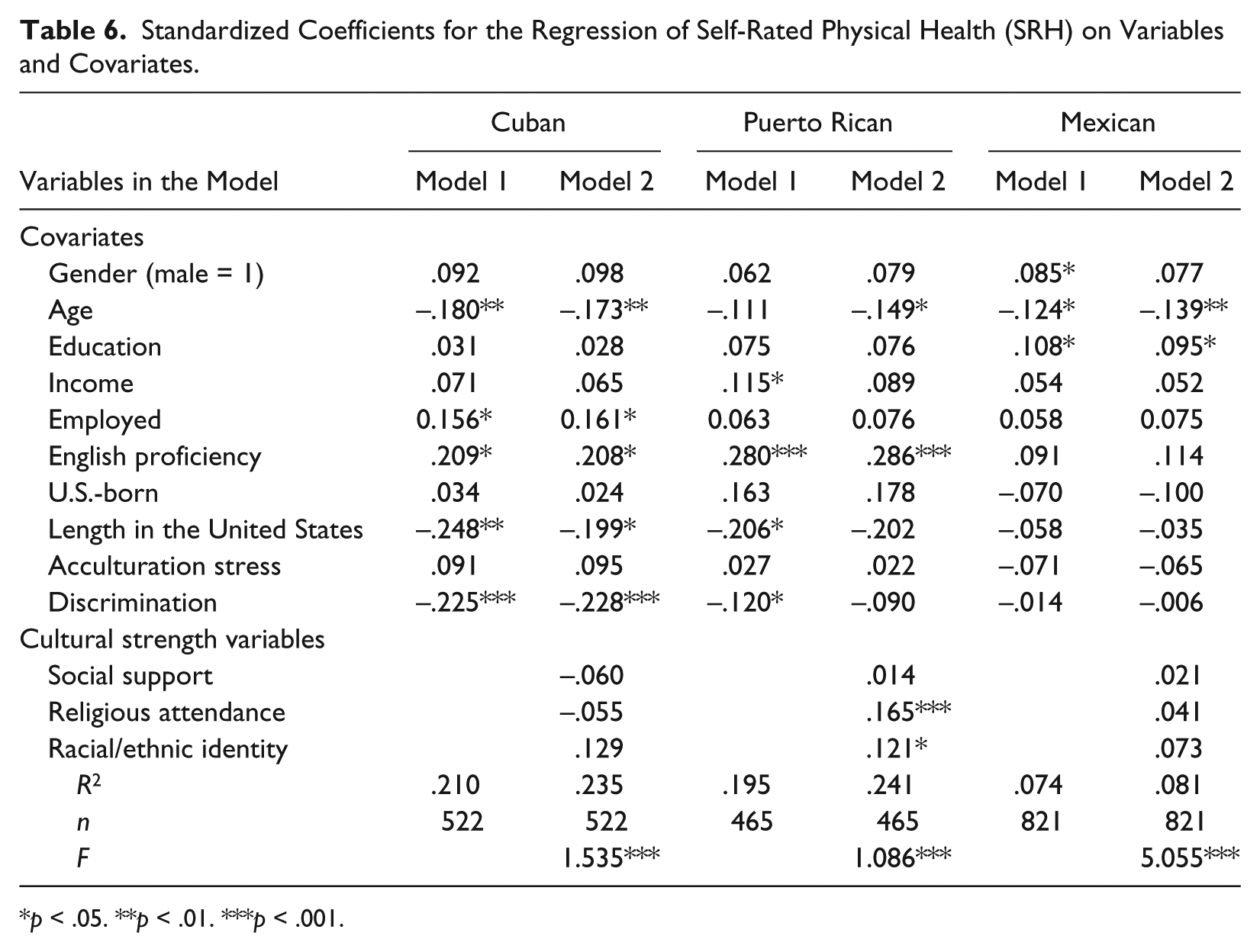
p < .05. **p < .01. ***p < .001.
