
Abstract
The aim of the present study is to investigate the efficacy of internet-based cognitive behavior therapy (ICBT) for individuals with social anxiety (SA) and different levels of Taijin Kyofusho (TKS) in China. The ICBT program was translated into Chinese with some specific contents adapted for Chinese culture. Participants (N = 80) with SA were assigned either to a treatment (n = 55) or control group (n = 25). Both groups were further divided into subgroups, based on their Taijin Kyofusho Scale (TKSS) scores. Participants in the ICBT treatment group reported significant posttreatment reductions in Social Interaction Anxiety Scale and Social Phobia Scale scores, relative to participants in the control group. In addition, participants in the treatment group with higher pretreatment TKS levels showed significantly greater reductions in TKSS scores. Results suggest that ICBT is a promising approach for the treatment of individuals with SA both with and without features of TKS. Clinical and cross-cultural implications, mechanisms of change, limitations, and future directions are discussed.
Individuals with social anxiety (SA) tend to fear and avoid social situations, often due to an excessive concern about embarrassing themselves. Taijin Kyofusho (TKS) is a culturally bound form of SA, more commonly seen in Eastern cultures where individuals worry that their behaviors, expressions, or physical characteristics will offend or make others feel uncomfortable (Kleinknecht et al., 1997). Similar to SA, individuals with TKS also report avoidance behaviors, including avoidance of social situations or eye contact, and physical discomfort, including shaking, sweating, and muscular tension. However, rather than a preoccupation with self-embarrassment, as found in SA, individuals with TKS fear embarrassing others. As such, SA and TKS have been described as self- and other-focused manifestations of SA, respectively (Norasakkunkit et al., 2012).
Taijin Kyofusho was first proposed by Shoma Morita, a Japanese psychiatrist (Kleinknecht et al., 1997). Since the 1920s, it was included as a diagnostic category for Japanese patients with SA disorder. Both the Diagnostic and Statistical Manual of Mental Disorders (fifth edition; DSM-5; APA, 2013) and the International Classification of Diseases (10th edition; ICD-10; World Health Organization, 1992) recognize TKS as a component of SA disorder, meaning TKS symptoms are not prerequisite for SA disorder (Lim, 2013). Studies have shown the co-occurrence in SA individuals with TKS is more than 50% in both the United States and Japan (Kleinknecht et al., 1997), and that the correlation between self-report measures of SA and TKS are significantly higher in Eastern countries, such as China and Japan (Wang et al., 2018; Zhu et al., 2014).
The prevalence rates of TKS have been shown to be higher in Eastern countries compared with Western countries (Essau et al., 2012; Vriends et al., 2013; Wang et al., 2018). For example, Vriends et al. (2013) found that TKS is more prevalent in college students in Indonesia than in Switzerland. Similar results were found when comparing students in China and Japan to students in the United States and England (Essau et al., 2012; Wang et al., 2018). On the contrary, the prevalence of SA disorder in Western countries, such as the United States (approximately 7%; Ruscio et al., 2008) and Brazil (approximately 9%; Vorcaro et al., 2004), are higher than those in Eastern countries, where approximately 0.2%, 0.6%, and 0.8% of the population are diagnosed with SA disorder using psychiatric surveys in China (Shen et al., 2006), Korea (Cho et al., 2007), and Japan (Kawakami et al., 2005), respectively.
Culturally Divergent Self-Construals and Cognitive Processes in SA and TKS
As SA is related to the interactions between people, the importance of cultural context in SA cannot be ignored (Zhu et al., 2014). Cultural differences may lead to different kinds of SA, such as TKS. Sato et al. (2014), for example, found that low relational mobility may lead to high sensitivity to rejection and TKS symptoms, which is particularly common in East Asian cultures where people try to maintain social harmony and avoid potential rejection from others. Self-construals (independent vs. interdependent) are another factor related to SA and TKS (Dinnel et al., 2002; Zhou et al., 2014). An independent self-construal reflects an image of self that tends to emphasize the separateness and uniqueness of an individual, whereas a person with a predominantly social orientation of self as interdependent with others tends to emphasize one’s connectedness and relations (Markus & Kitayama, 1991). Thus, individuals with an interdependent self-construal are more likely to believe one’s failure would bring shame not only on oneself, but also on one’s family. As such, these individuals with an interdependent self-construal tend to primarily turn their attention outward, and—in the context of SA—are more likely to excessively monitor their environment for signs that their behavior may be harming others. To support this view, research has demonstrated a strong association between self-construal and SA variables (Okazaki, 2002). Specifically, interdependent and independent self-construal scores are strongly associated with self-report measures of TKS and SA, respectively (Norasakkunkit et al., 2012). That is, in East Asian countries, such as Japan and China, where people tend to emphasize more interdependent self-construals, the “other-focused” component of SA (i.e., TKS) is more common than the “self-focused” component of SA (Kleinknecht et al., 1997). In contrast, in North American cultural contexts, where people tend to emphasize more independent self-construals, the most common feature of SA is “self-focused” and characterized by a tendency for excessive concern of embarrassing oneself in social situations. In this “self-focused” SA, one selectively attends outward to monitor the environment for social cues that one is possibly failing to make a good impression.
Research on cultural differences in cognitive processes further elucidates the differences between SA and TKS. According to this line of research, cultural differences in self-construals (independent vs. interdependent) were related to cognitive processes (holistic vs. analytic), which, in turn, were associated with SA and TKS. Masuda et al. (2008) demonstrated that East Asians tend to pay attention to the entire visual field of a picture (holistically), whereas North Americans tend to pay significantly more attention to the central figure in the picture (analytically). Norasakkunkit et al. (2012) found Japanese participants to report both higher holistic cognition and TKS scores, while North American participants reported higher SA scores, which were associated with decreased levels of holistic cognition.
Internet-Based Treatment of SA
Internet-based cognitive behavioral therapy (ICBT) is one of the treatments that has been shown to be efficacious in treating SA (Berger et al., 2009, 2011). ICBT is a general concept referring to an online self-help intervention based on cognitive behavioral therapy. There are many different versions of ICBT targeting different conditions, such as depression, generalized anxiety disorder (GAD), and posttraumatic stress disorder (PTSD; Dear et al., 2011; Richards & Richardson, 2012; Spence et al., 2011). Researchers at the University of Bern in Switzerland designed an online, self-guided intervention for SA (Berger et al., 2009) based on Clark and Wells’ (1995) cognitive behavioral model. This was one of the first ICBT interventions for treating SA. Henceforth, this intervention will be referred to as Berger et al.’s ICBT. This intervention includes psycho-education (e.g., readings elucidating the mechanism of SA), emotion regulation skills (e.g., relaxation) and practice assignments (e.g., exposure to feared stimuli). Besides improving SA symptoms, there was also a study showing changes in related symptoms and cognitions using the Chinese version of Berger et al.’s ICBT, such as depression (Kishimoto et al., 2016). These findings suggest this self-guided intervention has potential to yield improvements in other domains of mental health, beyond SA symptoms. Accordingly, the present study aims to explore the efficacy of Berger et al.’s ICBT program in reducing symptoms of TKS among participants with SA in China.
