
Abstract
We make meaning of disease, suffering, and death through narrative, by telling a story. In a therapeutic narrative approach, this article explores the influence of shamanic intervention in psycho-oncology. This qualitative study seeks to present the narrative effects of detailed shamanic sessions (the use of the drum and telling and interpreting visions according to the shamanic mythology) in the context of psycho-oncological treatment. In particular, the narrative positions of a patient (Mrs. AA) are described (using a software linguistic analysis, T-LAB) as they occurred before and after shamanistic sessions. The authors suggested that the shamanism sessions enabled Mrs. AA to produce a larger and more singular narrative about her end-of-life experience: from the initial narrative position of feeling “the acute consciousness of finiteness” to an emergent narrative position based on “consciousness of an interdependence/interconnection in all human and spiritual relationships.”
Narratives are not just the stories we tell our children at night; they are the stories we tell ourselves, the stories that help us make sense out of and find meaning in our experiences (Klein, 2010). Constructing stories is a natural human process that allows one to organize and remember events in a coherent fashion while integrating thoughts and feelings (Pennebaker & Seagal, 1999). In the humanistic approach (Santarpia, 2016), narration is a written or verbalized gestalt (autobiographical, fictional, or poetic), bringing to mind the capacity of the reflexive consciousness to mobilize the meaning-making process based on the following:
Human and motivational systems (attachment, sensuality, sexuality, exploration, transcendence, caregiving, social affirmation, aversive responses (Lichtenberg, Lachmann, & Fosshage, 2011; Maslow, 1943)
The multiple positions of the self (Hermans, 1993) that address the other (real or imaginal) in time (Ricoeur, 1984), in space, and in the world (Bruner, 1986)
William James (1890) thought that beings are organized and directed by needs or motives; particular events receive emotional value when certain human basic motives are fulfilled or frustrated (Hermans, 1999; Lichtenberg et al., 2011; Maslow, 1943). This idea was the starting point for a narrative theory of the self based on the metaphor of the person as a “motivated storyteller” (Hermans, 1999).
Brain imaging (Hasson, Yang, Vallines, Heeger, & Rubin, 2008; Honey et al., 2012; Lerner, Honey, Silbert, & Hasson, 2011; Regev, Honey, Simony, & Hasson, 2013; Silbert, Honey, Simony, Poeppel, & Hasson, 2014; Simony et al., 2016) supports the idea that when we tell stories to others, there is a synchronization between the brain of the person telling a story and the one listening to it. An unconscious reciprocity therefore exists between the storyteller and the person who hears it. The narrative serves perhaps as a bridge, thus opening the door for deeper inwardness and relationship(s). A shared neural mechanism supporting both production and comprehension facilitates communication and underlines the importance of studying these elements within unified frameworks (Silbert et al., 2014). Kidd and Castano (2013) show that reading literary fiction temporarily enhances the capacity to identify and understand another’s subjective states. The capacity to remain open to the individual’s story not only enables the therapist to experience the world as the other person may perceive it but also offers an opportunity to “know and become familiar with” oneself as well. The patient in this sense becomes a “reflection” or “mirror” of the other.
Referring to the therapeutic use of constructing stories, the idea that the verbalization of feelings can help reduce distress is not new in psychology (Titchener, 1908). Several empirical studies have now demonstrated that verbal disclosure of a traumatic experience can improve physical and psychological well-being in the long term (Hemenover, 2003; Pennebaker, 1997). Pennebaker and colleagues (Pennebaker, 1989, 1997, 2000; Pennebaker & Seagal, 1999) have demonstrated that when individuals write about emotional experiences, significant physical and mental health improvements follow: faster healing after surgery, low blood pressure, stronger immune function, reduced physical symptoms, better sleep in cancer patients, and less fatigue during rheumatoid arthritis. Emotional, physical, and spiritual health and well-being is contingent on the “telling of the story.”
Narrative and Palliative Care
Protracted illness in particular has the ability to disrupt the life story (Frank, 2013) and can radically frustrate basic human motives. Frank’s term deep illness (Frank, 1998) concerning protracted illness is experienced in the certainty that it will be permanent, and with fear of this permanence. Dame Cecily Saunders (1978) can be credited as the caregiver who first advocated the value of listening to the patient’s story; taping and transcribing the illness experiences of hundreds of her dying patients, she transformed medicine (Wittenberg, Ragan, Ferrell, & Virani, 2017). She noted that the care of the whole person included the treatment of “total pain”: physical, emotional, social, and spiritual (Sasser & Puchalski, 2010).
Indeed, facing the end of life, death, evoked by serious diseases (e.g., cancer) is not only a question of techno-scientific medicine, of medical treatment, but also a therapeutic work on our narrative identity 1 (Ricoeur, 1984) and on the appropriate use of a discourse on the disease that can alleviate the anxieties (Kleinman, 1988; Pennebaker, 2000). The literature that connects narrative and palliative care is rich and varied (for a detailed review, see Charon, 2006; DasGupta & Hurst, 2007; Kleinman, 1988; Stanley & Hurst, 2011): A study of 105 published narratives of health care (Wittenberg-Lyles, Greene, & Sanchez-Reilly, 2007) concluded that using patient and caregiver narratives in health care can assist practitioners. A “good death” includes a relationship between the patient and the practitioner “strong enough to overcome the patient’s feelings of isolation and abandonment” (Wittenberg-Lyles et al., 2007, p. 200). Narrative becomes intrinsic to ensuring patients’ quality of life throughout the continuation of an illness.
Narratives in Shamanic Mythology
In palliative care, little is known about the therapeutic effects of narrative interventions.
Archetypal and post-Jungian approaches (Hillman, 1985, 1997; Samuel, 1995) proposed the idea of therapy “as a search for mythological narrative.” Myths are the stories, the narrative systems people tell to explain nature, history, and customs. From this perspective, a myth is a story of ample perspective in which patients can recognize and distance themselves from their individualism. The myth has the power to restore the individual’s connection to the unconscious. The mythological narrative may not only help the individual connect with unconscious material that belongs exclusively to him/her (personal unconscious 2 ), but it may also allow for the reorganization or integration of the ego 3 (Jung, 1960/1969) into both the larger Self 4 and the archetypal world (collective unconscious 5 ). This is especially important for cancer patients who may attempt to find meaning in their end-of-life experience(s).