SRMH
Among sociodemographic factors (Table 5), Gender was a consistent predictor for SRMH for all Latino subgroups, with men uniformly reporting better mental health than women in Model 1. The association was largest for Cuban men, whose SRMH was on average 0.125 SD higher than that of female Cubans. The effect sizes for Puerto Rican and Mexican men were B = .103 and B = .093, respectively. Education was associated with better SRMH for Puerto Ricans and Mexicans, with statistically indistinguishable coefficients for both, but not Cubans. Entry of cultural strength factors, in Model 2, reduced the coefficient for Mexicans. Each 1 SD increase in Education was associated with 0.143 and 0.130 SD increase in SRMH for Puerto Ricans and Mexicans, respectively. Employment and Income, in Model 1, were not associated with changes in SRMH. However, Employment was significantly associated with SRMH for Cubans in Model 2. Employed Cubans had on average 0.142 SD higher SRMH when compared with their unemployed counterparts.
Among acculturation factors (Model 1), English Proficiency was always associated with increased SRMH and the effect seemed to be largest for Cubans, the least acculturated subgroup with respect to their lowest average level of English skills and of length of staying in the United States. Length of time in the United States, however, was consistently associated with lower SRMH only for Mexicans with each unit of its SD increase contributing to a 0.162 SD decrease in reported mental health. Acculturation Stress and U.S.-Born had no significant effect. Nevertheless, perceived Discrimination was consistently associated with reduced mental health for Puerto Ricans (0.162 SD decrease) and Mexicans (0.093 SD decrease) but not for Cubans. For cultural strength factors, in Model 2, RA appeared to benefit only Puerto Ricans with each 1 SD increase in Education linked to a 0.126 SD increase in their SRMH. REI was a statistically significant protective factor for all three subgroups whereas SS was not for any subgroup. Entry of the cultural strength factors reduced the magnitude of the detrimental effect of Discrimination for both Puerto Ricans and Mexicans. Thus, these psychosocial–behavioral factors appeared to moderate the effects of Discrimination on SRMH for the two subgroups.
F tests (Table 5) for all final models were significant. Model 2 explained 17.7% and 18% of the variation in SRMH for Cubans and Puerto Ricans, respectively, but accounted only for 11.5% of the variation in SRMH for Mexicans. Improvement between Models 1 and 2 (not shown in the table) was statistically significant for Cubans, F(3, 446) = 4.14, p = .007; Puerto Ricans, F(3, 412) = 4.87, p = .002; and Mexicans, F(3, 744) = 5.10, p = .002.
Thus, inclusion of the protective factors in Model 2 increased the explained variance of our models to a statistically significant extent for all three Latino subgroups.
Self-rated physical health
Among sociodemographic factors (Table 6), there was no association of gender with SRH for Cubans and Puerto Ricans in Model 1. The significant association of gender with SRH for Mexicans vanished after protective factors were entered in Model 2. Age was associated with lower SRH for all three subgroups in Model 2, especially among the oldest subgroup (Cubans). Social strata factors presented with different associations across three subgroups. Education had an effect only for Mexicans; per unit SD increase in Education was associated with a 0.095 SD increase in SRH in Model 2. Income had no effect on SRH for Cubans and Mexicans, and its positive effect for Puerto Ricans in Model 1 vanished in Model 2. Employment was associated with better SRH only for Cubans; employed Cubans had on average 0.161 SD higher SRH than that of their unemployed counterparts.