A growing body of research has demonstrated that traditional individual psychotherapy models are proving incapable of addressing the mental health needs globally (Becker & Kleinman, 2013), especially in China (Cyranoski, 2010) where psychologists/counselors are lacking (Qian et al., 2010). New approaches are needed to increase access to effective mental health care in a way that is culturally informed, economical, feasible, and scalable. ICBT is one promising solution to closing the large gap between mental health treatment need and actual treatment received. The Chinese version of Berger et al.’s ICBT program for SA has already been researched among Chinese samples. Results suggest the intervention is efficacious in treating SA (Chen et al., 2012), as well as depression (Kishimoto et al., 2016).
Although empirical studies in Japan provide preliminary support for interventions treating TKS, including Morita Therapy and antidepressants (Nagata et al., 2005), no study has examined the efficacy of an intervention for TKS in China. Given that SA and TKS share similar symptoms, we are interested in exploring whether Berger et al.’s ICBT could be effective in treating not only SA, but also TKS symptoms in China.
Aims and Hypotheses of the Present Study
Accordingly, the aims of this study are to investigate the efficacy of Berger et al.’s ICBT for SA individuals with TKS symptoms and to compare the relative efficacy of ICBT for SA without TKS symptoms. Given that ICBT was designed to treat SA and that all participants in the current study met criteria for SA, our first hypothesis is that both SA groups, those with and without TKS, will demonstrate significant reductions in SA symptoms. Although individuals with SA and TKS exhibit some different symptoms, they also share some symptoms in common. Given the overlap in symptoms in SA and TKS and the fact that we use an ICBT program which has undergone cultural adaptation, we assumed SA individuals with TKS in China can also benefit from the ICBT program. Therefore, our second hypothesis is that among SA individuals with TKS, participants in the treatment group will report significant posttreatment reductions in TKS symptoms compared with control group participants.
Method
Participants and Recruitment
Participants were recruited through various sources, including poster advertisements at the Peking University counseling center, the university listserv/BBS, and on Wechat 1 forums. Individuals aged 18–35 years who were interested in the study completed a battery of self-report measures online (N = 354). 2 Participants with Social Interaction Anxiety Scale (SIAS) scored above 32 (Berger et al., 2011; Kishimoto et al., 2016) were invited via email to participate in a structured diagnostic interview. Participants were interviewed by trained professionals with a background clinical psychology using the Mini-International Neuropsychiatric Interview (MINI) either face to face, via video conference, or by phone. See Figure 1 for exclusion criteria. Participants who reported suicidality were excluded and referred to counseling services. In all, 80 participants met study eligibility criteria. These individuals received an email with instructions for accessing the ICBT program and informed consent materials. The present study was approved by the ethics committee in School of Psychological and Cognitive Sciences at Peking University.
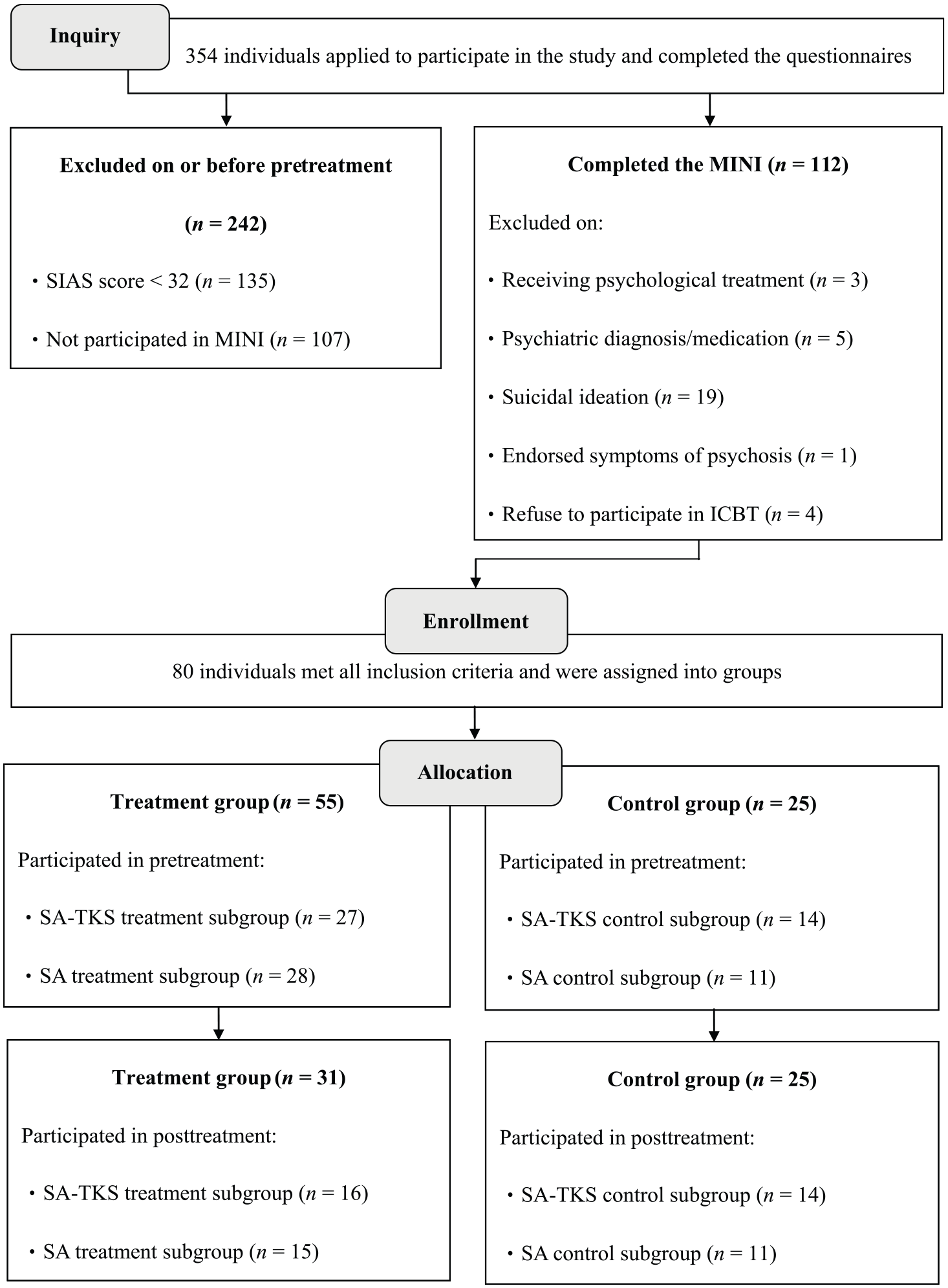
Participant flow.