In tribal cultures, myths renew the person’s relationship with the divine. A balance between the human realm and the “land of the gods and goddesses” or, psychologically speaking, between the ego and the unconscious is therefore experienced. The biographical dimension (our life story) is thus inscribed in the collective dimension, and its existential sufferings become more bearable, because it’s possible to see the underlying metaphysical cause (Venturini, 1998a, 1998b). Our words give rise to the revelation of other, more distant voices (Santarpia, 2016; Venturini, 1998a, 1998b), and myths are characterized by rhetorical figures (allegories, metaphors, etc.).
In this article, we ask whether a mythological narrative exists that has the power to perform a spiritual transformation on a chronically ill body, even in the face of death.
One of the earliest known genres of mythological narrative in which disease becomes a vehicle for spiritual transformation is that of the shaman (Klein, 2010). Shamans develop symbol systems drawn from the archetypal images that are vital to their psychic healing technique (Grim, 1983). Shamanic tradition has marked universal human cultures, has a history that dates back between 30,000 and 40,000 years, and has been evidenced by the repeated discovery of various ancient cave paintings evoking shamanic activities such as dancing, playing the drum, and dressing with animal skin (Eliade, 1964; Harner, 1980; Moreno, 1988; Pickren, 2014). Michael Harner (1980) defines shamanism as an ancient tradition that uses a modified state of consciousness to acquire knowledge and power to help others. The use of the drum is usual in the shamanic rituals. Drumming facilitates modified states of consciousness and is a seen as a means of healing (Harner, 1980; Simon, 1998), symbolizing the cycles of seasons (winter, spring, summer, autumn) and of life (birth, life, death). The drum allows access to a specific state of consciousness, called the “shamanic state of consciousness.” It is characterized by the organized and multimodal (visual, auditory, tactile, kinesthetic) presence of mental imagery, compatible with shamanic mythology (Houran, Lange, & Crist-Houran, 1997; Noll, 1983, 1985; Walsh, 1995).
Shaman mythology consists of a superior, middle, and inferior world. The middle world is kind of a nonordinary counterpart to our “ordinary” reality. Natural spirits, for instance, are common in the shamanic middle world (Serr, 2017). The higher and the lower world exist outside time and space. In their journeys to the lower world, shamans explore and come into contact with power animals, visions of specific animals that transmit direct messages or symbolic actions relating to the meaning of the disease for the patients. The higher world is inhabited by spiritual guides who assist the shaman in healing work (Achterberg, 1985; Eliade, 1964; Harner, 1980; Money, 1997, 2001; Simon, 1998).
The shamanic tradition insists on the idea that disease is a message for the patient’s soul; it marks the need for a change and a new existential meaning (Money, 1997). Death is also a possibility to evolve, as it pushes the human to a full and meaningful existence (Buckley, 1993). Disease is the result of a loss of power, energy, or soul. Loss of soul occurs when we lose part of our vital force due to emotional or physical trauma; it exposes itself to a fragmentation of the self: A part of the soul flies into the world of spirits when the situation is too painful to bear. Souls can be stolen by those who (spirits or men) are not energized or who are full of envy (Eliade, 1964; Harner, 1980; Hultkrantz, 1996; Schmais, 1988; Simon, 1998). Illness thus becomes “dis-ease” The connection to the unconscious or the “soul” is truncated, and the person experiences isolation and aloneness. The subsequent suffering that is encountered not only results in detachment and the individual’s experience of a “loss of soul,” but it also manifests in dissociation from other human beings and the universe as well. Within this framework, the patient’s experience of healing does not necessarily connote a “cure,” but it denotes instead the renewal of the person’s ability to reconnect with his or her self. This relationship, however, extends beyond the parameters of the individual’s ego and also embraces a connection with the entire universe or “spiritual world.” In tribal cultures, the shaman was responsible for facilitating the health not only of the individual but of the tribe as well. Through the use of various incantations and rituals, shamans were able to “join with” these spirits and forces that transcended the boundaries of the ego. The lessons and insight that were attained through their communication with the “inner realm” were, in turn, transcribed to the tribal community. Shamans as “healers” were guardians of the individual and tribal “soul” and hence were pivotal in maintaining balance and harmony (Canda, 1983). Shamanic ritual and technique can serve as a mentor, therefore, to therapy and the therapeutic alliance, which focuses on caring for the person’s “soul” and fostering the proper rapport between the ego and the unconscious. Shamans often do not view illness as inherently “negative” but, instead, as an event that holds the potential for spiritual transformation and growth. Moreover, many studies have confirmed the erroneous association between people with schizophrenia and shamans (Boyer, Klopfer, Brawer, & Kawai, 1964; Noll, 1983; Van Ommeren et al., 2002). In fact, the shaman, as a healer, helps ameliorate the human’s connection with the divine or spirit world. The shaman is capable of “traveling through the supernatural worlds and seeing superhuman beings: gods, demons, spirits of the dead, etc. . . .” (Eliade, 1964, p. 509).
Eliade (1964) states, The shaman must first know if the soul of the sick man has been led astray from the village or if it has been stolen by demons and imprisoned in the other world. In the first case, healing is not too difficult: the shaman captures the soul and reintegrates it into the body of the sick person. In the latter case, it must descend to the lower world, and this is a complicated and dangerous undertaking. (p. 264)
Narrative therapy, through the “sharing of the story,” not only affords the person an opportunity to “process” the experience but also assists them in “meaning-making.” Along with the individual’s ability to ascribe meaning to an event, the narrative can empower and lend itself to an experience healing and “wholeness.” The experience of “separateness” therefore remains nonexistent in shamanic consciousness. Shamanic consciousness recognizes the nondual nature of the universe and sees the interconnectedness and interrelatedness of all things. This view lies in sharp contrast to Western culture, which often underscores the autonomy and independence of the individual. The shaman’s capacity to transcend the parameters between the self and the nonself affords him/her the ability to perceive the world through the prism of the experiences of others rather than solely through the lens of his/her own personal experience and belief system (Meuche, 2015).