Among acculturation factors, every SD increase in English Proficiency was tied to an improved SRH for Cubans and Puerto Ricans of 0.208 and 0.286 SDs, respectively, in Model 2. Whereas Length in the United States was associated with reduced SRMH for Mexicans (Table 5), it had no effect on their SRH at all (Table 6). Also, it was now related to a decreased physical health for Cubans in Model 2. However, once cultural strength factors were entered in Model 2, the magnitude of this effect reduced in Cubans from –0.248 (Model 1) to –0.199 SD (Model 2) and disappeared for Puerto Ricans. Discrimination also showed a pattern opposite to that of SRMH (Table 6) with a significant negative association only for Cubans in Model 2, but not for Mexicans and Puerto Ricans. Acculturation Stress and U.S.-Born had no effect on SRH for any subgroup. For cultural strength factors, in Model 2, RA had a statistically significant influence only for Puerto Ricans with every 1 SD related to an increase in SRH by 0.165 SD. REI also had a protective effect for Puerto Ricans with each SD increase linked with a 0.121 SD improvement in SRH. In Model 2, the role of Discrimination for Puerto Ricans was nullified after entry of SS, RA, and REI. Entering SS, RA, and REI as a group in Model 2 reduced the coefficient size for Length in the United States for Cubans, nullified the effect of Length in the United States for Puerto Ricans, and removed the effect of Gender for Mexicans.
As shown in F tests (Table 6), all final models were significant, and Model 2 accounted for 23.5% of the variation in SRH among Cubans and 24.1% among Puerto Ricans but only 8.1% among Mexicans. Improvement between Models 1 and 2 (not shown in the table) was statistically significant for both Cubans, F(3, 446) = 4.33, p = .05, and Puerto Ricans, F(3, 412) = 6.85, p = .001, but not for Mexicans, F(3, 744) = 1.12, p = .15. Thus, addition of the cultural strength factors improved the models for Cubans and Puerto Ricans. Finally, post hoc analyses showed no interaction of cultural strengths and discrimination.
Additional analyses on RC
Patterns from models that included RC instead of RA in Model 2 were similar (Tables 5 and 6) as reflected by significance patterns and the magnitude of the coefficient determining SRMH and SRH (data not shown). Education had a positive association with the SRH of Mexicans. The magnitude of a negative association of Discrimination on SRH is higher than that in the SRMH model for Puerto Ricans. Also, its negative impact on the SRH became significant for Mexicans. RC was not associated with SRMH and SRH for any subgroup. The patterns of REI and SS were mostly similar to those in Model 2 using RA, except a highly significant REI effect on the SRH of Mexicans.
Discussion
Expanding the NLAAS literature, the present study provides novel information on differential roles of certain cultural strengths in SRMH and SRH among three major Latino subgroups. To our knowledge, as a major contribution to Latino studies, this subcultural analysis extends the previous literature (e.g., Zsembik & Fennell, 2005) alerting the subgroup differences in health status of Latino subgroups at a national level. Despite previous evidence on the potential protection of RA for SRMH (Robinson et al., 2012) and of REI for both SRMH and SRH in all Latinos (Ai, Aisenberg, et al., 2014), our findings reveal varying associations across three major subgroups. Specifically, religions involvement emerged as a robust contributor only to SRMH and SRH of the Puerto Rican subgroup, partly supporting our hypothesis. REI, however, increases with level of SRH only for Cubans, despite its association with SRMH in all subgroups. Interestingly, such positive relationships do not fall in line with levels of perceived discrimination, to some extent challenging psychologists’ assumption that the positive functions of cultural strengths would intertwine with REI-related stress (Fischer et al., 2010; Tajfel, 1982). Because previous theoretical frameworks define minorities in a broader sense (e.g., religious, sexual), our differential findings in Latinos should be further elaborated on the social context in which each ethnic culture emerges.
Regarding positive findings from Puerto Ricans, there are common experiences shared between this Latino subgroup and African American population that is heavily involved in religious services in certain urban communities. African Americans and Puerto Ricans co-reside in such areas in which sharp socioeconomic status (SES) contrasts are present (Healey & O’Brien, 2014). Members of the two groups could experience similar social strata, neighborhood living conditions, and historical experiences (Healey & O’Brien, 2014). Thus, they can fall in the same web of social disadvantages and discrimination with regard to SES, skin color, and impoverished residential locations in a racially dichotomized society. In reports from the National Survey of American Life, earlier studies showed that religious involvement counteracted the impact of discrimination on overall health of African Americans (Chatters et al., 2008; Ellison et al., 2008). Both African Americans and Caribbean Blacks used religion (e.g., identification with the Black church) to cope with racial discrimination (Hayward & Krause, 2015), while church attendance had a significant and positive association with mental health and life satisfaction (Assari, 2013), a finding that is similar to that among Puerto Ricans in the current study.