Materials
SIAS
The Chinese version of the SIAS (Ye et al., 2007) is a widely used scale designed to assess SA symptoms during social interactions. Nineteen items are included and are rated from 4 = extremely to 0 = not at all. Confirmatory factor analysis showed that this single-factor scale has adequate construct validity (χ2/df = 3.20, p < .001; goodness-of-fit index [GFI] = .832, adjusted goodness-of-fit index [AGFI] = .790, comparative fit index [CFI] = .838, Tucker–Lewis Index [TLI] = .818, root mean square error of approximation [RMSEA] = .090), and the Cronbach’s α is .75 indicating adequate internal consistency in the current study.
Social Phobia Scale (SPS)
The Chinese version of the SPS (Ye et al., 2007) is a widely used measure designed to assess anxiety in social situations. Twenty items are rated from 4 = extremely to 0 = not at all. Confirmatory factor analysis showed that this single-factor scale has adequate construct validity (χ2/df = 3.23, p < .001; GFI = .802, AGFI = .755, CFI = .835, TLI = .815, RMSEA = .091), and the Cronbach’s α is .87 indicating high internal consistency in the current study.
Taijin Kyofusho Scale (TKSS)
The TKSS (Kleinknecht et al., 1997; Wang et al., 2018) is a 31-item scale designed to assess participants’ concern that they would do something to offend or embarrass others. Items were assessed on a 7-point scale, from 1 = exactly true to 7 = totally false. The total score for each participant ranged from 31 to 217. The English, Japanese, and Chinese versions of the TKSS have been demonstrated to possess robust internal consistency with Cronbach’s αs of .93, .92, and .94, respectively, for American, Japanese, and Chinese individuals (Kleinknecht et al., 1997; Wang et al., 2018). Confirmatory factor analysis showed that this single-factor scale has good construct validity (χ2/df = 3.26, p < .001; CFI = .93, incremental fit index [IFI] = .93, Bentler–Bonett Normed Fit Index [NFI] = .91, RMSEA = .093), and the Cronbach’s α is .91 indicating high internal consistency in the current study.
MINI (Chinese version)
The MINI (Si et al., 2009) is a structured interview designed to assess psychological symptoms and diagnoses according to the Diagnostic and Statistical Manual of Mental Disorders (fourth edition; DSM-IV; American Psychiatric Association, 1994) and ICD-10. It was designed by Sheehan et al. (1997) with the purpose of screening individuals’ psychiatric symptoms within a short amount of time (approximately 30 min). The psychiatric symptoms are calculated based on the instructions of the MINI. The Chinese version of the MINI (Si et al., 2009) had high Cronbach’s α (.94) and test–retest reliability (.97).
ICBT Intervention
Authorization to use Berger et al.’s (2009) ICBT intervention in the current study was obtained from the University of Bern in Switzerland. The program contains eight modules and six assignments (see Table 1). It requires approximately 8 weeks to complete. All course materials and assignments are provided on the internet, and participants complete the readings and assignments on their own. Participants could contact researchers via email if they had questions about the lessons. The content of the ICBT used in this study was translated from German to Mandarin by two bilingual psychologists worked in Germany and also revised by a group of eight clinical psychologists (including one psychology professor and seven graduate psychology students).
Overview of ICBT Modules and Assignments.

Note. ICBT = internet-based cognitive behavior therapy.
Minor adaptations were made to the ICBT materials (e.g., culturally relevant illustrations) to better suit Chinese participants. For example, in the fourth module “Attention Training,” one of the exercises in Berger et al.’s ICBT was to tell a 1-min story in front of an image of an audience. During the talk, participants should pay attention to their thoughts, emotions, and feelings. The story was based on European history. We believed most Chinese participants would not relate to the story, so we replaced it with a story based on Chinese history and context. In other words, the structure of Berger et al.’s ICBT did not change, only materials that were strongly culturally oriented and may influence efficacy were revised for the Chinese participants.
Procedure
Individuals interested in the study completed a battery of self-report measures online (TKSS, SIAS, and SPS). Eligible participants (i.e., those with SIAS scores > 32) were invited to participate in a structured diagnostic interview (MINI) by researchers with a background in clinical psychology. A weighted randomization procedure (Berger et al., 2009) was used to assign eligible participants to treatment conditions; two thirds of participants were assigned to the treatment group and one third to the control group. Each group was further assigned to subgroups based on their TKSS scores (Figure 1). The treatment subgroups were the SA with TKS treatment subgroup (SA-TKS treatment subgroup; SIAS scores > 32 and TKSS scores ≥ 130; n = 27) and SA without TKS treatment subgroup (SA treatment subgroup; TKSS scores < 130; n = 28). The wait-list control subgroups were the SA with TKS control subgroup (SA-TKS control subgroup; TKSS scores ≥ 130; n = 14) and the SA without TKS control subgroup (SA control subgroup; TKSS scores < 130; n = 11).
Participants were requested to complete one module each week. However, they could complete them at their own pace within 8 weeks of enrollment. Course content was unlocked after participants completed the previous week’s readings and assignments. Participants were encouraged to continue practicing the exercises and tasks from the previous modules. After 8 weeks, participants were locked out of the program. During the intervention, participants in the treatment group could contact a researcher with questions about the website or course through email.
Participants completed a posttreatment battery of measures following completion of the ICBT course. Participants in the control group received a posttest battery (TKSS, SIAS, and SPS) 2 months after the pretest measures were completed, and then they received access to the same ICBT course after completing the ICBT course.
Power Analysis
G*Power Version 2 (Mayr et al., 2007) was used to calculate sample size. Results suggested that 54 participants were sufficient for a medium effect size (f = .25) using mixed analysis of variance (ANOVA).