Hypothesis
Hermans (1999) with his colleagues (Hermans, Rijks, & Kempen, 1993), analyzing the verbalizations of the participants, suggested that dialogue is made possible by the temporary hierarchical arrangement of “I-positions” that periodically and spontaneously realign themselves, with dominant “I-positions” retreating into the background and previously nondominant self-positions coming to the forefront. In this article, we describe the narrative positions of the self or “I-positions” (Hermans, 1993) in Mrs. AA’s narrative of her illness taken before, during, and after a western shamanic treament. In our research, after the statistical computation (see the methodology), we looked for the associations recalling moments of the patient’s narrative (M1, M2, M3…) of a general narrative position concerning a global existential experience. Recurrent themes revolved around finding meaning in life, her connection to humanity, balance and harmony with the universe, and a sense of transcendence (Breitbart, 2002; Bryson, 2004; Byrne, 2002; Carroll, 2001; Dyson, Cobb, & Forman, 1997; Frankl, 1959; Taylor & Ferszt, 1990; Yalom, 1980). Following the phenomenological tradition (Giorgi, 1997, 2009; Husserl, 1977), these narrative moments are integral parts of the whole and belong to the entire narrative position of the self (Hermans, 1999; Hermans et al., 1993). From this, based on our findings and perspective, we conclude therefore that these narrative moments cannot be separated from the general meaning structure (narrative position).
We propose that the shamanic mythology can become a vehicle for spiritual transformation. The authors also wish to suggest that shamanism can be used as a creative intervention in enabling patients to produce larger and more singular narratives that we would designate as a “transpersonal narrative position” surrounding end-of-life experiences. We believe that it is crucial for the reader to understand that an individual’s continued experience of “wholeness” while living with cancer encompasses not only a sense of physical well-being and security but also a feeling of emotional and spiritual integrity. Although a person’s physical, emotional, and spiritual well-being can stand alone, these components nevertheless are undeniably connected and related to one another. Shamanism has much to contribute therefore as medicine begins to expand its understanding of an individual’s care from a holistic viewpoint. Through the employment of various shamanic techniques such as chanting, drumming, and singing, patients are afforded an opportunity to find strength in their self. They can begin to address the challenges inherent in ascribing meaning to their illness and experiences.
Method
This piece of research is based on the methodology of idiographic science (Salvatore, Valsinier, Strout, & Clegg, 2009; Toomela, 2009; Valsinier, 2007): Cases should be understood as singular individuals constrained by the given time and the given environment. Moleenar and Valsinier (2005) proposed that “case-specific uniqueness” can act “as a representation of generic, universal processes (p. 1). Moreover, several authors have argued about the relevance of case studies in psychotherapeutic process research, especially the possibility of answering the questions of how and why change occurred (Gedo, 1999; Hilliard, 1993; Kazdin, 1981; Kiesler, 1981; Moleenar & Valsinier, 2005; Morgan & Morgan, 2001; Stiles, 2003, 2007; Yin, 2005).
One such case study was conducted in a French oncology unit by a psychology intern with academic supervision. Mrs. AA is a 63-year-old married woman whose 30-year-old son recently returned to live in the parental home. After spending nearly 40 years as a leading model in the clothing industry, she stopped her career on the discovery of advanced breast cancer. She signed a “consent to participate” form, which specified that she could leave the study at any time and that all personal information about her would be kept strictly confidential. Prior to her participation in this research study, Mrs. AA was screened by the attending psychiatrist to determine whether or not any substance abuse history and/or current drug use existed. The results of the psychiatric evaluation neither indicated any history of drug abuse nor had Mrs. AA experienced any significant psychiatric events in her life, such as psychosis or schizophrenia. Her scores on the anxiety effect, measured by The State-Trait Anxiety Inventory (Spielberger, 1983), also demonstrated “weak” to “very weak” anxiety. After careful deliberation and further consultation with the psychiatrist, it was decided that Mrs. AA was suited to partake in this study. It should be noted that throughout the protocol Mrs. AA continued to undergo psychiatric evaluation in which her psychological/emotional stability and integrity were closely monitored. Given these indicators, the visions and narrative that Mrs. AA shared with the team do not appear to be influenced by any chronic mental illness or modified state of consciousness initiated by drug use.
Presentation of Shamanic Therapist
This study was made possible thanks to the participation of a 57-year-old French female Mrs. BF, a professional music therapist who undertook substantial training in shamanism with a female Amazonian Indian shaman. 6 Mrs. BF completed 7 years of training with two or three trips to the Amazon Rainforest. She also learnt and integrated Amazonian and Ojibway shamanic traditions. She performs rituals for releasing, cleansing, and harmonizing (using plants). These ceremonies are essential to purifying the body, spirit, and heart, and they can be used for healing. Generally, she dances and plays the drum in her interventions; however, in these specific sessions, she played traditional musical instruments: the singing bowls, the chimes, the rain stick, the drum, and the sanza. Mrs. BF sang lullabies: “buenas noches” from Chilean tradition, “pehe pehe” from Tahitian tradition, and/or “yemaya” from African culture. The therapeutic style of the shamanic therapist was inspired by Rogerian psychotherapeutic principles: empathy, congruence, nondirectivity, and unconditional positive regard that empowers and motivates the client in the therapeutic process (Rogers, 1951, 1961, 1975). During the sessions, this approach and style allowed the unconscious material to flow naturally and according to its own rhythm and beat. She trusted this “process,” or, metaphorically speaking, honored the wisdom and knowledge of the spirit world. She did not lead the process but, rather, guided the person on the journey and acted as an interpreter of dreams.
