
Abstract
This population-based study (N = 908,468) examines the effects of spousal loss on being absent from work due to illness or injury (sickness absence) among employed individuals in Norway. Fixed-effects models capturing antecedent and short- and long-term effects of spousal loss over a 15-year period were estimated to explore gender and age differences in the impact of widowhood. The crisis model, the social-role model, and the life course perspective are discussed. Furthermore, the study calls into question whether parenthood explains the gendered age gradient of the widowhood effect. The results show that the theoretical relevance of the crisis and social-role models is best understood in dialogue with a gendered life course approach. The results show that the crisis response is especially high among young widowers, whereas the recovery period is markedly prolonged among young widows. Parenthood at the time of widowhood explains much of the age difference among widowers and widows.
Although the transition to widowhood is a natural and inevitable part of the life course for many people, spousal loss has long been considered the most distressing life event, especially when it occurs at a young age (Holmes and Rahe 1967; Kraus and Lilienfeld 1959). Indeed, extensive research has shown that widowhood is associated with a multitude of adverse health outcomes, including excess mortality (e.g., Shor et al. 2012), lower levels of self-reported health (Joung et al. 1997; Lee et al. 2001; Liu 2012; Liu and Umberson 2008; Williams and Umberson 2004), higher levels of drug use and depression (Barrett 2000; Carnelley, Wortman, and Kessler 1999; Carr and Utz 2001; Lee and DeMaris 2007; Sasson and Umberson 2014; van Grootheest et al. 1999; Wheaton 1990), higher prevalence of chronic conditions and diseases (Dupre and Meadows 2007; Hughes and Waite 2009), lower levels of life satisfaction (Næss, Blekesaune, and Jakobsson 2015), and higher levels of sickness absence (Vahtera et al. 2006) compared with married individuals. Recently, there has been a growing interest in how the timing of spousal loss in relation to chronological age affects health outcomes following widowhood (Carr and Utz 2001; Dupre, Beck, and Meadows 2009; Dupre and Meadows 2007; Hughes and Waite 2009; Liu 2012; Liu and Umberson 2008; Sasson and Umberson 2014; Wheaton 1990; Williams and Umberson 2004). However, empirical evidence of how age interacts with widowhood and health remains ambiguous, although mortality studies have generally found that younger individuals, especially men, are more vulnerable to widowhood than are older individuals (for a review, see Shor et al. 2012).
The purpose of this study was to analyze the health effects of losing one’s spouse at a relatively early life stage using long-term sickness absence as measure of general health. Sickness absence is here defined as absence from work, because of illness or sickness lasting 15 days or longer, that was approved by a treating doctor. Administrative data covering the entire Norwegian population over 15 years were used to address two research questions: (1) How do short- and long-term effects of widowhood vary by age and gender? (2) To what extent does parenthood explain the gendered age gradient of the widowhood effect?
In Norway, complete sickness absence periods lasting 15 days or longer are available in population-based registries dating back to 1993, with data on a multitude of sociodemographic variables, including detailed family history. As a health measure, long-term sickness absence has the advantage of being assessed and approved by a treating doctor. Norway’s generous and universally available sickness absence policy, in combination with one of the highest labor participation rates among the Organization for Economic Cooperation and Development (OECD) countries (particularly among women; OECD 2013), makes sickness absence data a valuable measure of general health. Indeed, sickness absence, especially long-term sickness absence, is a reliable indicator of health among employed individuals, covering a wide range of sicknesses and diseases (Kivimäki et al. 2003; Melchior et al. 2003; Suominen et al. 2007). Previous research on marital status and sickness absence has made important contributions to our understanding of marital status and health (Blekesaune and Barrett 2005; Dahl, Hansen, and Vignes 2015; Kivimaki et al. 1997, 2002; Suominen et al. 2007; Vahtera et al. 2006), although to my knowledge no studies have explored age differences in the effects of widowhood on sickness absence.
Background
The impact of widowhood on health has been discussed predominantly in relation to two influential theoretical models of marital status and health: the social-role model and the crisis model. The social-role model, dating back to the classical sociological work of Durkheim ([1897] 1952), focuses on the protective effects of marriage on individuals and on the chronic strain of not being married. According to this perspective, being married is assumed to facilitate social integration, emotional support, and economic and material well-being, and to discourage unhealthy behaviors, such as smoking, alcohol consumption, drug use, an unhealthy diet, and avoidance of health checkups. Correspondingly, the social-role model assumes that losing one’s spouse, either through divorce or widowhood, will result in a permanent loss of such health-related advantages as long as the individual stays unmarried (Booth and Amato 1991). Furthermore, the protective and detrimental features of marital statuses are assumed to operate differently for men and women, causing a gendered balance of costs and rewards when entering and exiting marriage (Williams and Umberson 2004).
With respect to health, men are usually assumed to benefit more from marriage than are women, as wives are better than husbands at providing social and emotional support, and thus men lose more than women when widowed. Women are better at receiving and seeking social support outside marriage than men are and therefore are able to maintain high levels of social integration even after marital disruption (Umberson, Wortman, and Kessler 1992). For example, Pihlblad and Adams (1972) found that five years after widowhood, men lost 50% of their social network, whereas women experienced no reduction. Women, however, are assumed to be more vulnerable than men to economic and material losses when exiting marriage (Umberson et al. 1992), although it is likely that inheritance and welfare transfers moderate such losses when exiting marriage through widowhood (Joung et al. 1997; Lillard and Waite 1995). A fundamental assumption underlying the social-role model is that the protective and detrimental features of marriage and widowhood persist, or even accumulate, over time (Liu 2012).
According to the crisis model, health differences between marital groups are caused not by the permanent benefits of being married or the chronic strains of being outside marriage but by the temporary stress reactions associated with the transitions between roles. In the case of widowhood, the traumatic experience of losing one’s spouse may elicit intense grief, feelings of helplessness, loneliness, insomnia, and suicidal ideation (Stroebe, Schut, and Stroebe 2007). Such psychological symptoms of bereavement have been linked to somatic and immune-endocrine outcomes (e.g., Gerra et al. 2003). In addition, widowhood not only entails the loss of a loved one but marks the transition to a new lifestyle and circumstances to which individuals must adjust. Spousal loss may therefore create stresses that are likely to diminish over time, such as economic stress, parental stress, and stress associated with increased household tasks (Hemstrom 1996; Liu 2012; Smith and Zick 1996; Umberson 1987).
There is empirical support for both the social-role and crisis models, leading most to conclude that the two models should be viewed as complementary processes. Several studies have found excess mortality and depression levels to be highest 6 to 12 months following widowhood, after which they decline to a level similar to or marginally higher than those among continuously married individuals (Brockmann and Klein 2004; Carnelley et al. 1999; Johnson et al. 2000; Lee, Willetts, and Seccombe 1998; Martikainen and Valkonen 1996b). Similar findings have also been reported with regard to self-reported health (Barrett 2000; Liu and Umberson 2008), depressive symptoms (Sasson and Umberson 2014), and sickness absence (Vahtera et al. 2006). Others have found support for the social-role model and observed an elevated risk of experiencing death or chronic conditions long after the transition to widowhood (Berntsen and Kravdal 2012; Blomgren et al. 2012; Carr and Utz 2001; Hughes and Waite 2009). Much research has shown that these long-term effects are higher among men than among women (Brockmann and Klein 2004; Dupre and Meadows 2007; Johnson et al. 2000; Joung et al. 1997; Martikainen and Valkonen 1996a; Rogers 1995; Schaefer, Quesenberry, and Wi 1995; van Grootheest et al. 1999), although some studies have found higher excess mortality among widows compared with widowers (Berntsen and Kravdal 2012; Manor and Eisenbach 2003). Vahtera et al. (2006) found higher sickness absence rates immediately after family death or serious illness and a longer recovery period among women than among men.