Statistical Analyses
The Reliable Change Index (RCI)
RCI (Jacobson & Truax, 1991) is a within-individual difference score which was used to examine the reliability of the observed changes in participants’ pre- and posttreatment scores. The formula is as follows:
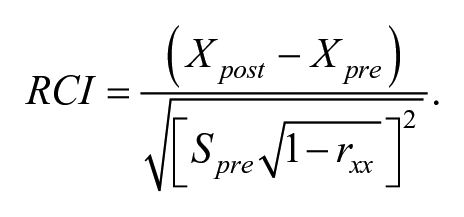
Xpost = participants’ posttreatment score; Xpre = participants’ pretreatment score; Spre = standard deviation in pretreatment score in the whole sample; rxx = retest reliabilities in the scale. If the RCI value is greater than 1.96, the magnitude of that change is believed to represent a clinically significant improvement. Conversely, RCI values below −1.96 suggests reliable deterioration, and RCI value between −1.96 and 1.96 suggests a nonsignificant change. Intention-to-treat analyses were also used to calculate improvement rates based on the number of the participants in the initially assigned treatment groups including dropouts.
Hierarchical linear modeling (HLM)
HLM (Gai & Zhang, 2005; Singer & Willett, 2003) is used to examine repeated measures data that are nested in multiple levels. In the present study, the repeated measurement (time variable: 0 = posttreatment, 1 = pretreatment) of the dependent variables (SIAS and SPS) in Level 1 are nested within other independent variables in Level 2, which include the SA symptom (0 = SA without TKS, SA-TKS; 1 = SA with TKS, SA), treatment (0 = ICBT; 1 = control condition), age and gender (0 = male; 1 = female).
To test Hypotheses 1, to determine whether time had a significant effect on the dependent variables (SIAS and SPS scores), we first ran an unconditional linear model with the time variable (pre- and posttreatment) as a predictor in Level 1. Next, we ran another unconditional linear model with SA symptom (SA with or without TKS), treatment (ICBT or control condition), gender and age in Level 2 to examine whether these predictors had an effect on SIAS and SPS scores. Third, a conditional linear model was run to examine the results within and between subjects.
Mixed ANOVA
To test Hypothesis 2, mixed ANOVA was used to compare mean TKSS change scores in the SA with TKS control and treatment subgroups (SA-TKS treatment vs. SA-TKS control subgroup).
Results
Demographics
Tables 2 and 3 show the demographic descriptions of participants and descriptive statistics for all scales, respectively. The correlations among the pairs of the three scales were also provided in Table 4.
Demographic Data for All Participants.
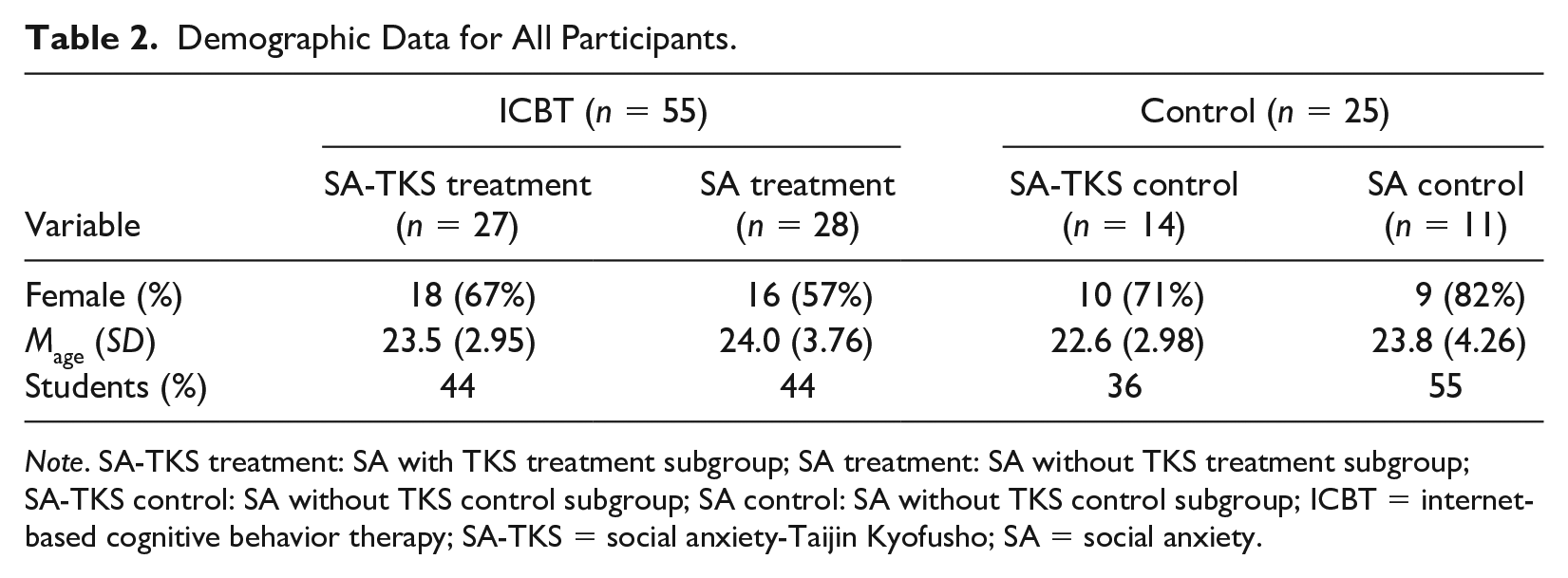
Note. SA-TKS treatment: SA with TKS treatment subgroup; SA treatment: SA without TKS treatment subgroup; SA-TKS control: SA without TKS control subgroup; SA control: SA without TKS control subgroup; ICBT = internet-based cognitive behavior therapy; SA-TKS = social anxiety-Taijin Kyofusho; SA = social anxiety.
Mean Values and Standard Deviations for Each Group.