Her interventions belong to the Core Shamanism approach, identified by the research of Michael Harner (1972, 1973, 1980), whose publications reintroduced shamanism to the West. Core Shamanism incorporates the techniques of different shamanic traditions to make them usable and accessible to people in Western cultures. In this article, we will use the definition of “shamanic therapist” or “therapist” when we talk about Mrs. BF.
Design and Procedure
During the sessions, the lighting was reduced to approximately 10 cd/m2, the temperature was 21°C, and the sonor level was 40 dB (weak noise generated by the electricity supply). A massage table was provided (see Figure 1), on which the patient was invited to lie down and on which there are blankets and sheets. There are two sofas. The first sofa allows the therapist to place/order her musical instruments, and on the second, the therapist positions herself behind the patient so that she does not see her. The shamanic therapist sat on a black chair at the patient’s bedside.

Setting for the shamanic sessions.
Data Collection and Analysis
Preliminary Interview
We established a research protocol focused on three stages (a preliminary interview, shamanic interventions, and a final interview), organized over 5 weeks. A preliminary interview of about 45 minutes was conducted in which the patient’s phenomenological experiences of the illness were discussed (Kaufmann & Singly, 2011). This interview model was inspired by Rogerian nondirectivity approach (Rogers, 1951). It was used to make a connection with the patient’s phenomenological world. Shamanism stresses the significance of “preparation” through the use of ritual and various techniques before the individual descends into the realm of the gods and goddesses. If the person is inadequately suited for the journey, he/she runs the risk of being spiritually and psychologically devoured. The shaman thus spends a great deal of time with the individual to develop rapport and trust. Similarly, psychotherapy denotes the importance of establishing a therapeutic relationship with the patient before any descent into the inner world of the unconscious can be undertaken.
Shamanic Intervention
One week after the preliminary interview, the therapeutic work for the patient started. It consisted of three shamanic sessions of about 1 hour (50-55 minutes approximately), each one being offered once a week, following shamanic principles and mythology.
Session I
The first session was characterized by a suggestive narrative of the therapist focused on the power of the drum and the power of the animal world: You will listen to me. I followed the teachings of an Indian shaman from the Amazon and learned to understand the power of the drum. For the Indians the drum was a healing instrument. This drum generates a particular sound and beat and in five minutes one can experience a modified state of consciousness. This state of consciousness is very similar to the experience of dreaming. It is a world of endless possibilities and vision.
After this presentation, the therapist played an audio recording of a drum shamanic session
7
(15 minutes). Then the therapist asked the participant to lie down on the table and relax by trying to loosen the body by being comfortably positioned. After the sound recording of the drum, time (15 minutes) is dedicated to the storytelling of visions and their interpretation.
8
Therapist vision concerning Mrs. AA. In my journey, I saw a wolf. She lived in a community that was home to her cubs. I saw you there with all the little cubs surrounding you. You told them stories. You were respected by the tribe. You were the wolf who has knowledge and who was seen taking care of her family. It was you who told magic stories to the children. Therapist interpretation concerning Mrs. AA. Mrs. AA, you could welcome the children and tell them stories (Patient smiles). Even if you don’t have the opportunity to play and to run with them, the children will come to see you. Thanks to the wisdom you hold, they will listen to you and your stories.
The experience continued for the patient. She listened to the songs and traditional music (15 minutes). Mrs. BF sang lullabies. The session finished with a reassuring speech by the therapist. This helped the patient return to the ordinary state of consciousness.
Session II
The second session had the same temporal organization with an important variation—the therapist played the drum. Mrs. AA could “travel” and “tell her visions.” Mrs. AA vision. I saw birds and clouds. And, I saw gray swirls. These swirls were blue, and I just stayed there, present in the moment, and simply watched their movement. Therapist interpretation. There is a movement of gray towards the blue. You are moving towards the opening and the positivity. This positive space of beauty, sun, and sky awaits you.
Session III
In the third session (as in the first session), the therapist activated the recording and set out on a “journey” through the “high world” to heal the patient’s crystal body.
Therapist vision. I did not see crystals. I was in a cabin. I went up and saw a large shell that welcomes you. I did not see crystals. I saw shapes. I saw the energy at the level of the head. There was a black stone at the level of the third eye. It was necessary though for this stone to depart? The stone dissolved. I saw many white shapes that circulated in the body. I asked my guides what I should do and for guidance. . . . Cleaning deep. At your feet, there was a hot water bottle. And this bottle; it sucked to provide great cleaning. I saw the body open wide; there was a lot of whiteness, and it was very bright. I saw a beautiful energy circulating, and I asked my masters to continue. I asked them to continue what needed to be done. Therapist interpretation. I have not seen black things. One can often see broken and burnt crystals with spears. This is not the case here. I saw energy, beams, circular membrane, and the third eye. A chest and foot purification. There was purification and a beautiful space. It is good; you are in the hands of the guides.
In summary, each shamanic session consisted of 5 minutes of interview, 15 minutes of drumming, 15 minutes of either the therapist’s narrative or the patient’s narrative, 15 minutes of traditional music and songs, and 5 minutes of reassuring speech to conclude the experience; in total, the session was 50 to 55 minutes approximately.
Final Interview
Last (Stage 3), a final interview on the experience was conducted by the psychologist, using nondirectivity approach (Rogers, 1951).
Analysis of the Narrative
The interviews and sessions were recorded on a Dictaphone and then transcribed accurately, as a support for analysis of the data. It was analyzed with the aid of the software T-LAB version 9.1.3, a linguistic and statistical tool for text analysis, developed by Franco Lancia (2004, 2007). In choosing T-LAB software over others, two advantages were key: the multitude of instruments offered for text analysis and the possibility to use them in an integrated way (e.g., word association, thematic analysis, co-occurrence analysis, comparative analysis), and the possibility of analyzing a very large text. T-LAB works on a corpus that can be composed of one or more texts and can be divided into different subsets, according to the variables employed for describing the texts.