Age and Bereavement
Partly in an attempt to overcome the theoretical dichotomy of the social-role and crisis models, a growing body of research inspired by the life course perspective conceptualizes widowhood as a critical life event embedded in changing historical and social contexts (Carr and Utz 2001; Dupre et al. 2009; Dupre and Meadows 2007; Hughes and Waite 2009; Liu 2012; Liu and Umberson 2008; Sasson and Umberson 2014; Wheaton 1990; Williams and Umberson 2004). These authors understand widowhood as a potential trigger event that alters individual trajectories of mental and physiological health over the life course. However, they emphasize that the level and type of stress reactions induced by the transition to widowhood, as well as the role features of widowhood itself, vary across different contexts. Particular focus has been on the timing of critical life events in relation to chronological age and the shifting functioning of the marital institution over time (e.g., Barrett 2000; George 1993).
An underlying assumption in this research is that the health effects of widowhood are worse if spousal loss happens at an unusual or vulnerable stage of the life course. For example, it is possible that there is a “pileup” effect of stressors over the life course, leaving older individuals less capable of managing critical life events (Ensel et al. 1996; Williams and Umberson 2004). For example, older adults are more likely to have weaker social networks and fewer friends than are younger individuals (Stephens et al. 2011). On the other hand, it is possible that widowhood at a younger age is associated with additional stressors and strains, such as parenting or increased economic hardship. For example, it is more likely that younger widows and widowers need to adjust to both the loss of a loved one as well as to increased childcare responsibilities (Hemstrom 1996; Joung et al. 1997; Liu 2012; Smith and Zick 1996).
Previous studies have shown that having children elevates the risk of receiving sickness absence benefits when divorced (Blekesaune and Barrett 2005; Dahl et al. 2015). Dahl et al. (2015) found that the long-term effects of divorce on sickness absences were especially high among women with children. In this group, the sickness absence rate was nine percentage points higher five years after divorce compared to the married years preceding divorce, whereas the difference was only two percentage points among men. However, it is likely that parenthood affects divorced and widowed individuals differently. First, whereas children necessarily stay with the remaining spouse when widowed, mothers are most often left with the childcare responsibilities after divorce. In Norway, only 7% to 8% of divorced men have primary custody of their children (Lyngstad, Kitterød, and Nymoen 2014). Second, it is reasonable to suppose that conflict with the ex-spouse about child custody constitutes an important source of stress in divorce. Such extra strain is clearly not present in spousal loss, but it is possible that men struggle more with increased family responsibilities following spousal death than do women, who are generally more involved in childcare (Lee et al. 1998). On the other hand, it may be that the presence of children, especially older children, represents a source of social support when losing a spouse through death. Indeed, several studies have found lower excess mortality following widowhood among individuals with children (Hemstrom 1996; Manor and Eisenbach 2003; Mineau, Smith, and Bean 2002).
Although a great deal of research has shown age differences on the effect of widowhood (e.g., Williams and Umberson 2004), these results have remained ambiguous with regard to which age group is most vulnerable. It is likely that these discrepancies are caused by different measures of health, methodological approaches, and sample sizes. For example, mortality studies, most often based on population registries, have consistently found a stronger effect of widowhood among younger individuals compared with older individuals, especially among men (e.g., Johnson et al. 2000; Manor and Eisenbach 2003; Martikainen and Valkonen 1996b; Mineau et al. 2002; Smith and Zick 1996). In their review article of 123 publications on widowhood and mortality, Shor et al. (2012) conclude that men have higher excess mortality following widowhood than women but that men’s excess mortality declines more rapidly than women’s. By age 90, there is no gender difference in excess mortality following widowhood. Some studies have also found support for a negative age gradient of the widowhood effect, showing that widowhood at younger ages is associated with lower levels of self-reported health (Liu and Umberson 2008) and higher depression scores (Sasson and Umberson 2014). In contrast, Liu (2012) and Williams and Umberson (2004) found a positive age gradient of the widowhood effect, showing that the transition to widowhood is associated with worse health among older versus younger adults. Williams and Umberson (2004) even found evidence of a long-term positive effect of widowhood among younger men.
Selection Processes
Both the crisis and social-role models assume a causal relationship between widowhood and health with widowhood leading to worse health. However, it is possible that health differences between married and widowed individuals are caused not directly by the transition to widowhood but rather by selection processes. For example, positive associative mating may result in homogenous couples, causing husbands and wives to resemble each other on traits relevant to mortality and sickness absence (e.g., Kalmijn 1998). It is also possible that the bereaved shared an unfavorable environment with the deceased spouse, either in the form of an unhealthy lifestyle or a shared accident (Elwert and Christakis 2008; Hemstrom 1996; Martikainen and Valkonen 1996a; Sasson and Umberson 2014). Both situations could result in an association between widowhood and sickness absence even if the death of one had no causal effect on the sickness absence of the other. Although it is difficult to establish the relative importance of selection processes when studying marital status and health (e.g., Goldman 1993), findings from previous research indicate that such selection processes have limited power for explaining differences between widowed and married individuals. For example, Joung et al. (1998) found that the presence of chronic conditions among married individuals predicted divorce but not widowhood (see also Elwert and Christakis 2008).
In this article, I address selection processes by comparing the propensity of sickness absence following the transition to widowhood with the sickness absence rate before the spouse died. If spousal homogamy is an important factor in explaining sickness absence differences between continuously married and widowed individuals, there should be a high sickness absence rate among widowed individuals long before their transition to widowhood. However, as emphasized by Carr and Utz (2001), spousal loss often happens after a period of ill health, so the detrimental effects of widowhood may begin long before actual spousal death, even if selection processes are ruled out. In such cases, spousal loss may even produce an element of relief (Berntsen and Kravdal 2012; Wheaton 1990; Williams and Umberson 2004). To explore such processes and to avoid a misclassification of sickness absence rates during the baseline period, I estimated the antecedent effects of widowhood in addition to short- and long-term effects.
Data and Methods
The data for this study were from the longitudinal FD-Trygd database from Statistics Norway. This high-quality database was established in 1992 and covered all Norwegians 16 years and older. In these data, sociodemographic information was available from 1992, whereas income and welfare-related variables were added in 1993 and beyond. Because these data came from public registries, problems such as selection bias and sample attrition were reduced. For many variables, such as gender and marital status, there were no missing data; for other variables, missing data rates were negligible. For the purposes of this study, I organized the data into 15 waves (one per year from 1993 through 2007).