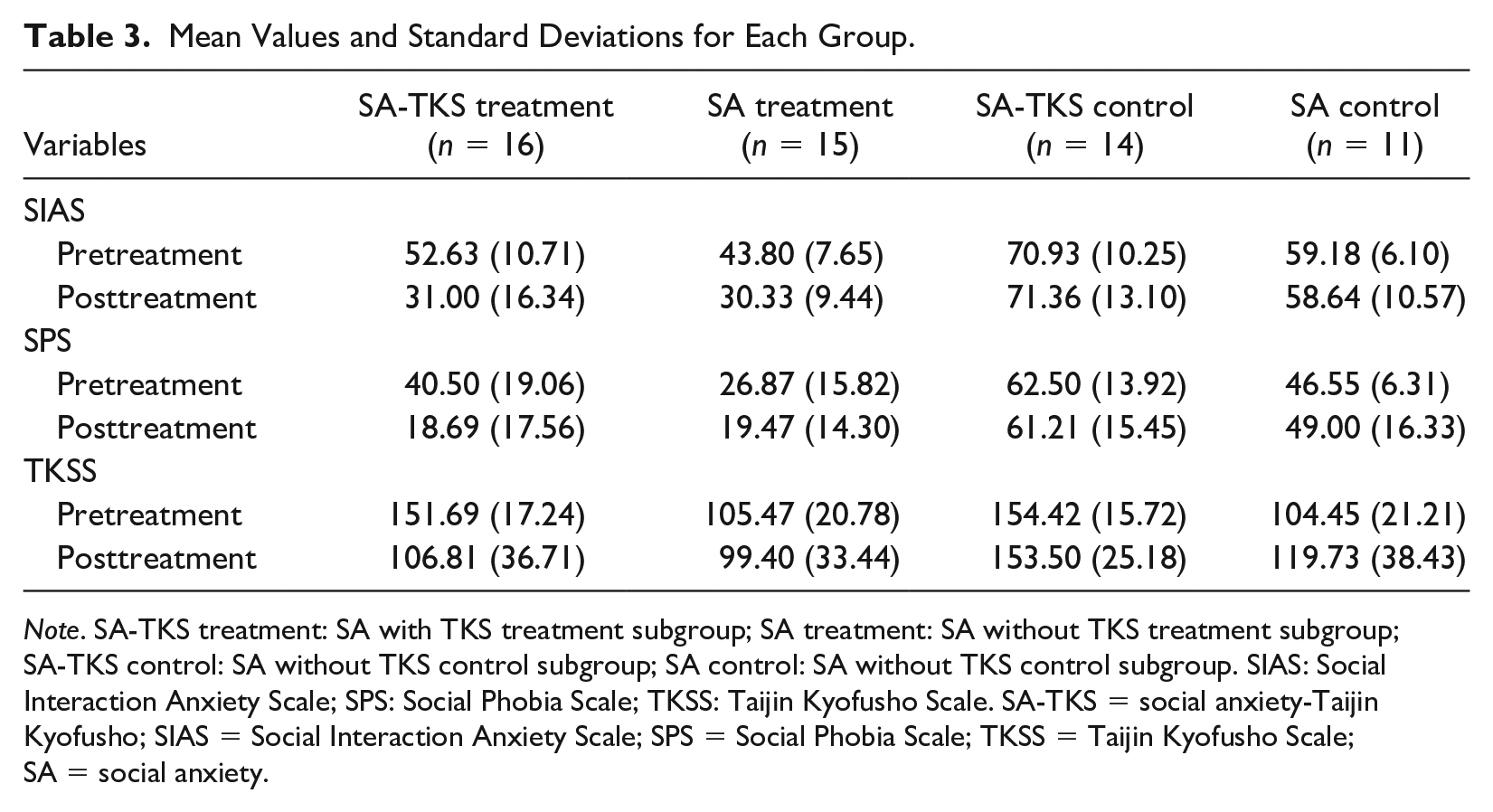
Note. SA-TKS treatment: SA with TKS treatment subgroup; SA treatment: SA without TKS treatment subgroup; SA-TKS control: SA without TKS control subgroup; SA control: SA without TKS control subgroup. SIAS: Social Interaction Anxiety Scale; SPS: Social Phobia Scale; TKSS: Taijin Kyofusho Scale. SA-TKS = social anxiety-Taijin Kyofusho; SIAS = Social Interaction Anxiety Scale; SPS = Social Phobia Scale; TKSS = Taijin Kyofusho Scale; SA = social anxiety.
Correlations Between SIAS, SPS, and TKSS Scores.
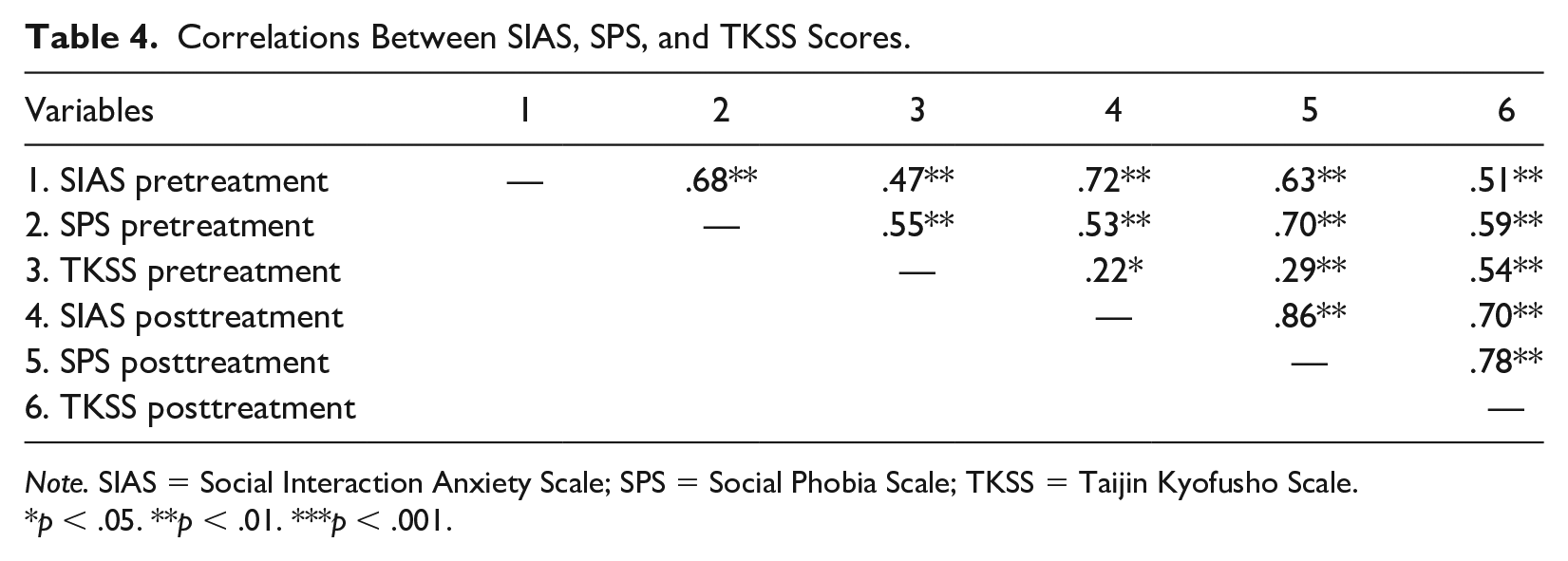
Note. SIAS = Social Interaction Anxiety Scale; SPS = Social Phobia Scale; TKSS = Taijin Kyofusho Scale.
p < .05. **p < .01. ***p < .001.
Adherence and Attrition
Table 5 showed the percentages of adherence in each module and treatment subgroup. Participants who completed less than two modules or did not complete posttest were regarded as dropouts. For SA-TKS treatment subgroups, 11 participants were considered dropouts, wherein nine participants completed less than two modules and two participants completed all of the modules but did not complete posttest assessments. For SA treatment subgroups, 13 participants were considered dropouts, wherein 11 participants completed less than two modules and two participants completed all of the modules but did not complete posttest assessments. Participants who completed three or more modules and also completed posttest assessments were regarded as completers. The SA-TKS and SA treatment subgroups had 16 and 15 completers, respectively.