In this research, we used a “word association analysis.” This T-LAB tool allowed us to pick out a co-occurrence relationship within any corpus. This strategy determined the local meaning of selected keyword, on the basis of a specific keyword-in-context list (Weber, 1984), following the principles of a directed content analysis (Hsieh, 2005). Word co-occurrences are computed within elementary contexts (sentences or paragraphs). Each time, the selection of associated words is carried out by the computation of an “Association Index” (Cosine, Dice, Jaccard), and their computation is quite fast. Moreover, the user had to take into account that the greater the number of words included in their list, the more reliable the similarity values become. In our analysis, first we added temporal variables in the preparation of “the Corpus”: “Before” for the narrative in the preliminary interview and “After” in the final interview. Second, we organized a target conceptual category of DISEASE evoking our topic research (see target term in the radial diagrams, Figures 2 and 3), composed of five lemmatized keywords referring (cancer, disease, to_be_sick, chemotherapy, hospital). We organized another conceptual category crucial for our research, SHAMANIC-WORLD (see Figure 4) composed of five lemmatized keywords (spiritual_guides, shaman, shamanism, spirit, to_make_a_trip). We chose a level of word association significativity (p ≤ .05) and Cosine as the association index. Finally, this content analysis strategy generated a radial diagram, where the selected conceptual target is placed in the center and the other words are distributed around it, each at a distance proportional to its degree of association. The significant relationships are therefore one-to-one, to the central lemma, and to each of the others. After the statistical computation, we looked for the associations (see repeated characters that have a “bold” font style in our narrative examples) recalling moments of the patient’s narrative (see M1, M2, M3, etc., in the results) of a general narrative position evoking a global existential experience (e.g., “the acute consciousness of the finiteness”).
Results
The examined corpus for Mrs. AA was made up of 1,561 transcripted words; 10,029 occurrences (single words); and 1,406 lemmatized words; the number of hapax 9 was 797.
We chose a general list of lemmatized words ≥7 to generate a vocabulary before and after the shamanic intervention (see the appendix).
Mrs. AA’s Narrative (Before): The Acute Consciousness of the Finiteness
Concerning the conceptual category DISEASE (keywords: cancer, disease, chemotherapy to_be_sick, hospital) in preliminary interview (temporal variable, before, see Figure 2) is associated with “Reunion Islands” (χ2 = 6.00; p =.014), with “month” (χ2 = 4.87; p = .037), “scared” (χ2 = 3.96; p = .047), “She” (χ2 = 3.62; p = .05), “we” (χ2 = 4.33; p = .03). These associations (see repeated characters that have a bold font style in our narrative examples) in the preliminary interview concerning the disease evoked a rich narrative concerning “the acute consciousness of the finiteness.” This general meaning of narrative structure started with the moments surrounding the “announcement of the severity of cancer with the dramatic conflict to accept it or not (M1)”: M1. The blood test revealed that I had a very advanced breast M1. M1. I never accepted the M1. I had a very very very strong M1. I said yes to continued treatment, of course, because there had been some improvement. I was exhausted exhausted. When I did not have the

In the radial diagrams, the conceptual category DISEASE is placed in the center, before the intervention, in the preliminary interview. The others lemmatized words are distributed around it, each at a distance proportional to its degree of association. In the bold characters, we identified the lemmatized keywords associated with DISEASE and with a specific level of word association significativity (p ≤ .05), Cosine as an association index.
A successive crucial moment of her “acute consciousness of the finiteness” was discovering the reoccurrence of the cancer “with an increased and strong need to approach the family and her homeland (M2)”: M2. When my M2.
Mrs. AA’s Narrative (After): Consciousness of the Interconnection/Interdependence in All Relations
Concerning the conceptual category, DISEASE (keywords: cancer, disease, chemotherapy to_be_sick, hospital) in the final interview (temporal variable, after, see Figure 3) is associated with “Energy” (χ2 = 14.31; p = .001), with “week” (χ2 = 5.05; p = .0025), “To give” (χ2 = 4.45; p = .035), “Shamanic-world” (χ2 = 3.60; p = .05).
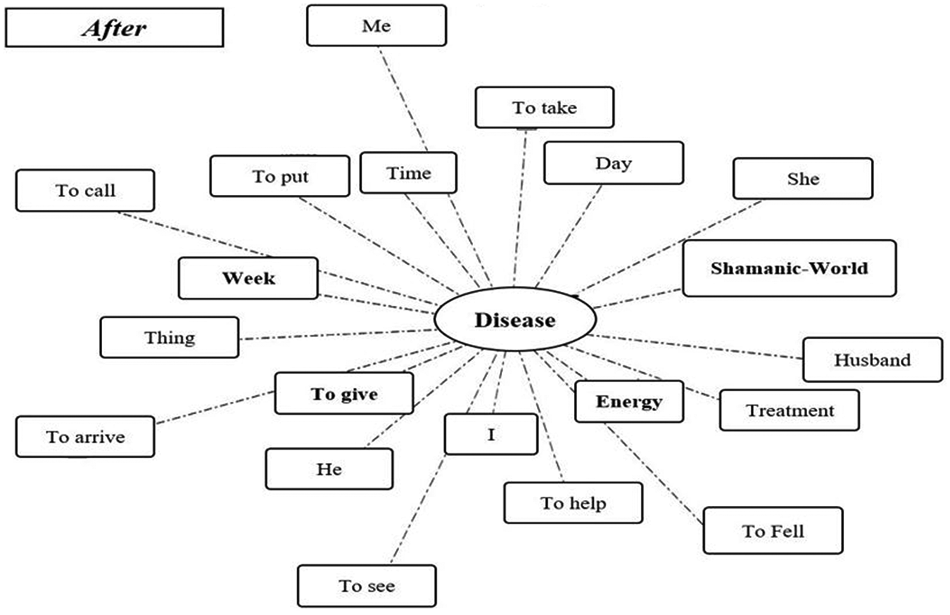
In the radial diagrams, the conceptual category DISEASE is placed in the center, after the intervention, in the final interview. The other lemmatized words are distributed around it, each at a distance proportional to its degree of association. In the bold characters, we identified the lemmatized keywords associated with DISEASE and with a specific level of word association significativity (p ≤ .05), Cosine as the association index.