All workers ages 18 to 66 years were entitled to long-term sickness benefits paid by the National Insurance Scheme (NIS) if they had been employed for at least 14 days, their annual income was at least half the basic amount (US$5,100 in 2006), and their sickness could be categorized according to the Norwegian version of the International Classification of Primary Care. Grief or social issues did not qualify individuals for sickness absence benefits without a diagnosis, such as depression, anxiety, or sleep disturbance. The statutory sickness benefits were 100% of pensionable income and were paid from the first day of sickness for a period of 260 workdays. Sickness absence periods shorter than 15 days were unavailable in administrative registers and were therefore not analyzed. Although this was an important limitation of the data used in this study, previous research has shown that long-term sickness absence captures more serious ill health incidences and is a better predictor of mortality than short-term sickness absence (Kivimäki et al. 2003; Melchior et al. 2003; Vahtera, Pentti, and Kivimaki 2004). In addition, because long-term sickness absence had to be assessed and approved by a treating doctor, bias due to variations in individual tolerance levels when feeling unfit to work was reduced.
According to the NIS rules, I began by selecting individuals whose work income was at least half the basic amount. To ensure that all widowed individuals were observed for an adequate baseline period preceding spousal loss (at least four years), individuals who became widowed before 1997 were excluded. Analyses with a longer baseline did not lead to substantially different results. To reduce problems with outflow to the occupational early retirement scheme, which was available to about 60% of the working population after the age of 62 years, the sample was restricted to individuals born after 1945. Thus, the oldest widowed individual in my data experienced spousal loss at the age of 61 years in 2007 and was observed for the first time at age 48 in 1993. Correspondingly, the youngest widowed individual in this data set was born in 1965 and widowed in 1997 at 32 years and was 28 years old during the first observation year. Only continuously married individuals or those who experienced widowhood were included in analyses. The analyses were based on a total of 908,468 individuals, 17,720 of whom experienced spousal loss during the observation period.
Thus, compared with previous studies on the health effects of widowhood at younger ages, this study had the advantage of being based on a large number of younger widowed individuals, making it possible to study age and gender differences in the short- and long-term effects of widowhood on health over several years. However, to be included in the analyses, individuals had to be gainfully employed. It is unlikely that this sample restriction caused bias at the time of spousal loss, but it was possible that widowed individuals had a higher propensity of leaving the labor market than continuously married individuals (e.g., through unemployment, disability, emigration, or in the worst case, their own death). This may have led to downward biased estimates of the effect of widowhood on health, especially when estimating long-term effects of widowhood. To investigate a potential attrition bias among widowed individuals, I estimated rates of attrition due to unemployment (including retirement through disability pension), own death, and other loss of data (e.g., emigration, etc.) over five years for widowed and married individuals (see Table 1). Because rates of attrition out of the labor market are closely related to gender, age, and year, each widowed individual was matched to a randomly selected married individual with similar demographic information.
Attrition Rates Due to Unemployment, Own Death, or Other Loss of Data (Emigration, etc.) after Five Years for Widowed and Married Individuals, by Gender, FD-Trygd Database, 1993–2007 (N = 24,634).
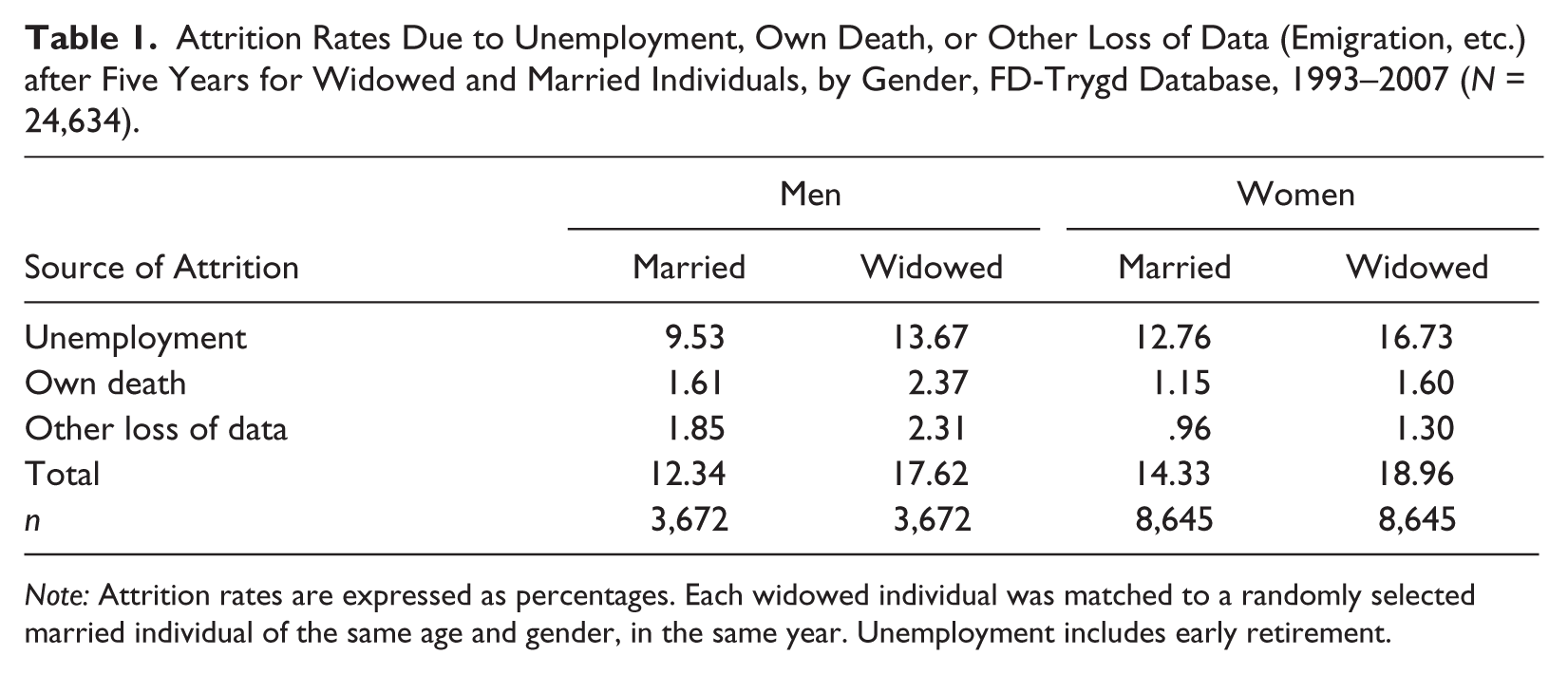
Note: Attrition rates are expressed as percentages. Each widowed individual was matched to a randomly selected married individual of the same age and gender, in the same year. Unemployment includes early retirement.
As expected, and in line with previous research, Table 1 shows that mortality and unemployment were higher among widowed individuals than among married individuals. In total, 17.6% of widowers left the labor market five years after the death of their wife, whereas 12.3% of married men left the labor market over the same period. Among women, as many as 19% of widows left the labor market, compared with 14.3% of married women. Thus, it is likely that employed widowers and widows are in better health compared to widowers and widows who have left the labor market. As a consequence of this selection bias, the long-term effects of widowhood on sickness absence should be interpreted with some caution. The implications of this potential attrition bias are further described in the Discussion section. In addition, because of a special agreement between the state and the NIS prior to 2000, information on state employees’ sickness absences before that time were insufficient or missing; thus, state employees before 2000, who represented about 7.5% of the total sample and 15% of the yearly observations, were excluded from analyses.