Adherence in Each Module and Groups.
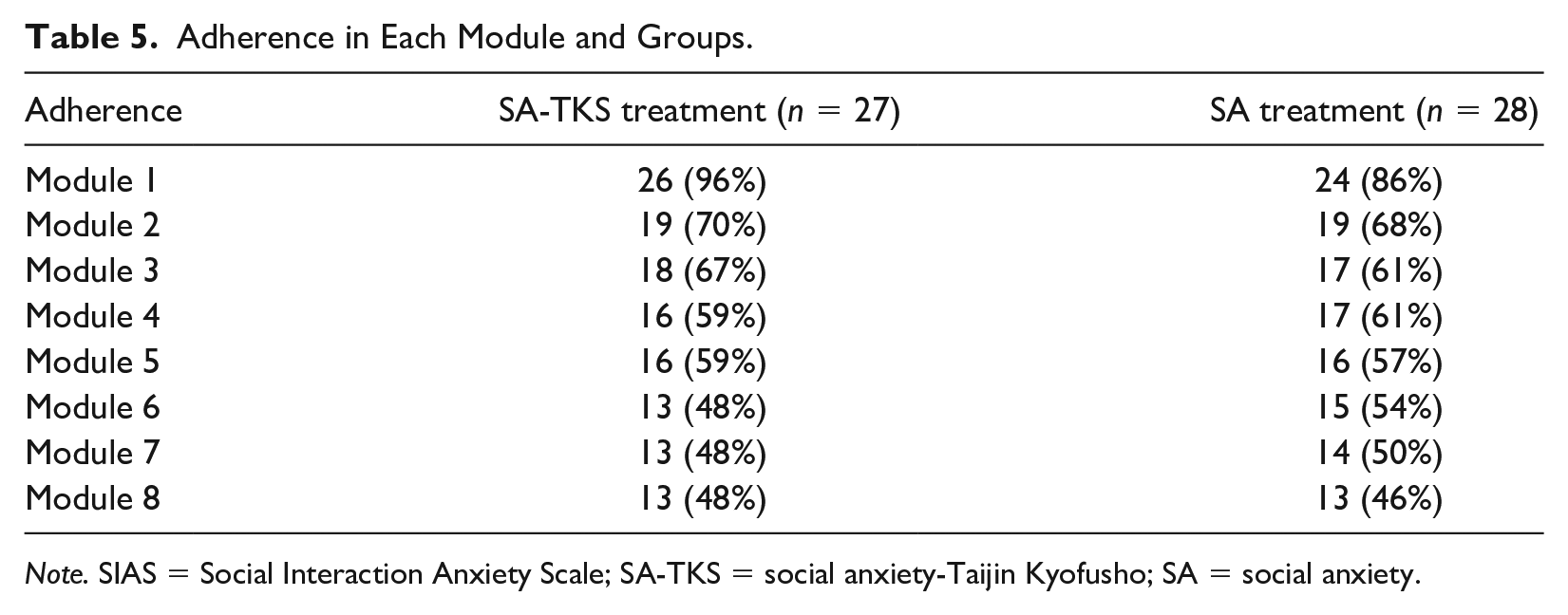
Note. SIAS = Social Interaction Anxiety Scale; SA-TKS = social anxiety-Taijin Kyofusho; SA = social anxiety.
The mean number of completed modules was 5.00, SD = 3.20 (n = 27), in the SA-TKS treatment subgroup and 4.79, SD = 3.46 (n = 28). Chi-square showed nonsignificant difference between groups in the adherence of all modules (χ2 = 5.78, p = .57), including dropouts.
RCI
Intention-to-treat analyses were used to estimate results, which indicated that among the 55 participants in the treatment group, 42% (n = 12 in SA-TKS treatment subgroup; n = 11 in SA treatment subgroup) and 29% (n = 11 in SA-TKS treatment subgroup; n = 5 in SA treatment subgroup) of participants reported significant improvements (RCI > 1.96) in SIAS and SPS scores, respectively. None of treatment group participants reported significant deterioration (RCI < .96) in SIAS and SPS scores. The pretreatment to posttreatment effect size (Cohen, 1998) based on the paired t test was large for SIAS but small for SPS, t(54) = 5.53, p < .001, d = .80 and t(54) = 3.84, p < .001, d = .48; SIAS and SPS, respectively.
Among the 25 participants in the control group, 20% (n = 2 in SA-TKS control subgroup; n = 3 in SA control subgroup) and 12% (n = 1 in SA-TKS control subgroup; n = 2 in SA control subgroup) of participants reported improvements in SIAS and SPS scores, respectively. Also, 8% (n = 0 in SA-TKS control subgroup; n = 2 in SA control subgroup) and 8% (n = 0 in SA-TKS control subgroup; n = 2 in SA control subgroup) of control group participants reported deterioration in SIAS and SPS scores, respectively.
For participants in the SA-TKS treatment and control subgroups, intention-to-treat analyses were used to estimate the results, which indicated that among the 27 participants in the SA-TKS treatment subgroup, the improvement rate was 44% (n = 12) and the deterioration rate was 4% (n = 1) in TKSS scores. Among the 14 participants in the SA-TKS control subgroup, 7% (n = 1) of participants reported improvement and 7% (n = 1) reported deterioration in TKSS scores. The pretreatment to posttreatment effect size based on the paired t test was large, d = .92, t(26) = 3.97, p = .001. These results support our first and second hypotheses.
HLM
The results for the full HLM analyses are reported in Tables 6–8. Model 1, an unconditional linear model, indicated a significant slope across time for SIAS and SPS. Intention-to-treat analysis was used in which the pretreatment data was forward for the dropouts to replace missing values (posttreatment scores). These results indicate that time was a significant predictor of SIAS and SPS in Level 1. In addition, the significance of the residual for SIAS and SPS indicated that there were differences among individuals. Therefore, more variables should be examined in Level 2 to further elucidate these results. Model 2, an unconditional linear model, indicated that treatment (ICBT or control condition) was also a significant predictor of SIAS and SPS in Level 2. Age and sex were not significant predictors of outcomes, and therefore both variables were eliminated in Level 2 in Model 3.
Results From Model 1.

Note. df = 154; Level 1: time variable (pre- and posttreatment). SIAS = Social Interaction Anxiety Scale; SPS = Social Phobia Scale.
p < .05. **p < .01. ***p < .001.
Results From Model 2.