These associations in the final interview concerning the disease (cancer) evoked a rich narrative on “the consciousness of the interconnection/interdependence in all relations (visible and invisible).” This general meaning of narrative structure started with the moment of “feeling yourself as a channel of interchangeable energy for herself and for others (M1)”: M1. Because it is true that since M1. The therapist treated me very well. She sees the M1. My sister-in-law called me and told me “You were
Following this, a crucial moment of her “consciousness of the interdependence and interconnection of all things” was seen, based on “the feeling of being in a new group, a new society (M2)”: M2. Now I have plans. In this
The narrative positions cited above intersected and combined with “the new and positive perception (M3) of the pain”: M3. Yesterday I had M3. One thing that is also important is the role of songs. She (therapist) sang at the end of the sessions. The songs soothed us. She
Concerning the specific relationship with the conceptual category SHAMANIC-WORLD (keywords: spirit, shamanist, shamanism, to make_a_trip, spiritual_guides), the final interview (temporal variable, before, see Figure 4) is associated with “Body” (χ2 = 9.18; p = .014) and with “I” (χ2 = 5.06; p = .024). In the general narration, we identified “the consciousness of the interconnection/interdependence in all relations (visible and invisible).” Mrs. AA mobilized a new narrative position, characterized by “the spiritual world composed of benevolent spirits that heal human bodies and her body (M4)”: M4. In any situations the M4. Creation, where there are forces. We constitute the M4. So now M4. We call them ( M4. M4. M4. My step-mother communicates with the M4. The therapist is a woman of extraordinary beauty. She is kind. She is the kind of person M4. M4. In the last session, M4.
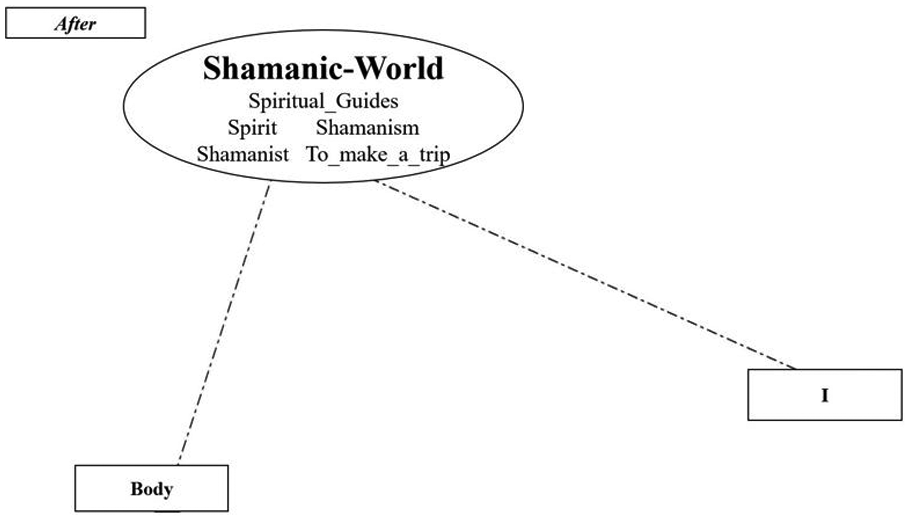
In the radial diagrams, the conceptual category SHAMANIC-WORLD is placed in the center, with two associative lemmatized keywords, “body” and “me” (word association significativity, p ≤ .05).
Discussion
Narratives are the stories we tell ourselves, the stories that help us make sense out of and find meaning in our experiences (Klein, 2010). Constructing stories is a human process which allows one to organize and remember events in a coherent fashion while integrating thoughts and feelings (Pennebaker & Seagal, 1999). Shamanic narrative and mythology is not simply a “story.” It serves a transcendent function and possesses the power to draw the individual inward and beyond the ego. Understood within this context, visions, metaphorical interpretations, and mythology have the ability, therefore, to orient the person’s vision toward realities existing beyond the parameters and boundaries of ordinary (ego) consciousness.
In this article, we described the positions of the self or “I-positions” (Hermans, 1993) in Mrs. AA’s narrative of her illness carried out before, during and after a Western shamanic treatment. We argued that shamanic mythology could become a vehicle for spiritual transformation. We suggested that shamanic intervention enabled the patient to produce a larger and more singular narrative that we could call a “transpersonal narrative position” about end-of-life experiences. In keeping with our objective research, we observed in the preliminary interview a dominant narrative position focused on “the acute consciousness of the finiteness for the patient and her family in relation to the disease.”
This general existential narration was invoked in a rich amount of literature (Furer & Walker, 2008; Meuche, 2015, 2016, 2017; Yalom, 2009). In his essay Thoughts for the Times on War and Death, Freud (Freud, 1915/1952) noted that “our unconscious does not believe in its own death; it behaves as if immortal” (p. 765). Modern theories are based on Becker’s existential view of death (Becker, 1973). He suggested that death anxiety is a real and basic fear that underlies many forms of anxiety and phobia (Furer & Walker, 2008). Becker’s work led to the development of terror management theory in which, according to terror management theory, when people are reminded of their mortality, their need for meaning increases. As witnessed in Mrs. AA’s encounter, her renewed connection to the “spiritual guides” afforded meaning to the cancer experience and offered a “sense of purpose” for her life. If illness is construed within the framework of “dis-ease” and connotes a brokenness and separation in a person’s relationship with the unconscious or divine, it might then be suggested, perhaps, that the capacity “to join and become one with” the unconscious material or spirit world is integral to healing and the individual’s experience of “wholeness.”
In our results, we observed a singular narrative in our patient. Mrs. AA talked about “the consciousness of the interconnection/interdependence in all relations (visible and invisible)”: I told her to take my energy, because I was going to see a lady (the therapist) who gave me a lot of energy . . . she gave me a lot of energy. And when I feel sick, now I know what to do, my future will be to help others.” This experience of Mrs. AA echoes the heart and essence of indigenous cultures and the tribal psyche.