Sickness absence was treated as a dummy variable, coded as 1 for a reported period of sickness benefits in a given year and 0 otherwise. I also conducted analyses for which I used the number of sickness absence days as the dependent variable, but because this variable was severely skewed with many observations of 0, I used the dummy variable. However, the results did not differ substantially between these analytical approaches.
Because this article was concerned with how sickness absence rates change after the transition to widowhood compared with the married years preceding widowhood, linear probability fixed-effects regression models with robust standard errors were used. Traditionally, logit models are viewed as more suitable for discrete dependent variables, because these models guarantee that the probability of y = 1 falls between 0 and 1, and because they are better suited to binary response distributions. Nevertheless, the advantages of using logit probability models compared with linear probability models have been disputed (e.g., Hellevik 2009; Mood 2010). In addition, when estimated on panel data, fixed-effects logit regression models put serious restrictions on the estimation sample, as they can include only units that change the value of the dependent variable during the observation period. Because of these limitations, I estimated linear probability models. It should be noted, however, that results from logit fixed effects models do not differ markedly from the results reported herein.
To ensure that the model was sensitive to the temporal processes associated with widowhood (i.e., separation of preceding, short-term, and long-term effects), the effects of widowhood were captured by a set of eight “pulse variables” (Di, j ), which took the value of 1 in the jth period before and after the transition to widowhood and 0 otherwise (for discussions on dynamic treatment effects, see Andreß, Golsch, and Schmidt 2013; Laporte and Windmeijer 2005; Lechner 2015). The fixed-effects panel data model was therefore:

where Xit was a set of time-varying control variables, and β and γ were vectors of parameters to be estimated. The event of widowhood was captured by eight dummy variables: (1) Di,–3, which equals 1, to indicate three years preceding widowhood; (2) Di,–2 = 1, if there were two years preceding widowhood; (3) Di,–1 = 1, in the year preceding widowhood; (4) Di,0 = 1, in the year of spousal death; (5) Di,1 = 1, in the first year following widowhood; (6) Di,2 = 1, in the second year following widowhood; (7) Di,3 = 1, in the third and the fourth; and (8) Di,4 = 1, in the fifth and subsequent years after spousal death. The baseline period was the years of marriage, excluding the final three years before widowhood. Thus, this approach captured the preceding effects of widowhood with γ−3, γ−2, and γ−1; an immediate effect with γ0; short-term effects with γ1 and γ2; and long-term effects with γ3 and γ4.
Because fixed-effects models were applied, all unobserved time-invariant variables (ai) were controlled for. This ensured that potential, permanent health differentials between individuals who stayed married and who became widowed (i.e., selection processes) were dealt with effectively. Because fixed-effects models provide estimates only for variables that change during the observation period, no estimate of the sickness absence rates for married individuals was given by the model. Because this study was concerned primarily with how the health situation changed when entering widowhood, this was a minor analytic problem. However, sickness absence rates for married individuals were provided as descriptive statistics (see Results section).
Six time-varying measures were included in the models. First, a dummy variable of 1 was used if the individual entered a new marriage after experiencing widowhood and 0 for all other observations. According to the social-role model, entering a new marriage would remove the chronic strain of being widowed and restore the protective features of marriage, primarily among men. Second, a metric variable capturing the individual’s adjusted household income was included. Widowhood is likely accompanied by a loss of income, especially among women, as well as a reduced household size (e.g., van Grootheest et al. 1999). In general, there is an inverse relationship between income and health, which could be explained by material conditions, working conditions, and health behaviors (e.g., Ross, Mirowsky, and Goldsteen 1990). Using the modified equivalent scale developed by OECD (2015), the income variable was calculated by adjusting the total household income according to the number and ages of household members. Thus, this variable ensured that incomes of heterogeneous households were converted into comparable units of economic welfare. Given that the analyses were restricted to employed individuals, the amount of missing income data was negligible. Third, a dummy variable of 1 was used if the individual’s full-time work was included. Fourth, a measure of the municipal unemployment level was included. An inverse relationship between unemployment and sickness absence has been previously reported, which has been explained by social stress and health selection (i.e., people entering and leaving the labor market depending on the state of their health and the unemployment rate; e.g., Alexanderson et al. 2003). Fifth, to ensure that the estimates were not biased by seasonal fluctuations (e.g., changes in the sickness absence policy or the labor market), a set of year dummy variables was included. Because fixed-effects models estimate within-individual changes, the year dummy variables also captured the effect of aging; however, the relationship between aging and sickness absence is known to be nonlinear. A squared term of age was therefore included in the models. As a result of this approach, the linear relationship between age and the likelihood of sickness absence was captured by the year dummy variables, and the squared term captured the nonlinear effect of age. Descriptive statistics for all independent variables are in Appendix Table A1 (in the online supplemental material, available at journals.sagepub.com/home/hsb).
Gender, Age, and Parenthood When Widowed
As discussed in the Background section, previous research has repeatedly shown that the impact of widowhood on health varies with gender and age. The inherent downside of estimating fixed-effects models is that it is not possible to include time-invariant independent variables. However, it is possible to explore interaction effects either by performing separate analyses for subgroups or by including interaction terms (e.g., Andreß et al. 2013). Both approaches were used here. First, separate fixed-effects models were estimated for women and men. Second, in order to study how age interacts with the effect of widowhood on health, a dummy variable for age at widowhood (32 to 45 years) was estimated in interaction with the time dummy variables (Di, j ) (widowhood in the age category 46 to 61 years was the reference category). Analyses with more age groups (yielding very similar estimates) were also performed, but only two age groups were applied to increase comprehensibility and limit data output.
As hypothesized in the Background section, it is possible that having children when widowed elevates the stress response and either prolongs or shortens the recovery period when adapting to the new life situation. As suggested by several scholars, it is also possible that the presence of children may explain the age gradient of the widowhood effect. To investigate this, two dummy variables measuring the presence of (1) children under 11 years and (2) children 11 years and older when widowed were estimated in interaction with the post-widowhood time dummy variables (Di,0–Di,4). In these analyses, the reference category was widowed individuals without children at the time of spousal loss. The time dummy coefficients are presented in the figures, whereas the regression models are presented in Appendix Table A2 (in the online supplemental material, available at journals.sagepub.com/home/hsb).
Results
Figure 1 shows the descriptive sickness absence rate across the observation years for men and women who were widowed or continuously married at ages 32 to 45 and 46 to 61 years. First, as many previous studies have shown, there were considerable gender and age differences in the sickness absence rates. Middle-aged individuals have a higher probability of receiving sickness absence benefits compared with younger individuals, and women’s sickness absence rate is higher than that of men. Second, independent of age, the sickness absence rate among widowers and widows, respectively, is about 13 and 15 percentage points higher than those continuously married.