Indeed, Latinos hold strong religious systems that serve as a source of strengths, similar to African Americans (Andrés-Hyman et al., 2006; Chatters et al., 2008; Comas-Diaz, 2012; Paniagua, 2014). Interestingly, both Mexicans and Puerto Ricans, two socially disadvantaged subgroups, are highly involved in church activities. Yet, null finding from the Mexican subgroup seems to be contrary to the assumption concerning religious or spiritual involvement as a resource for ethnic minority communities (Fischer et al., 2010; Sue & Sue, 2013). Culturally speaking, considerable variations exist between the two Latino subgroups, including but not limited to their heritage, immigration experiences, legal status, geographic locations, job types, and poverty levels (Healey & O’Brien, 2014). Puerto Ricans, for example, are all born as citizens and mostly live in relatively stable urban communities, whereas many Mexicans are immigrants with some lacking documented status and employed in dangerous agricultural and construction jobs (Kochhar, 2012). An unstable home environment could lead to inconsistent community resources (e.g., church support), leaving them to rely on other resources undetected in this study.
Alternatively, not all Latinos share every type of religious compotent in their belief systems (Paniagua, 2014). Certain Latinos may believe that prayers will cure a physical or mental health problem and/or that mental health problems are caused by evil spirits (Comas-Diaz, 2012; Paniagua, 2014). The church has the power to address these problems for them, and religous leaders can be key figures in assisting them with mental health problems. Other Latinos may consult spiritualists, or indigenous healers for, to cope with physical and mental health problems (Comas-Diaz, 2012). It remains unclear how Latino spiritual and cultural legacies interplay with complex processes of acculturation and SES stratification and how their living condition affects the expression of cultural strengths. All these nuances warrant future investigation to provide constructive information to inform culturally responsive health and mental health services for Mexicans and other Latinos.
Concerning a uniformly positive role of REI in subgroup metal health, this study somewhat corroborates previous findings from all Latinos (Ai, Aisenberg, et al., 2014; López, 2008; Pérez et al., 2008). As for physical health, however, REI may play a significant part only among Puerto Ricans. Expanding Ai, Aisenberg, et al.’s (2014) study, our findings suggest that Latino identity may function in different ways among subgroups. Whereas the previous study did not indicate this moderation (Ai, Aisenberg, et al., 2014), entry of REI and religious involvement reduces the detrimental role of discrimination in mental health of both Mexicans and Puerto Ricans. The salient moderating effect reinforces psychologists’ framework on the protection of REI for marginalized minorities (Fischer et al., 2010; Tajfel, 1982), involving its buffer against deleterious impacts of discrimination (Mossakowski, 2003). Also, adding cultural strengths nullified the role of discrimination on physical health of Puerto Ricans. The REI–physical health link in Cubans supports a different function of REI, given their strongest ethnic identity. As noted, REI can promote a strong sense of belonging and mutual support (Phinney & Ong, 2007) and positive feelings about one’s cultural membership (Tajfel & Turner, 1986).
Dovetailing with an all-Latino study (Ai, Aisenberg, et al., 2014), SS is not related to either outcome in any subgroup, despite an established relationship for all Latinos in a major NLAAS study (Mulvaney-Day et al., 2007), when religious involvement and REI were not tested. Accordingly, our null finding may imply that the relatively under-investigated cultural strength factors could be stronger predictors than SS, when three factors are investigated together in Latinos. It is also plausible that the function of SS may be better examined with more precise indicators containing more items (e.g., relationship quality, McShall & Johnson, 2015; or family bound, Ai, Aisenberg, et al., 2014; Ai, Pappas, et al., 2015; Sue & Sue, 2013) for Latinos.