In Lakota cosmology and spirituality, for instance, this is designated in an understanding of “wa’ce waki’ya” or “I am embracing relatives all around us”: For Lakota people, all aspects of life are intimately connected to good health and well-being. The interconnections among family, tribe, and clan with moral, political, and ceremonial life all contribute to a sense of harmony and balance called “wicozani” (good total health) by the Lakota and “hozhon” (harmony, beauty, happiness, and health) by the Navajo. For Lakota people, life is like a circle—continuous, harmonious, and cyclical, with no distinctions. Medicine and healing are a coming-together of all the elements in this circular pattern of life. The circle of healing is formed by the interconnections among the sick person, his or her extended family or relatives, the spirits, the singers who helped with ceremonial songs, and the medicine practitioner. (Voss, Douville, Little Soldier, & Twiss, 1999, p. 233)
Although it can be argued that the altered state of consciousness experienced by individuals who have been prescribed morphine or other opiates is similar to the experiences of those who have engaged in shamanic ritual, it is important perhaps to underscore the long-term emotional well-being and often life-changing influence of the “visions” and insight patients have gained from shamanic interventions (Vuckovic, Guillion, Williams, Ramirez, & Schneider, 2007). The significance of Mrs. AA’s experience of “nonduality” as referenced by her description of “the interconnectedness and interrelatedness of all things” appears to have a very positive and transformative influence on the manner and fashion in which she not only interpreted her illness but also construed the world and her place within it. Mrs. AA discovered comfort in her experiences and noted a profound difference in what she prioritized in her life after the experience with her therapist.
In the “new narrative position,” Mrs. AA internalized the therapist figure with her lullabies, her music, and her beauty. This internalization process activated an emergent and benevolent part of the self: One thing that is also important is the role of the songs. She (therapist) sang at the end of the sessions. The songs soothed us. The therapist is a woman of extraordinary beauty. She is kind. She is the kind of person I love. I love her physical appearance, her natural beauty, her charm, her kindness, she is adorable. And we can entrust our body to her, because she heals our body, our soul, our spirit, our soul.
Finally, Mrs. AA expressed a strong belief in a spiritual world: Creation, where there are forces. We constitute the spirits. They constitute us, the spirits are true, live. I believe in them.” and “We call them (spiritual_guides) with our means, we pray to them. I believe in the forces of the universe, yes I believe in them. . . . I am sensitive to spirits, to angels, we must not forget the angels.
On this kind of transpersonal narrative, Voss, White, and Lunderman (2004) wrote as follows: Each person is a living testament as well as a legacy of his or her ancestral spirits and the spirits of creation. These ancestral spirits and spirits of creation can and do influence the individual in important and significant ways. What is personal and what is ancestral are related; the boundaries of self-and-other are permeable (p. 55).
In line with our hypothesis, Mrs. AA produced a larger and more singular narrative. Mrs. AA seems to have internalized the therapist’s narrative.
Guided by the use of shamanic mythology and her therapist, Mrs. AA was able to reframe and transform her cancer experience and view it as a gift or path in which to seek and attain enlightenment and healing.
Shamans are important today because they express symbolically and poetically the forces that animate the natural and spiritual world. This particular ability to resonate with the natural world is seen as an important need in our time (Grim, 1983). Shamanic mythology can provide clinical psychologists and psychotherapists, especially those working in palliative care, an alternative resource in their meaning-making with patients.
Footnotes
Appendix
Vocabulary Before and After the Shamanic Intervention.

| Lemma | Before | After | Lemma | Before | After | Lemma | Before | After | Lemma | Before | After | Lemma | Before | After | Lemma | Before | After |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ABLE | 3 | 2 | HAPPY | 0 | 7 | OPEN | 4 | 0 | TO BELIEVE | 1 | 7 | TO START | 15 | 13 | TO SEND | 4 | 0 |