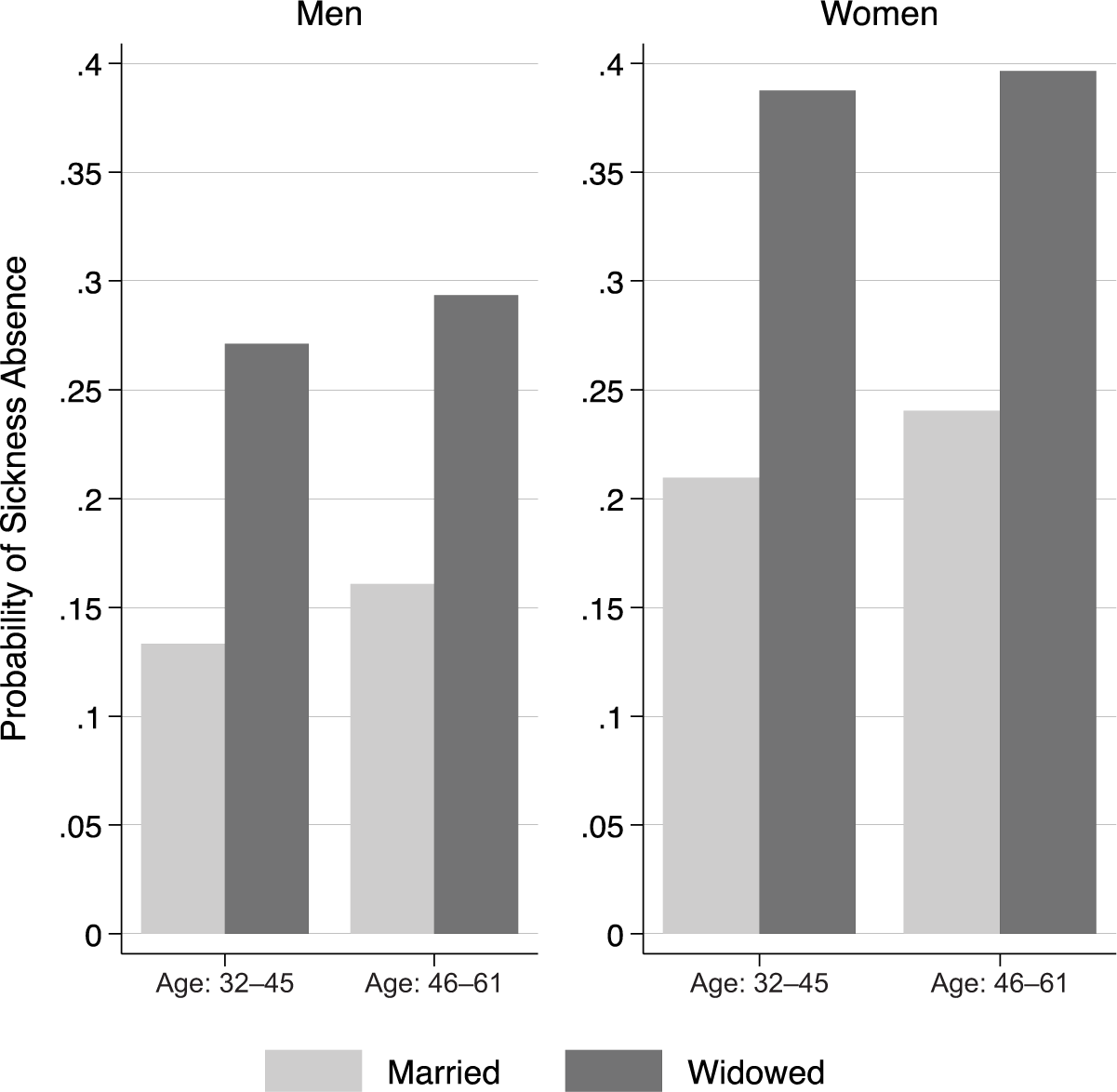
Sickness Absence Rate by Marital Status, Age, and Gender, FD-Trygd Database, 1993–2007 (N = 908,468).
Figure 2 shows how the sickness absence rates change over time for those who experience widowhood, relative to those who remain married during the observation period within the same age group. First, four to five years preceding spousal death, widowers have a rate of sickness absence similar to that of continuously married individuals in the same age category. Thus, it seems reasonable to conclude that selection processes do not explain widowed individuals’ high sickness absence rate. Second, the sickness absence rate increases sharply in the years preceding spousal loss and peaks in the year of spousal death for all groups. For women and younger widowers, the sickness absence rate increases with about 35 percentage points in the year of spousal death. Compared with the pre-widowhood level, this represents a nearly fourfold increase in sickness absence among men and a threefold increase among women. Among men who experience widowhood when middle-aged, the peak is somewhat lower. Third, widowed individuals have a high rate of sickness absence long after the transition to widowhood, especially among women who experience widowhood at an early life stage. In this group, the sickness absence rate actually increases further to more than 35 percentage points one year after spousal loss and thereafter drops to about 10 percentage points higher five years or more after spousal loss. Thus, widowhood seems to elicit a high crisis response among younger widowers, whereas spousal loss is associated with a prolonged recovery period among younger widows.
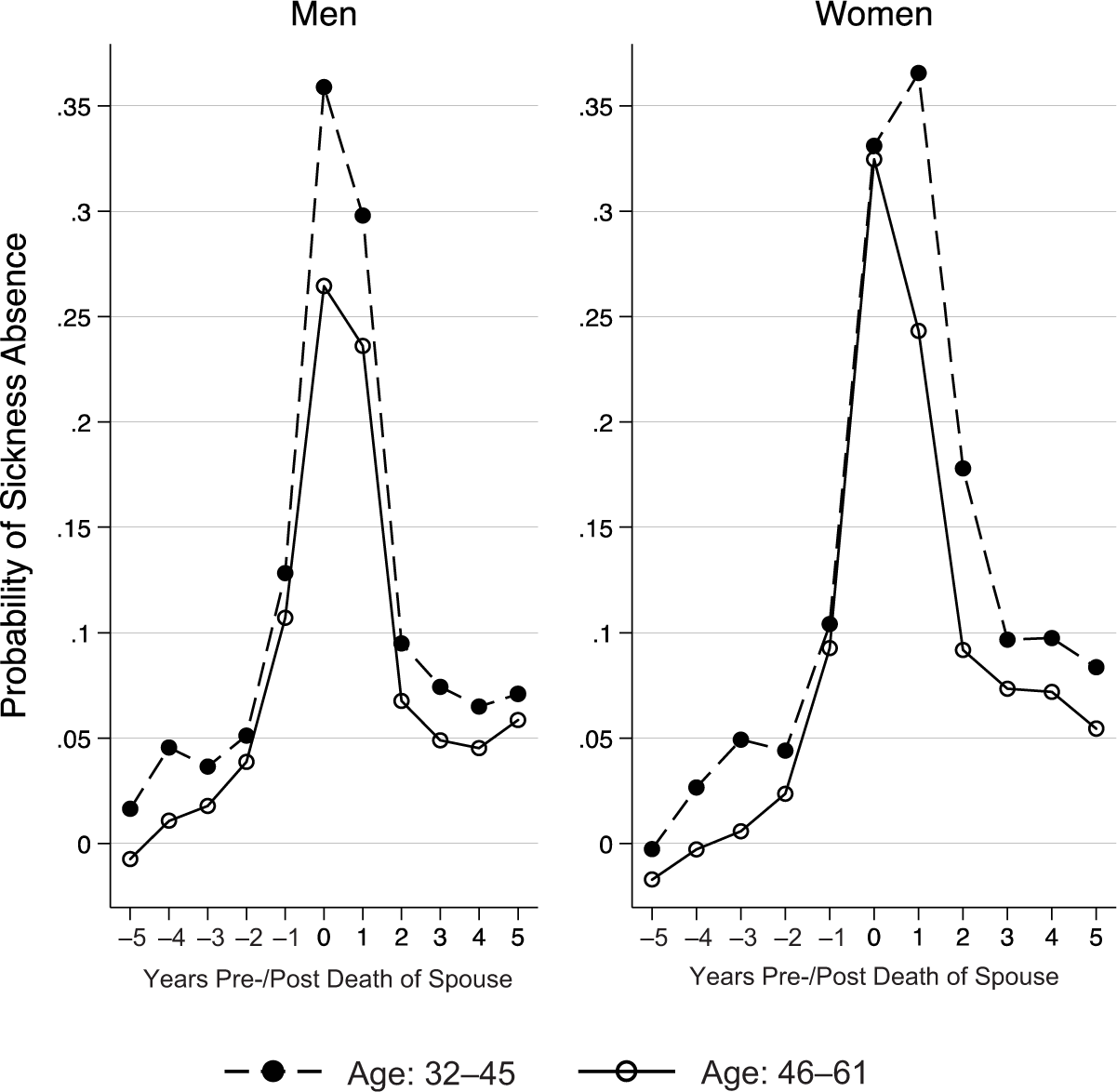
Sickness Absence Rate before and after Spousal Loss Compared with Those Continuously Married (Indicated by 0 on the y-axis) by Age and Gender, FD-Trygd Database, 1993–2007 (N = 908,468).