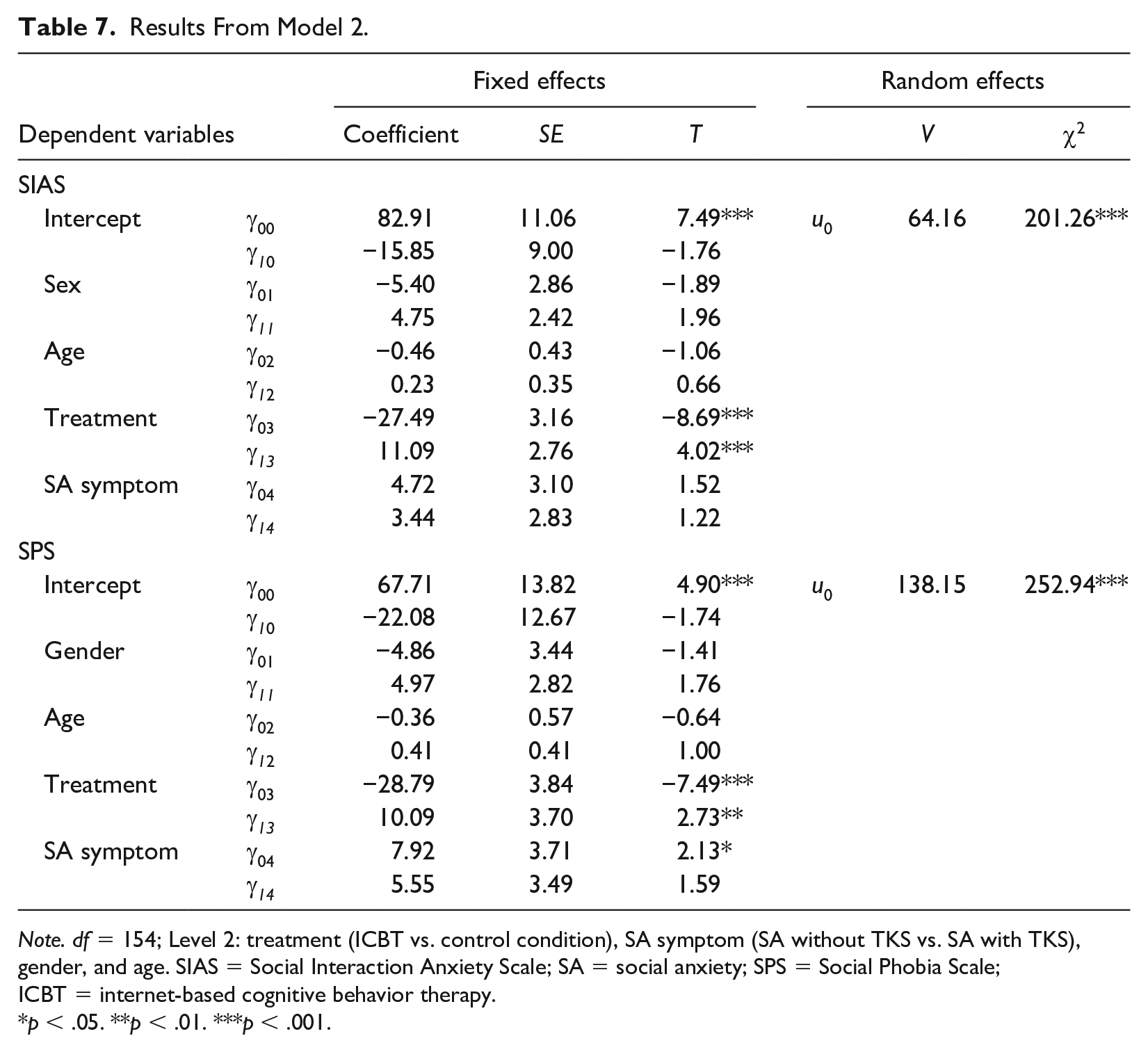
Note. df = 154; Level 2: treatment (ICBT vs. control condition), SA symptom (SA without TKS vs. SA with TKS), gender, and age. SIAS = Social Interaction Anxiety Scale; SA = social anxiety; SPS = Social Phobia Scale; ICBT = internet-based cognitive behavior therapy.
p < .05. **p < .01. ***p < .001.
Results for Model 3.
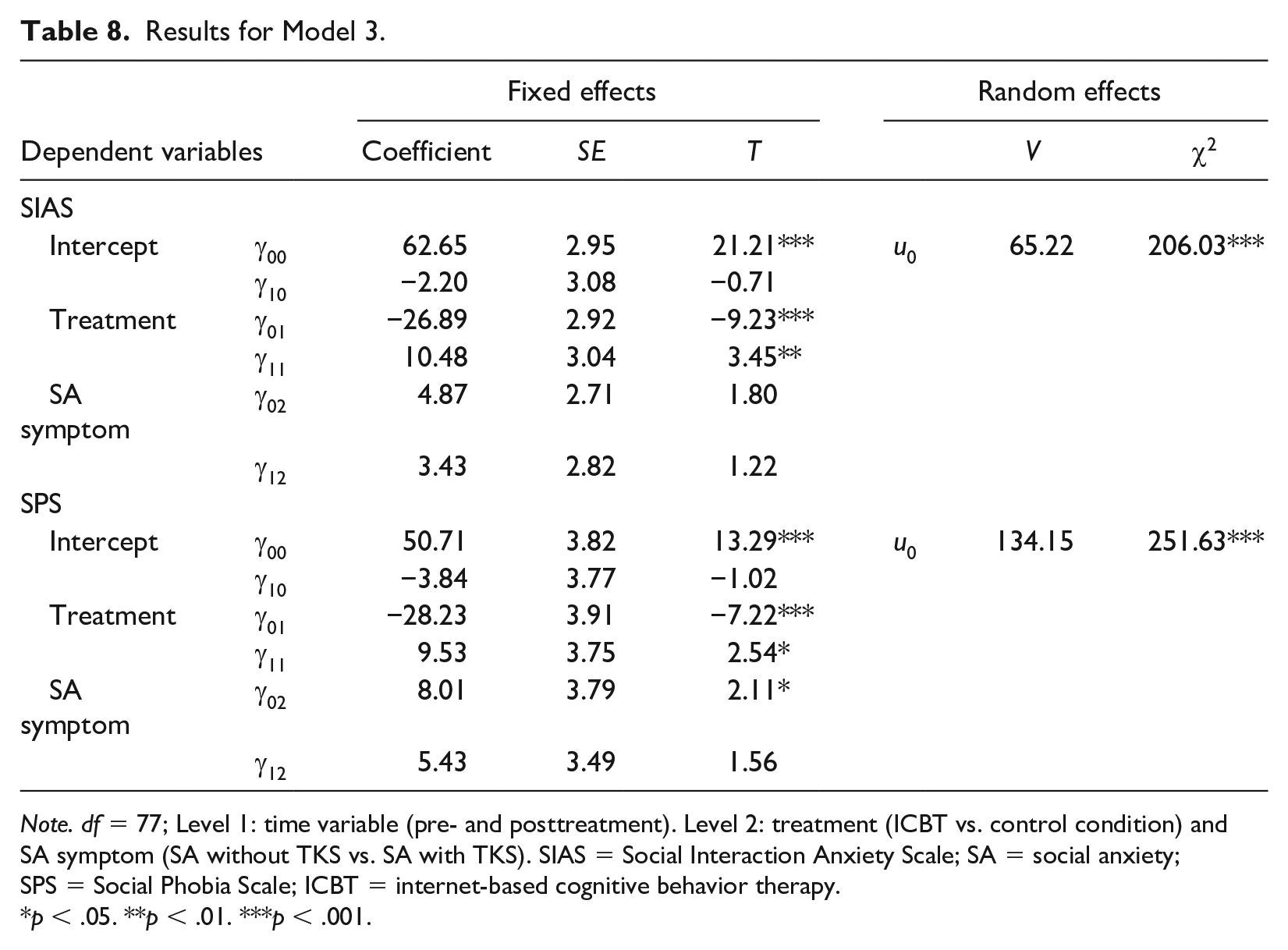
Note. df = 77; Level 1: time variable (pre- and posttreatment). Level 2: treatment (ICBT vs. control condition) and SA symptom (SA without TKS vs. SA with TKS). SIAS = Social Interaction Anxiety Scale; SA = social anxiety; SPS = Social Phobia Scale; ICBT = internet-based cognitive behavior therapy.