| ACTIVITY | 0 | 4 | HARD | 4 | 1 | PAPER | 1 | 3 | TO CALL | 3 | 11 | TO STAY | 3 | 5 | TO SPEAK | 15 | 13 |
| AFTER | 4 | 0 | HE | 57 | 48 | PART | 5 | 0 | TO CARE | 3 | 3 | TO CALL | 6 | 2 | TO START | 3 | 5 |
| ALLEY | 3 | 2 | HEAD | 4 | 4 | PATIENT | 9 | 3 | TO CARRY ON | 3 | 3 | TO CARE | 3 | 11 | TO STAY | 6 | 2 |
| ALSO | 3 | 2 | HEAR | 1 | 6 | PEOPLE | 4 | 0 | TO COME BACK | 4 | 0 | TO CARRY ON | 3 | 3 | TO STOP | 3 | 2 |
| BEAUTIFUL | 3 | 3 | HEAVY | 0 | 4 | PERSON | 7 | 3 | TO COMMUNICATE | 0 | 5 | TO COME BACK | 3 | 3 | TO SUFFER | 4 | 0 |
| BEGINNING | 1 | 4 | HOUR | 3 | 1 | PLEASE | 4 | 12 | TO CRY | 10 | 0 | TO COMMUNICATE | 4 | 0 | TO TAKE | 13 | 5 |
| BEINGS | 2 | 2 | HOUSE | 6 | 8 | POSITIVE | 6 | 0 | TO DEEPEN | 0 | 5 | TO CRY | 0 | 5 | TO THINK | 4 | 3 |
| BLOOD | 4 | 0 | HUGE | 2 | 2 | POSSIBLE | 1 | 3 | TO EXHAUST | 4 | 0 | TO DEEPEN | 10 | 0 | TO TRY | 8 | 7 |
| BODY | 2 | 16 | HUNDRED | 3 | 2 | POWER | 1 | 5 | TO EXIT | 6 | 0 | TO EXHAUST | 0 | 5 | TO UNDERSTAND | 4 | 4 |
| BREAST | 6 | 0 | HUSBAND | 17 | 10 | PRETTY | 4 | 2 | TO FALL | 5 | 1 | TO EXIT | 4 | 0 | TO WAKE | 0 | 5 |
| CANCER | 10 | 0 | I | 219 | 177 | PRODUCT | 4 | 0 | TO FEEL | 3 | 11 | TO FALL | 6 | 0 | TO WATCH | 4 | 2 |
| CAR | 5 | 1 | INTERNET | 1 | 3 | PROFESSIONAL | 5 | 0 | TO FIND | 6 | 3 | TO FEEL | 5 | 1 | TO WORK | 9 | 2 |
| CARE | 3 | 1 | JOB | 10 | 1 | QUICK | 7 | 0 | TO FOCUS | 1 | 3 | TO FIND | 3 | 11 | TOILET | 7 | 0 |
| CHEMOTHERAPY | 12 | 4 | LATEST | 4 | 6 | REALLY | 1 | 4 | TO FORGET | 3 | 3 | TO FOCUS | 6 | 3 | TREATMENT | 2 | 5 |
| CHILD | 5 | 0 | LEAVE | 6 | 0 | RECEIVER | 0 | 5 | TO GIVE BACK | 2 | 2 | TO FORGET | 1 | 3 | TREE | 0 | 4 |
| CURRENT | 2 | 2 | LET | 6 | 2 | RELATIVELY | 1 | 5 | TO GIVE BIRTH | 0 | 6 | TO GIVE BACK | 3 | 3 | TRUE | 3 | 2 |
| DAY | 19 | 16 | LEVER | 2 | 3 | REQUEST | 1 | 3 | TO GO | 7 | 4 | TO GIVE BIRTH | 2 | 2 | VERY MUCH | 11 | 4 |
| DESIRE | 0 | 5 | LIFE | 13 | 11 | RESPONSIBILITY | 7 | 4 | TO HELP | 10 | 6 | TO GO | 0 | 6 | WARNING | 3 | 1 |
| DIFFICULT | 2 | 2 | LOVE | 6 | 1 | SHAMAN | 4 | 0 | TO IMPLEMENT | 4 | 0 | TO HELP | 7 | 4 | WATER | 0 | 6 |
| DISEASE | 9 | 1 | LUCK | 3 | 1 | SICK | 0 | 13 | TO IMPORT | 4 | 3 | TO IMPLEMENT | 10 | 6 | WE | 81 | 49 |
| DOCTOR | 3 | 1 | MANAGE | 4 | 0 | SISTER | 6 | 5 | TO INFORM | 0 | 4 | TO IMPORT | 4 | 0 | WEEK | 10 | 4 |
| DRUG | 5 | 0 | ME | 15 | 37 | SMALL | 4 | 0 | TO KNOW | 1 | 6 | TO INFORM | 4 | 3 | WIG | 5 | 0 |
| EASY | 5 | 1 | MEANING | 4 | 6 | SO MUCH | 12 | 14 | TO LEARN | 8 | 0 | TO KNOW | 0 | 4 | WONDERFUL | 3 | 6 |
| ENERGY | 3 | 4 | MEETING | 4 | 3 | SOCIETY | 9 | 1 | TO LEAVE | 7 | 11 | TO LEARN | 1 | 6 | WORD | 3 | 4 |
| EVENING | 7 | 1 | MEETING | 0 | 6 | SON | 5 | 3 | TO LIVE | 8 | 3 | TO LEAVE | 8 | 0 | WORLD | 3 | 5 |
| EXPERIENCE | 1 | 10 | MESSAGE | 5 | 0 | SPIRITS | 10 | 12 | TO LOSE | 3 | 2 | TO LIVE | 7 | 11 | WRONG | 11 | 1 |
| FAMILY | 8 | 1 | METASTASIS | 4 | 0 | SPIRITUAL_GUIDES | 0 | 14 | TO LOVE | 10 | 18 | TO LOSE | 8 | 3 | YEAR | 16 | 14 |
| SCARED | 4 | 3 | MOM | 2 | 3 | STATE | 0 | 7 | TO LOWER | 3 | 1 | TO LOVE | 3 | 2 | YOU | 47 | 53 |
| FIRST | 2 | 5 | MONTH | 16 | 9 | STEPMOTHER | 3 | 4 | TO OCCUPY | 3 | 1 | TO LOWER | 10 | 18 | |||
| FLOWER | 0 | 4 | MORE | 0 | 7 | SURE | 0 | 8 | TO PREFER | 4 | 0 | TO MAKE_A_TRIP | 3 | 1 | |||
| FOOT | 5 | 1 | MORNING | 1 | 6 | THE SAME | 5 | 2 | TO PREPARE | 0 | 6 | TO OCCUPY | 3 | 3 | |||
| FRIEND | 9 | 1 | MORPHINE | 2 | 4 | THEY | 4 | 1 | TO PUT | 5 | 8 | TO PREFER | 3 | 1 | |||
| GARDANNE (city) | 4 | 0 | NEED | 3 | 3 | THING | 18 | 5 | TO REACH | 3 | 1 | TO PREPARE | 4 | 0 | |||
| GIVE | 12 | 17 | NEW | 1 | 5 | TIME | 11 | 15 | TO REMAKE | 4 | 0 | TO PUT | 0 | 6 | |||
| GRANNY | 4 | 4 | NEXT DAY | 4 | 2 | TIME | 1 | 3 | TO SCAN | 4 | 0 | TO REACH | 5 | 8 | |||
| HAIR | 5 | 0 | NIECE | 4 | 0 | TIRED | 13 | 7 | TO SEE | 22 | 23 | TO REMAKE | 3 | 1 | |||
| HAIRDRESSER | 5 | 0 | NORMAL | 3 | 1 | TO ACCEPT | 1 | 5 | TO SEND | 4 | 0 | TO SCAN | 4 | 0 | |||
| HAND | 5 | 2 | NURSE | 4 | 0 | TO ARRIVE | 12 | 12 | TO SPEAK | 15 | 13 | TO SEE | 22 | 23 |
Acknowledgements
The authors would like to express their thanks to Tonino Anzante for commenting on and proofreading this work.
Authors’ Note
We dedicate this article to Isaia Casale and to the memory of Giuseppe Santarpia, who passed away on November 22, 2015.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.