Figure 2 provides descriptive information uncontrolled for other factors, such as aging, changes in household income, and seasonal fluctuations. For instance, it may well be that the relatively high sickness absence rate long after the transition to widowhood is the result of individuals growing older or stress associated with income loss. To handle such confounding factors and to explore how the presence of children moderates or facilitates the effects of widowhood, I estimated linear probability fixed-effects models separately for men and women. Eight time-specific dummy variables around the event of spousal loss, in interaction with age, capture the lag and lead effects of widowhood and provide gender- and age-sensitive estimates of how the sickness absence rates changes from the married years preceding spousal death into widowhood. The baseline period covers the married years (four or more) before the event of spousal death. The full models are presented in Appendix Table A2 (in the online supplemental material, available at journals.sagepub.com/home/hsb).
The results of the linear probability fixed-effects models are shown in Figure 3. It is important to note that the effects of spousal loss among young individuals (age 32 to 45) are calculated by summarizing the coefficients for middle-aged widowed individuals and the interaction coefficients. Overall, this graph displays a similar pattern to that observed in the descriptive statistics, but after controlling for aging, changes in household income, and seasonal fluctuations, there is little evidence of a lasting effect of widowhood five or more years after spousal loss. Among widowers, the sickness absence rate is only about 2.6 percentage points higher five or more years after spousal loss compared with the married years preceding widowhood, whereas among middle-aged widows, we observe a full adaption to the pre-widowhood level (–.002). However, in line with the social-role model, Table A2 reveals that remarriage is associated with a further decrease in the sickness absence rate, especially among men. On average, remarriage is associated with a 1.6-percentage-point reduction in the sickness absence rate among widows and a 4.4-percentage-point reduction among widowers. In other words, the relatively small long-term disadvantage associated with being widowed disappears completely when widowers remarry.
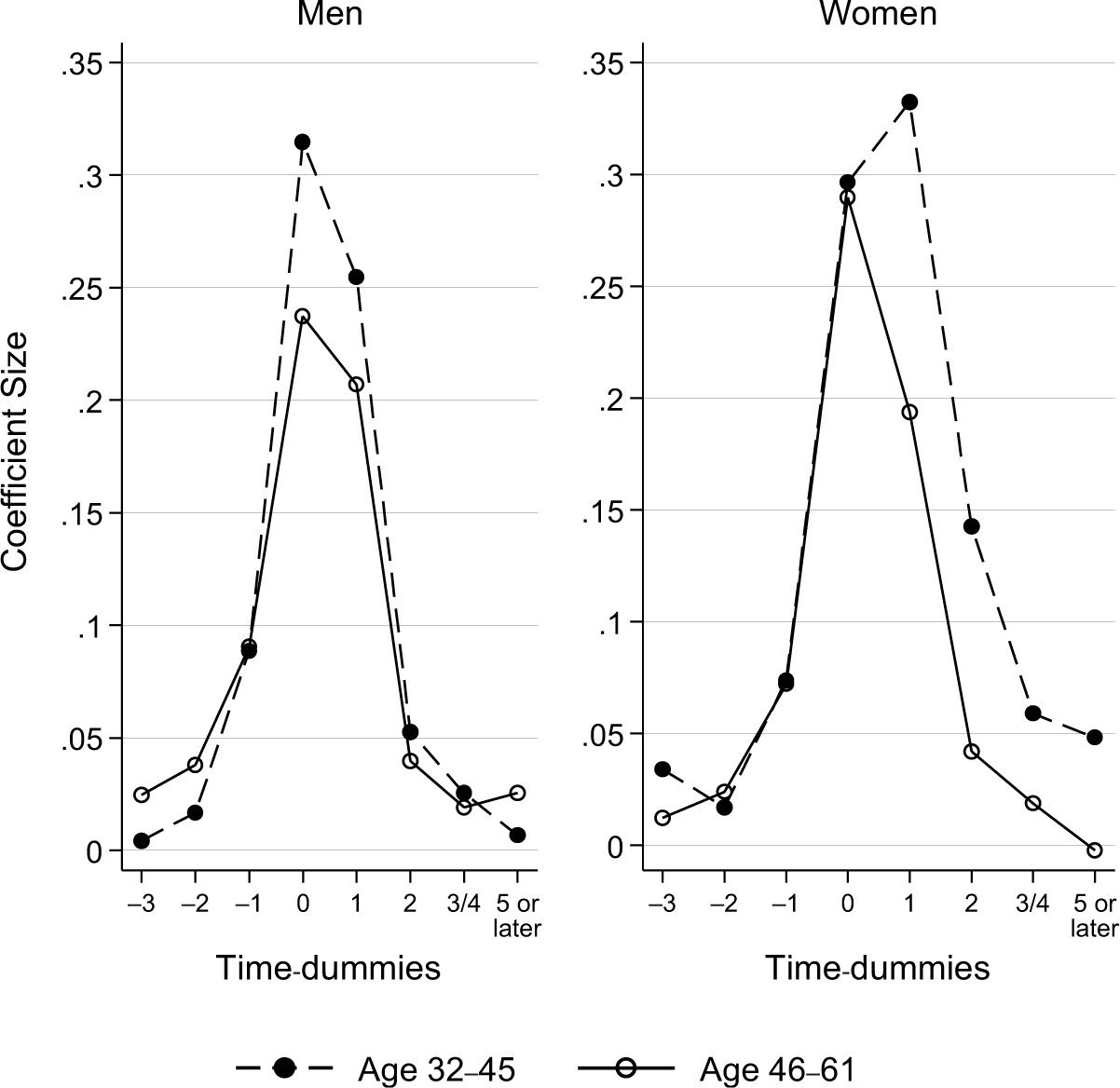
Time-dummy Coefficients from the Linear Fixed-effects Models: Model 1 by Age and Gender, FD-Trygd Database, 1993–2007 (N = 908,468).