p < .05. **p < .01. ***p < .001.
The final model (Model 3) was a conditional model including the time variable in Level 1, SA symptom and treatment in Level 2, and SIAS and SPS as dependent variables. Results demonstrated significant differences between the treatment and control groups. Specifically, participants who received ICBT reported greater reductions in SIAS and SPS scores. Moreover, there was no significant difference between SA symptom, indicating that participants who received ICBT reported reductions SIAS and SPS, with no significant differences between the SA treatment and SA-TKS treatment subgroups.
TKS Treatment Versus Control Subgroups
The SA-TKS treatment and SA-TKS control subgroups were analyzed using a 2 × 2 mixed-design ANOVA. Comparisons between the SA-TKS treatment and SA-TKS control subgroups revealed interaction effects for TKSS scores, F(1,41) = 9.70, p = .003. The partial η² was .19, which represents a large effect size (Cohen, 1998). The SA-TKS treatment subgroup demonstrated significant reductions in TKSS scores (pretest M ± SD: 152.22 ± 16.27, posttest M ± SD: 125.63 ± 37.49), while SA-TKS control subgroup participants did not report significant changes in their scores on the measure (pretest M ± SD: 149.00 ± 20.89, posttest M ± SD: 153.88 ± 35.49). These results support our second hypothesis.
Discussion
The present study explored the efficacy of ICBT for SA individuals in China with and without TKS features. Consistent with previous research conducted in Switzerland (Berger et al., 2009, 2011), the Chinese version of the ICBT program demonstrated efficacy in reducing symptoms of SA among participants in China (Kishimoto et al., 2016). Moreover, despite research demonstrating important cross-cultural differences in holistic cognition and self-construals between the different manifestations of SA (Norasakkunkit et al., 2012), results from the present study suggest Berger et al’s ICBT can be used to treat SA individuals both with and without TKS.
Although the program was designed for SA individuals and does not specifically target TKS symptoms, it is not surprising that Berger et al.’s ICBT was found to be effective in treating TKS symptoms in SA individuals with TKS. This may be due to the high correlation among SIAS, SPS, and TKSS scores in our current sample. Since previous studies have shown that the fear of making others uncomfortable—one of the core features of TKS—is an integral part of SA among the Chinese and even central to East Asian cultural scripts for SA (Zhou et al., 2014; Zhu et al., 2014), it is possible that TKS symptoms may reduce when SA symptoms are reduced even though the former is not targeted in the ICBT. Another possible explanation may be that this program teaches individuals skills to have greater awareness and control of their attention, thinking, and emotions. These skills are used in a variety of treatments for mental health problems, including SA and TKS. For example, relaxation techniques, problem-solving strategies, and exposure practices are used to help overcome the problematic cognitive (e.g., exaggeration of threat), emotional (e.g., fear of fear), and behavioral (i.e., avoidance) patterns common across both components of anxiety. In fact, these treatment components are common across most CBT-based treatments for anxiety disorders, including panic, GAD, and PTSD (Dear et al., 2011; Spence et al., 2011).
One limitation in our study was that our sample was primarily young female university students in China. It will be important for researchers to replicate our findings with larger, more diverse and multi-national samples. A second limitation is the absence of a standard treatment control group, such as CBT individual therapy. Nonetheless, we believe a wait-list control group was sufficient for the purpose of the present study, as the large effect size found in our study warrants future research with a larger sample and with clinical populations diagnosed with SA disorder.
The present study makes a novel contribution to the literature by providing preliminary results supporting the efficacy of ICBT for reducing reported features of both SA and TKS. However, since our ICBT program was translated from the Berger et al. version with minimal cultural adaptation, future research should revise our version to explore the effect of more substantive cultural adaptations, such as adding content about self- and other-focused SA symptoms. Future research should also conduct a component analysis of each module to explore differences in the relative efficacy of the course content and assignments in the ICBT program for the two components of anxiety (SA vs. TKS) and between cultures (e.g., Switzerland vs. China). This line of research may also help better understand the nature, treatment and cross-cultural factors underlying the two types of SA. Finally, future studies should examine ICBT with clinical samples who present with TKS, that is, individuals with TKS, but not SA. This study indicates improvement in TKS symptoms; therefore, it is important to know if individuals with TKS but without SA can also benefits from ICBT.
Clinical implications suggest that ICBT could assist individuals not only in reducing their SA symptoms, but also their TKS symptoms. Furthermore, ICBT not only demonstrates clinical efficacy in Western countries (Berger et al., 2009), but also in China (Kishimoto et al., 2016), where people tend to have different self-construals and cognitive processes. As such, ICBT demonstrates potential for helping close the treatment gap for SA in China.
Footnotes
Authors’ Note
Marcus Rodriguez is also affiliated with Boston Child Study Center, Boston, MA, USA. Yin Yang is now affiliated with Beijing Sport University, Beijing, China.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the National Social Science Foundation of China (Grants 15ZDB139).