Overall, our findings suggest subgroup variations in acculturation factors and in their role in endpoints, consistent with the literature. English proficiency appears to be beneficial for mental health of all subgroups and is associated with better physical health for Puerto Ricans and Cubans. Yet, the pattern does not support Ortega and colleagues’ (2008) study showing a desirable role of poor/fair English proficiency for all Latinos. The differences could be based on different outcome measures (psychopathology vs. positive SRMH and SRH). Similar to Lorenzo-Blanco and Cortina’s (2013) study, U.S.-born and length of stay are correlated with discrimination in all three subgroups. However, our bivariate analyses reveal the strongest effect size in the Mexican subgroup. Length of stay predicts poor mental health only for Mexicans, congruent with Vega et al.’s (1998) Mexican paradox. The interplay of acculturation with poor well-being in Mexicans may also imply the lack of stable community resources for them. Longer stays in the United States are tied with poorer physical health for Cubans, who had the least acculturation but the highest acculturation stress. Yet, consistent with other Latino studies (Ai, Aisenberg, et al., 2014; Vega et al., 2004), acculturation stress plays little role in SRMH and SRH.
Although the average level of perceived discrimination is not high, relative to Cubans, Mexicans and Puerto Ricans have significantly higher levels of discrimination, equivalent to that of Asian Americans and close to that of African Americans (Gee et al., 2007). Among Mexicans and Puerto Ricans, perceived discrimination predicts poorer mental health, enriching the literature on its detrimental influences (Ai, Aisenberg, et al., 2014; Gee et al., 2006; Gee et al., 2007). Perceived discrimination is also tied with poorer physical health of Cubans and was not buffered by cultural strengths, a finding resembling that from all Latinos (Molina et al., 2013).
Finally, Mexicans and Puerto Ricans report remarkably lower levels of SES than Cubans. The variation and associated differential prediction for SRMH and SRH across subgroups are consistent with previous findings (Chatterji et al., 2007; Espino & Franz, 2002; Faught & Hunter, 2012; Gonzalez-Barrera & Lopez, 2013; Passel & Cohn, 2009; Pérez et al., 2008; Zsembik & Fennell, 2005). With the Mexican subgroup falling at the bottom of the SES bracket, its pattern lends support for Healey and O’Brien’s (2014) statement on their persistent poverty, resembling African Americans in the U.S. South (e.g., low-wage occupations). Whereas employment appears to protect only Cubans, education may benefit Mexicans and Puerto Ricans, suggesting differential subgroup social capitals.
With respect to study limitations, a cross-sectional design neither permits claims of causality nor eliminates rival explanations. A self-reported survey may not adequately reflect SRMH and SRH detectable through clinical diagnosis. The assessment reflects reductionism particularly in the measure of religious involvement, in a manner that is suboptimal for a complex construct. Intra-subgroup variations within each subgroup should be acknowledged. Not all Mexicans and Puerto Ricans are disadvantaged with respect to national origins, SES, and acculturation. Early Cuban immigrants tended to be more affluent and educated, hold more resources, and own businesses, but recent counterparts tend to be worse off financially (Healey & O’Brien, 2014). The NLAAS did not collect data on acculturation stress for U.S.-born respondents who may experience it too. The study explains only a small proportion of SRMH and SRH for Mexicans. In-depth research is warranted for this largest subgroup.
Despite these caveats, the study adds new value to the Latino research literature. Although not all cultural strength factors may be protective for all subgroups, the inconsistent finding does not discredit them as cultural resources. Interpretations for mixed links must be made in line with their subcultural experiences. Our findings also imply that psychologists’ assumptions about the role of cultural strengths in socially disadvantaged group can be better understood in the subcultural context. The findings require further investigation and confirmation through rigorous clinical and prospective studies.
Footnotes
Acknowledgements
The authors gratefully acknowledge the contributions of Jeffrey Shook, PhD/JD, to initial reading of the first draft manuscript and of Harold Weiss, PhD, to initial data analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.