The transition to widowhood is first and foremost associated with a severe crisis reaction in the years immediately surrounding spousal loss. The sickness absence rate increases with about 30 percentage points among widows and younger widowers compared with the pre-widowhood period and thereafter drops greatly during the following years. Among women who experience spousal loss at an early life stage, the recovery period is markedly prolonged. In this group, the average sickness absence rate is almost 15 percentage points higher than during the reference period two years after spousal loss (.042 + .101). Even five or more years following spousal loss, the sickness absence rate is 5 percentage points higher compared with the pre-widowhood period. Among men, the long-term effects of spousal loss are not apparently influenced by the age at which the transition occurs, but there is a higher crisis response in the year of spousal death and in the following year if widowhood occurs during the youngest age period. Thus, we observe that age at the time of widowhood makes important contributions to how widowhood affects the sickness absence rate, albeit differently among widowers and widows.
As discussed in the Background section, it is reasonable to expect that the age gradient of the widowhood effect will be related to parenthood and the presence of children. To investigate this, a set of interaction variables was used to measure how the crisis response and recovery period differ among widowers and widows who had younger and older children at the time of widowhood. As with the age interaction variables, the effects of widowhood among individuals with younger and older children were obtained by summing the interaction coefficients and coefficients for the time-specific dummy variables. The impact of children is presented in Model 2 in Table A2 and in Figure 4 (younger widowed individuals are the reference group in the figure).
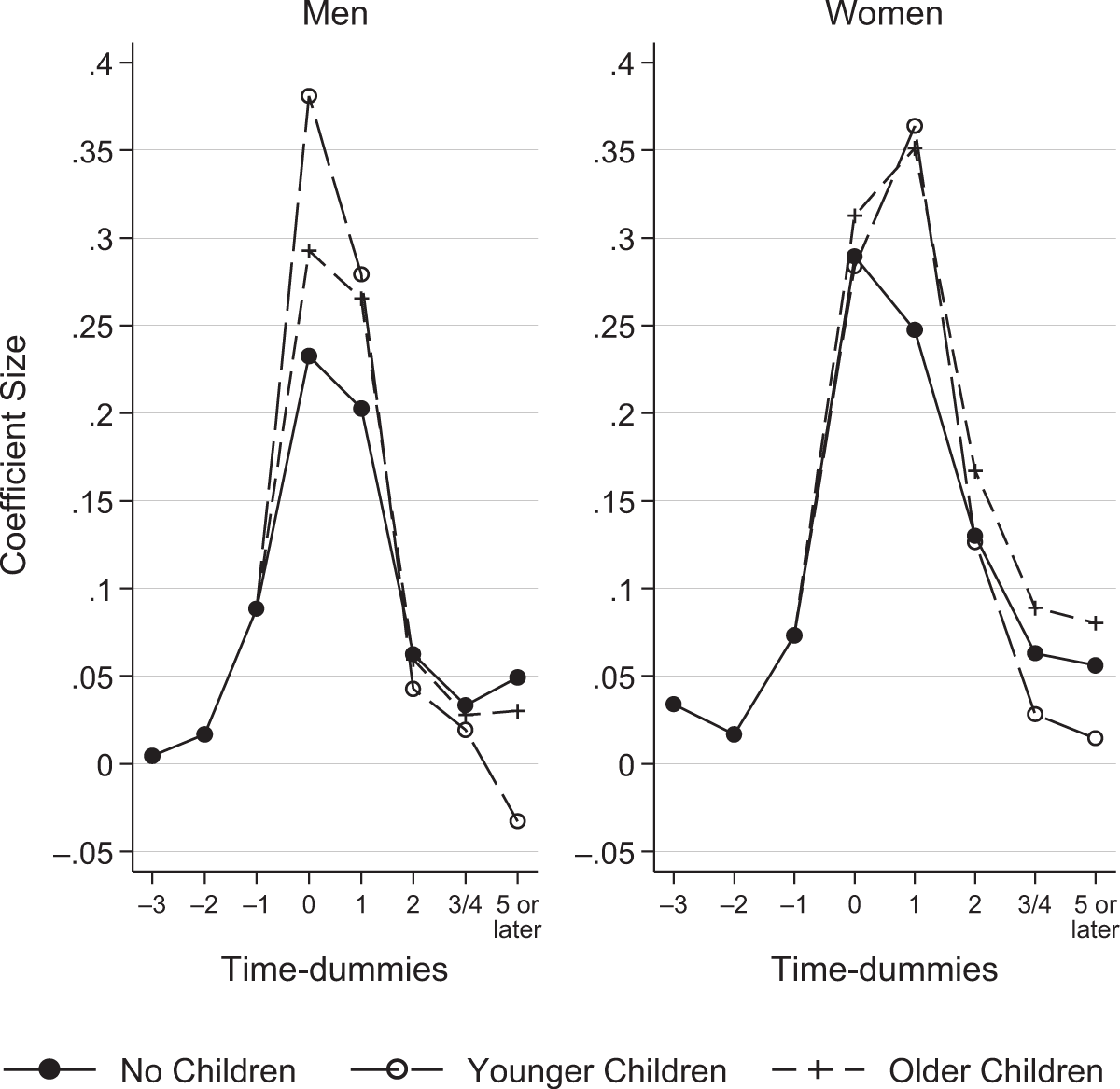
Time-dummy Coefficients for Younger Widowers and Widows with No Children, Younger Children (Age < 11 Years) and Older Children (Age ≥ 11 Years), FD-Trygd Database, 1993–2007 (N = 908,468).
Among men, having children at the time of widowhood facilitates the crisis response but moderates the long-term effect, especially if the widowers had children younger than 11 years. Compared with childless widowers, having young children at the time of widowhood is associated with a sickness absence rate that is 14.8 and 7.6 percentage points higher in the year of spousal loss and the following year, respectively. The long-term effect of widowhood, however, is reduced by more than 8 percentage points if the men had younger children at the time of spousal loss. Thus, parenthood seems to elevate the stress when widowed but may represent a long-term social resource among widowers.
Among widows, having children at the time of spousal loss affects the recovery period, albeit differently with younger and older children. Having younger children is associated with a sickness absence rate that is 11.6 percentage points higher in the year after spousal loss compared with widows without children, but, as among widowers, young children reduce the long-term strain (by 4.2 percentage points). Having older children at the time of spousal loss is associated with a prolonged recovery period, even five or more years after the transition to widowhood.
The age difference in the effect of widowhood after controlling for the presence of children is shown in Figure 5. The reference group is widowed individuals without children. There is practically no age difference in the effect of widowhood among men, whereas the prolonged recovery period among younger widows is somewhat reduced. Thus, it seems reasonable to conclude that the higher crisis response among younger widowers compared with middle-aged widowers is related to the stress of childcare, whereas the presence of children can explain a certain amount of the prolonged recovery period among young widows.

Time-dummy Coefficients for Widowers and Widows with No Children by Age, FD-Trygd Database, 1993–2007 (N = 908,468).
Discussion
The purpose of this study was to examine the health impact of losing one’s spouse at an early life stage, with particular attention to the gendered and age gradients of the widowhood effect, by using medically certified sickness absence in Norway as a measure of general health. In line with previous research, these results underscore the importance of conceptualizing the detrimental effects of widowhood in accordance with the duration of the widowhood state, the timing of spousal loss in relation to chronological age, and how these variables interact with gender (Barrett 2000; Hughes and Waite 2009; Liu 2012; Sasson and Umberson 2014; Williams and Umberson 2004).
It seems reasonable to conclude that the differences in sickness absence rates between married and widowed individuals are not a result of selection processes. Four to five years preceding spousal death, married individuals and those who will lose their spouse have a similar rate of sickness absence. However, the results show that the sickness absence rate increases markedly two years preceding widowhood and thus highlight that widowhood is a process that begins long before the spouse’s actual death. The most likely explanation for such an antecedent effect of widowhood is that spousal loss is often preceded by a period of spousal illness and stress associated with caregiving responsibilities. An antecedent effect of widowhood on health was previously found by Sasson and Umberson (2014), Lee and DeMaris (2007), and Carr and Utz (2001).
In theoretical terms, the empirical findings lend clear support to the crisis model. The sickness absence rate peaks in the year of spousal death and remains high for about one year after the transition to widowhood, whereupon the rate drops markedly. Returning to work shortly after experiencing a traumatic life event is obviously difficult. More than half of employed widows receive sickness absence benefits for more than 14 days during the year of spousal loss and during the following year, whereas about 40% and 50% of the middle-aged and younger husbands, respectively, receive sickness absence benefits in the year of spousal loss. With the exception of middle-aged men (who stand out with a relatively low crisis response), these short-term effects are about the same among men and women measured in percentage points. However, relative to the pre-widowhood sickness absence level, the crisis response is greatest among young men.
Clear support for the crisis model does not imply a dismissal of the social-role model. First, the recovery period shown in these data is remarkably long: it takes about three years for the sickness absence rate to level off and stabilize. Martikainen and Valkonen (1996a), Schaefer et al. (1995), and Stroebe et al. (2007) found that excess mortality following widowhood dropped after about six months. Even the study by Vahtera et al. (2006) comparing sickness absence rates before and after family death and illness reported a shorter recovery period than found here. According to their findings, it takes from 7 to 18 months for sickness absence rates to level off and stabilize. A possible explanation for this discrepancy in findings may be that Vahtera et al. (2006) included shorter sickness absence periods not requiring approval by a treating doctor, and they also focused on other family members’ illnesses and deaths. In terms of the recovery period, the current study corresponds more with the study by Carnelley et al. (1999) showing that depression levels following widowhood did not fully recover for three years. Thus, the analyses here show that the detrimental effects of widowhood last well beyond the initial transition period (for similar findings, see also Berntsen and Kravdal 2012; Blomgren et al. 2012; Hughes and Waite 2009).
Second, it is likely that higher attrition rates among widowed individuals (i.e., outflow to unemployment or own death) may have resulted in somewhat downward biased estimates when estimating the long-term effects of widowhood. Indeed, Table 1 reveals that both mortality and unemployment were higher five years after spousal loss than among those continuously married, indicating a considerable long-term strain of widowhood.
Third, in support of the social role model, the results show that women who experience spousal loss at an early life stage experience a high rate of sickness absence even five or more years after spousal loss. This may indicate that losing one’s husband at an early life stage represents not only a traumatic life experience with short-term health consequences but also a transition to a new social role encompassing serious and long-lasting challenges. The linear probability fixed-effects models show that neither aging nor changes in household income or seasonal fluctuations could explain the long-term strain associated with being widowed.
Fourth, in accordance with the assumptions underlying the social role model, entering a new marriage reduces the sickness absence rate, primarily among men. This indicates that the protective features of marriage are restored when entering a new marriage, especially among men.
Thus, the analyses here lend support for both the crisis and social-role models. However, the explanatory power of these theoretical models seems dependent upon gender and age. The crisis model appears to explain the development of the sickness absence rate among younger widowers, whereas the social-role model is more applicable to younger widows. In both cases, the impact of widowhood is stronger when it occurs at an early life stage. A greater crisis response to widowhood among younger men is shown extensively in previous research (e.g., Shor et al. 2012; Stroebe et al. 2007), whereas a prolonged recovery period after widowhood among widows is found mainly in studies using sickness absence and depression scores as health measures (Umberson et al. 1992; Vahtera et al. 2006; Williams and Umberson 2004). Mortality studies, conversely, have found a prolonged recovery period among widowers, not widows (for a relevant review, see Shor et al. 2012). It is likely that this discrepancy in findings is related to different measures of health (mortality vs. self-reported health).
Furthermore, the analyses here show that the presence of children at the time of widowhood explains much of the age gradient of the widowhood effect, especially among men. As previously suggested and discussed by several scholars (e.g., Hemstrom 1996; Joung et al. 1997; Liu 2012; Smith and Zick 1996), this indicates that the excess strain associated with experiencing widowhood at a young age is explained not by age in itself but rather the broader life stage in which these individuals are situated. To my knowledge, this has not been empirically shown in previous research. Moreover, these analyses show that the additional stress associated with having young children decreases over time and may even benefit widowers and widows in the long term. Having older children does not alter the long-term effect of widowhood among men but seems to prolong the recovery period among widows. A potential explanation for this may be that older children (defined as 11 years and older) may have moved out of the household when reaching adulthood, whereas younger children still live with the widowed parent and may offer their parent social support. It therefore seems that parenthood increases the short-term stress associated with the transition into widowhood but may represent a long-term social resource, especially among men.
Overall, this work shows that the theoretical relevance of both the crisis and social-role models are best understood in dialogue with a life course approach. Spousal loss is obviously a traumatic life experience with serious health-related consequences, especially if it occurs at an early life stage and the bereaved must care for vulnerable children. In line with several other studies on marital transitions and health, this paper illustrates that studying sickness absence as a measure of general health over time offers new insight into how critical life events affect health at young ages (e.g., Blekesaune and Barrett 2005; Dahl et al. 2015; Kivimaki et al. 2002; Vahtera et al. 2006).
An inherent limitation to using sickness absence as a measure of general health is that the generalizability is limited to the working population. According to Statistics Norway (2015), widowed individuals under 60 years constitute only 7.7% of the widowed population in Norway during 2014 (7.4% among widows and 8.8% among widowers). As a result, the findings from this study are not directly comparable to studies of health and widowhood in old age but rather are restricted to an age group when spousal loss is relatively rare. Thus, this study’s primary contribution is improved knowledge about how spousal loss affects health at younger ages. In that sense, sickness absence seems to be a valuable measure for younger populations, especially in countries where labor market participation rates are high for both men and women, and sickness absence benefits are universally available (as is the case in Norway). Another potential limitation with using sickness absence as a measure of general health is that treating doctors may be inclined to diagnose their patients with diagnoses that give access to sickness absence benefits. Although it is possible that doctors’ sympathy may explain parts of the revealed pattern (especially among individuals with children), it is unlikely that doctors will misdiagnose their patients out of sympathy long after the death of their spouse.
A greater limitation of the present study is that widowed individuals have higher rates of attrition out of the data compared with married individuals (see Table 1), potentially causing downward biased estimates. Higher outflow rates to unemployment and disability pension are especially likely to leave a positively health-selected group of employed widowed individuals as time passes. As a result, the relatively small long-term disadvantage associated with being widowed and the steep drop in the sickness absence rate after widowhood should be interpreted with some care. Thus, this paper underscores the need for more research on how and why the impact of widowhood is moderated over the life course and in various contexts, ideally comparing different health measures.
Footnotes
Supplemental Material
Appendices are available in the online version of the article.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.